
Assessment of the Effect of A-PRF Application during the Surgical Extraction of Third Molars on Healing and the Concentration of C-Reactive Protein

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
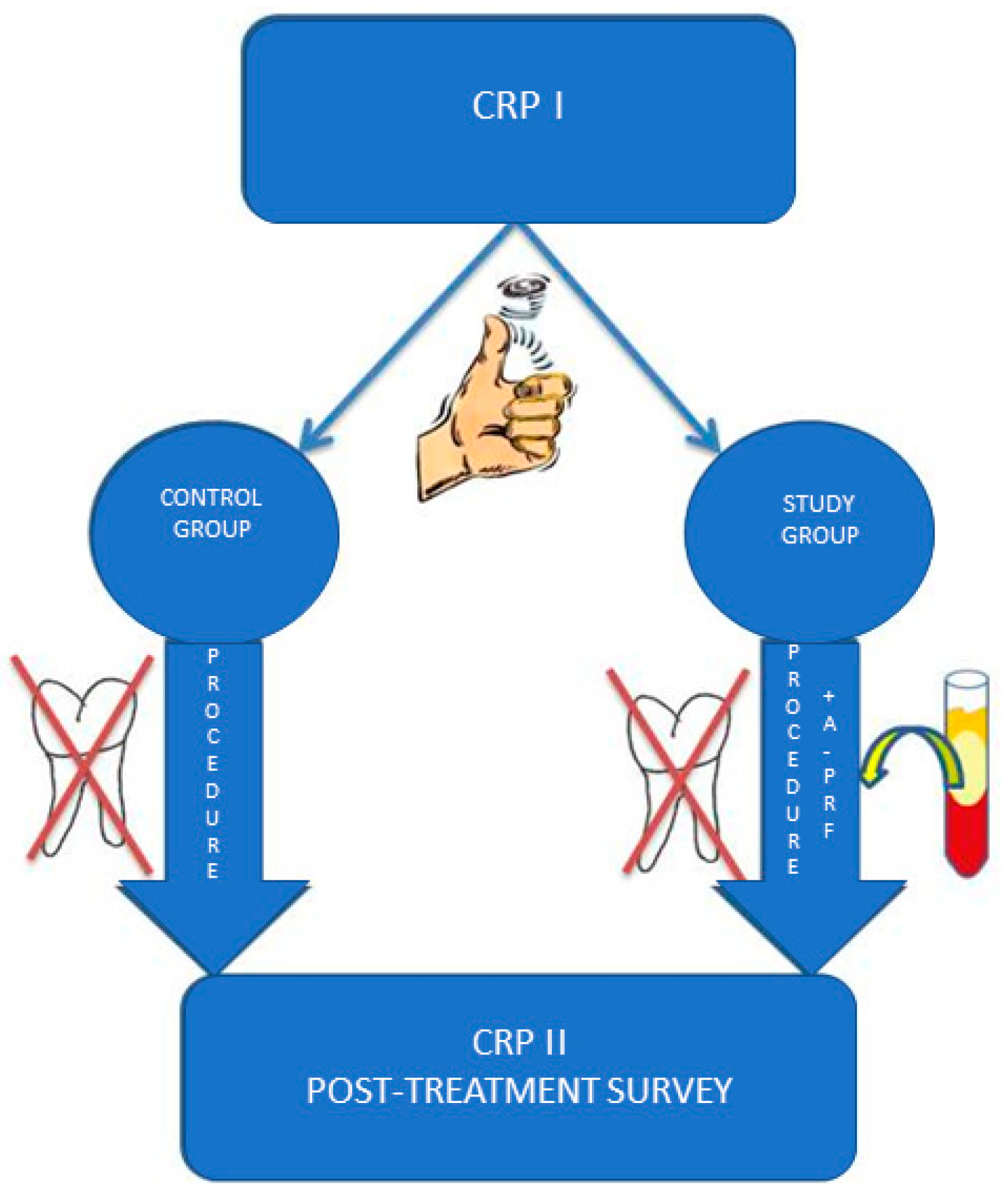
2.1. Experimental Groups
2.2. Patient Selection
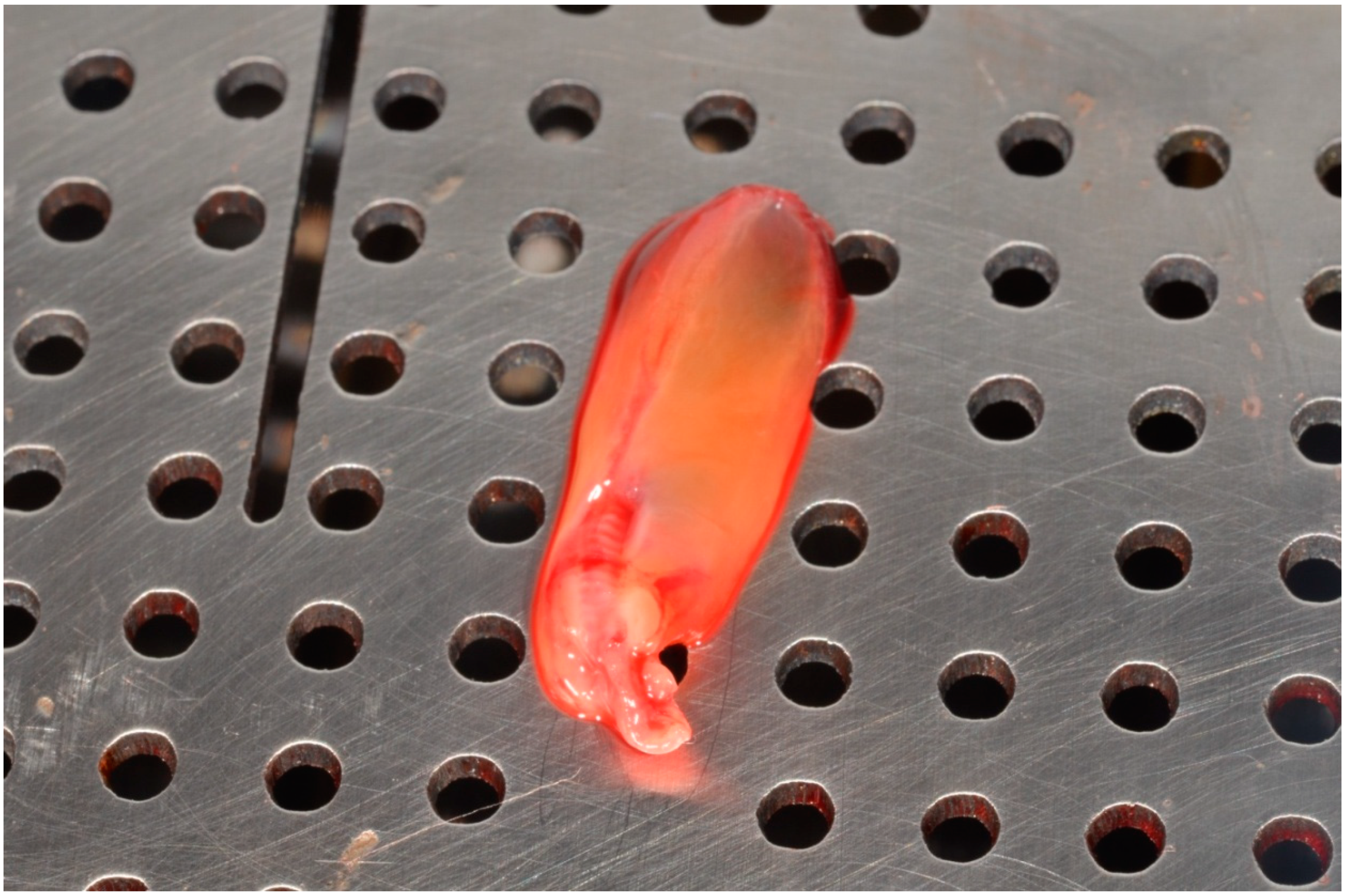
2.3. PRF Management
2.4. Surgical Procedures and Intrasurgical Measurements
2.5. Blood Test Methodology
2.6. Methodology of Blood Biochemical Testing
2.7. Control Day
- swelling
- pain
- subjective trismus
- redness at the treatment site
- dry mouth
- burning
2.8. Statistical Analysis
3. Results
3.1. CRP
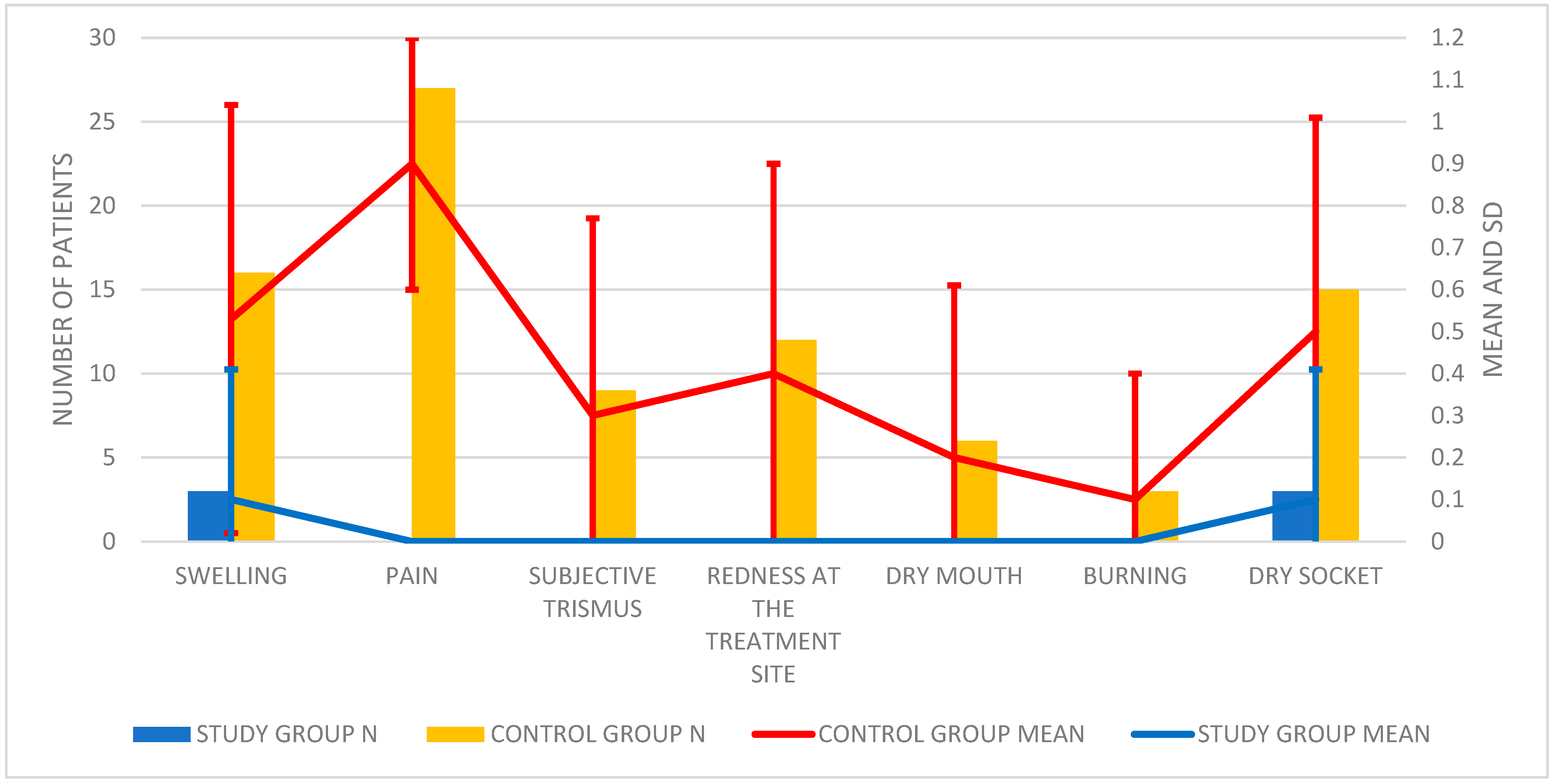
3.2. Postoperative Survey
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosa, A.L.; Carneiro, M.G.; Lavrador, M.A.; Novaes, A.B. Influence of flap design on periodontal healing of second molars after extraction of impacted mandibular third molars. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2002, 93, 404–407. [Google Scholar] [CrossRef]
- Ayranci, F.; Omezli, M.M.; Sivrikaya, E.C.; Rastgeldi, Z.O. Prevalence of Impacted Wisdom Teeth in Middle Black Sea Population. J. Clin. Exp. Investig. 2017, 8, 58–61. [Google Scholar] [CrossRef] [Green Version]
- Nejat, A.; Shamsabadi, R.M.; Rezaei, N.; Eshghpour, M.; Nezadi, A.; Moradi, A. Pattern of mandibular third molar impaction: A cross-sectional study in northeast of Iran. Niger. J. Clin. Pract. 2014, 17, 673–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansimranjit Kaur, U.; Vishnu, K.; Samrat, G. Prevalence and Pattern of Third Molar Impaction among Residents of District Panchkula, India. Int. Healthc. Res. J. 2018, 2, 41–44. [Google Scholar] [CrossRef] [Green Version]
- Kumar Pillai, A.; Thomas, S.; Paul, G.; Singh, S.K.; Moghe, S. Incidence of impacted third molars: A radiographic study in People’s Hospital, Bhopal, India. J. Oral Biol. Craniofacial Res. 2014, 4, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Bayoumi, A.M.; Baabdullah, R.M.; Bokhari, A.F.; Nadershah, M. The Prevalence Rate of Third Molar Impaction among Jeddah Population. Int. J. Dent. Oral Heal. 2016, 2, 1–4. [Google Scholar] [CrossRef]
