
Fear of COVID-19 in Patients with Acute Myocardial Infarction

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population Characteristics
2.2. Criteria of Patient Eligibility
2.3. Fear of COVID-19 Scale
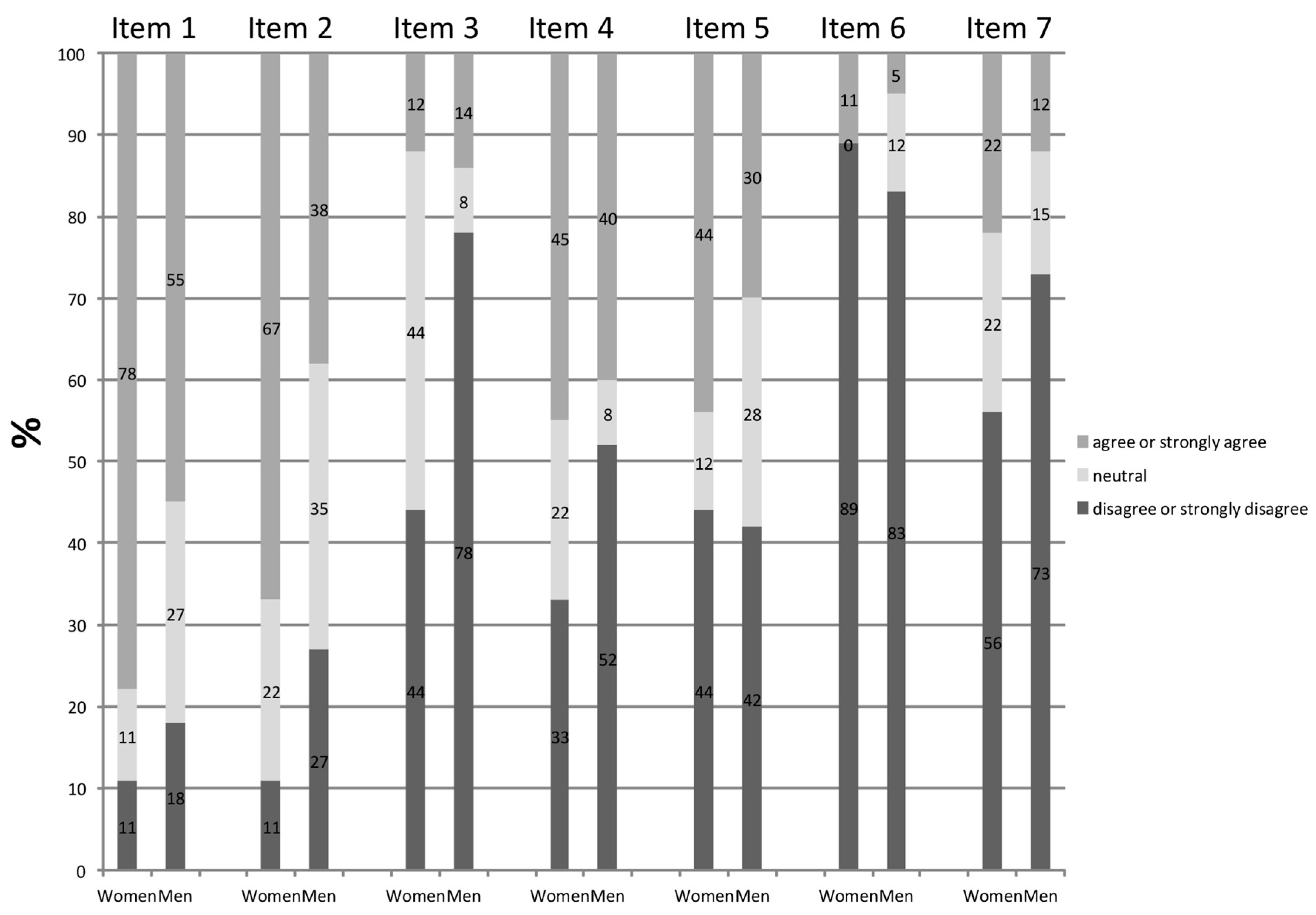
- I am most afraid of coronavirus;
- It makes me uncomfortable to think about coronavirus;
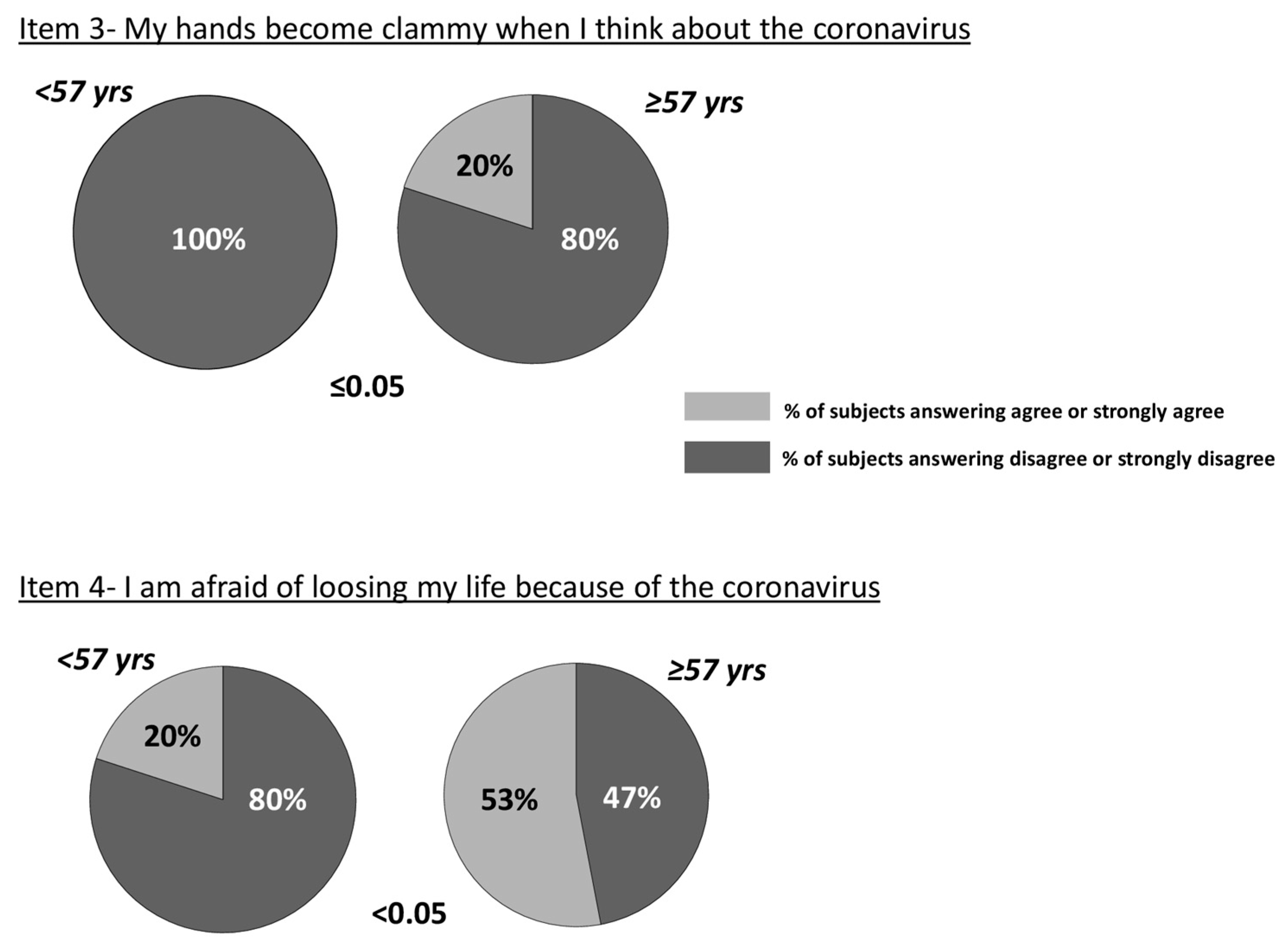
- My hands become clammy when I think about coronavirus;
- I am afraid of losing my life because of coronavirus;
- When I watch news and stories about coronavirus on social media, I become nervous or anxious;
- I cannot sleep because I’m worrying about getting coronavirus;
- My heart races or palpitates when I think about getting coronavirus.
