Article Text

Abstract
Introduction Patients with heart failure (HF) are classically categorised by left ventricular ejection fraction (LVEF). Efforts to predict outcomes and response to specific therapy among LVEF-based groups may be suboptimal, in part due to the underlying heterogeneity within clinical HF phenotypes. A multidimensional characterisation of ambulatory patients with and without HF across LVEF groups is needed to better understand and manage patients with HF in a more precise manner.
Methods and analysis To date, the first cohort of 1313 out of total planned 3000 patients with and without HF has been enroled in this single-centre, longitudinal observational cohort study. Baseline and 1-year follow-up blood samples and clinical characteristics, the presence and duration of comorbidities, serial laboratory, echocardiographic data and images and therapy information will be obtained. HF diagnosis, aetiology of disease, symptom onset and clinical outcomes at 1 and 5 years will be adjudicated by a team of clinicians. Clinical outcomes of interest include all-cause mortality, cardiovascular mortality, all-cause hospitalisation, cardiovascular hospitalisation, HF hospitalisation, right-sided HF and acute kidney injury. Results from the Preserved versus Reduced Ejection Fraction Biomarker Registry and Precision Medicine Database for Ambulatory Patients with Heart Failure (PREFER-HF) trial will examine longitudinal clinical characteristics, proteomic, metabolomic, genomic and imaging data to better understand HF phenotypes, with the ultimate goal of improving precision medicine and clinical outcomes for patients with HF.
Ethics and dissemination Information gathered in this research will be published in peer-reviewed journals. Written informed consent for PREFER-HF was obtained from all participants. All study procedures were approved by the Mass General Brigham Institutional Review Board in Boston, Massachusetts and performed in accordance with the Declaration of Helsinki (Protocol Number: 2016P000339).
Trial registration number PREFER-HF ClinicalTrials.gov identifier: NCT03480633.
- heart failure
- research design
- computer simulation
- biomarkers
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Heart failure (HF) is a complex and heterogenous disease state with numerous aetiologies that portends a significant burden of morbidity and mortality on healthcare systems globally.1–3 There are currently 26 million patients worldwide carrying a diagnosis of HF, and these patients are categorised into two or three groups based on their left ventricular ejection fraction (LVEF): HF with preserved ejection fraction (HFpEF), HF with reduced ejection fraction (HFrEF) and the latest category, HF with midrange ejection fraction (HFmrEF). While there is an increasing number of medications proven to improve survival and hospitalisation for patients with HFrEF,4–9 there are currently no medications with a demonstrated mortality benefit in HFpEF.10–13 This is likely due to an incomplete understanding of HFpEF pathophysiology as well as the substantial heterogeneity of HFpEF phenotypes, where a one-size-fits-all strategy may be ineffective. As such, novel approaches are needed to improve our understanding and management of HF.
Many have suggested that multidimensional phenotyping is required to better define groups of patients with HF, especially those with HFpEF.14–19 Clinical registries offer a unique opportunity for phenotyping HF cohorts as they provide real-life observational evidence to assess short-term and long-term responses to medial therapy and evaluation of disease progression. Despite this, there are few contemporary registries that comprehensively evaluate ambulatory patients with HF based in the USA.
Herein we describe the Preserved versus Reduced Ejection Fraction Biomarker Registry and Precision Medicine Database for Ambulatory Patients with Heart Failure (PREFER-HF) study to comprehensively evaluate the relationship between clinical characteristics, genomic, proteomic and metabolomic data, imaging information and clinical outcomes in an ambulatory US cohort. The design, enrollment, end points, and statistical considerations for the PREFER-HF study are described.