- Ratajczak, J.; Vangansewinkel, T.; Gervois, P.; Merckx, G.; Hilkens, P.; Quirynen, M.; Lambrichts, I.; Bronckaers, A. Angiogenic Properties of ‘Leukocyte- and Platelet-Rich Fibrin’. Sci Rep. 2018, 8, 14632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strauss, F.-J.; Nasirzade, J.; Kargarpoor, Z.; Stähli, A.; Gruber, R. Effect of platelet-rich fibrin on cell proliferation, migration, differentiation, inflammation, and osteoclastogenesis: A systematic review of in vitro studies. Clin. Oral Investig. 2019, 24, 569–584. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Ha, Y.; Kang, N.H. Effects of Growth Factors from Platelet-Rich Fibrin on the Bone Regeneration. J. Craniofacial Surg. 2017, 28, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Lundquist, R.; Dziegiel, M.H.; Ågren, M.S. Bioactivity and stability of endogenous fibrogenic factors in platelet-rich fibrin. Wound Repair Regen. 2008, 16, 356–363. [Google Scholar] [CrossRef]
- Schaller, B.; Miron, R.J.; Kobayashi, M.; Sawada, K.; Sculean, A.; Kobayashi, E.; Flückiger, L. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin. Oral Investig. 2016, 20, 2353–2360. [Google Scholar] [CrossRef]
- Kobayashi, M.; Kawase, T.; Horimizu, M.; Okuda, K.; Wolff, L.F.; Yoshie, H. A proposed protocol for the standardized preparation of PRF membranes for clinical use. Biologicals 2012, 40, 323–329. [Google Scholar] [CrossRef]
- Nishimoto, S.; Fujita, K.; Sotsuka, Y.; Kinoshita, M.; Fujiwara, T.; Kawai, K.; Kakibuchi, M. Growth Factor Measurement and Histological Analysis in Platelet Rich Fibrin: A Pilot Study. J. Maxillofac. Oral Surg. 2015, 14, 907–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masuki, H.; Okudera, T.; Watanabe, T.; Suzuki, M.; Nishiyama, K.; Okudera, H.; Nakata, K.; Uematsu, K.; Su, C.-Y.; Kawase, T. Growth factor and pro-inflammatory cytokine contents in platelet-rich plasma (PRP), plasma rich in growth factors (PRGF), advanced platelet-rich fibrin (A-PRF), and concentrated growth factors (CGF). Int. J. Implant. Dent. 2016, 2, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Dohan Ehrenfest, D.M.; Diss, A.; Odin, G.; Doglioli, P.; Hippolyte, M.P.; Charrier, J.B. In vitro effects of Choukroun’s PRF (platelet-rich fibrin) on human gingival fibroblasts, dermal prekeratinocytes, preadipocytes, and maxillofacial osteoblasts in primary cultures. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 108, 341–352. [Google Scholar] [CrossRef]