2.4. Statistical Analysis
3. Results
3.1. Total FCV-19S Score
3.2. FCV-19S Items
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Helal, A.; Shahin, L.; Abdelsalam, M.; Ibrahim, M. Global effect of COVID-19 pandemic on the rate of acute coronary syndrome admissions: A comprehensive review of published literature. Open Heart 2021, 8, e001645. [Google Scholar] [CrossRef] [PubMed]
- Gorini, F.; Chatzianagnostou, K.; Mazzone, A.; Bustaffa, E.; Esposito, A.; Berti, S.; Bianchi, F.; Vassalle, C. “Acute Myocardial Infarction in the Time of COVID-19”: A Review of Biological, Environmental, and Psychosocial Contributors. Int. J. Environ. Res. Public Health 2020, 17, 7371. [Google Scholar] [CrossRef]
- Tam, C.F.; Cheung, K.S.; Lam, S.; Wong, A.; Yung, A.; Sze, M.; Lam, Y.M.; Chan, C.; Tsang, T.C.; Tsui, M.; et al. Impact of Coronavirus Disease 2019 (COVID-19) Outbreak on ST-Segment-Elevation Myocardial Infarction Care in Hong Kong, China. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e006631. [Google Scholar] [CrossRef] [PubMed]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 27, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. Development and initial validation of the COVID Stress Scales. J. Anxiety Disord. 2020, 72, 102232. [Google Scholar] [CrossRef] [PubMed]
- Sakib, N.; Bhuiyan, A.K.M.I.; Hossain, S.; Al Mamun, F.; Hosen, I.; Abdullah, A.H.; Sarker, M.A.; Mohiuddin, M.S.; Rayhan, I.; Hossain, M.; et al. Psychometric Validation of the Bangla Fear of COVID-19 Scale: Confirmatory Factor Analysis and Rasch Analysis. Int. J. Ment. Health Addict. 2020, 11, 1–12. [Google Scholar] [CrossRef]
- Reznik, A.; Gritsenko, V.; Konstantinov, V.; Khamenka, N.; Isralowitz, R. COVID-19 Fear in Eastern Europe: Validation of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Soraci, P.; Ferrari, A.; Abbiati, F.A.; Del Fante, E.; De Pace, R.; Urso, A.; Griffiths, M.D. Validation and Psychometric Evaluation of the Italian Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 1–10. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Finset, A.; Bosworth, H.; Butow, P.; Gulbrandsen, P.; Hulsman, R.L.; Pieterse, A.H.; Street, R.; Tschoetschel, R.; van Weert, J. Effective health communication—A key factor in fighting the COVID-19 pandemic. Patient Educ. Couns. 2020, 103, 873–876. [Google Scholar] [CrossRef]
- De Rosa, S.; Spaccarotella, C.; Basso, C.; Calabrò, M.P.; Curcio, A.; Filardi, P.P.; Mancone, M.; Mercuro, G.; Muscoli, S.; Nodari, S.; et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur. Heart J. 2020, 41, 2083–2088, Erratum in Eur. Heart J. 2021, 42, 683. Erratum in Eur. Heart J. 2021, 42, 322. [Google Scholar] [CrossRef]
- Matsushita, K.; Hess, S.; Marchandot, B.; Sato, C.; Truong, D.P.; Kim, N.T.; Weiss, A.; Jesel, L.; Ohlmann, P.; Morel, O. Clinical features of patients with acute coronary syndrome during the COVID-19 pandemic. J. Thromb. Thrombolysis 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.K.; Paik, J.H.; Lee, Y.J.; Kang, S. Impact of the COVID-19 Outbreak on Emergency Care Utilization in Patients with Acute Myocardial Infarction: A Nationwide Population-based Study. J. Korean Med. Sci. 2021, 36, e111. [Google Scholar] [CrossRef] [PubMed]
- Pessoa-Amorim, G.; Camm, C.F.; Gajendragadkar, P.; De Maria, G.L.; Arsac, C.; Laroche, C.; Zamorano, J.L.; Weidinger, F.; Achenbach, S.; Maggioni, A.P.; et al. Admission of patients with STEMI since the outbreak of the COVID-19 pandemic: A survey by the European Society of Cardiology. Eur. Heart J. Qual. Care Clin. Outcomes 2020, 6, 210–216. [Google Scholar] [CrossRef]
- Miličić, D.; Brajković, L.; Maček, J.L.; Andrić, A.; Ardalić, Ž.; Buratović, T.; Marčinko, D. Type a Personality, Stress, Anxiety and Health Locus of Control in Patients with Acute Myocardial Infarction. Psychiatr. Danub. 2016, 28, 409–414. [Google Scholar] [PubMed]
- Khan, M.A.; Karamat, M.; Hafizullah, M.; Nazar, Z.; Fahim, M.; Gul, A.M. Frequency of anxiety and psychosocial stressful events in patients with acute myocardial infraction. J. Ayub. Med. Coll. Abbottabad. 2010, 22, 32–35. [Google Scholar] [PubMed]
- Aldujeli, A.; Hamadeh, A.; Briedis, K.; Tecson, K.M.; Rutland, J.; Krivickas, Z.; Stiklioraitis, S.; Briede, K.; Aldujeili, M.; Unikas, R.; et al. Delays in Presentation in Patients with Acute Myocardial Infarction During the COVID-19 Pandemic. Cardiol. Res. 2020, 11, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Sareen, J.; Erickson, J.; Medved, M.I.; Asmundson, G.J.; Enns, M.W.; Stein, M.; Leslie, W.; Doupe, M.; Logsetty, S. Risk factors for post-injury mental health problems. Depress. Anxiety 2013, 30, 321–327. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Policy Brief: COVID-19 and the Need for Action on Mental Health. Available online: https://unsdg.un.org/sites/default/files/2020-05/UN-Policy-Brief-COVID-19-and-mental-health.pdf (accessed on 25 June 2021).