Methods
Study design and setting
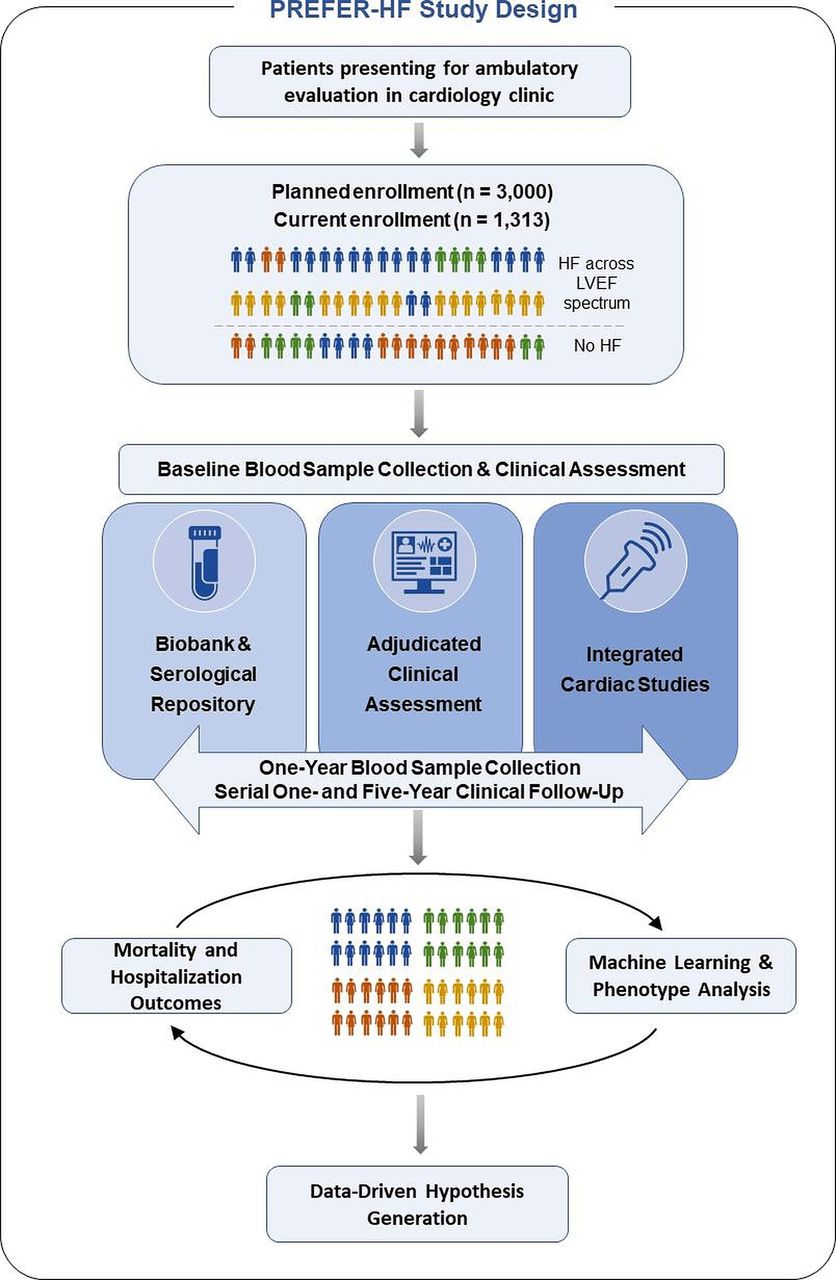
The PREFER-HF Study (ClinicalTrials.Gov, #NCT03480633) is a prospective, single-centre, investigator-initiated observational cohort study performed at the Massachusetts General Hospital (MGH), a large tertiary care academic medical centre in Boston, Massachusetts. All study procedures were approved by the Mass General Brigham Institutional Review Board and performed in accordance with the Declaration of Helsinki. A flow diagram of the PREFER-HF study design is shown in figure 1.

{kind=link}
Flow chart of patient enrollment and anticipated impact in the PREFER-HF study. HF, heart failure; LVEF, left ventricular ejection fraction; PREFER-HF, Preserved versus Reduced Ejection Fraction Biomarker Registry and Precision Medicine Database for Ambulatory Patients with Heart Failure.
