
Women’s Media Use and Preferences of Media-Based Interventions on Lifestyle-Related Risk Factors in Gynecological and Obstetric Care: A Cross-Sectional Multi-Center Study in Germany


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Population and Data Collection
2.3. Questionnaire
2.4. Dependent Variables
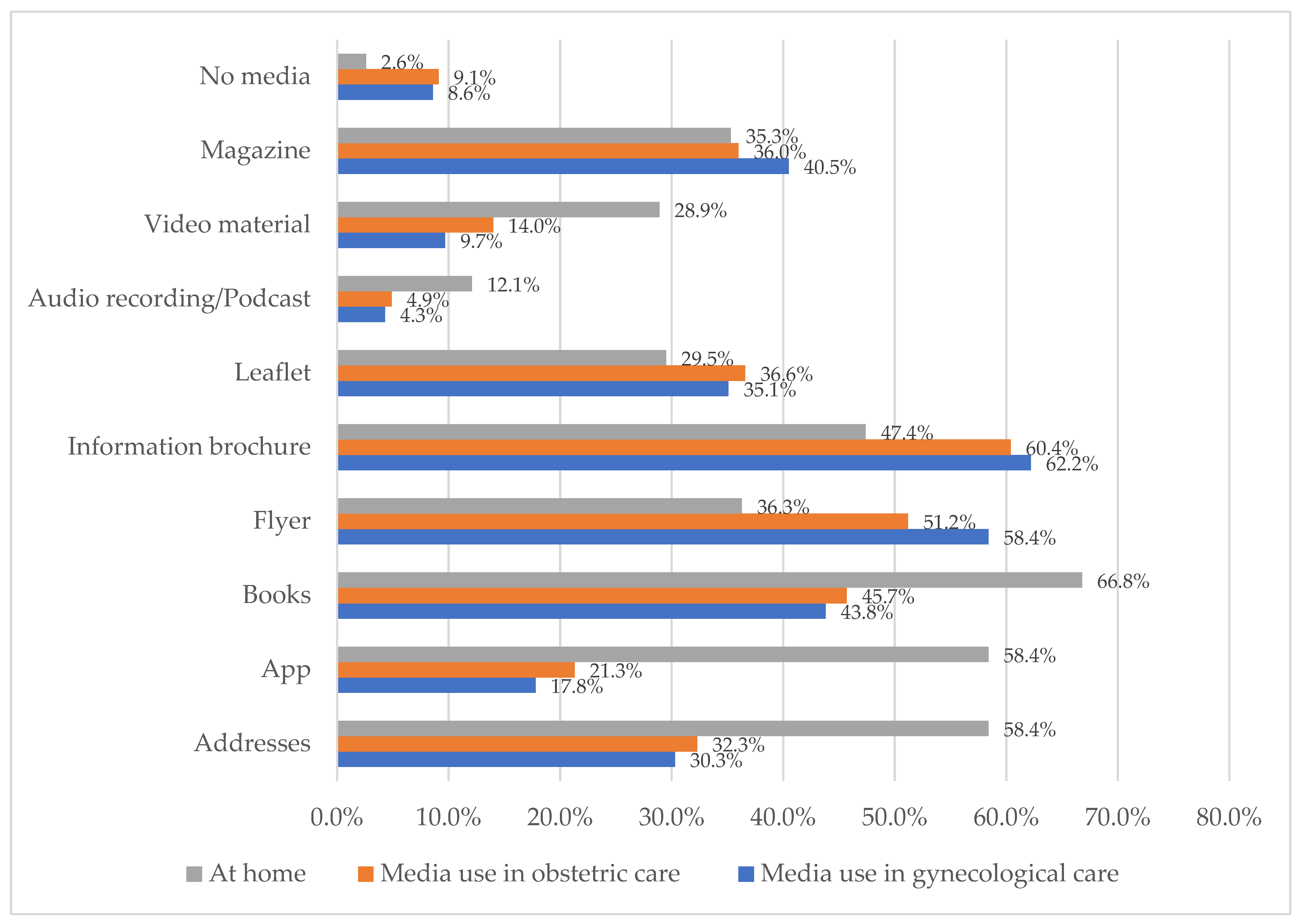
2.4.1. Women’s Media Use
2.4.2. Format Preferences of Media-Based Interventions
2.4.3. Content Preferences for Media-Based Interventions
2.5. Independent Variables
2.6. Statistical Analyses
3. Results
4. Discussion
4.1. Key Results
4.2. Discussion of the Key Results
4.3. Evaluation of Potential Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bell, K.; Corbacho, B.; Ronaldson, S.; Richardson, G.; Torgerson, D.; Robling, M.; on behalf of the Building Blocks Trial Group. The impact of pre and perinatal lifestyle factors on child long term health and social outcomes: A systematic review. Health Econ. Rev. 2018, 8, 2. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.H.; Chuang, L.M. Fetal exposure to parental smoking and the risk of type 2 diabetes: Are lifestyle-related factors more important? J. Diabetes Investig. 2016, 7, 472–475. [Google Scholar] [CrossRef] [Green Version]
- Flanigan, C.; Sheikh, A.; DunnGalvin, A.; Brew, B.K.; Alqvist, C.; Nwaru, B.I. Prenatal maternal psychosocial stress and offspring’s asthma and allergic disease: A systematic review and meta-analysis. Clin. Exp. Allergy 2018, 48, 403–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Napierala, M.; Mazela, J.; Merritt, T.A.; Florek, E. Tobacco smoking and breastfeeding: Effect on the lactation process, breast milk composition and infant development. A critical review. Environ. Res. 2016, 151, 321–338. [Google Scholar] [CrossRef]
- Greiner, T. Alcohol and Breastfeeding, a review of the issues. World Nutr. 2019, 10, 63–88. [Google Scholar] [CrossRef] [Green Version]
