
Abstract
The assessment of causality is fundamental to epidemiology and biomedical sciences. One well-known approach to distinguishing causal from noncausal explanations is the nine Bradford Hill viewpoints. A recent article in this journal revisited the viewpoints to incorporate developments in causal thinking, suggesting that the sufficient cause model is useful in elucidating the theoretical underpinning of the first of the nine viewpoints—strength of association. In this article, we discuss how to discern the causal mechanisms of interest in the sufficient cause model, which pays closer attention to the relationship between the sufficient cause model and the Bradford Hill viewpoints. To this end, we explicate the link between the sufficient cause model and the potential-outcome model, both of which have become the cornerstone of causal thinking in epidemiology and biomedicine. A clearer understanding of the link between the two models provides significant implications for interpretation of the observed risks in the subpopulations defined by exposure and confounder. We also show that the concept of potential completion times of sufficient causes is useful to fully discerning completed sufficient causes, which leads us to pay closer attention to the fourth of the nine Bradford Hill viewpoints—temporality. Decades after its introduction, the sufficient cause model may be vaguely understood and thus implicitly used under unreasonably strict assumptions. To strengthen our assessment in the face of multifactorial causality, it is significant to carefully scrutinize the observed associations in a complementary manner, using the sufficient cause model as well as its relevant causal models.


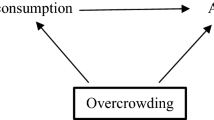
source population is selected for the matched study (1 = selected, 0 = not selected). The square around S = 1 indicates that the analysis is conditional on having been selected. Although the variables C and A are d-connected via two paths, C → A and C → S=1 ← A, these variables are independent by design (i.e., C ⫫ A|S = 1). In other words, the two paths “unfaithfully” cancel each other exactly
Similar content being viewed by others

