
“Medical Student Syndrome”—A Myth or a Real Disease Entity? Cross-Sectional Study of Medical Students of the Medical University of Silesia in Katowice, Poland

 and
and
Abstract: Background
1. Introduction
2. Materials and Methods
2.1. Cross-Section of the Group
2.2. Statistical Methods
3. Results
3.1. Analysis of the Level of Hypochondria and Nosophobia Symptoms
3.2. The Correlation between the Level of Nosophobia and Hypochondria Symptoms and the Year of Study
3.3. Gender Influence on the Studied Variables
3.4. Linking Psychiatric Treatment with the Severity of Nosophobia and Hypochondria Symptoms
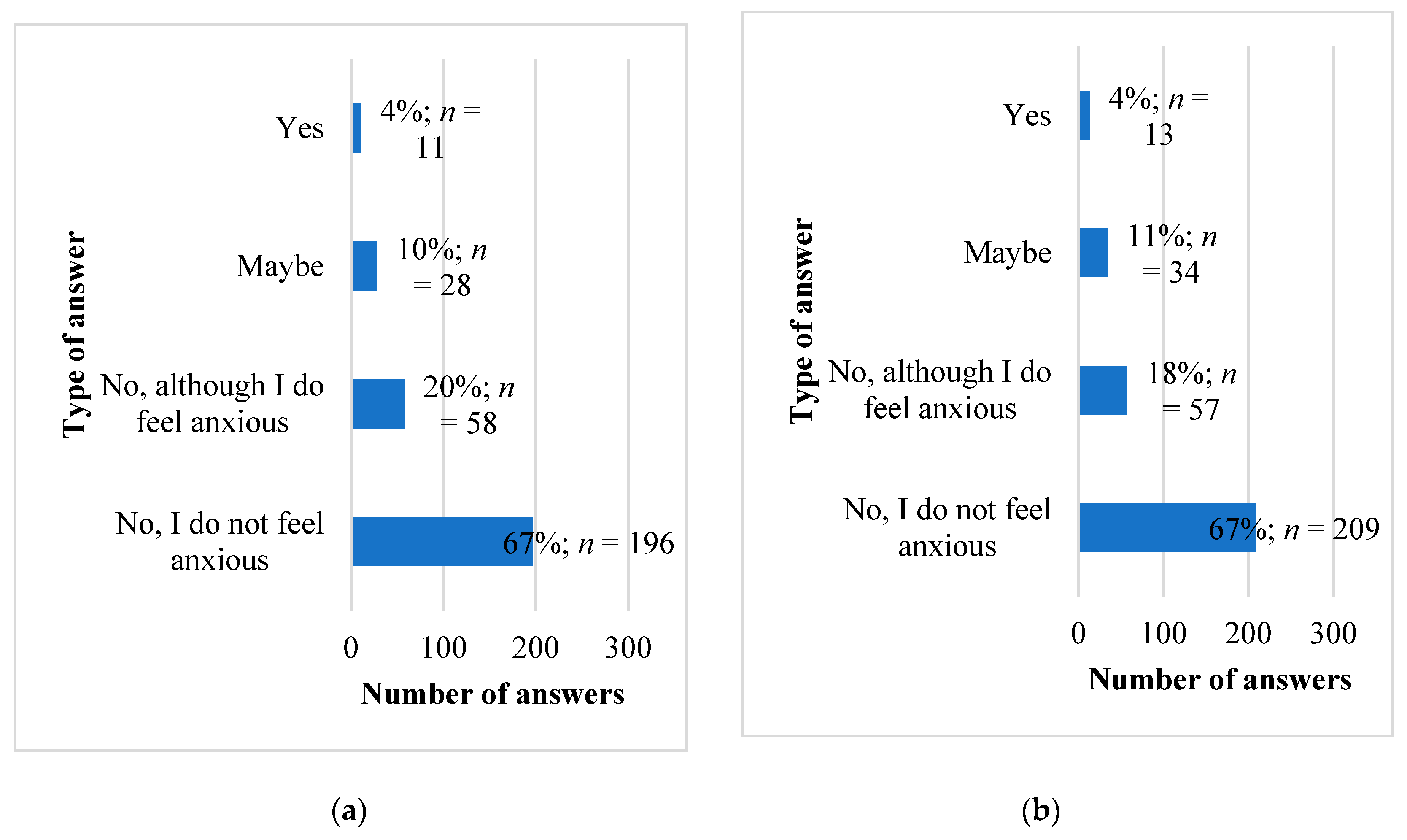
3.5. Observation of Disease Symptoms during Clinical Classes
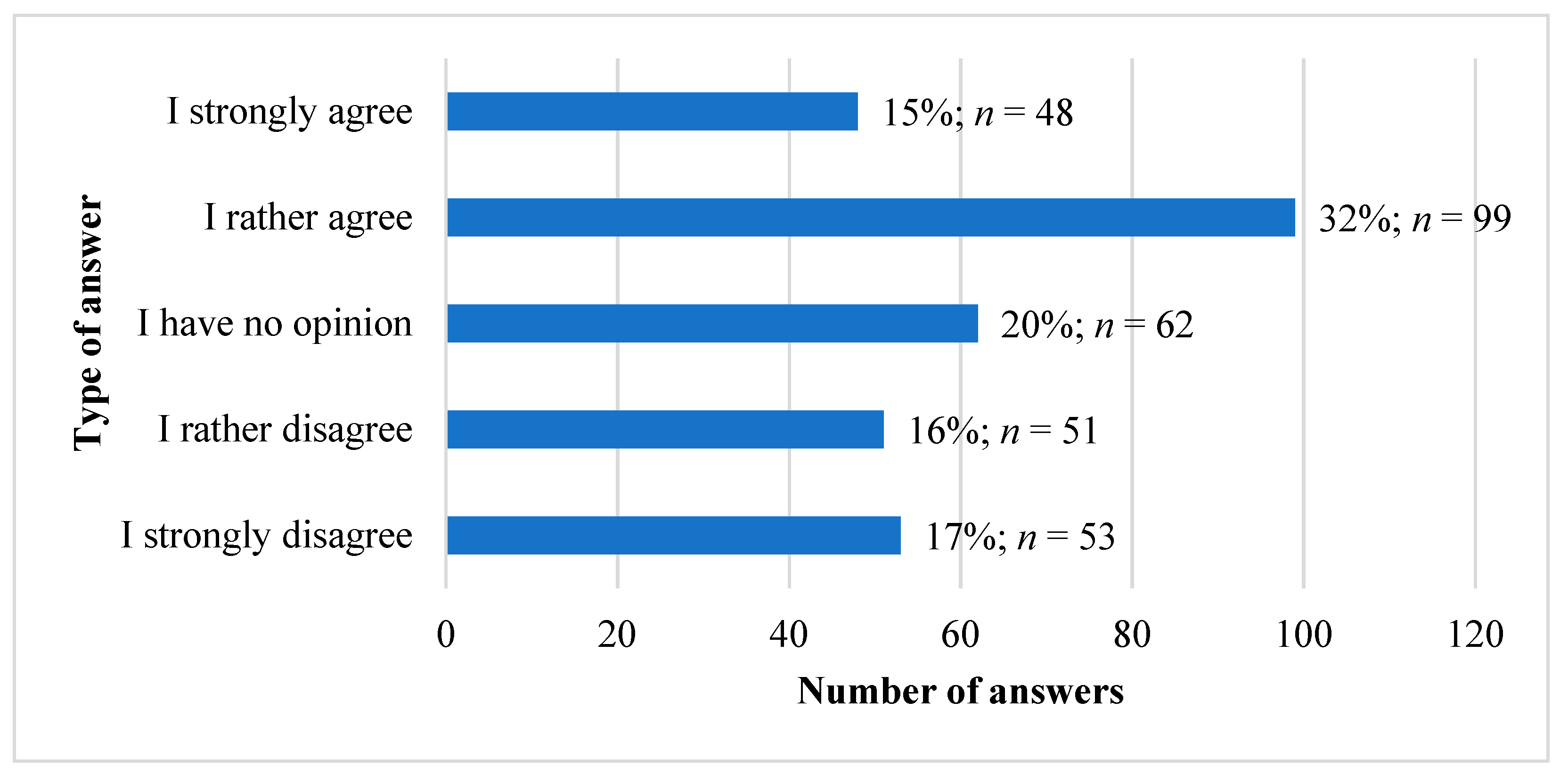
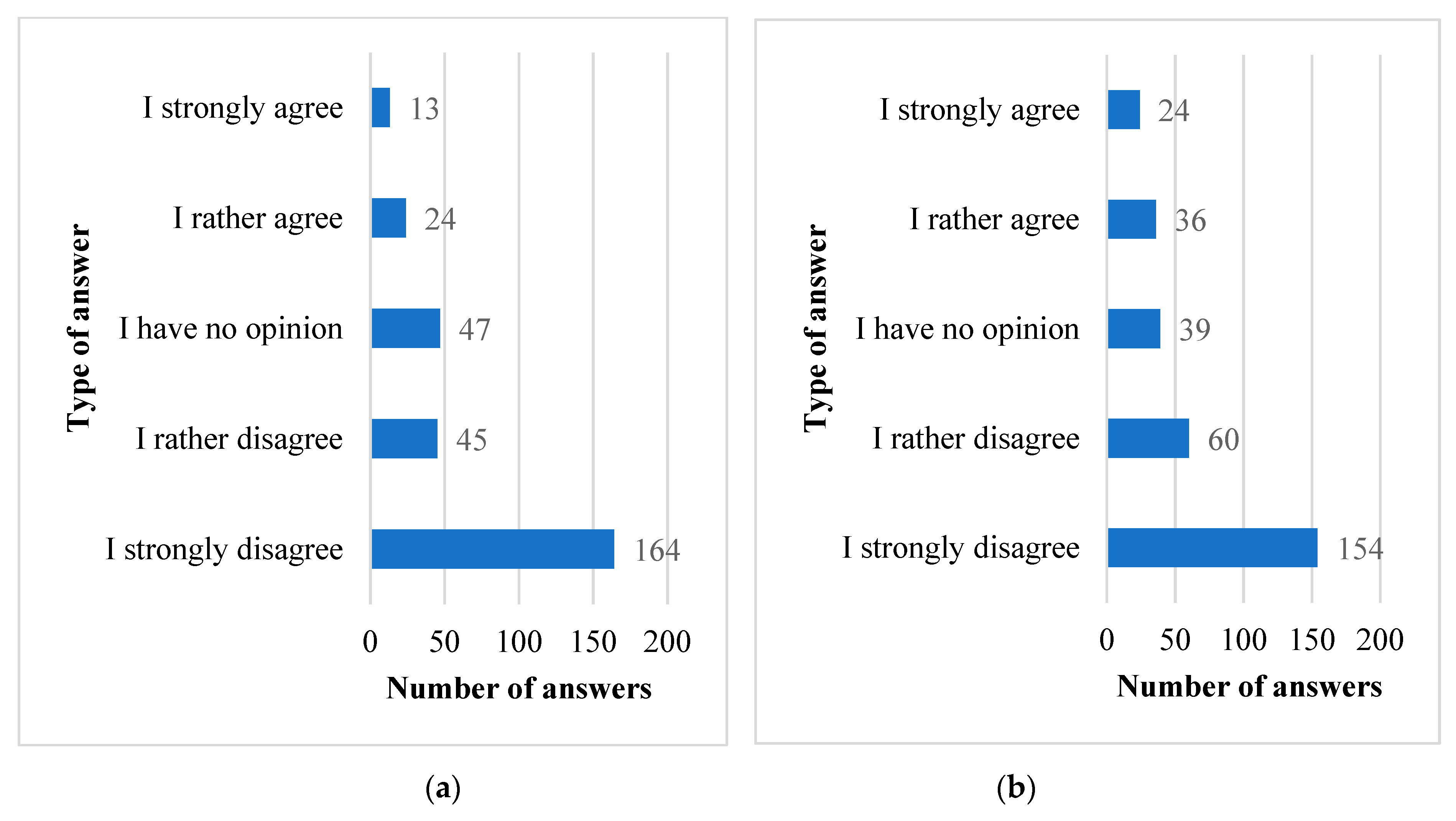
3.6. Hiding Health Problems and the Field of Study
3.7. What Are We Most Afraid of?
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Azuri, J.; Ackshota, N.; Vinker, S. Reassuring the medical students’ disease—Health related anxiety among medical students. Med. Teach. 2010, 32, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Hunter, R.C.; Lohrenz, J.G.; Schwartzman, A.E. Nosophobia and hypochondriasis in medical students. J. Nerv. Ment. Dis. 1964, 139, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Woods, S.M.; Natterson, J.; Silverman, J. Medical students’ disease: Hypochondriasis in medical education. J. Med. Educ. 1966, 41, 785–790. [Google Scholar] [PubMed]