- Chang, K.C.; Kuo, Y.J.; Soraci, P.; Scarf, D.; Broström, A.; Griffiths, M.D.; Pakpour, A.H. Fear of COVID-19 Scale (FCV-19S) across countries: Measurement invariance issues. Nurs. Open 2021, 8, 1892–1908. [Google Scholar] [CrossRef]
- Broche-Pérez, Y.; Fernández-Fleites, Z.; Jiménez-Puig, E.; Fernández-Castillo, E.; Rodríguez-Martin, B.C. Gender and Fear of COVID-19 in a Cuban Population Sample. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Długosz, P. Predictors of Mental Health after the First Wave of the COVID-19 Pandemic in Poland. Brain Sci. 2021, 11, 544. [Google Scholar] [CrossRef]
- Orrù, G.; Bertelloni, D.; Diolaiuti, F.; Conversano, C.; Ciacchini, R.; Gemignani, A. A Psychometric Examination of the Coronavirus Anxiety Scale and the Fear of Coronavirus Disease 2019 Scale in the Italian Population. Front. Psychol. 2021, 12, 669384. [Google Scholar] [CrossRef]
- Hossain, M.A.; Jahid, M.I.K.; Hossain, K.M.A.; Walton, L.M.; Uddin, Z.; Haque, M.O.; Kabir, M.F.; Arafat, S.M.Y.; Sakel, M.; Faruqui, R.; et al. Knowledge, attitudes, and fear of COVID-19 during the Rapid Rise Period in Bangladesh. PLoS ONE 2020, 15, e0239646. [Google Scholar] [CrossRef]
- Chi, X.; Chen, S.; Chen, Y.; Chen, D.; Yu, Q.; Guo, T.; Cao, Q.; Zheng, X.; Huang, S.; Hossain, M.M.; et al. Psychometric Evaluation of the Fear of COVID-19 Scale Among Chinese Population. Int. J. Ment. Health Addict. 2021, 1–16. [Google Scholar] [CrossRef]
- Yadav, U.N.; Yadav, O.P.; Singh, D.R.; Ghimire, S.; Rayamajhee, B.; Kanti Mistry, S.; Rawal, L.B.; Ali, A.M.; Kumar Tamang, M.; Mehta, S. Perceived fear of COVID-19 and its associated factors among Nepalese older adults in eastern Nepal: A cross-sectional study. PLoS ONE 2021, 16, e0254825. [Google Scholar] [CrossRef]
- Parlapani, E.; Holeva, V.; Nikopoulou, V.A.; Sereslis, K.; Athanasiadou, M.; Godosidis, A.; Stephanou, T.; Diakogiannis, I. Intolerance of Uncertainty and Loneliness in Older Adults During the COVID-19 Pandemic. Front. Psychiatry 2020, 11, 842. [Google Scholar] [CrossRef]
- Powell, T.; Bellin, E.; Ehrlich, A.R. Older adults and Covid-19: The most vulnerable, the hardest hit. Hast. Cent. Rep. 2020, 50, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Harper, C.A.; Satchell, L.P.; Fido, D.; Latzman, R.D. Functional Fear Predicts Public Health Compliance in the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2020, 1–14. [Google Scholar] [CrossRef]
- Rico-Uribe, L.A.; Caballero, F.F.; Martín-María, N.; Cabello, M.; Ayuso-Mateos, J.L.; Miret, M. Association of loneliness with all-cause mortality: A meta-analysis. PLoS ONE 2018, 13, e0190033. [Google Scholar] [CrossRef]
- Aguilera, G. Corticotropin releasing hormone, receptor regulation and the stress response. Trends Endocrinol. Metab. 1998, 9, 329–336. [Google Scholar] [CrossRef]