Availability of data and materials
Not applicable.
Code availability
Not applicable.
References
Rothman KJ, Greenland S. Causation and causal inference in epidemiology. Am J Public Health. 2005;95(Suppl 1):S144–50.
Lucas RM, McMichael AJ. Association or causation: evaluating links between “environment and disease.” Bull World Health Organ. 2005;83:792–5.
Morabia A. Hume, Mill, Hill, and the sui generis epidemiologic approach to causal inference. Am J Epidemiol. 2013;178:1526–32.
Olsen J, Jensen UJ. Causal criteria: time has come for a revision. Eur J Epidemiol. 2019;34:537–41.
VanderWeele TJ, Lash TL, Rothman KJ, et al. Causal inference and scientific reasoning. In: Lash TL, VanderWeele TJ, Haneuse S, et al., editors. Modern epidemiology. 4th ed. Philadelphia: Wolters Kluwer; 2021. p. 17–31.
Hill AB. The environment and disease: association or causation? Proc R Soc Med. 1965;58:295–300.
Rothman KJ, Lash TL, Haneuse S, et al. The scope of epidemiology. In: Lash TL, VanderWeele TJ, Haneuse S, et al., editors. Modern epidemiology. 4th ed. Philadelphia: Wolters Kluwer; 2021. p. 3–15.
Shimonovich M, Pearce A, Thomson H, et al. Assessing causality in epidemiology: revisiting Bradford Hill to incorporate developments in causal thinking. Eur J Epidemiol. 2021. https://doi.org/10.1007/s10654-020-00703-7.
Greenland S, Pearl J, Robins JM. Causal diagrams for epidemiologic research. Epidemiology. 1999;10:37–48.
Glymour MM. Using causal diagrams to understand common problems in social epidemiology. In: Oakes JM, Kaufman JS, editors. Methods in social epidemiology. 2nd ed. San Francisco: Jossey-Bass; 2017. p. 458–92.
Suzuki E, Shinozaki T, Yamamoto E. Causal diagrams: pitfalls and tips. J Epidemiol. 2020;30:153–62.
Rothman KJ. Causes. Am J Epidemiol. 1976;104:587–92.
Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336:924–6.
Greenland S, Poole C. Invariants and noninvariants in the concept of interdependent effects. Scand J Work Environ Health. 1988;14:125–9.
Flanders WD. On the relationship of sufficient component cause models with potential outcome (counterfactual) models. Eur J Epidemiol. 2006;21:847–53.
VanderWeele TJ, Hernán MA. From counterfactuals to sufficient component causes and vice versa. Eur J Epidemiol. 2006;21:855–8.
VanderWeele TJ, Robins JM. Empirical and counterfactual conditions for sufficient cause interactions. Biometrika. 2008;95:49–61.
Suzuki E, Yamamoto E, Tsuda T. On the link between sufficient-cause model and potential-outcome model. Epidemiology. 2011;22:131–2.
VanderWeele TJ, Richardson TS. General theory for interactions in sufficient cause models with dichotomous exposures. Ann Stat. 2012;40:2128–61.
Suzuki E, Mitsuhashi T, Tsuda T, et al. A counterfactual approach to bias and effect modification in terms of response types. BMC Med Res Methodol. 2013;13:101.
Cole SR, Frangakis CE. The consistency statement in causal inference: a definition or an assumption? Epidemiology. 2009;20:3–5.
VanderWeele TJ. Concerning the consistency assumption in causal inference. Epidemiology. 2009;20:880–3.
VanderWeele TJ, Robins JM. The identification of synergism in the sufficient-component-cause framework. Epidemiology. 2007;18:329–39.
Mansournia MA, Hernán MA, Greenland S. Matched designs and causal diagrams. Int J Epidemiol. 2013;42:860–9.
Rubin DB. Estimating causal effects of treatments in randomized and nonrandomized studies. J Educ Psychol. 1974;66:688–701.
Greenland S, Robins JM. Identifiability, exchangeability, and epidemiological confounding. Int J Epidemiol. 1986;15:413–9.
Kaufman JS, Poole C. Looking back on “causal thinking in the health sciences.” Annu Rev Public Health. 2000;21:101–19.
Little RJ, Rubin DB. Causal effects in clinical and epidemiological studies via potential outcomes: concepts and analytical approaches. Annu Rev Public Health. 2000;21:121–45.
Suzuki E, VanderWeele TJ. Mechanisms and uncertainty in randomized controlled trials: a commentary on Deaton and Cartwright. Soc Sci Med. 2018;210:83–5.
VanderWeele TJ, Knol MJ. Remarks on antagonism. Am J Epidemiol. 2011;173:1140–7.
Lin SH, Huang YT, Yang HI. On identification of agonistic interaction: Hepatitis B and C interaction on hepatocellular carcinoma. Stat Med. 2019;38:2467–76.
Lin JH, Lin KI, Lee WC, et al. Stochastic approach for mechanistic interaction under longitudinal studies with noninformative right censoring. Stat Med. 2020;39:114–28.
Huang YT, Tai AS, Chou MY, et al. Six-way decomposition of causal effects: unifying mediation and mechanistic interaction. Stat Med. 2020;39:4051–68.
Tai AS, Huang YT, Lee WC, et al. Conceptualization of agonistic interaction in a marginal sufficient component cause model: an alternative interpretation for subadditive interaction. J Chin Stat Assoc. 2020;58:168–98.
Suzuki E, Yamamoto E, Tsuda T. On the relations between excess fraction, attributable fraction, and etiologic fraction. Am J Epidemiol. 2012;175:567–75.
VanderWeele TJ. Attributable fractions for sufficient cause interactions. Int J Biostat. 2010;6:5.
Suzuki E, Tsuda T, Yamamoto E. Covariate balance for no confounding in the sufficient-cause model. Ann Epidemiol. 2018;28:48–53.
Suzuki E. Time changes, so do people. Soc Sci Med. 2012;75:452–6.
Greenland S, Brumback B. An overview of relations among causal modelling methods. Int J Epidemiol. 2002;31:1030–7.
Suzuki E. Generalized causal measure: the beauty lies in its generality. Epidemiology. 2015;26:490–5.
VanderWeele TJ. Sufficient cause interactions and statistical interactions. Epidemiology. 2009;20:6–13.
VanderWeele TJ. A word and that to which it once referred: assessing “biologic” interaction. Epidemiology. 2011;22:612–3.
Hafeman DM. A sufficient cause based approach to the assessment of mediation. Eur J Epidemiol. 2008;23:711–21.
VanderWeele TJ. Mediation and mechanism. Eur J Epidemiol. 2009;24:217–24.
Suzuki E, Yamamoto E, Tsuda T. Identification of operating mediation and mechanism in the sufficient-component cause framework. Eur J Epidemiol. 2011;26:347–57.
Greenland S, Robins JM. Conceptual problems in the definition and interpretation of attributable fractions. Am J Epidemiol. 1988;128:1185–97.
Suzuki E, Yamamoto E. Re: A graphical description of partial exchangeability. Epidemiology. 2021;32:e7–9.
VanderWeele TJ, Robins JM. Directed acyclic graphs, sufficient causes, and the properties of conditioning on a common effect. Am J Epidemiol. 2007;166:1096–104.
VanderWeele TJ, Robins JM. Minimal sufficient causation and directed acyclic graphs. Ann Stat. 2009;37:1437–65.
Mackie JL. Causes and conditions. Am Philos Q. 1965;2:245–64.
VanderWeele TJ. Hill’s causal considerations and the potential outcomes framework. Observ Stud. 2020;6:47–54.
Acknowledgements
We thank Edanz Group (https://en-author-services.edanz.com/) for editing a draft of this manuscript.
Funding
ES is supported by the Japan Society for the Promotion of Science (JSPS KAKENHI Grant Numbers, JP20K10471, JP18K10104, and JP20K10499). Funding sources had no involvement in study design, the collection, analysis and interpretation of data, the writing of the report, and the decision to submit the article for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
This is a theoretical study, and no ethical approval is required.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
In terms of the potential completion times of sufficient causes, Assumptions 1 and 2 can be algebraically rewritten as follows:
Assumption 1
Assumption 2
These clearly show that Assumption 2 is less strict than Assumption 1. As mentioned in the text, Assumption 3 is less strict than Assumption 2, which can be more readily seen by rewriting Assumption 3 as follows:
Assumption 3
Rights and permissions
About this article

Cite this article
Suzuki, E., Yamamoto, E. Strength in causality: discerning causal mechanisms in the sufficient cause model. Eur J Epidemiol 36, 899–908 (2021). https://doi.org/10.1007/s10654-021-00798-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-021-00798-6