- Waterman, L.Z.; Weinman, J.A. Medical student syndrome: Fact or fiction? A cross-sectional study. JRSM Open 2014, 5, 2042533313512480. [Google Scholar] [CrossRef] [PubMed]
- Ellingsen, A.E.; Wilhelmsen, I. Sykdomsangst blant medisin-og jusstudenter. Tidsskr. Nor. Lægeforen 2002, 122, 785–787. [Google Scholar]
- Howes, O.D.; Salkovskis, P.M. Health anxiety in medical students. Lancet 1998, 351, 1332. [Google Scholar] [CrossRef]
- Yang, F.; Meng, H.; Chen, H.; Xu, X.H.; Liu, Z.; Luo, A.; Feng, Z.C. Influencing factors of mental health of medical students in China. J. Huazhong Univ. Sci. Technol. Med. Sci. 2014, 34, 443–449. [Google Scholar] [CrossRef]
- De Berardis, D.; Campanella, D.; Gambi, F.; La Rovere, R.; Sepede, G.; Core, L.; Canfora, G.; Santilli, E.; Valchera, A.; Mancini, E.; et al. Alexithymia, fear of bodily sensations, and somatosensory amplification in young outpatients with panic disorder. Psychosomatics 2007, 48, 239–246. [Google Scholar] [CrossRef]
- De Berardis, D.; Serroni, N.; Campanella, D.; Marini, S.; Rapini, G.; Valchera, A.; Iasevoli, F.; Mazza, M.; Fornaro, M.; Perna, G.; et al. Alexithymia, Suicide Ideation, C-Reactive Protein, and Serum Lipid Levels Among Outpatients with Generalized Anxiety Disorder. Arch. Suicide Res. 2017, 21, 100–112. [Google Scholar] [CrossRef]
- Woźniewicz, A. Classification of psychosomatic disorders. Psychiatr. Psychol. Klin. 2018, 18, 283–289. [Google Scholar] [CrossRef]
- Okoi, N.O.; Etim, J.J. Nosophobia, hypochondriasis, and willingness of people to seek healthcare amidst the COVID-19 pandemic in Calabar Metropolis of Cross River State, Nigeria. Open J. Psychiatry Allied Sci. 2021, 12, 36–42. [Google Scholar] [CrossRef]