- He, L.; Lin, Y.; Hu, X.; Zhang, Y.; Wu, H. A comparative study of platelet-rich fibrin (PRF) and platelet-rich plasma (PRP) on the effect of proliferation and differentiation of rat osteoblasts in vitro. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 108, 707–713. [Google Scholar] [CrossRef]
- Caymaz, M.G.; O Uyanik, L. Comparison of the effect of advanced platelet-rich fibrin and leukocyte- and platelet-rich fibrin on outcomes after removal of impacted mandibular third molar: A randomized split-mouth study. Niger. J. Clin. Pract. 2019, 22, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Knapen, M.; Gheldof, D.; Drion, P.; Layrolle, P.; Rompen, E.; Lambert, F. Effect of Leukocyte- and Platelet-Rich Fibrin (L-PRF) on Bone Regeneration: A Study in Rabbits. Clin. Implant. Dent. Relat. Res. 2013, 17, e143–e152. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.B.; Meschi, N.; Temmerman, A.; Pinto, N.; Lambrechts, P.; Teughels, W.; Quirynen, M. Regenerative potential of leucocyte- and platelet-rich fibrin. Part B: Sinus floor elevation, alveolar ridge preservation and implant therapy. A systematic review. J. Clin. Periodontol. 2016, 44, 225–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Zhang, Y.; Choukroun, J.; Ghanaati, S.; Miron, R.J. Effects of an injectable platelet-rich fibrin on osteoblast behavior and bone tissue formation in comparison to platelet-rich plasma. Platelets 2018, 29, 48–55. [Google Scholar] [CrossRef]
- Miron, R.J.; Zucchelli, G.; Pikos, M.A.; Salama, M.; Lee, S.; Guillemette, V.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Wang, H.-L.; et al. Use of platelet-rich fibrin in regenerative dentistry: A systematic review. Clin. Oral Investig. 2017, 21, 1913–1927. [Google Scholar] [CrossRef]
- Lee, D.G.; Lee, K.S.; Shim, J.J.; Yoon, S.M.; Bae, H.G. Prognostic value of the C-reactive protein levels in the head injury. J. Korean Neurotraumatol. Soc. 2005, 1, 57–60. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M. Clinical Application of C-Reactive Protein for Cardiovascular Disease Detection and Prevention. Circulation 2003, 107, 363–369. [Google Scholar] [CrossRef]
