
Application of Machine Learning to Electroencephalography for the Diagnosis of Primary Progressive Aphasia: A Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. EEG Acquisition
2.3. Preprocessing
- 1.
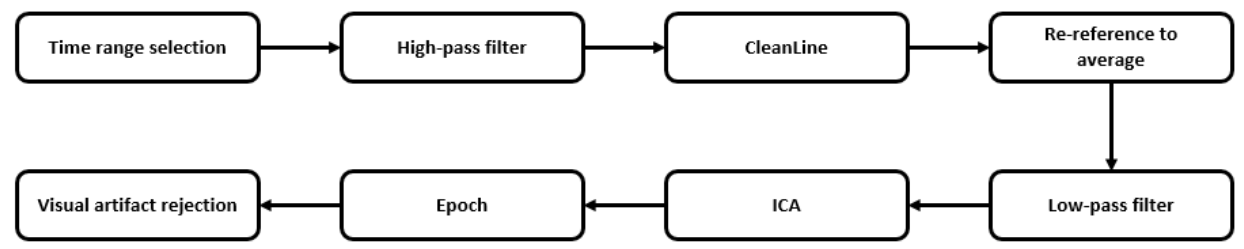
- Time ranges selection. Original signals are too long to be analyzed and can contain some additional noise, so we manually selected those time ranges with higher quality in the signal representation to get the most accurate and clean signal. This process also considered the labels recorded during the EEG acquisition and clinical assessment, which notify about the state of the patient, unexpected events, or activities that could impact on the signal.
- 2.
- High-pass filtering at 1 Hz. This filter was applied to remove baseline noise, remove noise introduced by sweating, and prepare the signal for ICA analysis.
- 3.
- Apply CleanLine process with the following configuration: 10 Hz of bandwidth at 50 Hz line frequency. This preprocessing step removes line noise and related harmonics from each one of the scalp channels using a novel approach, as described in [36]. For that purpose, and for each sliding window over the original data, a multi-taper FFT is applied to transform the signal to the frequency domain; after that, the complex amplitude of the desired frequency is extracted. With that information, a noise signal in the frequency domain is generated and, finally, the time-domain associated noise signal that needs to be extracted from the original one is also created.
- 4.
- Re-reference data to average. This is the most effective and easiest way to re-reference EEG data because it establishes that the summed up power across the scalp topography should sum zero. In other words, we removed the mean over all scalp channels to every single channel to make sure that all channels contribute with the same weight.
- 5.
- Low pass filter at 40 Hz. This step was applied in order to remove any possible undesired high-frequency signal that was not removed by CleanLine. Although other investigations are looking for biomarkers in higher frequency ranges of EEG signal, most recent research works are focusing in lower frequency ranges [37]. For simplicity of our analysis and control of error sources, we have limited our work to the lower frequency bands.
- 6.
- To apply ICA (Independent Component Analysis) to the signal. This method is a linear decomposition technique which aims to find the source signals from a set of mixed signals, as it occurs with EEG. Unlike PCA (Principal Component Analysis), ICA tries to retrieve those original signals that are maximally statistical independent in just one domain [38].
- 7.
- To epoch data into windows of duration equal to one second without overlapping.
- 8.
- Visual artifact rejection of epochs. As a final step, we reviewed manually all signals and all their epochs looking for artefacts or undesired signal events.
2.4. Quantitative EEG
- Delta from 1–4 Hz.
- Ipsilon from 4–8 Hz.
- Alpha from 8–14 Hz.
- Beta from 14–30 Hz.
- Gamma from 30–45 Hz.
- OoB (out of bag) for frequencies higher than 45 Hz.
2.5. Wavelet Transformation
- Subband 1 from 125 to 250 Hz.
- Subband 2 from 62.5 to 125 Hz.
- Subband 3 from 31.2 62.5 Hz.
- Subband 4 from 15.6 to 31.2 Hz.
- Subband 5 from 7.8 to 15.6 Hz.
- Subband 6 from 3.9 to 7.8 Hz.
- Subband 7 from 1.9 to 3.9 Hz.
- Subband 8 from 0 to 1.9 Hz.
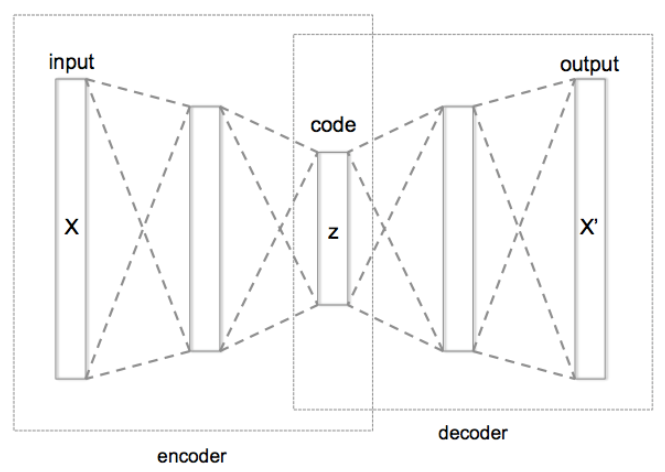
2.6. AutoEncoders
2.7. Graph Theory Analysis
- Node degree. This metric represents the number of links detected for every node.
- Path length. Mean of the shortest links present in the network.
- Clustering coefficient. Number of triangular connections in the network, divided by the theoretical maximum number of triangular connections. This variable represents the clustering capacity of the generated network.
2.8. Data Analysis
2.8.1. Binary Classification Model between PPA and CG
- Train-test split. In this step we randomly generated train and test samples from the original dataset by applying 80% for training sample and 20% for test. This split was stratified, namely, the proportion of examples in each class is preserved into train and test samples.
