
Minimally Invasive L5 Corpectomy with Navigated Expandable Vertebral Cage: A Technical Note

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
2.1. Patient History
2.2. Physical Examination
2.3. Preoperative Imaging
2.4. First Surgery and Postoperative Images
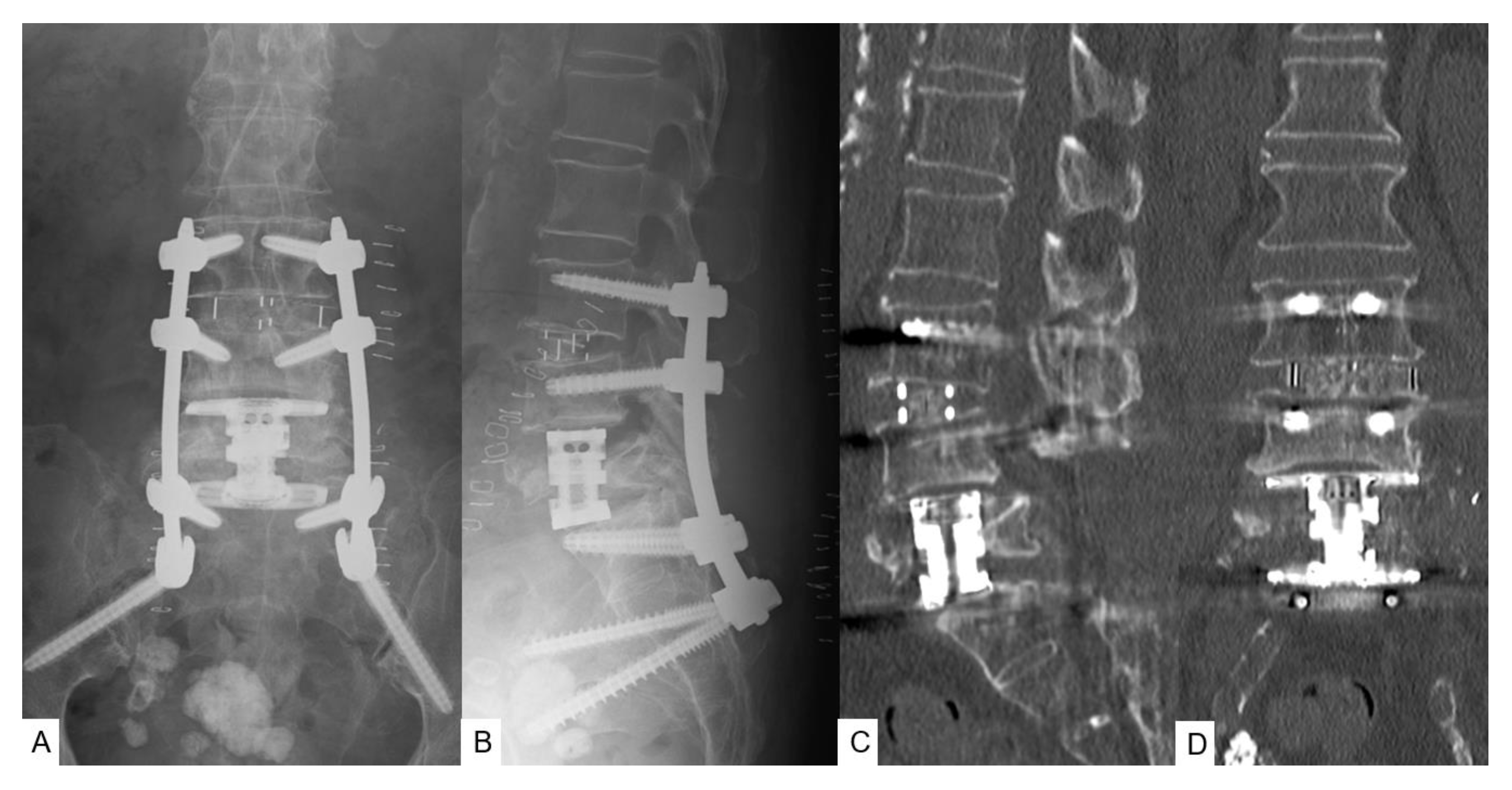
2.5. Second Surgery and Postoperative Images
2.6. Follow-Up Results
3. Operative Procedure
3.1. Mini-Extraperitoneal Approach
3.2. Corpectomy with Navigation
3.3. Navigated Expandable Vertebral Cage
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- D’Aquino, D.; Tarawneh, A.M.; Hilis, A.; Palliyil, N.; Deogaonkar, K.; Quraishi, N.A. Surgical approaches to L5 corpectomy: A systematic review. Eur. Spine J. 2020, 29, 3074–3079. [Google Scholar] [CrossRef] [PubMed]
- Vazan, M.; Ryang, Y.M.; Gerhardt, J.; Zibold, F.; Janssen, I.; Ringel, F.; Gempt, J.; Meyer, B. L5 corpectomy-the lumbosacral segmental geometry and clinical outcome-a consecutive series of 14 patients and review of the literature. Acta Neurochir. 2017, 159, 1147–1152. [Google Scholar] [CrossRef] [PubMed]
- Quraishi, N.A.; Konig, M.; Booker, S.J.; Shafafy, M.; Boszczyk, B.M.; Grevitt, M.P.; Mehdian, H.; Webb, J.K. Access related complications in anterior lumbar surgery performed by spinal surgeons. Eur. Spine J. 2013, 22 (Suppl. 1), S16–S20. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, M.; Fujiwara, Y.; Uotani, K.; Ayhan, S.; Yamauchi, T.; Sonawane, S.; Nakanishi, K. Minimally invasive thoracolumbar corpectomy with navigated expandable vertebral cage: A technical note. Interdis. Neurosurg. 2021, 24, 101123. [Google Scholar]
- Anand, N.; Baron, E.M.; Thaiyananthan, G.; Khalsa, K.; Goldstein, T.B. Minimally invasive multilevel percutaneous correction and fusion for adult lumbar degenerative scoliosis: A technique and feasibility study. J. Spinal Disord. Tech. 2008, 21, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Deml, M.C.; Mazuret Sepulveda, C.A.; Albers, C.E.; Hoppe, S.; Bigdon, S.F.; Häckel, S.; Milavec, H.; Benneker, L.M. Anterior column reconstruction of the thoracolumbar spine with a new modular PEEK vertebral body replacement device: Retrospective clinical and radiologic cohort analysis of 48 cases with 1.7-years follow-up. Eur. Spine J. 2020, 29, 3194–3202. [Google Scholar] [CrossRef]
