
MPC-Based Prediction of Anti-Mutant Effectiveness of Antibiotic Combinations: In Vitro Model Study with Daptomycin and Gentamicin against Staphylococcus aureus

 , ,
, ,
Abstract
:1. Introduction
2. Results
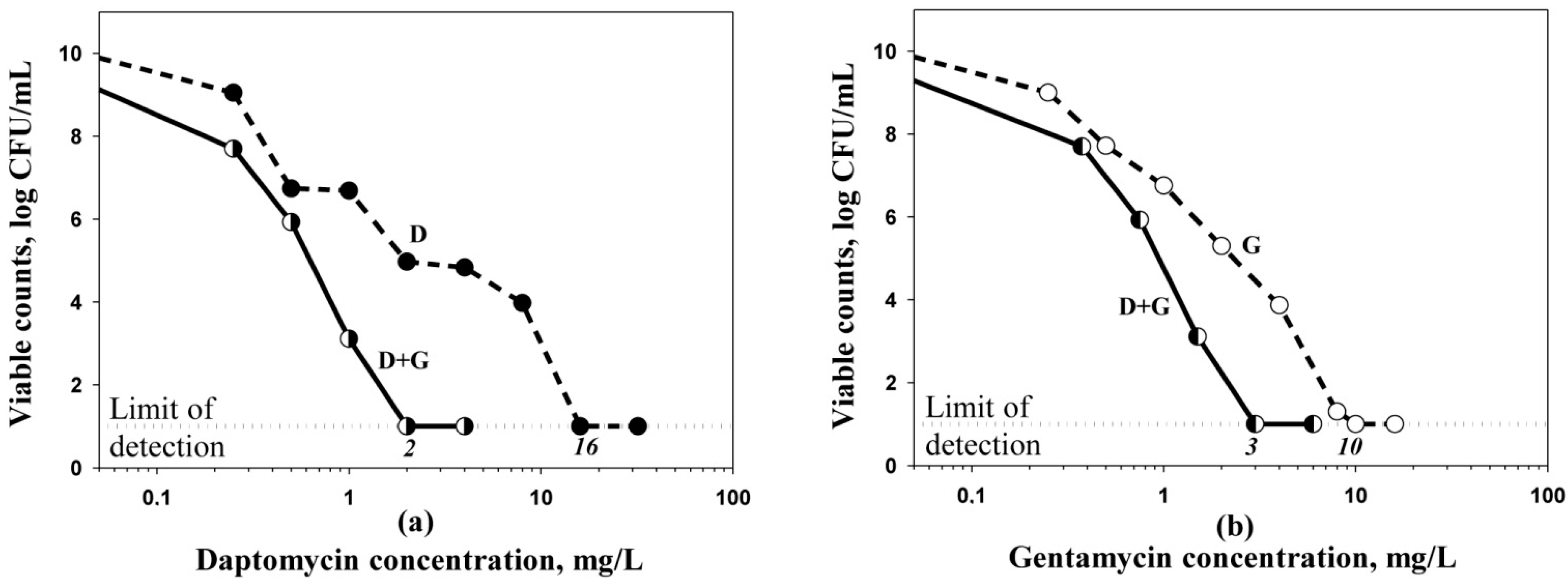
2.1. MPCs of Daptomycin and Gentamicin Alone and in Combination
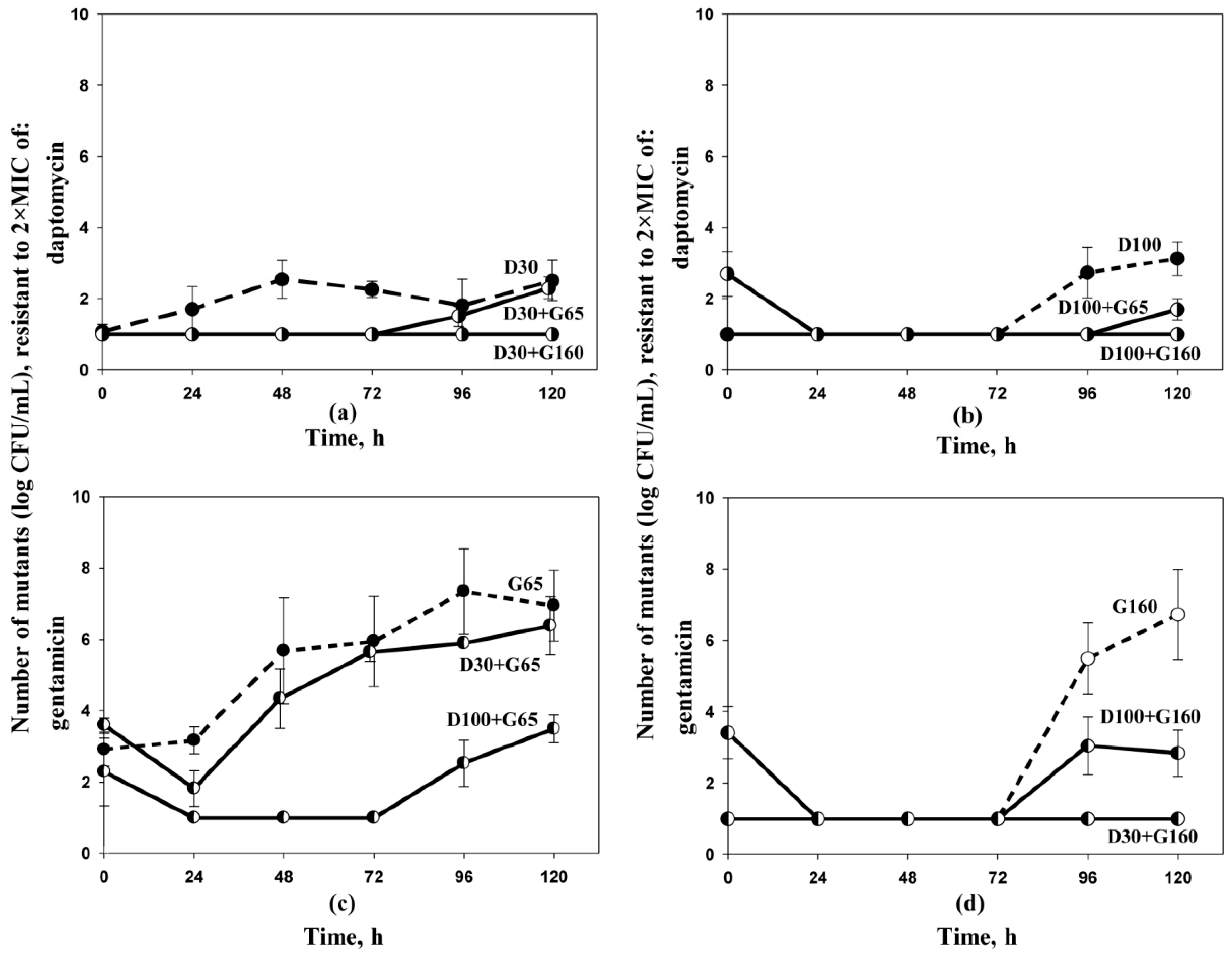
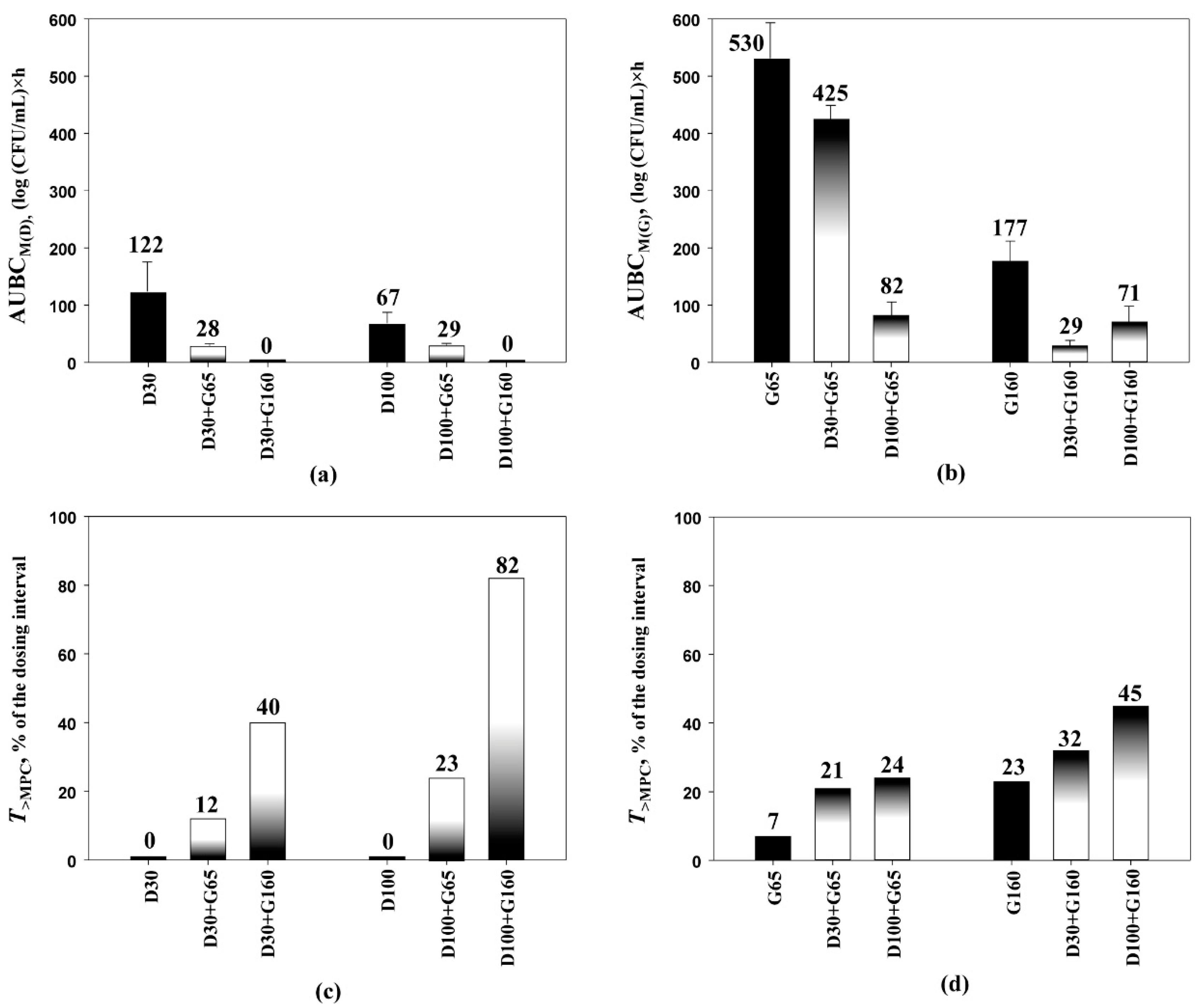
2.2. Antibiotic Pharmacodynamics with Resistant S. aureus Mutants
3. Discussion
4. Materials and Methods
4.1. Antimicrobial Agents, Bacterial Strain and Susceptibility Testing
4.2. MPC Determinations
4.3. Antibiotic Dosing Regimens and Simulated Pharmacokinetic Profiles
4.4. In Vitro Dynamic Model
4.5. Quantitation of the Antimicrobial Effects on the Resistant Subpopulations of S. aureus
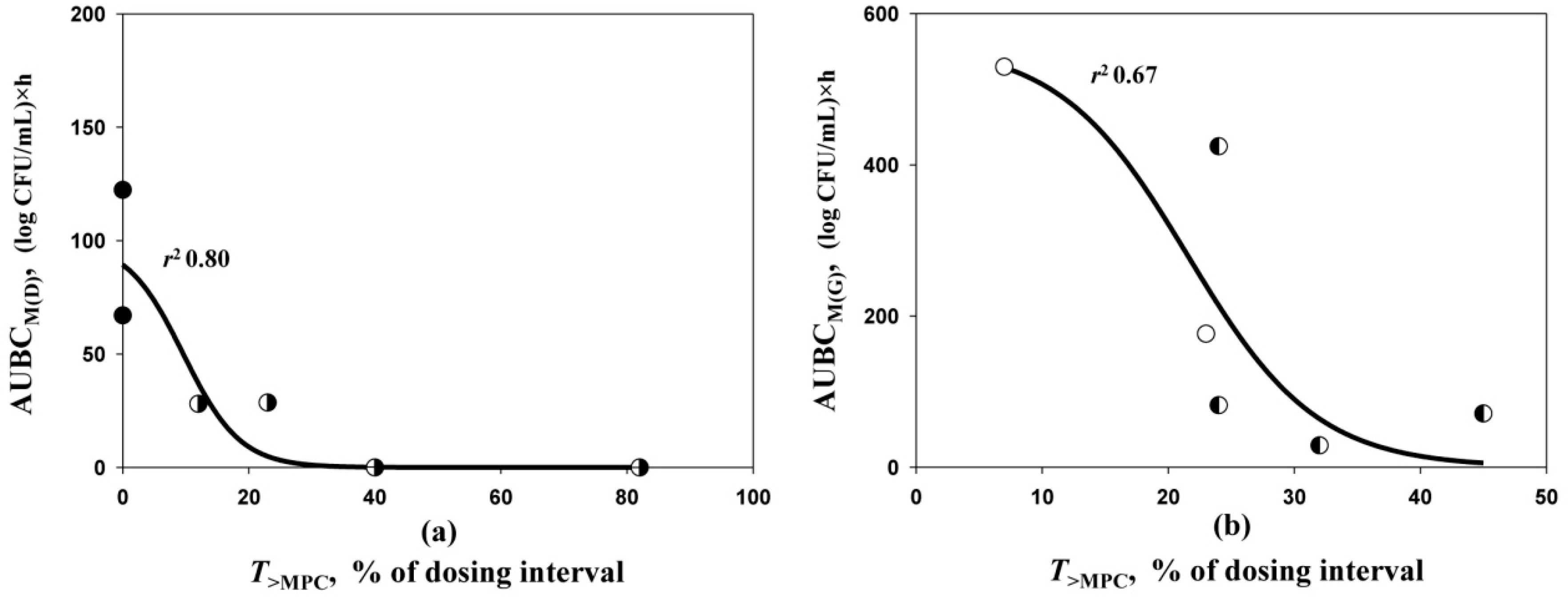
4.6. T>MPC Relationships with the Emergence of Resistance
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cervera, C.; Castañeda, X.; Pericas, J.M.; Del Río, A.; de la Maria, C.G.; Mestres, C.; Falces, C.; Marco, F.; Moreno, A.; Miró, J.M. Clinical utility of daptomycin in infective endocarditis caused by Gram-positive cocci. Int. J. Antimicrob. Agents 2011, 3, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Claeys, K.C.; Zasowski, E.J.; Casapao, A.M.; Lagnf, A.M.; Nagel, J.L.; Nguyen, C.T.; Hallesy, J.A.; Compton, M.T.; Kaye, K.S.; Levine, D.P.; et al. Daptomycin improves outcomes regardless of vancomycin MIC in a propensity-matched analysis of methicillin-resistant Staphylococcus aureus bloodstream infections. Antimicrob. Agents Chemother. 