- Scaling. We applied a MinMaxScaler method to each column in order to transform their range of values into the range [0, 1].
- Univariate Feature Selection. A feature selection step was applied to reduce the number of features to only 50 features from the original set (309). ANOVA F-value was computed for each column-target model and only the best 50 scores were selected.
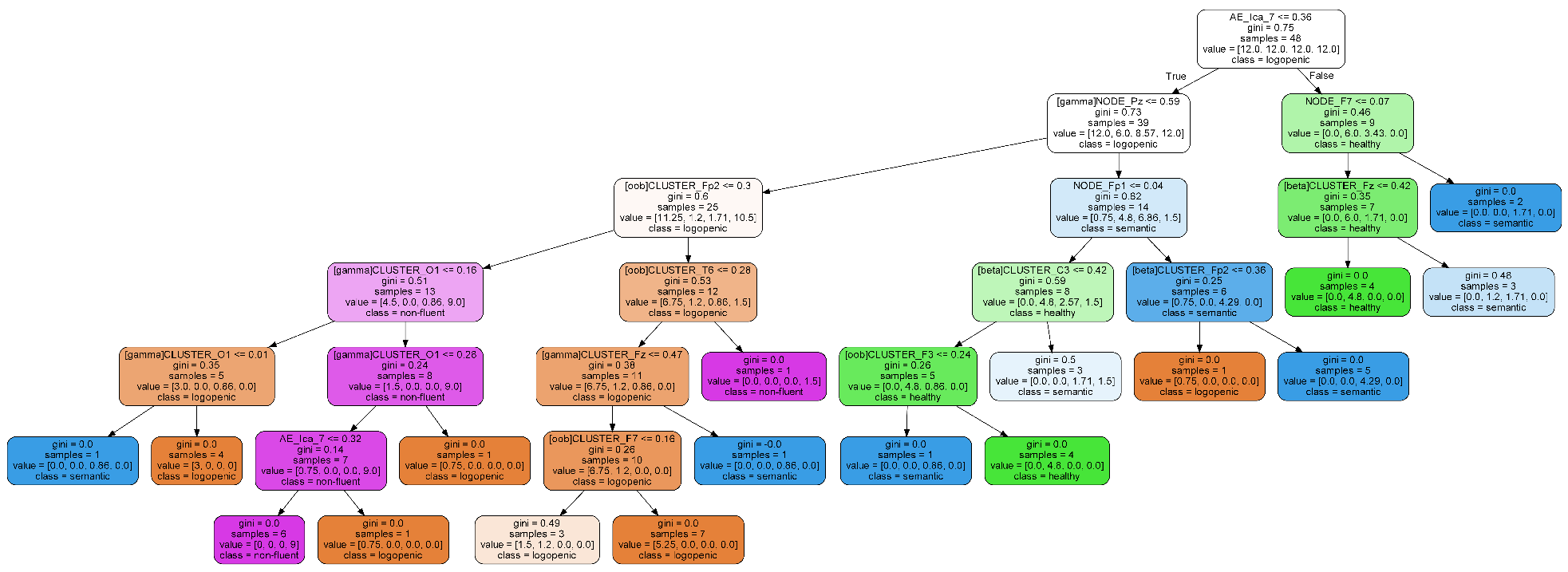
2.8.2. Classification Model for All Groups
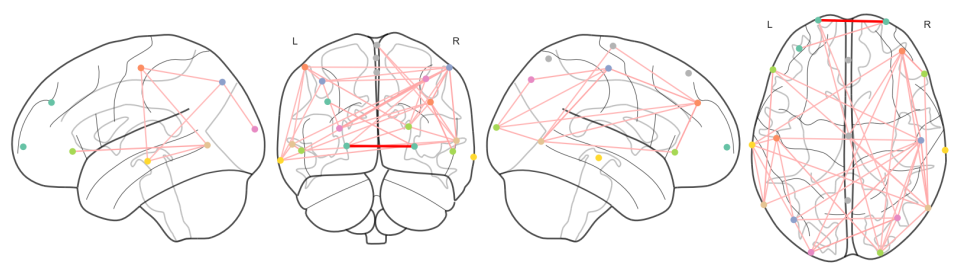
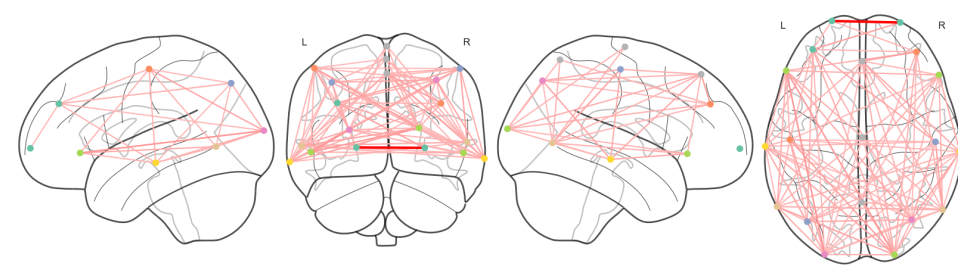
2.8.3. Network Analysis
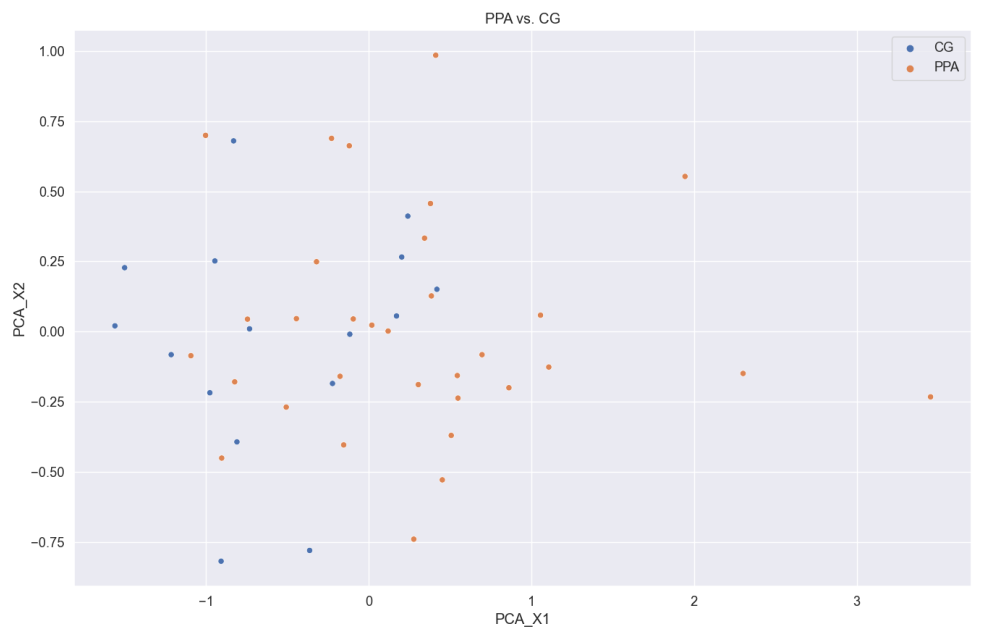
2.8.4. Principal Components Analysis
3. Results
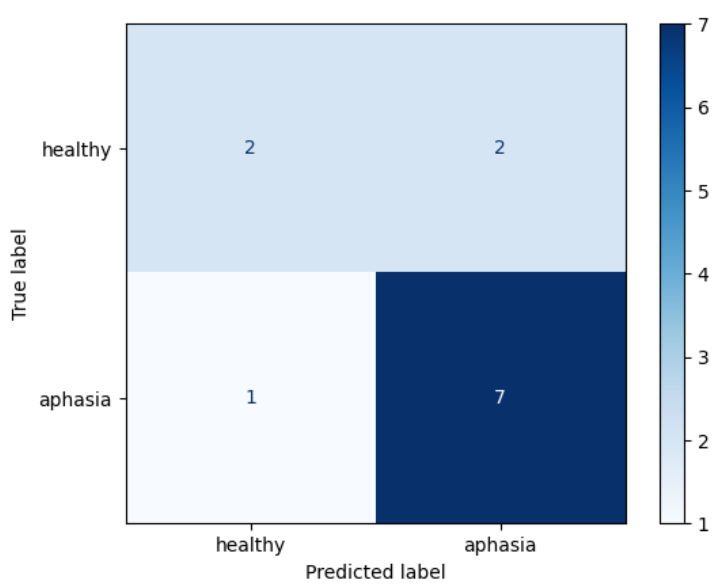
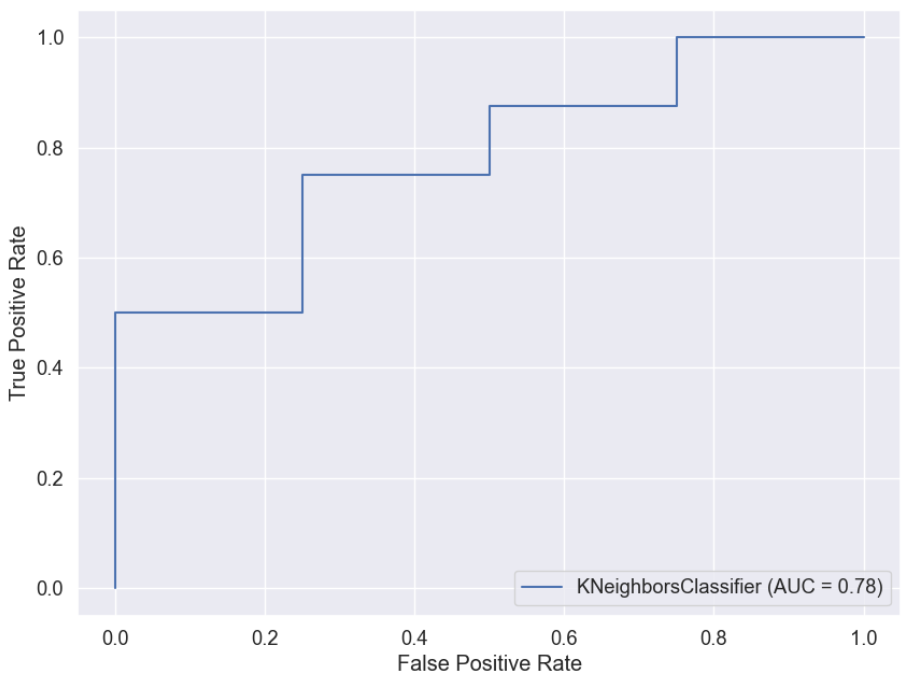
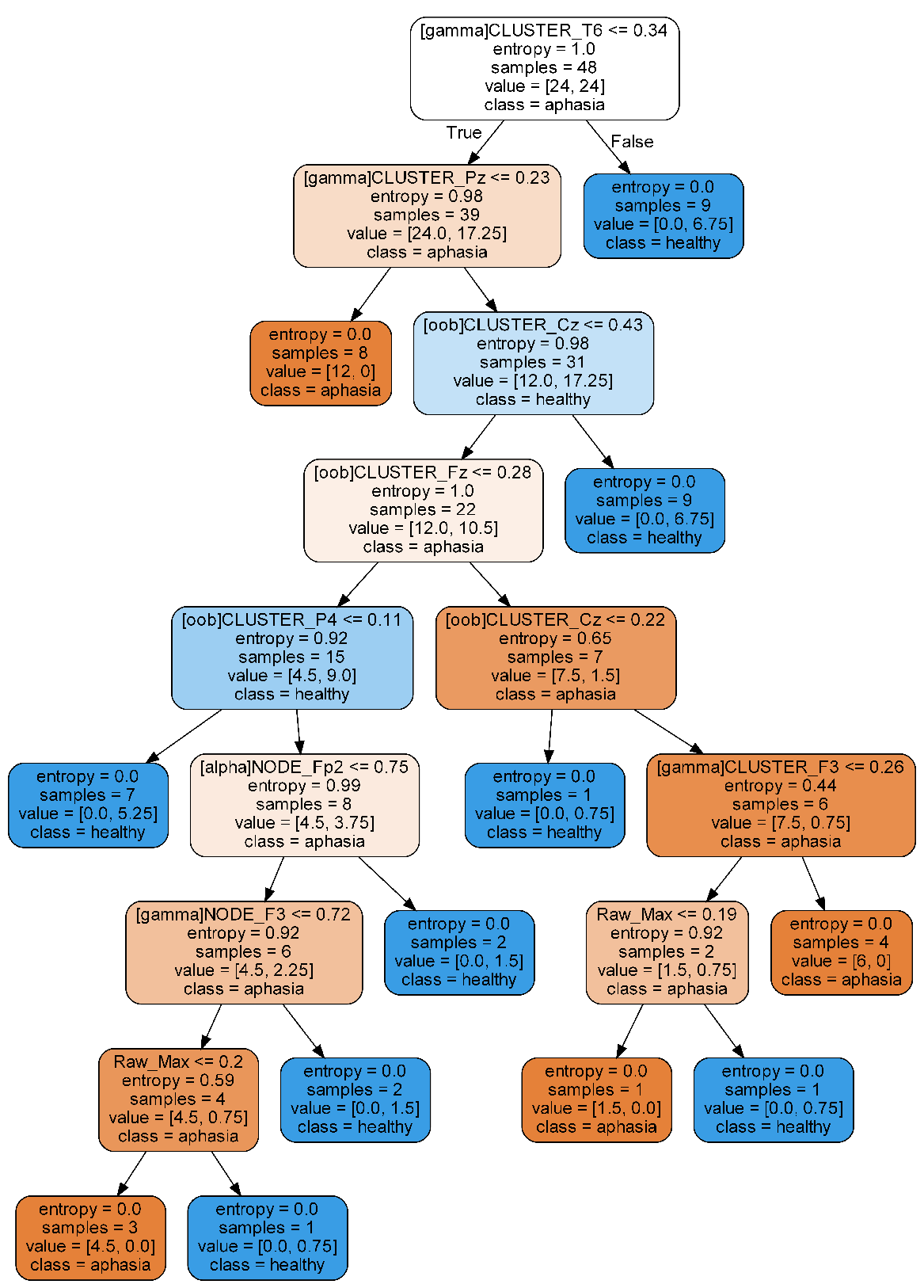
3.1. Classification Model between CG and PPA
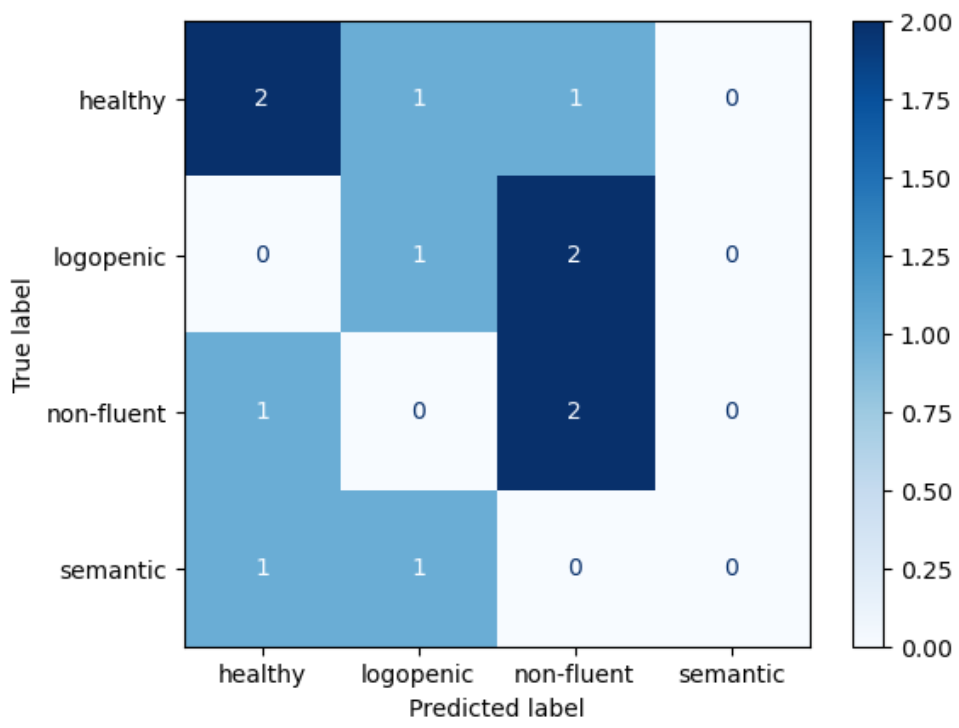
3.2. Classification Model between All Groups
4. Discussion
5. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ML | Machine Learning |
| EEG | Electroencephalogram |
| MRI | Magnetic Resonance Imaging |
| PET | Positron Emission Tomography |
| qEEG | quantitative EEG |
| MCI | Mild Cognitive Impairment |
| AD | Alzheimer Disease |
| ICA | Independent Component Analysis |
| PCA | Principal Component Analysis |
| WT | Wavelet Transform |
| GTA | Graph Theory Analysis |
| OoB | Out of Bag |
| CG | Control Group |
| PPA | Primary Progressive Aphasia |
| nfvPPA | Non-Fluent Primary Progressive Aphasia |
| svPPA | Semantic Primary Progressive Aphasia |
| lvPPA | Logopenic Primary Progressive Aphasia |
| SVM | Support Vector Machine |
| SD | Standard Deviation |
| ROC | Receiver Operating Characteristic |
| kNN | k-Nearest Neighbors |
| NB | Naive Bayes |
References
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. J. Neurol. 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [Green Version]
- Marshall, C.R.; Hardy, C.J.D.; Volkmer, A.; Russell, L.L.; Bond, R.L.; Fletcher, P.D.; Clark, C.N.; Mummery, C.J.; Schott, J.M.; Rossor, M.N.; et al. Primary progressive aphasia: A clinical approach. J. Neurol. 