- Limichane, N.; Olsen, N.J.; Mortensen, E.L.; Obel, C.; Heitmann, B.L.; Händel, M.N. Associations between maternal stress during pregnancy and offspring obesity risk later in life—A systematic literature review. Obes. Rev. 2020, 21, e12951. [Google Scholar] [CrossRef]
- Míguez, M.C.; Vázquez, M.B. Risk factors for antenatal depression: A review. World J. Psychiatry 2021, 11, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, C.E.; Barry, C.; Sabhlok, A.; Russell, K.; Majors, A.; Kollins, S.H.; Fuemmeler, B.F. Maternal pre-pregnancy obesity and child neurodevelopmental outcomes: A meta-analysis. Obes. Rev. 2018, 19, 464–484. [Google Scholar] [CrossRef] [PubMed]
- Candido, A.C.; Morais, N.S.; Dutra, L.V.; Pinto, C.A.; Franceschini, S.D.C.C.; Alfenas, R.C.G. Insufficient iodine intake in pregnant women in different regions of the world: A systematic review. Arch. Endocrinol. Metab. 2019, 63, 306–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogne, T.; Tielemans, M.J.; Chong, M.F.-F.; Yajnik, C.S.; Krishnaveni, G.V.; Poston, L.; Jaddoe, V.W.V.; Steegers, E.A.P.; Joshi, S.; Chong, Y.-S.; et al. Maternal vitamin B12 in pregnancy and risk of preterm birth and low birth weight: A systematic review and individual participant data meta-analysis. Am. J. Epidemiol. 2017, 185, 212–223. [Google Scholar] [CrossRef] [Green Version]
- WHO Global Health Observatory (GHO) Data: Risk Factors. Available online: https://www.who.int/gho/ncd/risk_factors/en/ (accessed on 4 August 2021).
- WHO Lebensstilbedingte Faktoren, Die Den Vorzeitigen Tod Aufgrund Nicht-Übertragbarer Krankheiten Beeinflussen. Available online: https://www.euro.who.int/__data/assets/pdf_file/0006/381327/factsheet-lifestyle-ger.pdf (accessed on 4 August 2021).
- European Comission: EU Burden from Non-Communicable Diseases and Key Risk Factors. Available online: https://ec.europa.eu/jrc/en/health-knowledge-gateway/societal-impacts/burden (accessed on 4 August 2021).