2016, 60, 5841–5848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, V.G., Jr.; Boucher, H.W.; Corey, G.R.; Abrutyn, E.; Karchmer, A.W.; Rupp, M.E.; Levine, D.P.; Chambers, H.F.; Tally, F.P.; Vigliani, G.A.; et al. S. aureus Endocarditis and Bacteremia Study Group. Daptomycin versus standard therapy for bacteremia and endocarditis caused by Staphylococcus aureus. N. Engl. J. Med. 2006, 355, 653–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, C.L.; Osaki-Kiyan, P.; Haque, N.Z.; Perri, M.B.; Donabedian, S.; Zervos, M.J. Daptomycin versus vancomycin for bloodstream infections due to methicillin-resistant Staphylococcus aureus with a high vancomycin minimum inhibitory concentration: A case–control study. Clin. Infect. Dis. 2012, 54, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Boyle-Vavra, S.; Jones, M.; Gourley, B.L.; Holmes, M.; Ruf, R.; Balsam, A.R.; Boulware, D.R.; Kline, S.; Jawahir, S.; Devries, A.; et al. Comparative genome sequencing of an isogenic pair of USA800 clinical methicillin-resistant Staphylococcus aureus isolates obtained before and after daptomycin treatment failure. Antimicrob. Agents Chemother. 2011, 55, 2018–2025. [Google Scholar] [CrossRef] [Green Version]
- Cavalcante, F.S.; Ferreira, D.C.; Chamon, R.C.; da Costa, T.M.; Maia, F.; Barros, E.M.; Dantas, T.S.; Dos Santos, K.R. Daptomycin and methicillin-resistant Staphylococcus aureus isolated from a catheter-related bloodstream infection: A case report. BMC Res. Notes 2014, 7, 759. [Google Scholar] [CrossRef] [Green Version]
- Dortet, L.; Anguel, N.; Fortineau, N.; Richard, C.; Nordmann, P. In vivo acquired daptomycin resistance during treatment of methicillin-resistant Staphylococcus aureus endocarditis. Int. J. Infect. Dis. 2013, 11, e1076–e1077. [Google Scholar] [CrossRef] [Green Version]
- Sotillo, A.; Paño-Pardo, J.R.; López-Quintana, B.; Gómez-Gil, R. Development of daptomycin resistance during therapy in a patient with methicillin-resistant Staphylococcus aureus endocarditis: A case report. Enferm. Infecc. Microbiol. Clin. 2016, 34, 534–535. [Google Scholar] [CrossRef]