2018, 265, 1474–1490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stiver, J.; Staffaroni, A.M.; Walters, S.M.; You, M.Y.; Casaletto, K.B.; Erlhoff, S.J.; Possin, K.L.; Lukic, S.; La Joie, R.; Rabinovici, G.D.; et al. The Rapid Naming Test: Development and initial validation in typically aging adults. Clin. Neuropsychol. 2021, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Matías-Guiu, J.A.; Cabrera-Martín, M.N.; Moreno-Ramos, T.; Valles-Salgado, M.; Fernandez-Matarrubia, M.; Carreras, J.L.; Matías-Guiu, J. Amyloid and FDG-PET study of logopenic primary progressive aphasia: Evidence for the existence of two subtypes. J. Neurol. 2015, 262, 1463–1472. [Google Scholar] [CrossRef] [PubMed]
- Tetzloff, K.A.; Whitwell, J.L.; Utianski, R.L.; Duffy, J.R.; Clark, H.M.; Machulda, M.M.; Strand, E.A.; Josephs, K.A. Quantitative assessment of grammar in amyloid-negative logopenic aphasia. Brain Lang 2018, 186, 26–31. [Google Scholar] [CrossRef]
- Matias-Guiu, J.A.; Pytel, V.; Hernández-Lorenzo, L.; Patel, N.; Peterson, K.A.; Matías-Guiu, J.; Garrard, P.; Cuetos, F. Spanish Version of the Mini-Linguistic State Examination for the Diagnosis of Primary Progressive Aphasia. J. Alzheimers Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Epelbaum, S.; Saade, Y.M.; Flamand Roze, C.; Roze, E.; Ferrieux, S.; Arbizu, C.; Nogues, M.; Azuar, C.; Dubois, B.; Tezenas du Montcel, S.; et al. A Reliable and Rapid Language Tool for the Diagnosis, Classification, and Follow-Up of Primary Progressive Aphasia Variants. Front. Neurol. 2020, 11, 571657. [Google Scholar] [CrossRef]
- Sajjadi, S.A.; Sheikh-Bahaei, N.; Cross, J.; Gillard, J.H.; Scoffings, D.; Nestor, P.J. Can MRI Visual Assessment Differentiate the Variants of Primary-Progressive Aphasia? AJNR Am. J. Neuroradiol. 2017, 38, 954–960. [Google Scholar] [CrossRef] [Green Version]
- Matias-Guiu, J.A.; Cabrera-Martín, M.N.; Matías-Guiu, J.; Carreras, J.L. FDG-PET/CT or MRI for the Diagnosis of Primary Progressive Aphasia? AJNR Am. J. Neuroradiol. 2017, 38, E63. [Google Scholar] [CrossRef] [Green Version]
- Matías-Guiu, J.A.; Cabrera-Martín, M.N.; Pérez-Castejón, M.J.; Moreno-Ramos, T.; Rodríguez-Rey, C.; García-Ramos, R.; Ortega-Candil, A.; Fernandez-Matarrubia, M.; Oreja-Guevara, C.; Matías-Guiu, J.; et al. Visual and statistical analysis of 18F-FDG PET in primary progressive aphasia. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 916–927. [Google Scholar] [CrossRef] [PubMed]