- Holder-Perkins, V.; Wise, T.N.; Williams, D.E. Hypochondriacal Concerns: Management Through Understanding. Prim Care Companion J. Clin. Psychiatry 2000, 2, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Shadid, A.; Shadid, A.M.; Shadid, A.; Almutairi, F.E.; Almotairi, K.E.; Aldarwish, T.; Alzamil, O.; Alkholaiwi, A.; Khan, S.U. Stress, Burnout, and Associated Risk Factors in Medical Students. Cureus 2020, 12, e6633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Backović, D.V.; Maksimović, M.; Davidović, D.; Zivojinović, J.I.; Stevanović, D. Stress and mental health among medical students. Srp. Arh. Celok. Lek. 2013, 141, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Hope, V.; Henderson, M. Medical student depression, anxiety and distress outside North America: A systematic review. Med. Educ. 2014, 48, 963–979. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; Thomas, M.R.; Shanafelt, T.D. Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian medical students. Acad. Med. 2006, 81, 354–373. [Google Scholar] [CrossRef] [PubMed]
- Puthran, R.; Zhang, M.W.; Tam, W.W.; Ho, R.C. Prevalence of depression amongst medical students: A meta-analysis. Med. Educ. 2016, 50, 456–468. [Google Scholar] [CrossRef]
- Shader, R.I. COVID-19 and Depression. Clin. Ther. 2020, 42, 962–963. [Google Scholar] [CrossRef]
- Nicolini, H. Depression and anxiety during COVID-19 pandemic. Cirugía Cir. 2020, 88, 542–547. [Google Scholar] [CrossRef]