- Mamluk, L.; Edwards, H.B.; Savović, J.; Leach, V.; Jones, T.; Moore, T.H.M.; Ijaz, S.; Lewis, S.J.; Donovan, J.L.; Lawlor, D.; et al. Low alcohol consumption and pregnancy and childhood outcomes: Time to change guidelines indicating apparently ‘safe’ levels of alcohol during pregnancy? A systematic review and meta-analyses. BMJ Open 2017, 7, e015410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittek, M.; Pfinder, M. Lebensstilbedingte Risiken in der Schwangerschaft und deren prä- und postnatalen Folgen. Gyn 2020, 25, 185–190. [Google Scholar]
- Wittek, M.; Svensson, L.; Pfinder, M. Lebensstilbedingte Risiken in der Stillzeit und deren Folgen. Gyn 2020, 25, 470–475. [Google Scholar]
- Oechsle, A.; Wensing, M.; Ullrich, C.; Bombana, M. Health Knowledge of Lifestyle-Related Risks during Pregnancy: A Cross-Sectional Study of Pregnant Women in Germany. Int. J. Environ. Res. Public Health 2020, 17, 8626. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Gesellschaft für Gynäkologie und Geburtshilfe; Arbeitsgemeinschaft Medizinrecht. Empfehlungen zu den ärztlichen Beratungs- und Aufkärungspflichten während der Schwangerenbertreuung und bei der Geburt. DGGG AGMedRecht. 2010. Available online: https://www.yumpu.com/de/document/read/5272683/download-pdf-datei-75-kb-dggg (accessed on 5 March 2021).
- Lange, A.; Kamtsiuris, P.; Lange, C.; Schaffrath, R.A.; Stolzenberg, H.; Lampert, T. Messung soziodemographischer Merkmale im Kinder- und Jugendgesundheitssurvey (KiGGS) und ihre Bedeutung am Beispiel der Einschätzung des allgemeinen Gesundheitszustands. Bundesgesundheitsbl-Gesundh.-Gesundh. 2007, 50, 578–589. [Google Scholar] [CrossRef]
- Winkler, J.; Stolzenberg, H. Adjustierung des Sozialen-Schicht- Index für die Anwendung im Kinder- und Jugendgesundheitssurvey (KiGGS). In Wismar Discussion Papers; 2009; Volume 7. Available online: http://hdl.handle.net/10419/39197 (accessed on 10 January 2021).
- Scheuch, E.K. Sozialprestige und soziale Schichtung. KZfSS 1970, 5, 65–103. [Google Scholar]
- Pfinder, M.; Liebig, S.; Feldmann, R. Adolescents’ use of alcohol, tobacco and il-licit drugs in relation to prenatal alcohol exposure: Modifications by gender and ethnicity. Alcohol Alcohol. 2014, 49, 143–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfinder, M.; Kunst, A.E.; Feldmann, R.; van Eijsden, M.; Vrijkotte, T.G.M. Educational differences in continuing or restarting drinking in early and late pregnancy: Role of psychological and physical problems. J. Stud. Alcohol Drugs 2014, 75, 47–55. [Google Scholar] [CrossRef]
- Van Velsen, L.; Beaujean, D.J.M.A.; van Gemert-Pijnen, J.E.W.C. Why mobile health app overload drives us crazy, and how to restore the sanity. BMC Med. Inform. Decis. Mak. 2013, 13, 23. [Google Scholar] [CrossRef] [Green Version]
- Tripp, N.; Hainey, K.; Liu, A.; Poulton, A.; Peek, M.; Kim, J.; Nanan, R. An emerging model of maternity care: Smartphone, midwife, doctor? Women Birth 2014, 27, 64–67. [Google Scholar] [CrossRef]
- Calvillo, J.; Román, I.; Roa, L.M. How technology is empowering patients? A literature review. Health Expect. 2015, 18, 643–652. [Google Scholar] [CrossRef] [Green Version]