- Tanaka, M.; Fujiwara, Y.; Uotani, K.; Maste, P.; Yamauchi, T. C-arm-free circumferential minimally invasive surgery for adult spinal deformity: Technical note. World Neurosurg. 2020, 143, 235–246. [Google Scholar] [CrossRef]
- Colosimo, C.; Gaudino, S.; Alexandre, A.M. Imaging in degenerative spine pathology. Acta Neurochir. Suppl. 2011, 108, 9–15. [Google Scholar]
- Pedicelli, A.; Rollo, M.; Piano, M.; Re, T.J.; Cipriani, M.C.; Colosimo, C.; Bonomo, L. Percutaneous vertebroplasty with a high-quality rotational angiographic unit. Eur. J. Radiol. 2009, 69, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Galibert, P.; Deramond, H.; Rosat, P.; Le Gars, D. Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty. Neurochirurgie 1987, 33, 166–168. [Google Scholar]
- Garfin, S.R.; Yuan, H.A.; Reiley, M.A. New technologies in spine: Kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine 2001, 26, 1511–1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, P.A.; Rawlinson, H.J.; Hadlow, A.T. Radiologic stability of titanium mesh cages for anterior spinal reconstruction following thoracolumbar corpectomy. J. Spinal Disord. Tech. 2004, 17, 44–52. [Google Scholar] [CrossRef]
- Sheng, X.; Ren, S. Surgical techniques for osteoporotic vertebral collapse with delayed neurological deficits: A systematic review. Int. J. Surg. 2016, 33, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Gaines, R.W.; Nichols, W.K. Treatment of spondyloptosis by two stage L5 vertebrectomy and reduction of L4 onto S1. Spine 1985, 10, 680–686. [Google Scholar] [CrossRef]
- Elnady, B.; Shawky, A.; Abdelrahman, H.; Elmorshidy, E.; El-Meshtawy, M.; Said, G.Z. Posterior only approach for fifth lumbar corpectomy: Indications and technical notes. Int. Orthop. 2017, 41, 2535–2541. [Google Scholar] [CrossRef] [PubMed]
- Dai, L.Y.; Jiang, L.S. Anterior-only instrumentation and grafting after L5 corpectomy for non-traumatic lesions. Acta Orthop. Belg. 2010, 76, 94–99. [Google Scholar] [PubMed]