- Mazza, M.G.; De Lorenzo, R.; Conte, C.; Poletti, S.; Vai, B.; Bollettini, I.; Melloni, E.M.T.; Furlan, R.; Ciceri, F.; Rovere-Querini, P.; et al. Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. Brain Behav. Immun. 2020, 89, 594–600. [Google Scholar] [CrossRef]
- Perrin, P.C.; McCabe, O.L.; Everly, G.S., Jr.; Links, J.M. Preparing for an influenza pandemic: Mental health considerations. Prehosp. Disaster Med. 2009, 24, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Smith, B.J.; Lim, M.H. How the COVID-19 pandemic is focusing attention on loneliness and social isolation. Public Health Res. Pract. 2020, 30, 3022008. [Google Scholar] [CrossRef] [PubMed]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on College Students’ Mental Health in the United States: Interview Survey Study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef] [PubMed]
- Lasheras, I.; Gracia-García, P.; Lipnicki, D.M.; Bueno-Notivol, J.; López-Antón, R.; de la Cámara, C.; Lobo, A.; Santabárbara, J. Prevalence of Anxiety in Medical Students during the COVID-19 Pandemic: A Rapid Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6603. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Bodicherla, K.P.; Raza, Q.; Sahu, K.K. Impact on mental health by "Living in Isolation and Quarantine" during COVID-19 pandemic. J. Fam. Med. Prim. Care 2020, 9, 5415–5418. [Google Scholar] [CrossRef]