Enrollment of up to 3000 study participants presenting to MGH for cardiovascular evaluation is planned. Recruitment began 7 April 2016 and, as of 1 April 2021, the first planned cohort of 1313 patients have been enroled and data collection is ongoing. Details regarding clinical diagnoses and year of diagnosis antecedent to HF onset, HF diagnosis presentation, enrollment and 1-year follow-up clinical information are obtained from review of the Mass General Brigham healthcare system electronic health record (EHR). Serial laboratory, cardiovascular imaging and procedural data will be obtained from Research Patient Data Registry (RPDR), a centralised clinical data warehouse that extracts clinical information across the Mass General Brigham hospital system at regular intervals. Natural language processing (NLP) will be used to extract information from RPDR. HF diagnosis presentation details were reviewed in EHR manually and adjudicated by a team of clinicians. Baseline blood samples and clinical information are collected at time of enrollment and cardiology clinic visit. A 1-year (±6 months) follow-up blood sample will be obtained, either through routine outpatient or research follow-up visit. Clinical outcomes at 1 and 5 years will be obtained and adjudicated.
Study objectives
The primary aim of the PREFER-HF study is to comprehensively characterise and evaluate clinical outcomes in ambulatory patients with and without HF by utilising detailed longitudinal clinical, genomic, proteomic, metabolomic and cardiovascular imaging data. Specific aims are detailed in box 1.
PREFER-HF study aims
HF characterisation
Compare baseline demographic, clinical, laboratory (including log-transformed cardiac biomarker concentrations) and echocardiographic parameters in classically defined LVEF-based HF groups and in control group (HF by three groups: HFpEF, HFmrEF and HFrEF and by two groups: HFpEF vs HFrEF).
Determine HF phenotypes in each of the HF groups from baseline demographic, clinical information and echocardiography data using machine learning (latent class regression and specific phenotype group assignment using model-based clustering) in the following groups: all HF, no HF, HFrEF, HFmrEF and HFpEF. Assess the role of LVEF in determining phenotype models.
Compare baseline clinical, laboratory (including cardiac biomarker concentrations) and imaging parameters in HF phenotypes.
Evaluate the change laboratory including biomarker concentrations and echocardiographic parameters from baseline to 1-year follow-up in HF groups.
In a subgroup of patients for whom gut metabolite data are available, examine the relationship between gut metabolites and baseline demographic, clinical, laboratory (including cardiac biomarker concentrations) and echocardiographic parameters including right ventricle data in HF and non-HF groups.
Examine genetic variants related to remodelling biomarkers and their associations with HF subtype by relating relevant single nucleotide polymorphisms associated with left ventricular remodelling pathways to HF subtypes.
HF prognosis
Evaluate the relationships between baseline demographic, clinical, laboratory (including cardiac biomarkers and gut metabolites) and echocardiographic parameters, and clinical endpoints at 1 and 5 years.
Examine the relationships between changes from baseline to 1-year follow-up in demographic, clinical, laboratory (including cardiac biomarkers) and echocardiographic parameters and clinical endpoints at 1 and 5 years.
Examine the relationship between HF phenotypes and clinical endpoints at 1 and 5 years.
Explore therapy interaction with HF phenotypes in clinical endpoints at 1 and 5 years.
Incident HF
In those who develop HF during follow-up period, determine predictors of incident HF using baseline, follow-up and change in demographic, clinical, laboratory (including cardiac biomarkers) and echocardiographic parameters.
Patient eligibility and enrollment
Patients 18 years of age and older evaluated in the outpatient cardiology clinic at MGH will be enroled. Patients are enroled if they provided informed consent. Patients on haemodialysis are excluded. HF was defined as a clinical syndrome of HF with supporting evidence by laboratory, echocardiographic, invasive haemodynamics or exercise haemodynamic studies as defined in table 1. Enroled patients are given an opt-in choice for genetic testing. Those who decline genetic testing are still included for all other aspects of the study. Patients with HF regardless of LVEF are enroled. LVEF at the time of HF diagnosis will be used to assign patients to one of the LVEF-based HF groups with the understanding that (1) LVEF may change over time for an individual patient while exhibiting clinical HF and (2) guideline-recommended LVEF cut-off values for classically defined HF groups may evolve over time.1 20 21 Patients with HF are initially assigned an LVEF-based group at study enrollment according to the following definition: LVEF ≥50% for HFpEF and LVEF <50% for HFrEF. Patients are defined as HFpEF with an LVEF ≥50%, as is precedent in both the 2013 American College of Cardiology/American Heart Association guidelines that were available at the time of study design prior to 2015,1 and which has been continually reflected in the most recent 2021 Universal Definition and Classification of Heart Failure.21 Patients were generally classified as HFrEF with an LVEF <50% at trial enrollment to broadly capture a group of patients who do not have HFpEF. In part, this broad definition was to account for the constant evolution in HF guidelines, which more recently have included a new category of HF for patients with LVEF 41%–49% defined as HFmrEF. Irrespective of the assigned category at trial enrollment, explicit data on LVEF are recorded so that patients with HF can be assessed across all definitions of HF, as well as irrespective of LVEF. Patients without a history of clinical HF were enroled to a control group.