- LaPlante, K.L.; Woodmansee, S. Activities of daptomycin and vancomycin alone and in combination with rifampin and gentamicin against biofilm-forming methicillin-resistant Staphylococcus aureus isolates in an experimental model of endocarditis. Antimicrob. Agents Chemother. 2009, 53, 3880–3886. [Google Scholar] [CrossRef] [Green Version]
- Miró, J.M.; García-de-la-Mària, C.; Armero, Y.; Soy, D.; Moreno, A.; del Río, A.; Almela, M.; Sarasa, M.; Mestres, C.A.; Gatell, J.M.; et al. Hospital Clinic Experimental Endocarditis Study Group. Addition of gentamicin or rifampin does not enhance the effectiveness of daptomycin in treatment of experimental endocarditis due to methicillin-resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 2009, 53, 4172–4177. [Google Scholar] [CrossRef] [Green Version]
- Jiang, J.H.; Peleg, A.Y. Daptomycin-Nonsusceptible Staphylococcus aureus: The role of combination therapy with daptomycin and gentamicin. Genes 2015, 6, 1256–1267. [Google Scholar] [CrossRef] [Green Version]
- Entenza, J.M.; Giddey, M.; Vouillamoz, J.; Moreillon, P. In vitro prevention of the emergence of daptomycin resistance in Staphylococcus aureus and enterococci following combination with amoxicillin/clavulanic acid or ampicillin. Int. J. Antimicrob. Agents 2010, 35, 451–456. [Google Scholar] [CrossRef]
- Rose, W.E.; Leonard, S.N.; Rybak, M.J. Evaluation of daptomycin pharmacodynamics and resistance at various dosage regimens against Staphylococcus aureus isolates with reduced susceptibilities to daptomycin in an in vitro pharmacodynamic model with simulated endocardial vegetations. Antimicrob. Agents Chemother. 2008, 52, 3061–3067. [Google Scholar] [CrossRef] [Green Version]