- Josephs, K.A.; Martin, P.R.; Botha, H.; Schwarz, C.G.; Duffy, J.R.; Clark, H.M.; Machulda, M.M.; Graff-Radford, J.; Weigand, S.D.; Senjem, M.L.; et al. [18F]AV-1451 tau-PET and primary progressive aphasia. Ann. Neurol. 2018, 83, 599–611. [Google Scholar] [CrossRef] [PubMed]
- Henry, M.L.; Hubbard, H.I.; Grasso, S.M.; Mandelli, M.L.; Wilson, S.M.; Sathishkumar, M.T.; Fridriksson, J.; Daigle, W.; Boxer, A.L.; Miller, B.L.; et al. Retraining speech production and fluency in non-fluent/agrammatic primary progressive aphasia. Brain 2018, 141, 1799–1814. [Google Scholar] [CrossRef] [Green Version]
- Henry, M.L.; Hubbard, H.I.; Grasso, S.M.; Dial, H.R.; Beeson, P.M.; Miller, B.L.; Gorno-Tempini, M.L. Treatment for Word Retrieval in Semantic and Logopenic Variants of Primary Progressive Aphasia: Immediate and Long-Term Outcomes. J. Speech Lang Hear Res. 2019, 62, 2723–2749. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, D.; Gorno-Tempini, M.L.; Rabinovici, G.D.; Santos-Santos, M.A.; Seeley, W.; Miller, B.L.; Pijnenburg, Y.; Keulen, M.A.; Groot, C.; van Berckel, B.N.M.; et al. Prevalence of amyloid-β pathology in distinct variants of primary progressive aphasia. Ann. Neurol. 2018, 84, 729–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMackin, R.; Muthuraman, M.; Groppa, S.; Babiloni, C.; Taylor, J.P.; Kiernan, M.C.; Nasseroleslami, B.; Hardiman, O. Measuring network disruption in neurodegenerative diseases: New approaches using signal analysis. J. Neurol. Neurosurg. Psychiatry 2019, 90, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Vinjamuri, R. (Ed.) Advances in Neural Signal Processing; IntechOpen: London, UK, 2020. [Google Scholar]
- Logothetis, N.K. What we can do and what we cannot do with fMRI. Nature 2008, 453, 869–878. [Google Scholar] [CrossRef]
- Paszkiel, S. Analysis and Classification of EEG Signals for Brain–Computer Interfaces; Springer: Berlin, Germany, 2020. [Google Scholar] [CrossRef]