- Yudkin, J.S.; Stehouwer, C.D.; Emeis, J.J.; Coppack, S.W. C-reactive protein in healthy subjects: Associations with obesity, insulin resistance, and endothelial dysfunction: A potential role for cytokines originating from adipose tissue? Arterioscler. Thromb. Vasc. Biol. 1999, 19, 972–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afari, N.; Mostoufi, S.; Noonan, C.; Poeschla, B.; Succop, A.; Chopko, L.; Strachan, E. C-Reactive Protein and Pain Sensitivity: Findings from Female Twins. Ann. Behav. Med. 2011, 42, 277–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekiye, A.; Sylvester, I.E.; Pius, I. High Sensitivity C-Reactive Protein in Patients with Acute Injuries. IOSR J. Dent. Med. Sci. 2015, 14, 94–98. [Google Scholar]
- Kao, P.C.; Shiesh, S.C.; Wu, T.J. Serum C-Reactive Protein as a Marker for Wellness Assessment. Ann. Clin. Lab. Sci. 2006, 36, 163–169. [Google Scholar] [PubMed]
- Smith, R.P.; Lipworth, B.J.; Cree, I.A.; Spiers, E.M.; Winter, J.H. C-reactive protein. A clinical marker in community-acquired pneumonia. Chest 1995, 108, 1288–1291. [Google Scholar] [CrossRef] [PubMed]
- Giannoudis, P.V.; Smith, M.R.; Evans, R.T.; Bellamy, M.C.; Guillou, P.J. Serum CRP and IL-6 levels after trauma. Not predictive of septic complications in 31 patients. Acta Orthop. Scand. 1998, 69, 184–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aher, V.; Chander, P.M.; Ali, F.M. C-reactive protein a better indicator of inflammation after third molar extraction. Niger. J. Clin. Pract. 2013, 16, 297. [Google Scholar] [CrossRef]
- Ren, Y.-F.; Malmstrom, H.S. Rapid quantitative determination of C-reactive protein at chair side in dental emergency patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 104, 49–55. [Google Scholar] [CrossRef]
- Irshad, A.S.; Mohamad, I.; Shahid, H.; Tajamul, H.; Zahoor, T. The CRP levels in patients of alveolar osteitis treated with eugional and Honey-Research. IOSR J. Dent. Med. Sci. 2015, 14, 57–61. [Google Scholar]
- Graziani, F.; D’Aiuto, F.; Gennai, S.; Petrini, M.; Nisi, M.; Cirigliano, N.; Landini, L.; Bruno, R.; Taddei, S.; Ghiadoni, L. Systemic Inflammation after Third Molar Removal: A Case-Control Study. J. Dent. Res. 2017, 96, 1505–1512. [Google Scholar] [CrossRef]
- Roberts, W.L.; Sedrick, R.; Moulton, L.; Spencer, A.; Rifai, N. Evaluation of four automated high-sensitivity C-reactive protein methods: Implications for clinical and epidemiological applications. Clin. Chem. 2000, 46, 461–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkins, J.; Gallimore, J.R.; Moore, E.G.; Pepys, M.B. Rapid automated high sensitivity enzyme immunoassay of C-reactive protein. Clin. Chem. 1998, 44 Pt 1, 1358–1361. [Google Scholar] [CrossRef]