- Herman, J.P.; Adams, D.; Prewitt, C. Regulatory changes in neuroendocrine stress-integrative circuitry produced by a variable stress paradigm. Neuroendocrinology 1995, 61, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.N.; McLaughlin, R.J.; Bingham, B.; Shrestha, L.; Lee, T.T.; Gray, J.M.; Hillard, C.J.; Gorzalka, B.B.; Viau, V. Endogenous cannabinoid signaling is essential for stress adaptation. Proc. Natl. Acad. Sci. USA 2010, 107, 9406–9411. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves de Andrade, E.; Šimončičová, E.; Carrier, M.; Vecchiarelli, H.A.; Robert, M.È.; Tremblay, M.È. Microglia Fighting for Neurological and Mental Health: On the Central Nervous System Frontline of COVID-19 Pandemic. Front. Cell Neurosci. 2021, 15, 647378. [Google Scholar] [CrossRef]
- Lundblad, D.; Holmgren, L.; Jansson, J.H.; Näslund, U.; Eliasson, M. Gender differences in trends of acute myocardial infarction events: The Northern Sweden MONICA study 1985–2004. BMC Cardiovasc. Disord. 2008, 8, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Miguel-Yanes, J.M.; Jiménez-García, R.; Hernandez-Barrera, V.; de Miguel-Díez, J.; Muñoz-Rivas, N.; Méndez-Bailón, M.; Pérez-Farinós, N.; López-Herranz, M.; Lopez-de-Andres, A. Sex Differences in the Incidence and Outcomes of Acute Myocardial Infarction in Spain, 2016–2018: A Matched-Pair Analysis. J. Clin. Med. 2021, 10, 1795. [Google Scholar] [CrossRef]
- Chang, S.S.; Lin, S.Y.; Lai, J.N.; Chen, K.W.; Lu, C.R.; Chang, K.C.; Chiu, L.T.; Kao, C.H. Sex differences in long-term cardiovascular outcomes among patients with acute myocardial infarction: A population-based retrospective cohort study. Int. J. Clin. Pract. 2021, 75, e14066. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, S.; Ruthrof, S.; Nowak, K.; Alff, A.; Klinghammer, L.; Schneider, R.; Ludwig, J.; Pfahlberg, A.B.; Daniel, W.G.; Flachskampf, F.A. Short-term prognosis of contemporary interventional therapy of ST-elevation myocardial infarction: Does gender matter? Clin. Res. Cardiol. 2009, 98, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Tzur Bitan, D.; Grossman-Giron, A.; Bloch, Y.; Mayer, Y.; Shiffman, N.; Mendlovic, S. Fear of COVID-19 scale: Psychometric characteristics, reliability and validity in the Israeli population. Psychiatry Res. 2020, 289, 113100. [Google Scholar] [CrossRef] [PubMed]
- Finell, E.; Tiilikainen, M.; Jasinskaja-Lahti, I.; Hasan, N.; Muthana, F. Lived Experience Related to the COVID-19 Pandemic among Arabic-, Russian- and Somali-Speaking Migrants in Finland. Int. J. Environ. Res. Public Health 2021, 18, 2601. [Google Scholar] [CrossRef]
- Tan, J.H.; Tong, J.; Ho, H.H. Delayed presentation of acute coronary syndrome with mechanical complication during COVID-19 pandemic: A case report. Eur. Heart J. Case Rep. 2020, 5, ytaa506. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, L. The Untold Toll—The Pandemic’s Effects on Patients without Covid-19. N. Engl. J. Med. 2020, 382, 2368–2371. [Google Scholar] [CrossRef] [PubMed]