- Moutinho, I.L.; Maddalena, N.C.; Roland, R.K.; Lucchetti, A.L.; Tibiriçá, S.H.; Ezequiel, O.D.; Lucchetti, G. Depression, stress and anxiety in medical students: A cross-sectional comparison between students from different semesters. Rev. Assoc. Med. Bras. 2017, 63, 21–28. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Nechita, F.; Nechita, D.; Pîrlog, M.C.; Rogoveanu, I. Stress in medical students. Rom. J. Morphol. Embryol. 2014, 55 (Suppl. S3), 1263–1266. [Google Scholar]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Liu, X.; Kakade, M.; Fuller, C.J.; Fan, B.; Fang, Y.; Kong, J.; Guan, Z.; Wu, P. Depression after exposure to stressful events: Lessons learned from the severe acute respiratory syndrome epidemic. Compr. Psychiatry 2012, 53, 15–23. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Senat Rzeczypospolitej Polskiej. Available online: https://www.senat.gov.pl/gfx/senat/pl/senatopracowania/175/plik/ot-674_zdrowie_psychiczne.pdf (accessed on 6 May 2021).
- Tjia, J.; Givens, J.L.; Shea, J.A. Factors associated with undertreatment of medical student depression. J. Am. Coll. Health 2005, 53, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, S. Epidemiology of Suicide and the Psychiatric Perspective. Int. J. Environ. Res. Public Health 2018, 15, 1425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Putowski, M.; Piróg, M.; Podgórniak, M.; Zawiślak, J.; Piecewicz-Szczęsna, H. Epidemiological analysis of suicides in Poland between 2000-2013. Probl. Hig. Epidemiol. 2015, 96, 264–268. [Google Scholar]
- Zamachy Samobójcze od 2017 Roku—Zamachy Samobójcze—Statystyka. Available online: https://statystyka.policja.pl/st/wybrane-statystyki/zamachy-samobojcze/63803,Zamachy-samobojcze-od-2017-roku.html (accessed on 6 May 2021).