- LaPlante, K.L.; Rybak, M.J. Impact of high-inoculum Staphylococcus aureus on the activities of nafcillin, vancomycin, linezolid, and daptomycin, alone and in combination with gentamicin, in an in vitro pharmacodynamic model. Antimicrob. Agents Chemother. 2004, 48, 4665–4672. [Google Scholar] [CrossRef] [Green Version]
- Tsuji, B.T.; Rybak, M.J. Short-course gentamicin in combination with daptomycin or vancomycin against Staphylococcus aureus in an in vitro pharmacodynamic model with simulated endocardial vegetations. Antimicrob. Agents Chemother. 2005, 49, 2735–2745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zinner, S.H.; Alieva, K.N.; Golikova, M.V.; Strukova, E.N.; Portnoy, Y.A.; Firsov, A.A. Anti-mutant efficacy of antibiotic combinations: In vitro model studies with linezolid and daptomycin. J. Antimicrob. Chemother. 2021, 76, 1832–1839. [Google Scholar] [CrossRef] [PubMed]
- Zinner, S.H.; Golikova, M.V.; Strukova, E.N.; Portnoy, Y.A.; Firsov, A.A. Predicting antibiotic combination effects on the selection of resistant Staphylococcus aureus: In vitro model studies with linezolid and gentamicin. Int. J. Antimicrob. Agents 2018, 52, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Firsov, A.A.; Golikova, M.V.; Strukova, E.N.; Portnoy, Y.A.; Dovzhenko, S.A.; Kobrin, M.B.; Zinner, S.H. Pharmacokinetically-based prediction of the effects of antibiotic combinations on resistant Staphylococcus aureus mutants: In vitro model studies with linezolid and rifampicin. J. Chemother. 2017, 29, 220–226. [Google Scholar] [CrossRef]
- Golikova, M.V.; Strukova, E.N.; Portnoy, Y.A.; Dovzhenko, S.A.; Kobrin, M.B.; Zinner, S.H.; Firsov, A.A. A novel parameter to predict the effects of antibiotic combinations on the development of Staphylococcus aureus resistance: In vitro model studies at subtherapeutic daptomycin and rifampicin exposures. J. Chemother. 2019, 17, 1–9. [Google Scholar] [CrossRef]