- Rifai, N.; Tracy, R.P.; Ridker, P.M. Clinical efficacy of an automated high-sensitivity C-reactive protein assay. Clin. Chem. 1999, 45, 2136–2141. [Google Scholar] [CrossRef] [Green Version]
- Roberts, W.L.; Moulton, L.; Law, T.C.; Farrow, G.; Cooper-Anderson, M.; Savory, J.; Rifai, N. Evaluation of nine automated high-sensitivity C-reactive protein methods: Implications for clinical and epidemiological applications. Part 2. Clin. Chem. 2001, 47, 418–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cei, S.; D’Aiuto, F.; Duranti, E.; Taddei, S.; Gabriele, M.; Ghiadoni, L.; Graziani, F. Third molar surgical removal: A posiible model of human systemic inflamation? A preliminary investigation. Eur. J. Inflamm. 2012, 10, 149–152. [Google Scholar] [CrossRef]
- Mantilla Gomez, S.; Danser, M.M.; Sipos, P.M.; Rowshani, B.; van der Velden, U.; van der Weijden, G.A. Tongue coating and salivary bacterial counts in healthy/gingivitis subjects and periodontitis patients. J. Clin. Periodontol. 2001, 28, 970–978. [Google Scholar] [CrossRef]
- Al-Hamed, F.S.; Tawfik, M.A.-M.; Abdelfadil, E. Clinical effects of platelet-rich fibrin (PRF) following surgical extraction of lower third molar. Saudi J. Dent. Res. 2017, 8, 19–25. [Google Scholar] [CrossRef] [Green Version]
- Fujioka-Kobayashi, M.; Miron, R.J.; Moraschini, V.; Zhang, Y.; Gruber, R.; Wang, H.-L. Efficacy of platelet-rich fibrin on socket healing after mandibular third molar extractions. J. Oral Maxillofac. Surg. Med. Pathol. 2021, 33, 379–388. [Google Scholar] [CrossRef]
- Kim, J.-C.; Choi, S.-S.; Wang, S.-J.; Kim, S.-G. Minor complications after mandibular third molar surgery: Type, incidence, and possible prevention. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 102, e4–e11. [Google Scholar] [CrossRef] [PubMed]
- Sanchís Bielsa, J.M.; Hernandez Bazan, S.; Peñarrocha Diago, M. Flap repositioning versus conventional suturing in third molar surgery. Med. Oral Patol. Oral Cir. Bucal. 2008, 13, E138–E142. [Google Scholar]
- Kareem, J.J. A Comparison between primary and secondary wound closure after surgical removal of lower third molars according to pain and swelling. MDJ 2008, 5, 410–417. [Google Scholar]