- Popa, L.L.; Dragoș, H.-M.; Strilciuc, Ș.; Pantelemon, C.; Mureșanu, I.; Dina, C.; Văcăraș, V.; Muresanu, D. Added Value of QEEG for the Differential Diagnosis of Common Forms of Dementia. Clin. EEG Neurosci. 2021, 52, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Metin, S.Z.; Erguzel, T.T.; Ertan, G.; Salcini, C.; Kocarslan, B.; Cebi, M.; Metin, B.; Tanridag, O.; Tarhan, N. The Use of Quantitative EEG for Differentiating Frontotemporal Dementia From Late-Onset Bipolar Disorder. Clin. EEG Neurosci. 2018, 49, 171–176. [Google Scholar] [CrossRef]
- Utianski, R.L.; Caviness, J.N.; Worrell, G.A.; Duffy, J.R.; Clark, H.M.; Machulda, M.M.; Withwell, J.L.; Josephs, K.A. Electroencephalography in primary progressive aphasia and apraxia of speech. Aphasiology 2018, 33, 1410–1417. [Google Scholar] [CrossRef]
- Grieder, M.; Koenig, T.; Kinoshita, T.; Utsunomiya, K.; Wahlund, L.O.; Dierks, T.; Nishida, K. Discovering EEG resting state alterations of semantic dementia. Clin. Neurophysiol. 2016, 127, 2175–2181. [Google Scholar] [CrossRef] [Green Version]
- Subasi, A.; Kevric, J.; Abdullah Canbaz, M. Epileptic seizure detection using hybrid machine learning methods. Neural Comput. Appl. 2019, 31, 317–325. [Google Scholar] [CrossRef]
- Hügle, M.; Heller, S.; Watter, M.; Blum, M.; Manzouri, F.; Dumpelmann, M.; Schulze-Bonhage, A.; Woias, P.; Boedecker, J. Early Seizure Detection with an Energy-Efficient Convolutional Neural Network on an Implantable Microcontroller. In Proceedings of the 2018 International Joint Conference on Neural Networks (IJCNN), Rio de Janeiro, Brazil, 8–13 July 2018; pp. 1–7. [Google Scholar] [CrossRef] [Green Version]
- Kiral-Kornek, I.; Roy, S.; Nurse, E.; Mashford, B.; Karoly, P.; Carroll, T.; Payne, D.; Saha, S.; Baldassano, S.; O’Brien, T.; et al. Epileptic Seizure Prediction Using Big Data and Deep Learning: Toward a Mobile System. EBioMedicine 2018, 27, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirowski, P.; Madhavan, D.; LeCun, Y.; Kuzniecky, R. Classification of patterns of EEG synchronization for seizure prediction. Clin. Neurophysiol. 2009, 120, 1927–1940. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, C.; Koenig, T.; Jelic, V.; Prichep, L.; John, R.E.; Wahlund, L.; Dodge, Y.; Dierks, T. Application and comparison of classification algorithms for recognition of Alzheimer’s disease in electrical brain activity (EEG). J. Neurosci. Methods 2007, 161, 342–350. [Google Scholar] [CrossRef]
