Article Text

Abstract
Objective To describe the development and implementation of a web-based high-quality data collection tool to track the outcomes of glaucoma treatments in routine practice.
Methods and analysis This is a prospective observational registry study. An international steering committee undertook an iterative structured process to define a minimum, patient-centred data set designed to track outcomes of glaucoma treatment. The outcomes were coded into a web-based programme allowing easy access for rapid data entry. Clinicians receive personal reports enabling instant audit of their outcomes. Analyses of aggregated anonymised data on real-world outcomes are analysed and periodically reported with the goal of improving patient care.
Results The minimum data set developed by the international steering committee includes the following: a baseline visit captures 13 mandatory fields in order to accurately phenotype each patient’s subtype of glaucoma and to allow comparison between services, and a follow-up visit includes only four mandatory fields to allow completion within 30 s.
Currently, there are 157 surgeons in 158 ophthalmology practices across Australia and New Zealand who are registered. These surgeons are tracking 5570 eyes of 3001 patients and have recorded 67 074 visits. The median number of eyes per surgeon is 22 eyes with a range of 1–575. The most common glaucoma procedure, excluding cataract surgery, is iStent inject, with 2316 cases.
Conclusion This software tool effectively facilitates data collection on safety and efficacy outcomes of treatments for different subgroups of glaucoma within a real-world setting. It provides a template to evaluate new treatments as they are introduced into practice.
- glaucoma
- treatment surgery
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Registries provide cost-effective longitudinal data of safety and efficacy of treatment outcomes in a range of diseases.
What are the new findings?
This paper describes the development and early data from a registry of glaucoma treatment outcomes.
How might these results change the focus of research or clinical practice?
The individual results provided to each clinician include comparative data with the registry as a whole and thereby drives improvements in clinical practice. The aggregated registry data are published providing clinicians with research outcome of different treatments over the medium to long term.
Introduction
The recent increase in new surgical treatment options for glaucoma has changed clinical care for many patients. Some procedures involve implanting devices, others use techniques to remove barriers to resistance in the outflow pathways. While there is a strong longitudinal evidence base for traditional surgeries such as trabeculectomy1 and tube shunt surgery,2 3 such evidence is not yet available for newer technologies. Well-designed randomised controlled pivotal trials of new devices have demonstrated short-term safety and efficacy4–6 but the 2-year follow-up window is relatively short in the context of the average glaucoma patient’s journey, and rarer but potentially serious complications may not be captured.
Furthermore, clinical trials determine whether new treatments work in highly controlled conditions for a highly selected group of patients that is unlikely to represent the general patient population with the disease.7 The internal validity of a clinical trial comes at a cost of external validity (or generalisability) of its results. It is therefore important to assess whether the results of pivotal clinical trials translate into similar patient outcomes in the general patient population under real-world conditions. These questions are best answered by population-based, post-marketing observational studies, which provide ongoing evaluation of both medical devices and drugs after regulatory approval. The importance of such observational studies has been reinforced with events such as the worldwide recall of the CyPass Micro-Stent because of safety concerns.8
Post-marketing observational studies complement prospective clinical trials by providing information on a real-world patient population undergoing a range of both established and new glaucoma surgeries. They may inform safety and efficacy in patient populations that were not originally studied and incorporate a broader set of outcome measures including patient preference, quality of life, long-term effectiveness and rare complications.
The Save Sight Registries use an efficient web-based data collection tool specifically to track the outcomes of ophthalmic treatments. This originally began with macular disease,9 which has now led to a wealth of data on long-term outcomes for macula treatments in routine clinical practice.10 11
The Fight Glaucoma Blindness! (FGB) Registry uses the same web-based software platform, which allows clinicians to rapidly audit their glaucoma surgical outcomes by anonymously comparing their outcomes with their peers. As the registry increases the number of eyes being followed, we will compare real-world outcomes against those reported in clinical trials. We will compare available devices regarding safety, long-term effectiveness and patient-reported outcomes. The careful baseline phenotype data collected will provide insight into personalised approaches to procedure selection in glaucoma.
In this paper, we describe the principles of design and development of the FGB tool and provide a summary of current patient characteristics.