Patient eligibility criteria for PREFER-HF
Blood sample acquisition
A 50 mL of blood sample was collected by venipuncture for the isolation of plasma (potassium EDTA Vacutainer), serum (serum Vacutainer) and DNA. Blood samples were centrifuged for 15 min at 1200 g. Plasma and serum were aliquoted (500 µL volume) and frozen at −80°C to allow additional testing of biomarkers. Buffy coat was aliquoted (2.5 mL) using the same blood sample for DNA extraction. Serial measurement of cardiac remodelling biomarkers including standard prognostic biomarkers include N-terminal pro-B-type peptide (NT-proBNP), high-sensitivity troponin T, novel biomarkers such as insulin-like growth factor-binding protein 7 (IGFBP7) and growth-differentiation factor 15 (GDF-15), and circulating gut metabolites including plasma trimethylamine N-oxide (TMAO), choline, betaine and carnitine. At follow-up visits, an additional 50 mL of blood sample will be collected and processed to similar specifications.
Clinical characteristics and adjudicated HF history
Detailed baseline clinical visit data, medical history, clinical events and end points for each study subject will be obtained (online supplemental appendix A). Medical history, cardiovascular history including HF onset and endpoints will be independently adjudicated by a panel of physicians (cardiologists and internal medicine physicians) according to prespecified definitions. For the assessment of HF diagnosis, clinical events and endpoints, adjudicating physicians will be provided with all available information through the integrated EHR or clinical history. To validate the adjudication process, 10% of cases will be randomly rereviewed by a different clinician (other than the original adjudicator). If there is a discordant finding, the case will be discussed as a group and consensus achieved.
Supplemental material
Uniquely, the presence and duration of symptoms and medical comorbidities prior to the diagnosis of HF will be temporally adjudicated. Moreover, detailed information with respect to primary and contributing (secondary and tertiary) HF aetiology will be clinically adjudicated. Candidate primary and contributing HF aetiologies will include ischaemic, valvular, hypertensive, tachycardia-mediated, restrictive heart disease, infiltrative heart disease (including amyloidosis), dilated cardiomyopathy, hypertrophic cardiomyopathy, eosinophilic, stress-induced, toxin-induced (including alcohol and chemoradiation), high-output HF, peripartum cardiomyopathy, congenial, idiopathic and iatrogenic causes. Such data are to be described further by the clinical history and physical examination recorded at the time of diagnosis and at the time of enrollment. Additionally, documentation of New York Heart Association Class as well as signs/symptoms of HF including dyspnoea on exertion, paroxysmal nocturnal dyspnoea, orthopnoea, chest discomfort, fatigue, loss of appetite, weight loss, lower extremity oedema, rales, jugular venous distention, S3 gallop and hepatojugular reflex will be captured.
Cardiovascular procedural and imaging data
All relevant and available cardiovascular procedural and multimodality imaging data will be collected via RPDR and available in both text-based reports and table-based data made possible through an integrated EHR. These data will include electrocardiograms, chest radiography, echocardiography, stress testing, cardiac MRI (cMRI), right heart catheterisations, coronary angiograms, pyrophosphate scans and cardiopulmonary exercise testing. NLP will be used to extract data from text-based cardiovascular procedural and imaging reports. In addition, general information and clinical diagnoses from these reports and clinic notes will be manually extracted and entered into a database by a clinical adjudication committee. Echocardiographic data will be reviewed. Uniquely, all echocardiographic images will be directly available for assessment both by the clinical adjudication team as well as established and novel machine learning algorithms to best characterise the temporal dynamics of echocardiographic parameters. Routine laboratory measurements and medication data will also be collected.