- Vo, V.; Auroy, L.; Sarradon-Eck, A. Patients’ Perceptions of mHealth Apps: Meta-Ethnographic Review of Qualitative Studies. JMIR mHealth uHealth 2019, 7, e13817. [Google Scholar] [CrossRef] [Green Version]
- Womack, J.J.; Anderson, L.N.; Ledford, C.J.W. Presence of Complex and Potentially Conflicting Information in Prenatal Mobile Apps. Health Promot. Pract. 2020, 21, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.G.; Simões, P.; Queirós, A.; Rodrigues, M.; Rocha, N.P. Mobile apps to quantify aspects of physical activity: A systematic review on its reliability and validity. J. Med. Syst. 2020, 44, 51. [Google Scholar] [CrossRef]
- Paulovich, B. Design to Improve the Health Education Experience: Using participatory design methods in hospitals with clinicians and patients. Visible Lang. 2015, 49, 144–159. [Google Scholar]
- Egbert, N.; Nanna, K. Health Literacy: Challenges and Strategies. OJIN 2009, 14. [Google Scholar] [CrossRef]
- Sustersic, M.; Gauchet, A.; Foote, A.; Bosson, J.L. How best to use and evaluate Patient Information Leaflets given during a consultation: A systematic review of literature reviews. Health Expect. 2017, 20, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, B.; Tendais, I.; Dias, C.C. Maternal Adjustment and Maternal Attitudes in Adolescent and Adult Pregnant Women. J. Pediatr. Adolesc. Gynecol. 2014, 27, 194–201. [Google Scholar] [CrossRef] [Green Version]
- Klein, J.; von dem Knesebeck, O. Inequalities in health care utilization among migrants and non-migrants in Germany: A systematic review. Int. J. Equity Health 2018, 17, 160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lebano, A.; Hamed, S.; Bradby, H.; Gil-Salmerón, A.; Durá-Ferrandis, E.; Garcés-Ferrer, J.; Azzedine, F.; Riza, E.; Karnaki, P.; Zota, D.; et al. Migrants’ and refugees’ health status and healthcare in Europe: A scoping literature review. BMC Public Health 2020, 20, 1039. [Google Scholar] [CrossRef]
- Wild, F. Ausgaben der Privatversicherten für Ambulante Hebammenleistungen; WIP-Wissenschaftliches Institut der PKV: Köln, Germany, 2015. [Google Scholar]
- Stacey, D.; Légaré, F.; Lewis, K.; Barry, M.J.; Bennett, C.L.; Eden, K.B.; Holmes-Rovner, M.; Llewellyn-Thomas, H.; Lyddiatt, A.; Thomson, R.; et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst. Rev. 2017, 4, CD001431. [Google Scholar] [CrossRef] [Green Version]
- LaRose, J.G.; Guthrie, K.M.; Lanoye, A.; Tate, D.F.; Robichaud, E.; Caccavale, L.J.; Wing, R.R. A mixed methods approach to improving recruitment and engagement of emerging adults in behavioural weight loss programs. Obes. Sci. Pract. 2016, 2, 341–354. [Google Scholar] [CrossRef]
- Weymann, N.; Härter, M.; Petrak, F.; Dirmaier, J. Health information, behavior change, and decision support for patients with type 2 diabetes: Development of a tailored, preference-sensitive health communication application. Patient Prefer. Adher. 2013, 7, 1091–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuciforo, E.V. Russian toasting and drinking as communication ritual. Russ. J. Commun. 2013, 5, 161–175. [Google Scholar] [CrossRef]