Methods
Structure of the FGB Registry
FGB consists of a steering committee and a publishing committee. The steering committee is a representative group of glaucoma specialists from across Australia and New Zealand. This committee oversees refinement of data points, outcomes and efficacy reporting and review requests from users regarding modifications. The publishing committee reviews submissions for possible publications, allocates an authorship team for each publication, and ensures adherence with participation and publishing guidelines.
In this report, ‘users’ are those entering data with the software, whereas ‘participants’ are those whose outcomes are being tracked.
Software and system design
The high prevalence of glaucoma and glaucoma suspects often leads to very busy glaucoma practices and clinics. It was therefore critically important to reduce the load of data capture by clinicians. The choice of data fields was made through an iterative process designed to capture relevant outcomes with the smallest number of data fields. Demographic data and basic clinical data can be entered by clinical assistants, but the treating physician is required to personally confirm critical clinical points such as the glaucoma phenotype.
Quality assurance measures were included to ensure that only complete and within range data can be entered into the system. Data can be ‘saved’ if incomplete and then ‘finalised’ when complete. Finalisation starts a built-in validation process that ensures all mandatory fields have been completed and that values are within predetermined ranges. Only finalised data are available for analysis and reporting.
The software used in FGB is a series of modules interacting with a core system. FGB is part of the broader Save Sight Registries group, with modules tracking treatments for retinal conditions, corneal disease, ocular tumours and uveitis. The core system provides a range of basic functions, which are used by each module for patient data management.
The FGB software is a web-based application, which was developed using freely available software such as Apache, MySQL, PHP and RubyonRails. This approach allows the application to be run on different server operating systems. Data may be entered into FGB either through a web interface or by modifying electronic patient management systems to automatically transmit data to the project database. The latter significantly simplifies the process for the user through single-point data entry.
Participant-reported outcomes (PROs) are collected using the ‘Glaucoma Activity Limitation’12 score and the ‘Glaucoma Ocular Surface Disease Index’.13 Patients can complete these using a specially adapted application for tablet computers catering for the particular needs of the visually impaired. These data are transmitted directly to the FGB database for further analysis. Importantly, collecting PROs will facilitate studies to determine whether particular treatments differ in outcomes from the patient perspective.
Data anonymity and security
The FGB Project software is designed to provide maximum data security and anonymity. Users enter data using either an anonymised or pseudo-anonymised identifier, such as a hospital or practice medical record number. The system also stores the unique identifier, demographic data, such as the date of birth, sex and ethnicity. No other personal information is recorded. All data transmissions between the user and the server are encrypted using 128-bit encryption (Secure Sockets Layer). The data are stored and backed up on secure servers at the University of Sydney’s Information and Communication Technology Department.
Anonymity of users is closely guarded, providing confidence for clinicians to enter data completely, including complications. Each user can only see their own data with summary descriptive data from the entire registry cohort. Auditing is easily achieved by comparing their own outcomes with those of their peers in the registry. Users can withdraw their data from the registry at any time without providing a reason.
Funding
To date, the registry has been supported by private healthcare insurance companies, the Royal Australian and New Zealand College of Ophthalmologists, and industry. The parameters relating to the relationship with industry have developed over the last decade with the retinal registries, and the glaucoma registry follows the same guidelines. Industry never has access to any raw data, and industry staff do not participate in data entry. If there is a topic of mutual interest to both the publications committee and members of industry, a paper can be commissioned, but industry plays no role in the design, data extraction, analysis or writing of the manuscript. They are provided a copy of an advanced draft of the paper and can provide non-binding comments on the manuscript for the authorship team to consider. Ultimately, each authorship team has complete control of the data and the publication.