Clinical end points
The primary clinical end point for PREFER-HF is time to a composite end point of all-cause mortality and HF hospitalisations (box 2). The secondary clinical end point for PREFER-HF is the time to presence of the following events: all-cause mortality, cardiovascular mortality, all-cause hospitalisation, cardiovascular hospitalisation, HF hospitalisation and acute kidney injury and will be assessed up to 5 years after the study closure. EHR documentation, the Social Security Death Index, postings of death announcements or follow-up with the patient and/or their primary physician will be used to confirm vital status.
End points of the PREFER-HF study
Primary end point
1. Time to composite end point of all-cause mortality and HF hospitalisations.
Secondary end point
1. Time to first event:
All-cause mortality
Cardiovascular mortality
HF hospitalisation
Acute kidney injury
2. Presence of event:
All-cause mortality
Cardiovascular mortality
All-cause hospitalisation
HF hospitalisation
Cardiovascular hospitalisation
Right-sided HF
Acute kidney injury
Powering and proposed statistical analysis
The study completed enrollment of a total 1313 patients in the first cohort which ensures an analysable sample of 1050 patients accounting for an assumed attrition and missing data rate of approximately 20%. Given the lack of validated data from which to calculate incidence and outcomes within phenotypes, a power calculation was not performed. A convenience sampling technique has been used, recognising that for some variables the PREFER-HF study will be significantly powered, but for other outcomes may be underpowered. Biomarker and baseline echocardiographic variables should be collected in all participants and thus available for analysis, while other cardiovascular procedures and imaging studies such as cardiac catheterisation, cMRI and stress tests will vary in number among participants and thus were obtained in a convenience sampling manner. The planned enrollment total is 3000 patients with approximately two-third of patients having HF, regardless of LVEF, and approximately one-third non-HF controls.
Univariable analysis as well as Pearson correlation coefficients, corresponding two-sided 95% CIs and p values will be calculated to explore the association between variables (log-transformed values for non-parametric variables). P values<0.05 will be deemed significant. Pearson correlation coefficients, corresponding two-sided 95% CI and p values will be calculated for each parameter. These calculations will be performed for both baseline and follow-up visit as well as change from baseline to follow-up (relative and absolute change) data. χ2 test will be used for the categorical variables and Student’s t-test, Mann Whitney U test or Kruskal-Wallis will be used as appropriate for continuous variables in comparison. Repeated measures will be analysed using Wilcoxon tests.
Candidate variables will be used to build a predictive multivariable model of time to the primary and secondary end point. Univariable screening will first be conducted with a retention value of p=0.10. These candidate variables will then be entered into a multivariable model using forward stepwise logistic or linear regression to identify independent predictors of the outcome of interest. Collinearity will be assessed, and non-parametric continuous variables will be transformed to fit a normal curve. Verification of goodness of fit will be confirmed with the Hosmer-Leme show test. ORs for outcome measures of interest will be generated and expressed with 95% CI, and Cox proportional hazards will be used to generate hazard ratios.
The role of biomarker and metabolite levels will be explored in the described models by including each as a continuous variable with absolute and relative chance in values expressed from baseline to follow-up visit. They will also be assessed as binomial categorical variables above and below the receiver operator curve optimised to a threshold or known diagnostic cut-off value for each biomarker or metabolite of interest. Net reclassification improvement and integrated discrimination improvement analyses will be performed to compare prediction of the desired outcome by including biomarker and metabolite levels.
Latent class analysis will be used to determine clusters of patient phenotypes, derived using maximum-likelihood estimation to identify the most common patterns of candidate variables. Data for the latent class model will include presence of and temporality of medical and cardiovascular history, echocardiographic measures and biomarkers. Cluster selection criteria will be determined using Bayesian information Criterion in determining the optimum number of clusters in groups of interest.