- Grossi, G.B.; Maiorana, C.; Garramone, R.A.; Borgonovo, A.; Creminelli, L.; Santoro, F. Assessing Postoperative Discomfort After Third Molar Surgery: A Prospective Study. J. Oral Maxillofac. Surg. 2007, 65, 901–917. [Google Scholar] [CrossRef] [PubMed]
- Osunde, O.; Adebola, R.; Saheeb, B. A comparative study of the effect of suture-less and multiple suture techniques on inflammatory complications following third molar surgery. Int. J. Oral Maxillofac. Surg. 2012, 41, 1275–1279. [Google Scholar] [CrossRef]
- Garcia Garcia, A.; Gude Sampedro, F.; Gandara Rey, J.; Gallas Torreira, M. Trismus and pain after removal of impacted lower third molars. J. Oral Maxillofac. Surg. 1997, 55, 1223–1226. [Google Scholar] [CrossRef]
- Townend, J. Third molar surgery: An audit of the indications for surgery, postoperative complaints and patient satisfaction. Br. J. Oral Maxillofac. Surg. 1995, 33, 265. [Google Scholar] [CrossRef]
- Dolanmaz, D.; Esen, A.; Isik, K.; Candirli, C. Effect of 2 flap designs on postoperative pain and swelling after impacted third molar surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, e244–e246. [Google Scholar] [CrossRef] [PubMed]
- Yuasa, H.; Sugiura, M. Clinical postoperative findings after removal of impacted mandibular third molars: Prediction of postoperative facial swelling and pain based on preoperative variables. Br. J. Oral Maxillofac. Surg. 2004, 42, 209–214. [Google Scholar] [CrossRef]
- Hashemi, H.M.; Beshkar, M.; Aghajani, R. The effect of sutureless wound closure on postoperative pain and swelling after impacted mandibular third molar surgery. Br. J. Oral Maxillofac. Surg. 2012, 50, 256–258. [Google Scholar] [CrossRef] [PubMed]
- Pasqualini, D.; Cocero, N.; Castella, A.; Mela, L.; Bracco, P. Primary and secondary closure of the surgical wound after removal of impacted mandibular third molars: A comparative study. Int. J. Oral Maxillofac. Surg. 2005, 34, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Gaya, V.O.; Capilla, M.V.; Mateos, R.G. Relación de las variables del paciente y de la intervención con el dolor y la inflamación postoperatorios en la exodoncia de los terceros molares. Med. Oral. 2002, 7, 360–369. [Google Scholar]
- de Santana-Santos, T.; de Souza-Santos, A.; Martins-Filho, P.R.; da Silva, L.C.; de Oliveira, E.S.E.D.; Gomes, A.C. Prediction of postoperative facial swelling, pain and trismus following third molar surgery based on preoperative variables. Med. Oral Patol. Oral Cir. Bucal. 2013, 18, e65–e70. [Google Scholar] [CrossRef]