Data export
The Save Sight Registries software was designed in part as an audit and research tool, thereby making data export and analysis features important. Users can download their own data at any time as a text file in comma-separated variable format, to undertake their own analyses. The software also has a built-in statistical report providing measures of glaucoma treatment efficacy and safety. Figure 1 shows a sample output for a given treatment modality; the data are presented in graphical form according to the World Glaucoma Association guidelines for reporting of glaucoma surgical trials.14
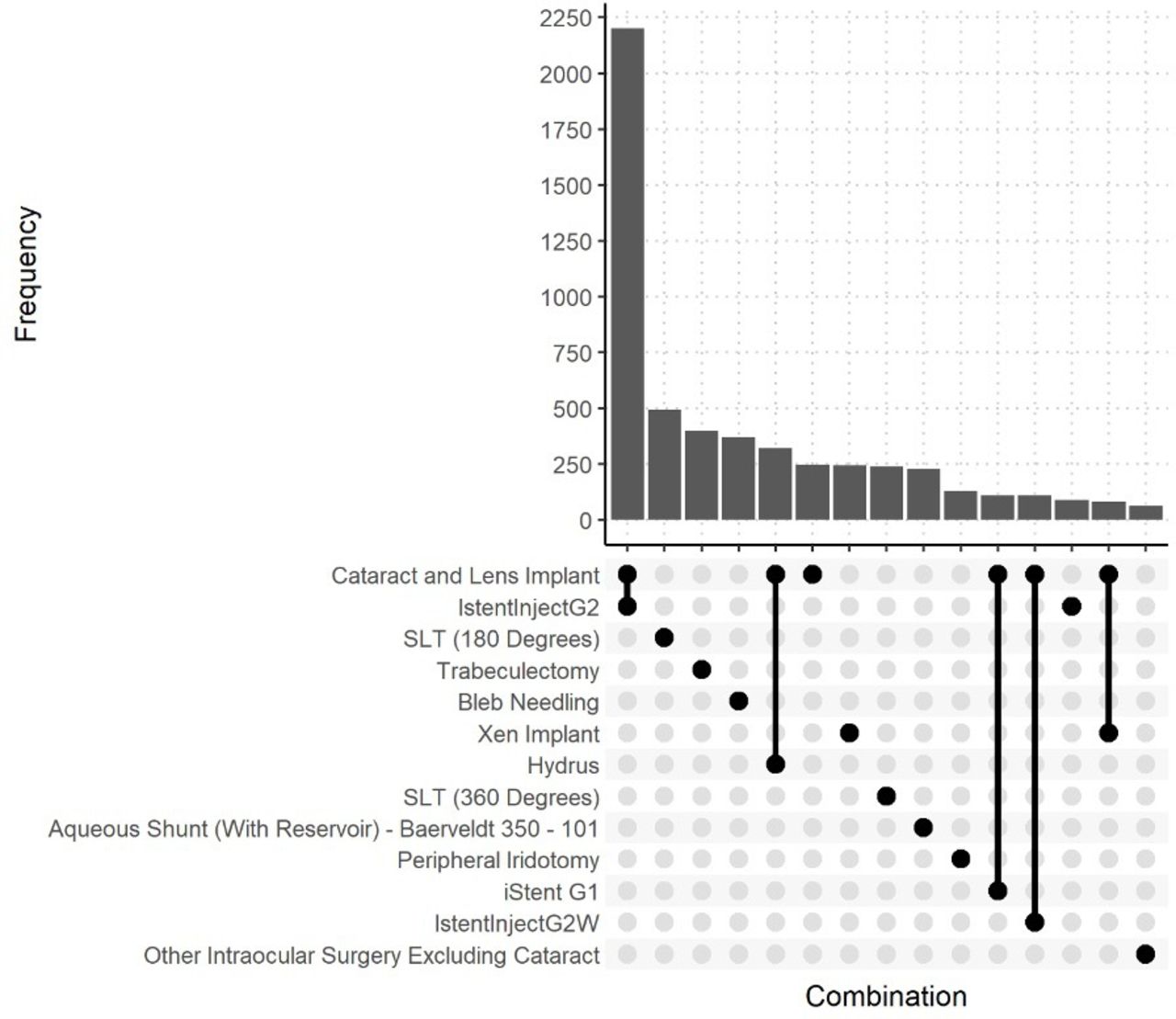
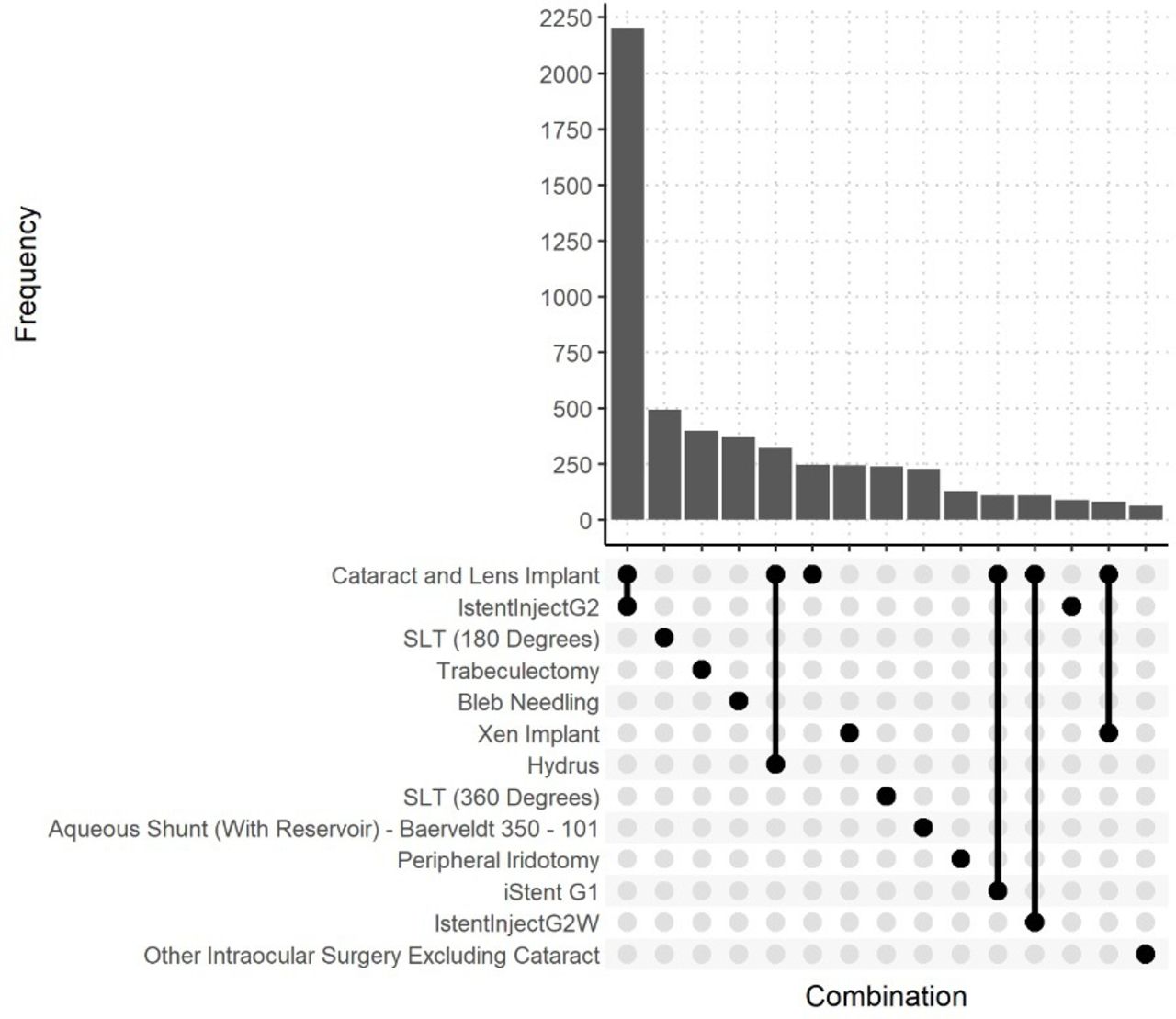
Upset plot of the 13 most common individual and combination procedures (saved and finalised) in the Fight Glaucoma Blindness! database.
Automated data import
Although the number of clinicians choosing to use the registry is already relatively high, the major impediment to more widespread uptake is the requirement for manual data entry. With increasing adoption of electronic medical records (EMRs), Save Sight Registries have developed a system to allow automated import of EMR data into the registry platform using CSV format. There are two forms of data that need to be captured. The first are structured fields collected directly within an EMR, for example, visual acuity and intraocular pressure (IOP). Exporting these data is relatively easy where these fields already exist within the EMR and a small amount of coding is required to ‘point’ the relevant data field from the EMR to the correct cell in the CSV file. Some alignment of fields is required in glaucoma procedure-specific fields such as a list of procedures, and a specific list of adverse events. Successful bulk import of data is already occurring in a number of centres for the retinal registries, and agreements are in place with a number of EMRs to undertake similar alignment of fields for FGB. The implementation of this should significantly increase uptake of registry use.
