
Antibiotic-Related Adverse Drug Reactions in Patients Treated on the Dermatology Ward of Medical University of Gdańsk

 and
and
Abstract
:1. Introduction
2. Results
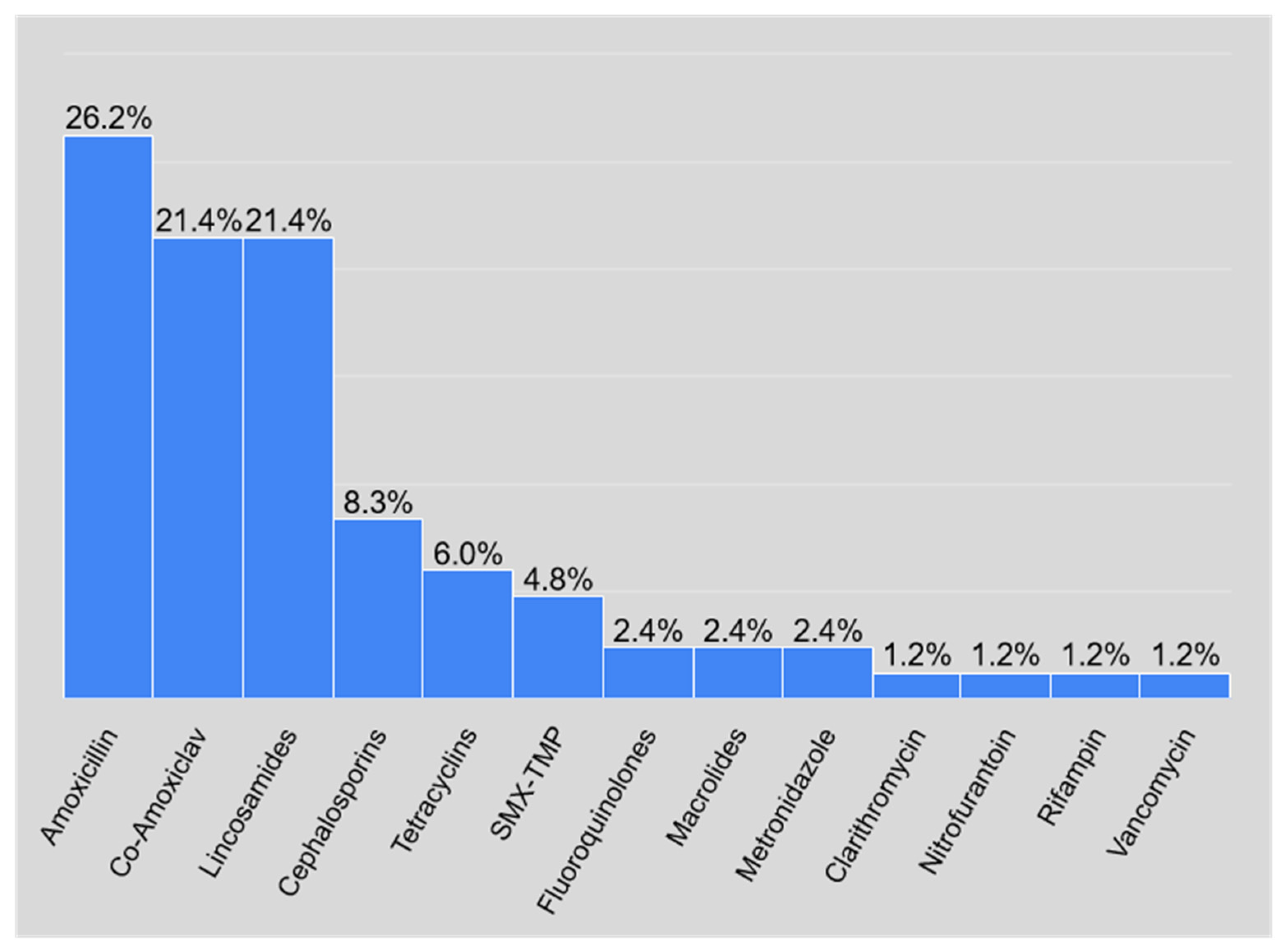
- Amoxicillin (22 cases, 26.2% of all reported cases).
- Amoxicillin–clavulanic acid and lincosamides (18 cases each, which accounted for 21.4% of all reported cases).