- Al-Samman, A.A. Pattern of Pain and Swelling after Periapical and Wisdom Tooth Surgery: Are age and Gender Predictive Factors? Iraqi Dent. J. 2017, 39, 51–58. [Google Scholar] [CrossRef]
- Al-Belasy, F.A. The relationship of “shisha” (water pipe) smoking to postextraction dry socket. J. Oral Maxillofac. Surg. 2004, 62, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Haraji, A.; Rakhshan, V.; Khamverdi, N.; Alishahi, H.K. Effects of intra-alveolar placement of 0.2% chlorhexidine bioadhesive gel on dry socket incidence and postsurgical pain: A double-blind split-mouth randomized controlled clinical trial. J. Orofac. Pain 2013, 27, 256–262. [Google Scholar] [CrossRef] [Green Version]
- Eshghpour, M.; Dastmalchi, P.; Nekooei, A.H.; Nejat, A. Effect of Platelet-Rich Fibrin on Frequency of Alveolar Osteitis Following Mandibular Third Molar Surgery: A Double-Blinded Randomized Clinical Trial. J. Oral Maxillofac. Surg. 2014, 72, 1463–1467. [Google Scholar] [CrossRef]
- Blondeau, F.; Daniel, N.G. Extraction of Impacted Mandibular Third Molars: Postoperative Complications and Their Risk Factors. JCDA 2007, 73, 325e. [Google Scholar]
- Singh, V.; Soni, N.; Mohammad, S.; Singh, R.; Pal, U.; Singh, R.; Aggrwal, J.; Pal, M. Effects of honey in the management of alveolar osteitis: A study. Natl. J. Maxillofac. Surg. 2016, 7, 136–147. [Google Scholar] [CrossRef] [Green Version]
- Mamoun, J. Dry Socket Etiology, Diagnosis, and Clinical Treatment Techniques. J. Korean Assoc. Oral Maxillofac. Surg. 2018, 44, 52–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolokythas, A.; Olech, E.; Miloro, M. Alveolar Osteitis: A Comprehensive Review of Concepts and Controversies. Int. J. Dent. 2010, 2010, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Gowda, G.G.; Viswanath, D.; Kumar, M.; Umashanker, D. Dry Socket (Alveolar Osteitis): Incidence, Pathogenesis, Prevention and Management. J. Indian Acad. Oral Med. Radiol. 2013, 25, 196–199. [Google Scholar]