The second group of data points to be collected are those external to the EMR, for example, from optical coherence tomography (OCT) and visual field platforms. These data points can be transferred using DICOM protocols, if the relevant data point is DICOM compatible. For example, Zeiss products are DICOM compatible; Humphrey visual field (HVF) mean deviation (MD) and OCT retinal nerve fibre layer (RNFL) thickness can be automatically extracted using the format and imported into the registry. Heidelberg has some OCT parameters available to export through DICOM, but not RNFL thickness. This is in development, and on its release from Heidelberg, there would be minimal extra work for the registry software to accept these data points into FGB.
Statistical methods
We calculated descriptive statistics for participants at the index visit, defined as the first visit recorded in the FGB database. Continuous variables were summarised using the median and 25th and 75th percentiles (Q1, Q3). We summarised categorical variables as percentages. All analyses were performed with R V.4.0.0.15
Results
Data fields: the minimum data set
The number of data points captured in FGB was kept to a minimum, based on the finding from other registry modules that every additional data point slowed down data entry and significantly reduced registry uptake. The FGB steering committee used an iterative structured process to define a minimum data set for outcomes of glaucoma treatments. A literature review identified a large group of potential outcome measures for patients with glaucoma. These were presented to the steering committee, with each initial round identifying measures for which there was unanimous agreement for either inclusion or exclusion. Measures for which there was disagreement were then systematically addressed in further rounds, with the case for and against being presented. An effort was made to exclude measures where the data could be captured through other measures, for example, recording ‘hypotony maculopathy’ can be derived by a combination of numerical hypotony with IOP, and reduction in visual acuity through the best corrected visual acuity (BCVA) field. The iterative approach allowed members to re-evaluate the necessity for particular fields, until a unanimous consensus led to the final minimum data set.
The final data set for baseline and follow-up visits is shown in boxes 1 and 2, respectively. Some data points are numerical (eg, IOP, acuity), others have drop-down menus (eg, diagnosis, procedures) and some that are not performed at every clinical visit have the option of ‘not performed’ (OCT parameters and visual field MD). The option to enter an adverse event is available at every visit after a procedure, and multiple adverse events can be entered on each visit. There are no options for free text. The available diagnosis categories for phenotyping patients are shown in box 3. Patient-reported outcomes are optionally recorded with the registry supporting the ‘Glaucoma Activity Limitation’ score12 and the ‘Glaucoma Ocular Surface Disease Index’.13 There is also the option of a ‘treatment only’ visit, where no clinical data are required, which provides the opportunity to enter data for a surgical procedure on a separate day to a clinical assessment.
Mandatory fields for Fight Glaucoma Blindness! baseline visit
Baseline visit mandatory fields
Diagnosis (available fields in Box 3).
Ocular conditions (drop-down menu of options).
Previous surgery/laser? (drop-down menu of procedures).
Highest recorded intraocular pressure (IOP).
Lens status.
Refraction.
Central corneal thickness.
Anterior segment findings (drop-down menu of options).
Advanced glaucoma (mean deviation >−15 dB or central involvement).
Visual acuity.
Visual field mean deviation (not performed an option).
RNFL thickness global value (not performed an option).
RNFL thickness superior sector (not performed an option).
RNFL thickness inferior sector (not performed an option).
IOP.
Medical treatments (drop-down menu of medication types).
Procedures (drop-down menu of procedures).
Mandatory fields for Fight Glaucoma Blindness! follow-up visit
Follow-up required fields
Diagnosis change? (only prompts once per year).
Visual acuity.
Visual field mean deviation (not performed an option).
RNFL thickness global value (not performed an option).
RNFL thickness superior sector (not performed an option).
RNFL thickness inferior sector (not performed an option).
Intraocular pressure.
Medical treatments.