- Cai, H.; Sha, X.; Han, X.; Wei, S.; Hu, B. Pervasive EEG diagnosis of depression using Deep Belief Network with three-electrodes EEG collector. In Proceedings of the 2016 IEEE International Conference on Bioinformatics and Biomedicine, BIBM 2016, Shenzhen, China, 15–18 December 2016; pp. 1239–1246. [Google Scholar]
- Hosseinifard, B.; Moradi, M.H.; Rostami, R. Classifying depression patients and normal subjects using machine learning techniques and nonlinear features from EEG signal. Comput. Methods Programs Biomed. 2013, 109, 339–345. [Google Scholar] [CrossRef]
- Gemein, L.; Schirrmeister, R.; Chrabaszcz, P.; Wilson, D.; Boedecker, J.; Schulze-Bonhage, A.; Hutter, F.; Ball, T. Machine-learning-based diagnostics of EEG pathology. NeuroImage 2020, 220, 117021. [Google Scholar] [CrossRef]
- Garn, H.; Coronel, C.; Waser, M.; Caravias, G.; Ransmayr, G. Differential diagnosis between patients with probable Alzheimer’s disease, Parkinson’s disease dementia, or dementia with Lewy bodies and frontotemporal dementia, behavioral variant, using quantitative electroencephalographic features. J. Neural Transm. 2017, 124, 569–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vecchio, F.; Miraglia, F.; Alú, F.; Orticoni, A.; Judica, E.; Cotelli, M.; Rossini, P.M. Contribution of Graph Theory Applied to EEG Data Analysis for Alzheimer’s Disease Versus Vascular Dementia Diagnosis. J. Alzheimers Dis. 2021, 82, 871–879. [Google Scholar] [CrossRef]
- Ieracitano, C.; Mammone, N.; Hussain, A.; Morabito, F.C. A Convolutional Neural Network based self-learning approach for classifying neurodegenerative states from EEG signals in dementia. In Proceedings of the 2020 International Joint Conference on Neural Networks (IJCNN), Glasgow, UK, 19–24 July 2020; pp. 1–8. [Google Scholar] [CrossRef]
- Matias-Guiu, J.A.; Suárez-Coalla, P.; Pytel, V.; Cabrera-Martín, M.N.; Moreno-Ramos, T.; Delgado-Alonso, C.; Delgado-Álvarez, A.; Matías-Guiu, J.; Cuetos, F. Reading prosody in the non-fluent and logopenic variants of primary progressive aphasia. Cortex 2020, 132, 63–78. [Google Scholar] [CrossRef]
- SCNN. Makoto’s Preprocessing Pipeline. 2021. Available online: https://sccn.ucsd.edu/wiki/Makoto’s_preprocessing_pipeline (accessed on 21 June 2021).