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. International Drug Monitoring: The role of National Centres. Report of a WHO Meeting; World Health Organization: Geneva, Switzerland, 1972. [Google Scholar]
- Nayak, S.; Acharjya, B. Adverse cutaneous drug reaction. Indian J. Dermatol. 2008, 53, 2–8. [Google Scholar] [CrossRef]
- Mockenhaupt, M. Epidemiology of cutaneous adverse drug reactions. Allergol. Sel. 2017, 1, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.J.; Chen, C.B.; Hung, S.I.; Ji, C.; Chung, W.H. Pharmacogenetic Testing for Prevention of Severe Cutaneous Adverse Drug Reactions. Front. Pharmacol. 2020, 11, 969. [Google Scholar] [CrossRef]
- Riedl, M.A.; Casillas, A.M. Adverse drug reactions: Types and treatment options. Am. Fam. Physician 2003, 68, 1781–1790. [Google Scholar]
- Lützow-Holm, C.; Rønnevig, J.R. Kutane legemiddelreaksjoner [Cutaneous drug reactions]. Tidsskr Nor Laegeforen. 2005, 22, 125. [Google Scholar]
- Blumenthal, K.G.; Peter, J.G.; Trubiano, J.A.; Phillips, E.J. Antibiotic allergy. Lancet 2019, 393, 183–198. [Google Scholar] [CrossRef]
- Thong, B.Y.; Tan, T.C. Epidemiology and risk factors for drug allergy. Br. J. Clin. Pharmacol. 2011, 71, 684–700. [Google Scholar] [CrossRef] [PubMed]
- Leong, K.P.; Thong, B.Y.; Cheng, Y.K.; Tang, C.Y.; Chng, H.H. Are there differences in drug allergy between the sexes? Ann. Acad. Med. Singap. 2003, 32, 151. [Google Scholar]
- Gerogianni, K.; Tsezou, A.; Dimas, K. Drug-Induced Skin Adverse Reactions: The Role of Pharmacogenomics in Their Prevention. Mol. Diagn. 2018, 22, 297–314. [Google Scholar] [CrossRef] [PubMed]
- Li, P.H.; Yeung, H.H.F.; Lau, C.S.; Au, E.Y.L. Prevalence, Incidence, and Sensitization Profile of β-lactam Antibiotic Allergy in Hong Kong. JAMA Netw. Open. 2020, 3, e204199. [Google Scholar] [CrossRef]
- Torres, M.J.; Blanca, M.; Fernandez, J.; Romano, A.; Weck, A.; Aberer, W.; Brockow, K.; Pichler, W.J.; Demoly, P.; ENDA; et al. Diagnosis of immediate allergic reactions to beta-lactam antibiotics. Allergy 2003, 58, 961–972. [Google Scholar] [CrossRef]
- Romano, A.; Blanca, M.; Torres, M.J.; Bircher, A.; Aberer, W.; Brockow, K.; Pichler, W.J.; Demoly, P.; ENDA; EAACI. Diagnosis of nonimmediate reactions to beta-lactam antibiotics. Allergy 2004, 59, 1153–1160. [Google Scholar] [CrossRef]
- Silviu Dan, F.; Mc Philips, S.; Warrington, R. The frequency of skin test reactions to side chain penicillin determinants. J. Allergy Clin. Immunol. 1993, 91, 694–701. [Google Scholar] [CrossRef]
- Weiss MAdkinson, N.F. Immediate hypersensitivity reactions to penicillin and related antibiotics. Clin. Allergy 1988, 18, 515–540. [Google Scholar] [CrossRef] [PubMed]
- Blanca, M. Allergic reactions to penicillins. A changing world? Allergy 1995, 50, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Blanca, M.; Torres, M.J. Reacciones de hipersensibilidad a antibióticos betalactámicos en la infancia [Hypersensitivity reactions to beta-lactam antibiotics in childhood]. Allergol. Immunopathol. 2003, 31, 103–109. (In Spanish) [Google Scholar] [CrossRef]
- Rosário, N.A.; Grumach, A.S. Allergy to beta-lactams in pediatrics: A practical approach. J. Pediatr. 2006, 82 (Suppl. 5), S181–S188. [Google Scholar] [CrossRef]
- Mulder, W.M.; Meinardi, M.M.; Bruynzeel, D.P. Huidreacties door geneesmiddelen [Cutaneous reactions to drugs]. Ned. Tijdschr. Geneeskd. 2004, 148, 415–420. (In Dutch) [Google Scholar]
- Goldberg, I.; Gilburd, B.; Shovman, O.; Brenner, S. Clinical and laboratory assays in the diagnosis of cutaneous adverse drug reactions. Isr. Med. Assoc. J. 2004, 6, 50–51. [Google Scholar]
- Halevy, S.; Cohen, A.D.; Grossman, N. [In vitro interferon-gamma release--a laboratory diagnosis of cutaneous adverse drug reactions]. Harefuah 2001, 140, 121–124, (In Dutch Hebrew). [Google Scholar]
- Halevy, S.; Cohen, A.D.; Grossman, N. Clinical implications of in vitro drug-induced interferon gamma release from peripheral blood lymphocytes in cutaneous adverse drug reactions. J. Am. Acad. Dermatol. 2005, 52, 254–261. [Google Scholar] [CrossRef]
- Pichichero, M.E. Use of selected cephalosporins in penicillin-allergic patients: A paradigm shift. Diagn. Microbiol. Infect. Dis. 2007, 57 (Suppl. 3), 13S–18S. [Google Scholar] [CrossRef] [PubMed]