- Kristjanson, A.F.; Wilsnack, S.C.; Zvartau, E.; Tsoy, M.; Novikov, B. Alcohol Use in Pregnant and Nonpregnant Russian Women. Alcohol. Clin. Exp. Res. 2007, 31, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Pfinder, M.; Lhachimi, S. Lifestyle-related risk factors during pregnancy: Even low-to-moderate drinking during pregnancy increases the risk for adolescent behavioral problems. J. Subst. Use 2020, 25, 135–140. [Google Scholar] [CrossRef]
- Patel, B.B.; Gurmeet, P.; Sinalkar, D.R.; Pandya, K.H.; Mahen, A.; Singh, N. A study on knowledge and practices of antenatal care among pregnant women attending antenatal clinic at a Tertiary Care Hospital of Pune, Maharashtra. Med. J. Dr. DY Patil Univ. 2016, 9, 354–362. [Google Scholar] [CrossRef]
- Essex, C.; Counsell, A.M.; Geddis, D.C. The demographic characteristics of early and late attenders for antenatal care. Aust. N. Z. J. Obstet. Gynaecol. 1992, 32, 306–308. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics (N = 219) | Total |
|---|---|
| % (n)/M (SD) | |
| Currently pregnant (yes, in %) | 57.8% (n = 126) |
| Currently lactating (yes, in %)) | 17.1% (n = 37) |
| Firm relationship (yes, in %) | 91.7% (n = 176) |
| Age (M (SD)) | 30.97 (5.516) |
| Socioeconomic status | |
| High (in %) | 46.2% (n = 84) |
| Middle (in %) | 41.8% (n = 76) |
| Low (in %) | 12.1% (n = 22) |
| Ethnicity | |
| German (in %) | 81.5% (n = 150) |
| Others (in %) | 18.5% (n = 34) |
| Health insurance status | |
| Private (in %) | 14.8% (n = 27) |
| Statutory (in %) | 79.1% (n = 144) |
| Others/None (in %) | 6.0% (n = 11) |
| Independent Variables | Media Use Regarding Health-Related Behaviors during Pregnancy | Media Use Regarding Health-Related Behaviors during Lactation | ||||
|---|---|---|---|---|---|---|
| % or M (SD) | OR (95% CI) | % or M (SD) | OR (95% CI) | |||
| Media Use (n = 157) | No Media Use (n = 43) | (n = 166) | Media Use (n = 157) | No Media Use (n = 43) | (n = 166) | |
| Currently pregnant | ||||||
| Yes | 98.1% | 1.9% | 1 | |||
| No | 76.5% | 23.5% | 0.30 (0.13, 0.67) ** | |||
| Currently lactating | ||||||
| Yes | 84.4% | 15.6% | 1 | |||
| No | 71.6% | 28.4% | 0.21 (0.05, 0.98) * | |||
| Firm relationship | ||||||
| Yes | 89.7% | 10.3% | 1 | 73.9% | 26.1% | 1 |
| No | 66.7% | 33.3% | 0.53 (0.13, 2.10) | 58.3% | 41.7% | 0.77 (0.19, 3.03) |
| Age | 31.8 (4.8) | 28.6 (5.9) | 1.11 (1.02, 1.21) * | 31.9 (4.7) | 29.3 (5.7) | 1.08 (1.00, 1.17) * |
| Socioeconomic status | ||||||
| High | 91.7% | 8.3% | 1 | 74.7% | 25.3% | 1 |
| Middle | 86.7% | 13.3% | 0.84 (0.35, 1.99) | 71.4% | 28.6% | 1.02 (0.46, 2.27) |
| Low | 82.4% | 17.6% | 1.95 (0.39, 9.86) | 66.7% | 33.3% | 0.97 (0.22, 4.28) |
| Ethnicity | ||||||
| German | 86.8% | 13.2% | 1 | 72.9% | 27.1% | 1 |
| Non-German | 93.1% | 6.9% | 1.29 (0.44, 3.79) | 68.8% | 31.2% | 0.80 (0.32, 2.00) |
| Health insurance | ||||||
| Private | 95.2% | 4.8% | 1 | 70.8% | 29.2% | 1 |
| Statutory | 86.9% | 13.1% | 1.24 (0.38, 4.01) | 73.2% | 26.8% | 1.42 (0.46, 4.38) |
| Others/None | 85.7% | 14.3% | 0.38 (0.07; 2.11) | 60.9% | 40.0% | 0.51 (0.09, 2.83) |
| Nagelkerkes R2 | 0.195 | 0.122 | ||||
| Independent Variables | Media in Gynecological Care | Media in Obstetric Care | Media at Home | ||||