Discussion
We describe the design and rationale of the PREFER-HF study, a prospective single-centre observational cohort study which has enrolled 1313 ambulatory patients to date in its first cohort. This approach integrates clinical data with proteomic, genomic, metabolomic and multimodal imaging data to determine HF phenotypes and enhance HF prediction and prognostication. In our study, performed at a large academic institution in the USA, we have enroled patients with HF across a broad spectrum of LVEF, as well as a comparator group of patients without HF but receiving care in a cardiology clinic, who are intended to be a representative sample of ambulatory patients in whom routine biomarker assessment may be considered and risk for incident HF may be elevated due to demographics and comorbidities.
Few bioregistries have comprehensively and longitudinally assessed biomarker dynamics in HF to determine their prognostic value. The The Biology Study to Tailored Treatment in Chronic Heart Failure (BIOSTAT-CHF) study is one such registry in which investigators prospectively enroled patients from across Europe from 2010 to 2012 and modelled predictors of HF mortality and hospitalisation based on a combination of genetic, biomarker and phenotypic data.22 23 The results of this bioregistry highlight the prognostic utility of such a study design; however, PREFER-HF stands apart in a few advantageous ways.
First, PREFER-HF addresses prognostication in a group of US patients strictly in the ambulatory setting without prerequisite therapy requirements, allowing for a broader group of patients with HF. This is in contrast to the European BIOSTAT-CHF registry that included both inpatient and outpatient settings and required patients to be on daily diuretic therapy of at least furosemide 40 mg daily, suboptimal guideline-directed medical therapy, and to have worsening signs and/or symptoms.24 As a more contemporary study, PREFER-HF aims to enrol a larger proportion of patients on newer HF therapies such as sodium-glucose cotransporter 2 inhibitors and angiotensin receptor/neprilysin inhibitors (ARNIs).
Second, it is among the first comprehensive bioregistries to not only enrol patients with HF, but also a control group of ambulatory patients without HF who presented for routine cardiac evaluation. Inclusion of this group allows for comparability and affords the opportunity for longitudinal follow-up to evaluate predictors of incident HF onset. Furthermore, the serial lab work and biomarker measurements along with direct assessment of echocardiographic images will allow for enhanced assessment and understanding of remodelling trajectories over time and how such dynamics relate to clinical outcomes.
Third, PREFER-HF is favourably designed to utilise cluster analyses to generate hypotheses regarding plausible HF phenotypes that are not biased by the traditional LVEF-based stratification. It is increasingly recognised that HF classification by a single LVEF alone may be insufficient and hinder the understanding of HF risk stratification and treatment options, especially among patients with HFpEF in which clinical trials have not demonstrated any proven therapies to reduce mortality.25–27 In fact, LVEF thresholds for HF utilised in clinical trials and guidelines are highly variable and have changed over the years.21 28 Meta-analyses of beta-blocker, mineralocorticoid antagonist and ARNI clinical trials across the LVEF spectrum have revealed a more nuanced picture of benefit.29–32 Furthermore, several studies have demonstrated dynamic changes in EF from over time.33–36 These computational analyses will be enhanced by comparison to a group of individuals without HF and may aid prediction of HF prognostication regarding clinical outcomes and response to treatment in patients with HF. In this way, this study may improve the understanding of vulnerable patients with HF and potentially identify those that may be targeted for existing and novel treatments in general clinical practice.