- SCNN. CleanLine. 2021. Available online: https://github.com/sccn/cleanline (accessed on 21 June 2021).
- Maturana-Candelas, A.; Gómez, C.; Poza, J.; Ruiz-Gómez, S.J.; Hornero, R. Inter-band Bispectral Analysis of EEG Background Activity to Characterize Alzheimer’s Disease Continuum. Front. Comput. Neurosci. 2020, 14, 70. [Google Scholar] [CrossRef]
- Beharelle, A.R.; Small, S.L. Chapter 64-Imaging Brain Networks for Language: Methodology and Examples from the Neurobiology of Reading. In Neurobiology of Language; Hickok, G., Small, S.L., Eds.; Academic Press: San Diego, CA, USA, 2016; pp. 805–814. [Google Scholar] [CrossRef]
- Smailovic, U.; Jelic, V. Neurophysiological Markers of Alzheimer’s Disease: Quantitative EEG Approach. Neurol. Ther. 2019, 8, 37–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheong, L.C.; Sudirman, R.; Hussin, S. Feature extraction of EEG signal using wavelet transform for autism classification. ARPN J. Eng. Appl. Sci. 2015, 10, 8533–8540. [Google Scholar]
- Mulders, P.; Eijndhoven, P.; Beckmann, C. Identifying Large-Scale Neural Networks Using fMRI; Academic Press: Cambridge, MA, USA, 2016; pp. 209–237. [Google Scholar] [CrossRef]
- Jalili, M.; Knyazeva, M.G. Constructing brain functional networks from EEG: Partial and unpartial correlations. J. Integr. Neurosci. 2011, 10, 213–232. [Google Scholar] [CrossRef]
- Prakash, B.; Baboo, G.K.; Baths, V. A Novel Approach to Learning Models on EEG Data Using Graph Theory Features-A Comparative Study. Big Data Cogn. Comput. 2021, 5, 39. [Google Scholar] [CrossRef]
- Wadhera, T. Brain network topology unraveling epilepsy and ASD Association: Automated EEG-based diagnostic model. Expert Syst. Appl. 2021, 186, 115762. [Google Scholar] [CrossRef]
- Snaedal, J.; Johannesson, G.H.; Gudmundsson, T.E.; Blin, N.P.; Emilsdottir, A.L.; Einarsson, B.; Johnsen, K. Diagnostic accuracy of statistical pattern recognition of electroencephalogram registration in evaluation of cognitive impairment and dementia. Dement. Geriatr. Cogn. Disord. 2012, 34, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Lindau, M.; Jelic, V.; Johansson, S.E.; Andersen, C.; Wahlund, L.O.; Almkvist, O. Quantitative EEG abnormalities and cognitive dysfunctions in frontotemporal dementia and Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2003, 15, 106–114. [Google Scholar] [CrossRef]
- Caso, F.; Cursi, M.; Magnani, G.; Fanelli, G.; Falautano, M.; Comi, G.; Leocani, L.; Minicucci, F. Quantitative EEG and LORETA: Valuable tools in discerning FTD from AD? Neurobiol. Aging 2012, 33, 2343–2356. [Google Scholar] [CrossRef]
- Tzimourta, K.D.; Christou, V.; Tzallas, A.T.; Giannakeas, N.; Astrakas, L.G.; Angelidis, P.; Tsalikakis, D.; Tsipouras, M.G. Machine Learning Algorithms and Statistical Approaches for Alzheimer’s Disease Analysis Based on Resting-State EEG Recordings: A Systematic Review. Int. J. Neural Syst. 2021, 31, 2130002. [Google Scholar] [CrossRef]
- Winters-Hilt, S.; Merat, S. SVM clustering. BMC Bioinform. 2007, 8 (Suppl. 7), S18. [Google Scholar] [CrossRef] [Green Version]
- Hastie, T.; Tibshirani, R.; Friedman, J. The Elements of Statistical Learning; Springer Series in Statistics; Springer New York Inc.: New York, NY, USA, 2001. [Google Scholar]
- Vecchio, F.; Miraglia, F.; Alù, F.; Menna, M.; Judica, E.; Cotelli, M.; Rossini, P.M. Classification of Alzheimer’s Disease with Respect to Physiological Aging with Innovative EEG Biomarkers in a Machine Learning Implementation. J. Alzheimers Dis. 2020, 75, 1253–1261. [Google Scholar] [CrossRef]