- Zeng, W.; Chen, R.; Wang, X.; Zhang, Q.; Deng, W. Prevalence of mental health problems among medical students in China: A meta-analysis. Medicine 2019, 98, e15337. [Google Scholar] [CrossRef]
- Kasprzak, M.; Kiejna, A. Comorbidity of mental disorders—Epidemiological data. Psychiatria 2010, 7, 1–10. [Google Scholar]
- United States Department of Health and Human Services, National Institute of Mental Health. Epidemiologic Catchment Area Study, 1980-1985: Household Survey, Wave I.; Inter-university Consortium for Political and Social Research: Ann Arbor, MI, USA , 1991. [Google Scholar] [CrossRef]
- Kessler, R.C.; Chiu, W.T.; Demler, O.; Merikangas, K.R.; Walters, E.E. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 617–627. [Google Scholar] [CrossRef] [Green Version]
- Jaeschke, R.; Siwek, M.; Grabski, B.; Dudek, D. Współwystępowanie zaburzeń depresyjnych i lękowych. Psychiatria 2010, 7, 189–197. [Google Scholar]
- Gentile, J.P.; Roman, B. Medical student mental health services: Psychiatrists treating medical students. Psychiatry 2009, 6, 38–45. [Google Scholar]
- Kiejna, A.; Piotrowski, P.; Adamowski, T.; Moskalewicz, J.; Wciórka, J.; Stokwiszewski, J.; Rabczenko, D.; Kessler, R.C. The prevalence of common mental disorders in the population of adult Poles by sex and age structure—An EZOP Poland study. Psychiatr. Pol. 2015, 49, 15–27. [Google Scholar] [CrossRef]
- Frąckowiak-Sochańska, M. Mental health of men and women. Gender and categories of “mental health” and “mental diseases”. Nowiny Lek. 2011, 80, 394–406. [Google Scholar]
- Królikowska, S. Nierówności w stanie zdrowia między kobietami a mężczyznami w kontekście płci biologicznej oraz społeczno-kulturowej. Acta Univ. Lodz. Folia Sociol. 2011, 39, 33–52. [Google Scholar]
- Przewodnik Po Social Media w Polsce—IAB Polska. Available online: https://www.iab.org.pl/baza-wiedzy/przewodnik-po-social-media-w-polsce/ (accessed on 19 June 2021).
- Welch, T.D. Is Facebook a viable recruitment tool? Nurse Res. 2020, 28, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Główny Urząd Statystyczny/Obszary tematyczne/Edukacja/Edukacja/Szkolnictwo Wyższe w Roku Akademickim 2020/2021 (Wyniki Wstępne). Available online: https://stat.gov.pl/obszary-tematyczne/edukacja/edukacja/szkolnictwo-wyzsze-w-roku-akademickim-20202021-wyniki-wstepne,8,7.html?fbclid=IwAR1ibgm1sDLwimQ26iBilsfM2C2BJyzDqi5o5guFA2Yj-OMQvZryMGdjavs (accessed on 19 June 2021).