- Allen, G.P.; Kaatz, G.W.; Rybak, M.J. Activities of mutant prevention concentration-targeted moxifloxacin and levofloxacin against Streptococcus pneumoniae in an in vitro pharmacodynamic model. Antimicrob. Agents Chemother. 2003, 47, 2606–2614. [Google Scholar] [CrossRef] [Green Version]
- Croisier, D.; Etienne, M.; Piroth, L.; Bergoin, E.; Lequeu, C.; Portier, H.; Chavanet, P. In vivo pharmacodynamic efficacy of gatifloxacin against Streptococcus pneumoniae in an experimental model of pneumonia: Impact of the low levels of fluoroquinolone resistance on the enrichment of resistant mutants. J. Antimicrob. Chemother. 2004, 54, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Firsov, A.A.; Strukova, E.N.; Shlykova, D.S.; Portnoy, Y.A.; Kozyreva, V.K.; Edelstein, M.V.; Dovzhenko, S.A.; Kobrin, M.B.; Zinner, S.H. Bacterial resistance studies using in vitro dynamic models: The predictive power of the mutant prevention and minimum inhibitory antibiotic concentrations. Antimicrob. Agents Chemother. 2013, 57, 4956–4962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Firsov, A.A.; Portnoy, Y.A.; Strukova, E.N.; Shlykova, D.S.; Zinner, S.H. Predicting bacterial resistance using the time inside the mutant selection window: Possibilities and limitations. Int. J. Antimicrob. Agents 2014, 44, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Alieva, K.N.; Golikova, M.V.; Portnoy, Y.A.; Dovzhenko, S.A.; Kobrin, M.B.; Zinner, S.H.; Firsov, A.A. Concentration-dependent enrichment of resistant Enterococcus faecium exposed to linezolid in an in vitro dynamic model. J. Chemother. 2018, 30, 364–370. [Google Scholar] [CrossRef]