- Kaner, T.; Oktenoglu, T.; Sasani, M.; Ozer, A.F. L5 vertebrectomy for the surgical treatment of tumoral and traumatic lesions of L5 vertebra. Orthop. Rev. 2012, 4, e10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiyama, A.; Sakai, D.; Sato, M.; Watanabe, M. The analysis of percutaneous pedicle screw technique with guide wire-less in lateral decubitus position following extreme lateral interbody fusion. J. Orthop. Surg. Res. 2019, 14, 304. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, M.; Singh, M.; Fujiwara, Y.; Uotani, K.; Arataki, S.; Yamauchi, T.; Nakanishi, K. Minimally invasive thoracolumbar corpectomy and percutaneous pedicle screw fixation with computer-assisted rod-bending system in single lateral position: Technical note. World Neurosurg. 2021, 151, 138–144. [Google Scholar] [CrossRef]
- Kwee, M.M.; Ho, Y.H.; Rozen, W.M. The prone position during surgery and its complications: A systematic review and evidence-based guidelines. Int. Surg. 2015, 100, 292–303. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Fridley, J.; Gokaslan, Z.; Telfeian, A.; Oyelese, A.A. Minimally invasive thoracolumbar corpectomy and stabilization for unstable burst fractures using intraoperative computed tomography and computer-assisted spinal navigation. World Neurosurg. 2019, 122, e1266–e1274. [Google Scholar] [CrossRef] [PubMed]
- Shousha, M.; El-Saghir, H.; Boehm, H. Corpectomy of the fifth lumbar vertebra, a challenging procedure. J. Spinal Disord. Tech. 2014, 27, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Shin, B.J.; James, A.R.; Njoku, I.U.; Härtl, R. Pedicle screw navigation: A systematic review and meta-analysis of perforation risk for computer-navigated versus freehand insertion. J. Neurosurg. Spine 2012, 17, 113–122. [Google Scholar] [CrossRef] [PubMed]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamauchi, T.; Jaiswal, A.; Tanaka, M.; Fujiwara, Y.; Oda, Y.; Arataki, S.; Misawa, H. Minimally Invasive L5 Corpectomy with Navigated Expandable Vertebral Cage: A Technical Note. Brain Sci. 2021, 11, 1241. https://doi.org/10.3390/brainsci11091241
Yamauchi T, Jaiswal A, Tanaka M, Fujiwara Y, Oda Y, Arataki S, Misawa H. Minimally Invasive L5 Corpectomy with Navigated Expandable Vertebral Cage: A Technical Note. Brain Sciences. 2021; 11(9):1241. https://doi.org/10.3390/brainsci11091241
Chicago/Turabian StyleYamauchi, Taro, Ashish Jaiswal, Masato Tanaka, Yoshihiro Fujiwara, Yoshiaki Oda, Shinya Arataki, and Haruo Misawa. 2021. "Minimally Invasive L5 Corpectomy with Navigated Expandable Vertebral Cage: A Technical Note" Brain Sciences 11, no. 9: 1241. https://doi.org/10.3390/brainsci11091241