- Główny Urząd Statystyczny. Kobiety w Polsce; Women in Poland; Zakład Wydawnictw Statystycznych: Warsaw, Poland, 2007; p. 46. [Google Scholar]
- Borges, N.J.; Manuel, R.S.; Elam, C.L.; Jones, B.J. Comparing millennial and generation X medical students at one medical school. Acad. Med. 2006, 81, 571–576. [Google Scholar] [CrossRef]
- Polyakova, M.; Persson, P.; Hofmann, K.; Jena, A.B. Does medicine run in the family—Evidence from three generations of physicians in Sweden: Retrospective observational study. BMJ 2020, 371, m4453. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Medical Students | Non-Medical Students | ||
|---|---|---|---|
| Sex | Female | 222 | 223 |
| Male | 91 | 70 | |
| Age | Average | 21.8 | 21.5 |
| Median | 22 | 21 | |
| Year of studies | I | 84 | 124 |
| II | 38 | 45 | |
| III | 41 | 41 | |
| IV | 86 | 49 | |
| V | 24 | 30 | |
| VI | 40 | 4 | |
| Financial situation | Very good | 120 | 49 |
| Quite good | 154 | 155 | |
| Average | 35 | 82 | |
| Bad | 4 | 7 | |
| Healthcare type | Private | 79 | 47 |
| Public | 71 | 120 | |
| both to a comparable degree | 163 | 126 |
| Variable under Test | Min | Max | M | SD | SKE | K | d | |
|---|---|---|---|---|---|---|---|---|
| Hypochondria symptoms | 7 | 33 | 12.95 | 4.42 | 0.97 | 0.87 | 0.13 * | |
| Nosophobia symptoms | 6 | 28 | 12.41 | 4.45 | 0.93 | 0.46 | 0.14 * | |
| Fear of pandemic | Before COVID-19 pandemic | 1 | 5 | 2.04 | 0.79 | 0.79 | −0.18 | 0.67 * |
| During COVID-19 pandemic | 0.75 | 4 | 1.01 | 0.29 | 0.29 | −0.56 | 0.10 * | |
| Variable under Test | Students | t | df | p | d | |||
|---|---|---|---|---|---|---|---|---|
| Non-Medical N = 293 | Medical N = 313 | |||||||
| M | SD | M | SD | |||||
| Hypochondria symptoms | 13.38 | 4.38 | 12.55 | 4.43 | 2.30 | 604 | 0.022 | 0.19 |
| Nosophobia symptoms | 12.28 | 4.58 | 12.52 | 4.33 | −0.67 | 604 | 0.501 | 0.05 |
| Students | Variable under Test | Year of Study | |
|---|---|---|---|
| rs | p | ||
| Non-medical N = 293 | Hypochondria symptoms | −0.11 | 0.071 |
| Nosophobia symptoms | −0.06 | 0.304 | |
| Medical N = 313 | Hypochondria symptoms | 0.07 | 0.238 |
| Nosophobia symptoms | 0.13 | 0.026 | |
| The whole group N = 606 | Hypochondria symptoms | −0.03 | 0.478 |
| Nosophobia symptoms | 0.04 | 0.293 | |
| Students | Variable under Test | Sex | U | p | rg | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | |||||||||
| N | Mrang | Me | N | Mrang | Me | |||||
| Non-medical | Hypochondria symptoms | 70 | 123.77 | 11 | 223 | 154.29 | 13 | 6179.00 | 0.009 | 0.21 |
| Nosophobia symptoms | 70 | 122.24 | 10 | 223 | 154.77 | 11 | 6071.50 | 0.005 | 0.22 | |
| Medical | Hypochondria symptoms | 91 | 156.96 | 12 | 222 | 157.02 | 12 | 10,097.00 | 0.996 | 0.00 |
| Nosophobia symptoms | 91 | 139.68 | 11 | 222 | 164.10 | 12 | 8525.00 | 0.030 | 0.16 | |
| The whole group | Hypochondria symptoms | 161 | 282.59 | 11 | 445 | 311.06 | 12 | 32,456.50 | 0.077 | 0.09 |
| Nosophobia symptoms | 161 | 262.41 | 11 | 445 | 318.37 | 12 | 29,207.00 | 0.001 | 0.18 | |
| Mental Disorders | Non-Medical Students | Medical Students |
|---|---|---|
| Depression | 38 | 21 |
| Anxiety disorders | 24 | 20 |
| Anxiety-depressive disorders | 3 | 10 |
| Neurosis | 8 | 7 |
| Obsessive–compulsive disorder | 2 | 6 |
| Personality disorder | 7 | 4 |
| Eating disorders | 4 | 5 |