- Alieva, K.N.; Strukova, E.N.; Golikova, M.V.; Portnoy, Y.A.; Zinner, S.H.; Firsov, A.A. Time inside the mutant selection window as a predictor of staphylococcal resistance to linezolid. J. Antibiot. 2018, 71, 514–521. [Google Scholar] [CrossRef]
- Cobussen, M.; Stassen, P.M.; Posthouwer, D.; van Tiel, F.H.; Savelkoul, P.H.M.; Havenith, T.; Haeseker, M.B. Improving peak concentrations of a single dose regimen of gentamicin in patients with sepsis in the emergency department. PLoS ONE 2019, 14, e0210012. [Google Scholar] [CrossRef] [Green Version]
- Demczar, D.J.; Nafziger, A.N.; Bertino, J.S., Jr. Pharmacokinetics of gentamicin at traditional versus high doses: Implications for once-daily aminoglycoside dosing. Antimicrob. Agents Chemother. 1997, 41, 1115–1119. [Google Scholar] [CrossRef] [Green Version]
- Dvorchik, B.H.; Brazier, D.; DeBruin, M.F.; Arbeit, R.D. Daptomycin pharmacokinetics and safety following administration of escalating doses once daily to healthy subjects. Antimicrob. Agents Chemother. 2003, 47, 1318–1323. [Google Scholar] [CrossRef] [Green Version]
- Golikova, M.V.; Strukova, E.N.; Portnoy, Y.A.; Zinner, S.H.; Firsov, A.A. Verification of a novel approach to predicting effects of antibiotic combinations: In vitro dynamic model study with daptomycin and gentamicin against Staphylococcus aureus. Antibiotics 2020, 9, 538. [Google Scholar] [CrossRef]
- Fuchs, P.C.; Barry, A.L.; Brown, S.D. Daptomycin susceptibility tests: Interpretive criteria, quality control, and effect of calcium on in vitro tests. Diagn. Microbiol. Infect. Dis. 2000, 38, 51–58. [Google Scholar] [CrossRef]