- Verdier, L.; Bertho, G.; Gharbi-Benarous, J.; Girault, J.P. Lincomycin and clindamycin conformations. A fragment shared by macrolides, ketolides and lincosamides determined from TRNOE ribosome-bound conformations. Bioorg Med. Chem. 2000, 8, 1225–1243. [Google Scholar] [CrossRef]
- Kulczycka-Mierzejewska, K.; Trylska, J.; Sadlej, J. Quantum mechanical studies of lincosamides. J. Mol. Model. 2012, 18, 2727–2740. [Google Scholar] [CrossRef] [Green Version]
- Spížek, J.; Řezanka, T. Lincosamides: Chemical structure, biosynthesis, mechanism of action, resistance, and applications. Biochem. Pharmacol. 2017, 133, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.G.; Daum, R.S.; Creech, C.B.; Young, D.; Downing, M.D.; Eells, S.J.; Pettibone, S.; Hoagland, R.J.; Chambers, H.F.; DMID 07-0051 Team. Clindamycin versus trimethoprim-sulfamethoxazole for uncomplicated skin infections. N. Engl. J. Med. 2015, 372, 1093–1103. [Google Scholar] [CrossRef] [Green Version]
- Sulewski, R.J., Jr.; Blyumin, M.; Kerdel, F.A. Acute generalized exanthematous pustulosis due to clindamycin. Derm. Online J. 2008, 14, 14. [Google Scholar]
- Aiempanakit, K.; Apinantriyo, B. Clindamycin-induced acute generalized exanthematous pustulosis: A case report. Medicine 2020, 99, e20389. [Google Scholar] [CrossRef]
- Schwab, R.A.; Vogel, P.S.; Warschaw, K.E. Clindamycin-induced acute generalized exanthematous pustulosis. Cutis 2000, 65, 391–393. [Google Scholar]
- Rajgopal Bala, H.; Jalilian, C.; Goh, M.S.; Williams, R.; Tan, G.; Chong, A.H. Two cases of amoxycillin-induced follicular acute localised exanthematous pustulosis. Australas. J. Dermatol. 2017, 58, e23–e25. [Google Scholar] [CrossRef]
- Smeets, T.J.; Jessurun, N.; Härmark, L.; Kardaun, S.H. Clindamycin-induced acute generalised exanthematous pustulosis: Five cases and a review of the literature. Neth. J. Med. 2016, 74, 421–428. [Google Scholar] [PubMed]
- De Cruz, R.; Ferguson, J.; Wee, J.S.; Akhras, V. Acute localised exanthematous pustulosis (ALEP) induced by clindamycin in pregnancy. Australas. J. Dermatol. 2015, 56, e55–e58. [Google Scholar] [CrossRef] [PubMed]
- Nordeng, S.; Nordeng, H.; Høye, S. Bruk av antibiotika i svangerskapet [Use of antibiotics during pregnancy]. Tidsskr Nor Laegeforen. 2016, 136, 317–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muanda, F.T.; Sheehy, O.; Bérard, A. Use of antibiotics during pregnancy and risk of spontaneous abortion. CMAJ 2017, 189, E625–E633. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Class | Number | Cumulative Number | Percent | Cumulative Percent |
|---|---|---|---|---|
| Amoxicillin | 22 | 22 | 26.19048 | 26.1905 |
| Co-Amoxiclav | 18 | 47 | 21.42857 | 55.9524 |
| Lincosamides | 18 | 68 | 21.42857 | 80.9524 |
| Cephalosporins | 7 | 29 | 8.33333 | 34.5238 |
| Tetracyclines | 5 | 83 | 5.95238 | 98.8095 |
| SMX-TMP | 4 | 78 | 4.76190 | 92.8571 |
| Fluoroquinolones | 2 | 49 | 2.38095 | 58.3333 |
| Macrolides | 2 | 70 | 2.38095 | 83.3333 |
| Metronidazole | 2 | 72 | 2.38095 | 85.7143 |
| Clarithromycin | 1 | 50 | 1.19048 | 59.5238 |
| Nitrofurantoin | 1 | 73 | 1.19048 | 86.9048 |
| Rifampin | 1 | 74 | 1.19048 | 88.0952 |
| Vancomycin | 1 | 84 | 1.19048 | 100.0000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sokolewicz, E.M.; Rogowska, M.; Lewandowski, M.; Puchowska, M.; Piechota, D.; Barańska-Rybak, W. Antibiotic-Related Adverse Drug Reactions in Patients Treated on the Dermatology Ward of Medical University of Gdańsk. Antibiotics 2021, 10, 1144. https://doi.org/10.3390/antibiotics10101144
Sokolewicz EM, Rogowska M, Lewandowski M, Puchowska M, Piechota D, Barańska-Rybak W. Antibiotic-Related Adverse Drug Reactions in Patients Treated on the Dermatology Ward of Medical University of Gdańsk. Antibiotics. 2021; 10(10):1144. https://doi.org/10.3390/antibiotics10101144
Chicago/Turabian StyleSokolewicz, Ewa Maria, Martyna Rogowska, Miłosz Lewandowski, Monika Puchowska, Dorota Piechota, and Wioletta Barańska-Rybak. 2021. "Antibiotic-Related Adverse Drug Reactions in Patients Treated on the Dermatology Ward of Medical University of Gdańsk" Antibiotics 10, no. 10: 1144. https://doi.org/10.3390/antibiotics10101144