|---|---|---|---|---|---|---|---|
| Information Brochures (n = 163) | Flyers (n = 163) | Information Brochures (n = 168) | Flyers (n = 145) | Books (n = 167) | Addresses (n = 167) | Apps (n = 167) | |
| Currently pregnant | |||||||
| Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | 1.85 (0.77, 4.41) | 1.43 (0.63, 3.25) | 3.26 (1.29, 8.20) ** | 0.98 (0.42, 2.28) | 1.24 (0.54, 2.81) | 0.81 (0.36, 1.83) | 0.44 (0.20, 1.00) * |
| Currently lactating | |||||||
| Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | 1.60 (0.49, 5.24) | 0.96 (0.31, 2.98) | 2.76 (0.83, 9.22) | 0.57 (0.18, 1.79) | 1.35 (0.43, 4.21) | 0.83 (0.27, 2.53) | 0.54 (0.17, 1.65) |
| Firm relationship | |||||||
| Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | 0.43 (0.11, 1.66) | 1.83 (0.44, 7.53) | 0.23 (0.06, 0.95) * | 1.61 (0.38, 6.78) | 1.69 (0.43, 6.55) | 1.06 (0.30, 3.78) | 1.51 (0.42, 5.48) |
| Age | 0.92 (0.86, 0.99) * | 0.95 (0.89, 1.02) | 0.91 (0.85, 0.97) ** | 0.96 (0.89, 1.03) | 1.00 (0.94, 1.06) | 0.95 (0.89, 1.01) | 0.96 (0.90, 1.03) |
| Socioeconomic status | |||||||
| High | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Middle | 0.84 (0.41, 1.75) | 1.71 (0.84, 3.48) | 0.66 (0.32, 1.37) | 2.21 (1.05, 4.66) * | 0.54 (0.26, 1.12) | 0.29 (0.13, 0.61) *** | 0.81 (0.39, 1.66) |
| Low | 0.36 (0.10, 1.29) | 2.08 (0.59, 7.31) | 0.47 (0.13, 1.72) | 0.48 (0.11, 2.00) | 0.43 (0.13, 1.45) | 0.20 (0.06, 0.70) ** | 0.58 (0.16, 2.02) |
| Ethnicity | |||||||
| German | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Non-German | 0.42 (0.18, 0.99) * | 1.16 (0.49, 2.75) | 0.38 (0.16, 0.89) * | 0.71 (0.28, 1.76) | 0.86 (0.37, 2.02) | 1.80 (0.72, 4.49) | 0.28 (0.12, 0.67) ** |
| Health insurance | |||||||
| Private | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Statutory | 0.51 (0.17, 1.48) | 2.00 (0.73, 5.46) | 0.90 (0.34, 2.42) | 0.57 (0.20, 1.60) | 0.97 (0.36, 2.66) | 2.72 (1.00, 7.45) * | 2.73 (1.03, 7.22) * |
| Others/None | 0.16 (0.32, 0.78) * | 4.34 (0.92, 20.42) | 0.28 (0.06, 1.36) | 0.49 (0.11, 2.25) | 2.08 (0.35, 12.49) | 0.60 (0.13, 2.88) | 2.31 (0.50, 10.61) |
| Nagelkerkes R2 | 0.139 | 0.102 | 0.186 | 0.105 | 0.047 | 0.165 | 0.134 |
| Independent Variables | Recommendations for Healthy Lifestyle/Behaviors | Recommendations for Avoidance of Lifestyle-Related Risks/Behaviors | Information on Potential Lifestyle-Related Risks | Recipes for Cooking | ||||
|---|---|---|---|---|---|---|---|---|
| During Pregnancy (n = 167) | During Lactation (n = 159) | During Pregnancy (n = 167) | During Lactation (n = 159) | During Pregnancy (n = 167) | During Lactation (n = 159) | During Pregnancy (n = 167) | During Lactation (n = 159) | |
| % (n) of women who prefer media content | 80.1% (n = 149) | 79.0% (n = 139) | 47.3% (n = 88) | 47.7% (n = 84) | 46.2% (n = 86) | 43.2% (n = 76) | 33.3% (n = 62) | 43.8% (n = 77) |
| Currently pregnant | ||||||||
| Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | 1.18 (0.41, 3.44) | 0.66 (0.25, 1.78) | 0.85 (0.39, 1.86) | 1.01 (0.46, 2.23) | 0.86 (0.40, 1.85) | 0.67 (0.30, 1.50) | 1.47 (0.67, 3.24) | 1.68 (0.75, 3.81) |
| Currently lactating | ||||||||
| Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | 2.93 (0.84, 10.24) | 1.51 (0.45, 5.03) | 0.54 (0.19, 1.54) | 0.98 (0.35, 2.76) | 2.08 (0.72, 6.02) | 1.47 (0.49, 4.40) | 2.31 (0.75, 7.15) | 4.61 (1.44, 14.74) ** |
| Firm relationship | ||||||||
| Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | a | 1.74 (0.33, 9.34) | 2.18 (0.61, 7.81) | 0.85 (0.25, 2.95) | 1.07 (0.31, 3.71) | 1.03 (0.29, 3.67) | 0.33 (0.08, 1.33) | 0.34 (0.09, 1.30) |
| Age | 0.93 (0.85, 1.20) | 0.91 (0.84, 0.99) * | 0.99 (0.93, 1.06) | 1.01 (0.94, 1.08) | 0.97 (0.91, 1.03) | 1.01 (0.94, 1.07) | 1.00 (0.94, 1.07) | 1.06 (0.99, 1.14) |
| Socioeconomic status | ||||||||
| High | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Middle | 0.81 (0.34, 1.94) | 0.91 (0.37, 2.24) | 0.58 (0.29, 1.17) | 0.82 (0.41, 1.64) | 1.24 (0.62, 2.47) | 1.07 (0.52, 2.18) | 1.74 (0.83, 3.64) | 1.67 (0.81, 3.46) |
| Low | 0.98 (0.16, 6.23) | 0.17 (0.04, 0.78) * | 0.24 (0.06, 0.90) * | 1.09 (0.31, 3.89) | 0.96 (0.28, 3.32) | 1.58 (0.43, 5.71) | 3.67 (1.02, 13.26) * | 6.30 (1.54, 25.84) ** |
| Ethnicity | ||||||||
| German | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Non-German | 0.31 (0.11, 0.83) * | 0.53 (0.19, 1.49) | 0.64 (0.27, 1.47) | 0.49 (0.21, 1.18) | 0.58 (0.25, 1.37 | 0.54 (0.22, 1.31) | 1.07 (0.44, 2.57) | 0.86 (0.35, 2.12) |
| Health insurance | ||||||||
| Private | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Statutory | 0.16 (0.02, 1.28) | 0.37 (0.08, 1.80) | 1.27 (0.49, 3.28) | 1.11 (0.42, 2.92) | 0.53 (0.20, 1.39) | 0.61 (0.23, 1.64) | 0.92 (0.33, 2.56) | 0.90 (0.33, 2.52) |
| Others/None | 0.60 (0.03, 11.20) | 0.39 (0.04, 3.48) | 0.19 (0.03, 1.13) | 0.25 (0.04, 1.49) | 0.24 (0.05, 1.21) | 0.09 (0.01, 0.91) * | 0.86 (0.17, 4.42) | 0.67 (0.12, 3.77) |
| Nagelkerkes R2 | 0.217 | 0.136 | 0.103 | 0.052 | 0.078 | 0.093 | 0.072 | 0.134 |
| Independent Variables | Movement Exercises | Relaxation Exercises | Potential Alternatives to Tobacco and Alcohol | Recommendations for Avoidance of Specific Medications | Recommendations for Essential Supplements | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| During Pregnancy (n = 167) | During Lactation (n = 159) | During Pregnancy (n = 167) | During Lactation (n = 159) | During Pregnancy (n = 168) | During Lactation (n = 159) | During Pregnancy (n = 167) | During Lactation (n = 159) | During Pregnancy (n = 167) | During Lactation (n = 159) | |
| % (n) of women who prefer media content | 59.7% (n = 111) | 40.3% (n = 71) | 55.4% (n = 103) | 46.6% (n = 82) | 17.1% (n = 33) | 21.0% (n = 37) | 59.1% (n = 110) | 58.0% (n = 102) | 48.4% (n = 90) | 47.2% (n = 83) |
| Currently pregnant | ||||||||||
| Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | 0.86 (0.38, 1.95) | 1.07 (0.48, 2.39) | 1.19 (0.55, 2.57) | 1.44 (0.66, 3.16) | 0.33 (0.13, 0.86) * | 3.09 (1.20, 7.90) * | 3.29 (1.24, 8.71) * | 1.62 (0.71, 3.69) | 2.43 (1.07, 5.53) * | 1.80 (0.80, 4.06) |
| Currently lactating | ||||||||||
| Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | 1.49 (0.51, 4.36) | 1.15 (0.41, 3.25) | 1.56 (0.55, 4.42) | 0.86 (0.31, 2.41) | 0.81 (0.24, 2.74) | 1.33 (0.41, 4.37) | 1.19 (0.35, 4.10) | 1.13 (0.39, 3.27) | 1.89 (0.64, 5.63) | 1.38 (0.48, 3.97) |