Procedures (drop-down menu of procedures).
Adverse events (only asked in eyes with a prior procedure).
Diagnosis categories available in Fight Glaucoma Blindness!
Procedure name
Ocular hypertension.
Primary open angle/normal tension glaucoma suspect.
Primary open-angle glaucoma.
Normal tension glaucoma.
Secondary open-angle glaucoma.
Primary congenital glaucoma.
Primary angle closure suspect.
Primary angle closure.
Primary angle closure glaucoma.
Secondary angle closure glaucoma.
Treatments available
For recording either prior procedures or a new procedure for a patient, a drop-down menu provides a comprehensive list of glaucoma treatment options. These include laser treatments such as selective laser trabeculoplasty and peripheral iridotomy, and traditional surgical procedures such as trabeculectomy and tube shunt surgery. All available minimally invasive glaucoma devices are represented, and any new procedures are added by FGB staff as required. Certain procedures trigger a secondary data field to become visible, for example, selecting trabeculectomy then requires stipulation of whether mitomicin-C was used, and at what concentration. Laser treatments can also be entered as procedures and audited in a similar way.
Medical treatments are captured in a separate field, each type of topical medication is individually recorded. To speed up data entry, a patient’s medications from the prior visit are automatically populated, the clinician then either confirms no change or can delete medications by clicking on one to remove it or add others from a drop-down menu.
Preliminary data
FGB was launched in November 2017. As of June 2021, there are 157 surgeons in 158 ophthalmology practices across Australia and New Zealand who are registered. These surgeons are tracking 5570 eyes in 3001 patients with 67 074 visits recorded. The median number of eyes per surgeon is 22 eyes with a range of 1–428. Patient baseline demographics are provided in online supplemental table 1.
Supplemental material
FGB now contains 5946 procedure events, the most common of which are shown in figure 2. Total numbers of the most common individual procedures are summarised in online supplemental table 2. While the most common procedure is cataract surgery, most of these surgeries were in combination with an angle-based MIGS device. Other cataract surgeries occurred during follow-up of other procedures, for example, a patient who required cataract surgery in the months-years following trabeculectomy.

{kind=link}
{kind=link}
Example of FGB personalised surgical report for a given procedure providing scatterplot outcomes and complete and qualified success. FGB, Fight Glaucoma Blindness!; IOP, intraocular pressure.
Discussion
FGB is an efficient web-based system that tracks glaucoma treatment outcomes for clinical audit, post-marketing observational studies and research. The design of a minimum, patient-centred data set balances the realities of busy clinics and data entry against the need for key high-quality data.
A key factor in success of registry uptake is to minimise the burden of data entry. While the baseline visit for patients with glaucoma is necessarily complex, follow-up visits are relatively brief. A follow-up visit collects visual acuity, IOP, medical treatment, visual field MD, OCT RNFL thickness (superior and inferior), whether any procedures were performed and whether there were any adverse events. Baseline visit data entry time varies with patient complexity but can often be completed in approximately 2 min. Follow-up visits can be completed in less than 30 s, while a compatible EMR with single-point data entry avoids the requirement for double data entry.
Registry-based studies provide valuable data on a number of levels. Individual surgeons are able to compare different procedure outcomes in their practice, for example, trabeculectomy outcomes against bleb-forming MIGS procedures. They can also compare outcomes with their peers, providing an important part of the audit cycle which is integral to improvement in practice.
Government and industry are able to identify how particular procedures are being used and what their effectiveness is in different patient populations in a real-world setting. The latter may also cost-effectively meet obligations for post-marketing surveillance. Such surveillance is becoming increasingly important in this current era of surgical innovation in glaucoma.
The search for safer and more effective surgical techniques comes with the risk of unintended harm. For example, after the Ex-Press shunt had obtained United States Food and Drug Administration approval, a number of cases of device-related erosion and endophthalmitis were reported.16 17 More recently, the CyPass Micro-Stent suprachoroidal device was found to be safe and effective in the 2-year pivotal trial,4 but the longer 5-year Compass-XT trial found that combined cataract plus CyPass patients had significantly higher rates of endothelial cell loss than the cataract alone control arm.8 Unless low probability adverse events are systematically tracked in large numbers of patients, such negative outcomes may not be identified. Systematic tracking of outcomes with a registry may allow earlier detection of a pattern of adverse events for a particular device or procedure. Furthermore, given the relatively long disease course for patients with glaucoma, registries can track medium to long-term ocular safety and efficacy outcomes in a much more cost-effective way than randomised trials.