| Panic attacks | 0 | 3 |
| Other | 12 | 9 |
| Students | Variable under Test | Psychiatric Treatment | U | p | rg | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes | |||||||||
| N | Mrang | Me | N | Mrang | Me | |||||
| Non-medical | Hypochondria symptoms | 235 | 140.74 | 12 | 58 | 172.35 | 14 | 5344.50 | 0.011 | 0.22 |
| Nosophobia symptoms | 235 | 141.42 | 11 | 58 | 169.60 | 12.5 | 5504.00 | 0.023 | 0.19 | |
| Medical | Hypochondria symptoms | 267 | 150.64 | 11 | 46 | 193.90 | 13 | 4443.50 | 0.003 | 0.28 |
| Nosophobia symptoms | 267 | 148.20 | 11 | 46 | 208.09 | 14.5 | 3791.00 | <0.001 | 0.38 | |
| The whole group | Hypochondria symptoms | 502 | 290.37 | 12 | 104 | 366.89 | 14 | 19,511.00 | <0.001 | 0.25 |
| Nosophobia symptoms | 502 | 289.44 | 11 | 104 | 371.37 | 13.5 | 19,045.50 | <0.001 | 0.27 | |
| Students | Declaration on Undertaking Psychiatric Treatment | χ2 | df | p | |||
|---|---|---|---|---|---|---|---|
| Before Pandemic | During Pandemic | ||||||
| N | % | N | % | ||||
| Non-medical N = 293 | 19 | 6.48 | 8 | 2.73 | 4.48 | 1 | 0.034 |
| Medical N = 313 | 10 | 3.19 | 6 | 1.91 | 1.00 | 1 | 0.317 |
| What Kind of the Disease do You Fear the Most? | Non-Medical Students | Medical Students |
|---|---|---|
| Tumor/Cancer | 217 | 235 |
| Psychiatric disorders | 116 | 142 |
| Diseases of the musculoskeletal system, e.g., degeneration of the spine | 106 | 81 |
| HIV/HCV/HBV infection | 58 | 78 |
| Cardiovascular disease | 47 | 56 |
| Complications of the disease I already have | 39 | 46 |
| Diabetes | 54 | 46 |
| Tick-borne diseases | 45 | 39 |
| Thyroid disease | 39 | 23 |
| Hashimoto | 39 | 23 |
| Neurological diseases, CNS diseases | 1 | 9 |
| Anemia | 19 | 7 |
| COVID-19 | 3 | 5 |
| Eye-related conditions | 0 | 5 |
| Dermatological conditions | 0 | 4 |
| Parasites | 0 | 2 |
| Digestive system conditions | 1 | 2 |
| Schizophrenia | 0 | 2 |
| Multiple sclerosis | 1 | 1 |
| Respiratory system diseases | 2 | 1 |
| ADHD | 0 | 1 |
| Cold | 3 | 0 |
| Other advisable | diseases of the joints, sinuses, autoimmune diseases | stroke, pregnancy, alcohol dementia, motor disability, conditions that affect fertility |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szczurek, K.; Furgał, N.; Szczepanek, D.; Zaman, R.; Krysta, K.; Krzystanek, M. “Medical Student Syndrome”—A Myth or a Real Disease Entity? Cross-Sectional Study of Medical Students of the Medical University of Silesia in Katowice, Poland. Int. J. Environ. Res. Public Health 2021, 18, 9884. https://doi.org/10.3390/ijerph18189884
Szczurek K, Furgał N, Szczepanek D, Zaman R, Krysta K, Krzystanek M. “Medical Student Syndrome”—A Myth or a Real Disease Entity? Cross-Sectional Study of Medical Students of the Medical University of Silesia in Katowice, Poland. International Journal of Environmental Research and Public Health. 2021; 18(18):9884. https://doi.org/10.3390/ijerph18189884
Chicago/Turabian StyleSzczurek, Katarzyna, Natalia Furgał, Dawid Szczepanek, Rashid Zaman, Krzysztof Krysta, and Marek Krzystanek. 2021. "“Medical Student Syndrome”—A Myth or a Real Disease Entity? Cross-Sectional Study of Medical Students of the Medical University of Silesia in Katowice, Poland" International Journal of Environmental Research and Public Health 18, no. 18: 9884. https://doi.org/10.3390/ijerph18189884