| Firm relationship | ||||||||||
| Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | 0.47 (0.13, 1.70) | 0.15 (0.03, 0.82) * | 0.95 (0.27, 3.31) | 0.41 (0.12, 1.49) | 3.01 (0.55, 16.33) | 0.42 (0.08, 2.13) | 0.33 (0.06, 1.80) | 0.52 (0.14, 1.96) | 0.45 (0.12, 1.62) | 0.48 (0.13, 1.76) |
| Age | 0.99 (0.93, 1.06) | 1.06 (0.98, 1.13) | 1.01 (0.95, 1.08) | 1.01 (0.95, 1.08) | 1.07 (0.98, 1.16) | 0.92 (0.84, 1.01) | 0.94 (0.86, 1.03) | 0.95 (0.89, 1.02) | 0.94 (0.88, 1.01) | 1.00 (0.94, 1.07) |
| Socioeconomic status | ||||||||||
| High | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Middle | 3.45 (1.64, 7.25) *** | 1.35 (0.66, 2.75) | 0.61 (0.30, 1.21) | 0.89 (0.44, 1.78) | 0.39 (0.15, 1.04) | 1.28 (0.53, 3.09) | 3.03 (1.09, 8.43) * | 0.80 (0.40, 1.61) | 0.64 (0.31, 1.30) | 0.70 (0.34, 1.43) |
| Low | 2.57 (0.71, 9.24) | 2.52 (0.63, 10.01) | 0.61 (0.18, 2.10) | 1.18 (0.33, 4.22) | 0.19 (0.04, 0.92) * | 1.01 (0.19, 5.23) | 6.55 (1.28, 33.44) * | 2.61 (0.58, 11.68) | 0.47 (0.13, 1.72) | 0.98 (0.27, 3.54) |
| Ethnicity | ||||||||||
| German | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Non-German | 1.04 (0.44, 2.46) | 0.92 (0.37, 2.25) | 1.46 (0.64, 3.34) | 0.86 (0.36, 2.03) | 8.97 (1.12, 71.54) * | 0.21 (0.04, 0.96) * | 0.12 (0.01, 0.93) * | 0.82 (0.34, 1.97) | 0.55 (0.23, 1.29) | 0.43 (0.17, 1.08) |
| Health insurance | ||||||||||
| Private | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Statutory | 0.25 (0.08, 0.77) * | 0.86 (0.31, 2.33) | 1.98 (0.72, 5.43) | 0.90 (0.34, 2.39) | 1.76 (0.52, 5.94) | 1.67 (0.43, 6.50) | 0.51 (0.15, 1.76) | 0.78 (0.28, 2.12) | 0.25 (0.08, 0.77) * | 0.37 (0.13, 1.06) |
| Others/None | 0.20 (0.04, 1.02) | 0.53 (0.10, 2.78) | 4.21 (0.90, 19.68) | 0.38 (0.07, 2.02) | 0.69 (0.12, 4.04) | 2.88 (0.42, 19.70) | 1.48 (0.25, 8.92) | 0.77 (0.15, 3.88) | 0.09 (0.02, 0.50) ** | 0.44 (0.08, 2.33) |
| Nagelkerkes R2 | 0.143 | 0.082 | 0.057 | 0.041 | 0.232 | 0.175 | 0.252 | 0.065 | 0.158 | 0.100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bombana, M.; Wittek, M.; Müller, G.; Heinzel-Gutenbrunner, M.; Wensing, M. Women’s Media Use and Preferences of Media-Based Interventions on Lifestyle-Related Risk Factors in Gynecological and Obstetric Care: A Cross-Sectional Multi-Center Study in Germany. Int. J. Environ. Res. Public Health 2021, 18, 9840. https://doi.org/10.3390/ijerph18189840
Bombana M, Wittek M, Müller G, Heinzel-Gutenbrunner M, Wensing M. Women’s Media Use and Preferences of Media-Based Interventions on Lifestyle-Related Risk Factors in Gynecological and Obstetric Care: A Cross-Sectional Multi-Center Study in Germany. International Journal of Environmental Research and Public Health. 2021; 18(18):9840. https://doi.org/10.3390/ijerph18189840
Chicago/Turabian StyleBombana, Manuela, Maren Wittek, Gerhard Müller, Monika Heinzel-Gutenbrunner, and Michel Wensing. 2021. "Women’s Media Use and Preferences of Media-Based Interventions on Lifestyle-Related Risk Factors in Gynecological and Obstetric Care: A Cross-Sectional Multi-Center Study in Germany" International Journal of Environmental Research and Public Health 18, no. 18: 9840. https://doi.org/10.3390/ijerph18189840