Larger observational studies have been established in ophthalmology, including the IRIS Registry in the USA.18 IRIS has prespecified fields that are automatically extracted from the EMRs of participating clinicians. Relevant fields for glaucoma include diagnosis codes, visual acuity, IOP, cup to disc ratio and any procedures undertaken. IRIS provides a large data set on practice patterns, but the outcomes tracked are not tailored for patients with glaucoma. Also, this approach has the same limitations that come with an EMR, most importantly the possibility of missing relevant data. Other examples of registry data include the Swedish National Cataract Register,19 and the UK’s Royal College of Ophthalmologists’ National Ophthalmology Database Study of Cataract Surgery.20 These registries found stability or a reduction in complications and an increase in preoperative visual acuity over time. The Australian Corneal Graft Registry has been tracking the outcomes of corneal transplantation since 1986 and has collected information on approximately 35 000 corneal transplants, allowing analysis of outcomes and risk factors for success and failure.21
We have designed the registry with processes that militate against the biases that are inherent in observational studies. ‘Information bias’ is relevant where users may have a vested interest in misreporting an outcome. To avoid this, each user alone has access to their data: the investigator team only has access to aggregated data for analysis. Such privacy encourages complete and frank data entry, which also minimises ‘selection bias’. In particular, this relates to a risk of users only enrolling patients who have a low risk of complications, however the incentive for this is low when only the user has access to their data. One important driver of uptake is that clinicians are able to receive full audit points for continuing professional development by using the registry. A requirement of this is to enter at least 85% of whichever procedure they chose to audit, a further part of minimising selection bias. ‘Channelling bias’ may occur when particular devices are used in patients with different glaucoma subtypes or severities. A registry necessarily collects real-world data, so we have tried to capture the necessary data to control against this in the analysis. For example, we capture all prior treatments as well as glaucoma subtype and severity. Each patient is individually tracked allowing statistical adjustment for unit of analysis factors where two eyes of one patient are included. Finally, loss to follow-up can introduce bias if it is non-random. FGB allows clinicians to ‘refer’ patients to another clinician if the patient moves; the patient’s longitudinal data remain intact if the receiving clinician also uses the platform.
While randomised controlled trials and registries answer different clinical questions and are not comparable, the potential scale of data available from our registry is already in evidence. The iStent G2 FDA pivotal trial included 387 patients randomised to cataract surgery with iStent G2 implantation,5 and in the first 2 years of FGB we are already tracking over 1600 of the same combination procedure.
We have described here the development of a web-based registry for tracking glaucoma outcomes. The registry is being used initially to assess safety and efficacy of glaucoma surgical devices and laser, although the software allows clinicians to audit and track the outcomes of any glaucoma population within their practice. There is no cost to individual users. We have now developed a template for expansion into other countries, so that local data and analysis can be managed by local clinicians.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Quality assurance activities are those undertaken by a healthcare provider to evaluate and improve treatment outcomes. Clinical audit is one aspect of quality assurance and clinical registries are tools that facilitate audit. The information collected in FGB is also routinely collected by treating doctors and therefore is classified as a quality improvement activity.The use of data sets broader than an individual clinician to investigate practice patterns and treatment outcomes is considered research, so approval from the relevant Human Research Ethics Committee (HREC) is required. Local ethics approval is required by each public hospital where clinicians wish to participate and overarching national ethics approval has been obtained from the Royal Australian and New Zealand College of Ophthalmologists HREC for patients being treated in private practice.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors had equal participation in planning, conduct, reporting, conception and design, and analysis and interpretation of data. ML is the guarantor of the report and
accepts full responsibility for the work and the conduct of the study, had access to the data, and controlled the decision to publish.
Funding Funding was supported by the Royal Australian and New Zealand College of Ophthalmologists and an unrestricted educational grant from Glaukos.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.