- Blaser, J. In-vitro model for simultaneous simulation of the serum kinetics of two drugs with different half-lives. J. Antimicrob. Chemother. 1985, 15, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Firsov, A.A.; Smirnova, M.V.; Strukova, E.N.; Vostrov, S.N.; Portnoy, Y.A.; Zinner, S.H. Enrichment of resistant Staphylococcus aureus at ciprofloxacin concentrations simulated within the mutant selection window: Bolus versus continuous infusion. Int. J. Antimicrob. Agents 2008, 32, 488–493. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibiotic | Daptomycin-to-Gentamicin AUC Ratio | Regimen | MPC, mg/L |
|---|---|---|---|
| Daptomycin | - | D30 | 16 |
| D100 | 16 | ||
| Daptomycin in the presence of gentamicin | 1:2 | D30+G65 | 2 |
| 1:5 | D30+G160 | 1.2 | |
| 1.5:1 | D100+G65 | 6 | |
| 1:1.5 | D100+G160 | 2 | |
| Gentamicin | - | G65 | 10 |
| G160 | 10 | ||
| Gentamicin in the presence of daptomycin | 1:2 | D30+G65 | 4 |
| 1.5:1 | D100+G65 | 4 | |
| 1:5 | D30+G160 | 6 | |
| 1:1.5 | D100+G160 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Golikova, M.V.; Strukova, E.N.; Portnoy, Y.A.; Zinner, S.H.; Firsov, A.A. MPC-Based Prediction of Anti-Mutant Effectiveness of Antibiotic Combinations: In Vitro Model Study with Daptomycin and Gentamicin against Staphylococcus aureus. Antibiotics 2021, 10, 1148. https://doi.org/10.3390/antibiotics10101148
Golikova MV, Strukova EN, Portnoy YA, Zinner SH, Firsov AA. MPC-Based Prediction of Anti-Mutant Effectiveness of Antibiotic Combinations: In Vitro Model Study with Daptomycin and Gentamicin against Staphylococcus aureus. Antibiotics. 2021; 10(10):1148. https://doi.org/10.3390/antibiotics10101148
Chicago/Turabian StyleGolikova, Maria V., Elena N. Strukova, Yury A. Portnoy, Stephen H. Zinner, and Alexander A. Firsov. 2021. "MPC-Based Prediction of Anti-Mutant Effectiveness of Antibiotic Combinations: In Vitro Model Study with Daptomycin and Gentamicin against Staphylococcus aureus" Antibiotics 10, no. 10: 1148. https://doi.org/10.3390/antibiotics10101148