- Gaubert, S.; Houot, M.; Raimondo, F.; Ansart, M.; Corsi, M.C.; Naccache, L.; Sitt, J.D.; Habert, M.O.; Dubois, B.; De Vico Fallani, F.; et al. A machine learning approach to screen for preclinical Alzheimer’s disease. Neurobiol. Aging 2021, 105, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Pytel, V.; Cabrera-Martin, M.; Delgado-Alvarez, A.; Ayala, J.; Balugo, P.; Delgado-Alonso, C.; Yus, M.; Carreras, M.; Carreras, J.; Matias-Guiu, J.; et al. Personalized repetitive transcranial magnetic stimulation for primary progressive aphasia. J. Alzheimers Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Matias-Guiu, J.A.; Díaz-Álvarez, J.; Cuetos, F.; Cabrera-Martín, M.N.; Segovia-Ríos, I.; Pytel, V.; Moreno-Ramos, T.; Carreras, J.L.; Matías-Guiu, J.; Ayala, J.L. Machine learning in the clinical and language characterisation of primary progressive aphasia variants. Cortex 2019, 119, 312–323. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PPA | nfvPPA | svPPA | lvPPA | |
|---|---|---|---|---|
| Number of participants | 40 | 18 (45%) | 10 (25%) | 12 (30%) |
| Age | 68.7 ± 6.94 | 68.55 ± 7.29 | 66.80 ± 6.35 | 70.50 ± 6.97 |
| Women | 26 (65%) | |||
| Years of education | 13.90 ± 4.26 | 13.33 ± 4.41 | 14.20 ± 4.15 | 14.50 ± 4.35 |
| Years since symptom onset | 4.00 ± 2.25 | 4.83 ± 1.94 | 4.00 ± 2.98 | 2.75 ± 1.42 |
| ACE-III | 55.78 ± 26.59 | 71.76 ± 22.07 | 53.89 ± 15.72 | 48.00 ± 23.37 |
| CDR-FTLD (Sum of boxes) | 2.6 ± 1.81 | 2.22 ± 1.54 | 2.60 ± 1.67 | 3.16 ± 2.26 |
| Model | F1-Score | Precision | Sensitivity | Accuracy |
|---|---|---|---|---|
| Decision Tree | 0.38 | 0.39 | 0.38 | 0.42 |
| kNN | 0.83 | 0.78 | 0.88 | 0.75 |
| SVM | 0.58 | 0.72 | 0.86 | 0.58 |
| Random Forest | 0.37 | 0.32 | 0.43 | 0.58 |
| Elastic Net | 0.4 | 0.33 | 0.5 | 0.66 |
| Gaussian NB | 0.78 | 0.9 | 0.75 | 0.83 |
| Multinomial NB | 0.73 | 0.73 | 0.75 | 0.75 |
| Model | F1-Score | Precision | Sensitivity | Accuracy |
|---|---|---|---|---|
| Decision Tree | 0.32 | 0.32 | 0.4 | 0.42 |
| kNN | 0.6 | 0.68 | 0.58 | 0.58 |
| SVM | 0.39 | 0.40 | 0.46 | 0.5 |
| Random Forest | 0.39 | 0.38 | 0.48 | 0.5 |
| Elastic Net | 0.34 | 0.31 | 0.33 | 0.38 |
| Gaussian NB | 0.27 | 0.25 | 0.31 | 0.33 |
| Multinomial NB | 0.2 | 0.2 | 0.25 | 0.25 |
| Model | F1-Score | Precision | Sensitivity | Accuracy |
|---|---|---|---|---|
| Decision Tree | 0.49 | 0.50 | 0.50 | 0.50 |
| kNN | 0.46 | 0.6 | 0.38 | 0.42 |
| SVM | 0.50 | 0.56 | 0.56 | 0.50 |
| Random Forest | 0.40 | 0.33 | 0.50 | 0.67 |
| Elastic Net | 0.40 | 0.33 | 0.50 | 0.67 |
| Gaussian NB | 0.37 | 0.32 | 0.44 | 0.58 |
| Multinomial NB | 0.56 | 0.56 | 0.56 | 0.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moral-Rubio, C.; Balugo, P.; Fraile-Pereda, A.; Pytel, V.; Fernández-Romero, L.; Delgado-Alonso, C.; Delgado-Álvarez, A.; Matias-Guiu, J.; Matias-Guiu, J.A.; Ayala, J.L. Application of Machine Learning to Electroencephalography for the Diagnosis of Primary Progressive Aphasia: A Pilot Study. Brain Sci. 2021, 11, 1262. https://doi.org/10.3390/brainsci11101262
Moral-Rubio C, Balugo P, Fraile-Pereda A, Pytel V, Fernández-Romero L, Delgado-Alonso C, Delgado-Álvarez A, Matias-Guiu J, Matias-Guiu JA, Ayala JL. Application of Machine Learning to Electroencephalography for the Diagnosis of Primary Progressive Aphasia: A Pilot Study. Brain Sciences. 2021; 11(10):1262. https://doi.org/10.3390/brainsci11101262
Chicago/Turabian StyleMoral-Rubio, Carlos, Paloma Balugo, Adela Fraile-Pereda, Vanesa Pytel, Lucía Fernández-Romero, Cristina Delgado-Alonso, Alfonso Delgado-Álvarez, Jorge Matias-Guiu, Jordi A. Matias-Guiu, and José Luis Ayala. 2021. "Application of Machine Learning to Electroencephalography for the Diagnosis of Primary Progressive Aphasia: A Pilot Study" Brain Sciences 11, no. 10: 1262. https://doi.org/10.3390/brainsci11101262