- Arrivi, A.; Dominici, M.; Bier, N.; Truglio, M.; Vaudo, G.; Pucci, G. Association Between Air Pollution and Acute Coronary Syndromes During Lockdown for COVID-19: Results from the Terni Hub Center. Front. Public Health. 2021, 9, 683683. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Overall Population | Women | Men | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Standard Deviation | Skewness | Kurtosis | Mean | Standard Deviation | Skewness | Kurtosis | Mean | Standard Deviation | Skewness | Kurtosis | |
| Item 1 | 3.7 | 1.1 | −0.5 | −0.6 | 4 | 1 | −0.8 | −0.2 | 3.6 | 1.2 | −0.4 | −0.6 |
| Item 2 | 3.6 | 1.1 | −0.4 | −0.6 | 3.8 | 0.97 | −0.4 | −0.6 | 3.2 | 1.1 | −0.1 | −0.7 |
| Item 3 | 2 | 1.2 | 0.5 | −0.5 | 2.4 | 1.3 | 0.46 | −0.5 | 1.9 | 1.1 | 1.2 | 0.5 |
| Item 4 | 2.9 | 1.4 | 0.1 | −1.4 | 3.1 | 1.3 | −0.2 | −1 | 2.9 | 1.4 | 0.2 | −1.4 |
| Item 5 | 2.8 | 1.3 | 0.1 | −1.1 | 3 | 1.6 | 0.1 | −1 | 2.8 | 1.3 | 0.1 | −1 |
| Item 6 | 1.8 | 0.9 | 1.3 | 1.6 | 2 | 1.2 | 1.7 | 2.2 | 1.7 | 0.9 | 1 | 0,3 |
| Item 7 | 2.1 | 1.2 | 1 | 0.2 | 2.6 | 1.6 | 0.6 | −1 | 2 | 1 | 1.1 | 0.4 |
| Total score | 18.5 | 6.6 | 0.4 | −0.4 | 20.7 | 7.4 | 0.5 | −0.4 | 18.2 | 6.5 | 0.4 | −0.5 |
| First Wave CV Outpatients | November 2020–May 2021 CV Outpatients | November 2020–May 2021 STEMI Patients | |
|---|---|---|---|
| Emotional fear reactions | |||
| 1. I am most afraid of the coronavirus | 3.5 (1.3) | 3.8 (1.3) | 3.7 (1.1) |
| 2. It makes me uncomfortable to think about the coronavirus | 3.2 (1.6) | 3.0 (1.2) | 3.3 (1.1) |
| 4. I am afraid of losing my life because of the coronavirus | 2.9 (1.6) | 2.7 (1.2) | 2.9 (1.4) |
| 5. When watching news and stories about the coronavirus on social media, I become nervous or anxious | 3.0 (1.8) | 2.4 (1.3) | 2.8 (1.3) |
| Symptomatic expression of fear | |||
| 3. My hands become clammy when I think about the coronavirus | 2.1 (0.7) | 1.9 (0.9) | 2.0 (1.2) |
| 6. I cannot sleep because I’m worrying about getting the coronavirus | 2.2 (0.8) | 1.4 (0.3) ** | 1.8 (0.9) * |
| 7. My heart rates or palpitates when I think about getting the coronavirus | 2.4 (1.0) | 1.6 (0.4) * | 2.1 (1.2) |
| Total mean | 2.8 (1.0) | 2.4 (0.7) | 2.6 (1.0) |
| Total score | 19.5 (6.7) | 16.7 (5.1) | 18.5 (6.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marotta, M.; Gorini, F.; Parlanti, A.; Chatzianagnostou, K.; Mazzone, A.; Berti, S.; Vassalle, C. Fear of COVID-19 in Patients with Acute Myocardial Infarction. Int. J. Environ. Res. Public Health 2021, 18, 9847. https://doi.org/10.3390/ijerph18189847
Marotta M, Gorini F, Parlanti A, Chatzianagnostou K, Mazzone A, Berti S, Vassalle C. Fear of COVID-19 in Patients with Acute Myocardial Infarction. International Journal of Environmental Research and Public Health. 2021; 18(18):9847. https://doi.org/10.3390/ijerph18189847
Chicago/Turabian StyleMarotta, Marco, Francesca Gorini, Alessandra Parlanti, Kyriazoula Chatzianagnostou, Annamaria Mazzone, Sergio Berti, and Cristina Vassalle. 2021. "Fear of COVID-19 in Patients with Acute Myocardial Infarction" International Journal of Environmental Research and Public Health 18, no. 18: 9847. https://doi.org/10.3390/ijerph18189847