The PREFER-HF registry will also allow for an exposure analysis to enhance efforts to identify incident HF in a timely fashion. The medical history documented in PREFER-HF is particularly structured to document the time-of-onset for many diseases within the medical history. Consideration of temporal data and duration of comorbidity exposure has not been previously studied in this way and will support the secondary aim to examine the relationship between baseline and/or follow-up biomarker concentrations and time to first events. The temporal data ascertained will also inform unsupervised machine learning models. While such methods have gained popularity and been increasingly applied to patients with HF to determine phenotypic differences among patients, many prior computational approaches have been limited to LVEF-based categories of patients with HF and have not been assessed comprehensively across an ambulatory population of patients with HF.14 16 19 37–39 Such methods will be important to apply and compare across other ongoing HF registry studies, including those patients in the global congestive heart failure,40 the Swedish-based Preserved and Reduced Ejection Fraction Epidemiological Regional Study (PREFERS Stockholm)41 and a smaller registry based in the UK.42
The PREFER-HF bioregistry will allow for evaluation of established biomarkers, such as BNP, NT-proBNP and troponin T or I, as well as emerging biomarkers including IGFBP7 and GDF-15. IGFBP7 is a protein member of the senescence-associated secretome which inhibits cell proliferation through G1 phase cell cycle arrest in states of cell injury and abnormal growth.43 44 Among patients with HF, it is thought that IGFBP7 may be a marker of impaired diastolic dysfunction with prognostic utility.43 45 Similarly, GDF-15 is a circulating biomarker which is increasingly shown to demonstrate sex-specific prognostic value among patients with cardiovascular disease and HF.46 47 Additionally, there has been increasing interest in the role intestinal microbiota play in regulating host metabolic pathways and disease manifestation.48 49 Theories regarding gut-oedema from HF and metabolomic changes have been suggested. One such gut metabolite, TMAO, has fostered significant interest given its association with increased risk for adverse cardiovascular outcomes50–53 and mortality in patients with HF.54 Characterisation of metabolites such as TMAO and others may be of significant importance in HF detection, characterisation, prognosis and treatment. This registry will allow for the longitudinal evaluation of known and novel biomarkers with the goal of establishing multiplex biomarker panels for HF prediction and disease progression.
The design and methods of PREFER-HF should be considered within the context of its limitations. First, the observational nature of this cohort limits our ability to infer causality. Second, the generalisability of this cohort of patients should be considered when applying the findings outside of this single-centre, tertiary academic centre in which the patient cohort may be limited to regional differences in racial, ethnic and socioeconomic diversity. In the future, the PREFER-HF study could benefit from partnership with other institutions and organisations to expand into a multicentre cohort. Additionally, the use of the EHR to retrospectively assess data on medical comorbidities may be incomplete. Finally, while the candidacy of identified biomarkers may prove insightful for elucidating pathophysiological differences, they may not translate to routine clinical use and further research needed.
Conclusions
The PREFER-HF study is a multidimensional and comprehensive evaluation of ambulatory patients with HF. This detailed bioclinical registry will capture the HF clinical presentation; comorbid illnesses and their temporal relation to HF onset; laboratory assessments, including proteomic, metabolomic and genomic data; cardiovascular imaging and procedure reports enhanced by ascertainment of direct echocardiographic images; and outcome data among patients across a broad spectrum of HF and those without HF. The synthesis of data generated from this trial will inform precision medicine and computational approaches to improve disease monitoring and clinical decision-making in the care of ambulatory patients with HF.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Written informed consent for PREFER-HF was obtained from all participants. All study procedures were approved by the Mass General Brigham Institutional Review Board in Boston, Massachusetts and performed in accordance with the Declaration of Helsinki (protocol number: 2016P000339).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
AA and AN are joint first authors.
Twitter @asnguonly
AA and AN contributed equally.
Contributors AA, AH, and HKG complemented the study concept and wrote the first draft of the manuscript. HKG and JLJ developed the study idea and concept. AB, KJB, RFC, DD, NF, MJ, DK, MM, CT, KW, MW, DAZ and JLJ provided critical and iterative revisions of the manuscript.
Funding This work was in part supported by Roche Diagnostics, Inc; the sponsor had no involvement in study design, collection, analysis and interpretation of data, in the writing of the report and in the decision to submit the article for publication. Dr Gaggin is supported in part by the Clark Fund for Cardiac Research Innovation.
Competing interests JLJ is a Trustee of the American College of Cardiology, has received grant support from Roche Diagnostics, Novartis Pharmaceuticals and Abbott Diagnostics, consulting income from Abbott Diagnostics, Janssen, Novartis and Roche Diagnostics, and participates in clinical endpoint committees/data safety monitoring boards for Abbott, AbbVie, Amgen, Bayer and Takeda. HKG has received research grant support from Roche Diagnostics, Jana Care, Ortho Clinical, Novartis, Pfizer, Alnylam, Akcea; consulting income from Amgen, Eko, Merck, Roche Diagnostics, Radiometer, Pfizer; Stock ownership for Eko; Research payments for clinical endpoint committees from Radiometer. She has also received research payment for clinical endpoint committees from Baim Institute for Clinical Research for Abbott, Siemens and Beckman Coulter.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.