- Blum, I. Contemporary views on dry socket (alveolar osteitis): A clinical appraisal of standardization, aetiopathogenesis and management: A critical review. Int. J. Oral Maxillofac. Surg. 2002, 31, 309–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoaglin, D.R.; Lines, G.K. Prevention of Localized Osteitis in Mandibular Third-Molar Sites Using Platelet-Rich Fibrin. Int. J. Dent. 2013, 2013, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hamed, F.S.; Tawfik, M.A.-M.; Abdelfadil, E.; Al-Saleh, M.A. Efficacy of Platelet-Rich Fibrin After Mandibular Third Molar Extraction: A Systematic Review and Meta-Analysis. J. Oral Maxillofac. Surg. 2017, 75, 1124–1135. [Google Scholar] [CrossRef]
- Asutay, F.; Geçör, O.; Acar, A.; Öztürk, S.; Malkoç, S. An evaluation of effects of platelet-rich-fibrin on postoperative morbidities after lower third molar surgery. Niger. J. Clin. Pract. 2016, 20, 1531–1536. [Google Scholar] [CrossRef] [Green Version]
- Rutkowski, J.L.; Fennell, J.W.; Kern, J.C.; Madison, D.E.; Johnson, D.A. Inhibition of alveolar osteitis in mandibular tooth extraction sites using platelet-rich plasma. J. Oral Implantol. 2007, 33, 116–121. [Google Scholar] [CrossRef]
- Ratiu, C.; Brocks, M.; Costea, T.; Moldovan, L.; Cavalu, S. PRGF-Modified Collagen Membranes for Guided Bone Regeneration: Spectroscopic, Microscopic and Nano-Mechanical Investigations. Appl. Sci. 2019, 9, 1035. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Lables | Study Group | Control Group |
|---|---|---|
| number of participants | 30 | 30 |
| sex | f: 1; m: 19 | f: 11; m: 19 |
| age (mean) | f: 25.91 ± 5.61; m: 25.42 ± 3.55 | f: 22.64 ± 2.46; m: 26.58 ± 3.80 |
| Group | Patient | Age | Sex | CRP I | CRP II | ∆CRP |
|---|---|---|---|---|---|---|
| Study | 1 | 26 | M | 0.40 | 0.20 | −0.20 |
| 2 | 20 | M | 0.44 | 2.68 | 2.24 | |
| 3 | 36 | K | 0.51 | 0.14 | −0.37 | |
| 4 | 23 | M | 1.50 | 2.29 | 0.79 | |
| 5 | 26 | M | 3.26 | 1.38 | −1.88 | |
| 6 | 36 | K | 1.72 | 1.99 | 0.27 | |
| 7 | 23 | M | 1.82 | 1.96 | 0.14 | |
| 8 | 22 | K | 1.30 | 1.14 | −0.16 | |
| 9 | 26 | M | 2.10 | 0.90 | −1.20 | |
| 10 | 27 | K | 4.98 | 1.50 | −3.48 | |
| 11 | 26 | M | 0.30 | 1.14 | 0.84 | |
| 12 | 22 | M | 1.22 | 3.91 | 2.69 | |
| 13 | 27 | K | 0.19 | 2.20 | 2.01 | |
| 14 | 26 | M | 3.30 | 1.34 | −1.96 | |
| 15 | 32 | M | 4.00 | 2.50 | −1.50 | |
| 16 | 24 | K | 1.50 | 1.00 | −0.50 | |
| 17 | 20 | K | 0.12 | 2.13 | 2.01 | |
| 18 | 22 | K | 1.50 | 1.10 | −0.40 | |
| 19 | 20 | K | 0.15 | 2.10 | 1.95 | |
| 20 | 33 | M | 3.90 | 2.30 | −1.60 | |
| 21 | 22 | M | 3.10 | 1.20 | −1.90 | |
| 22 | 27 | K | 4.96 | 1.54 | −3.42 | |
| 23 | 25 | M | 0.37 | 0.26 | −0.11 | |
| 24 | 27 | M | 2.09 | 0.94 | −1.15 | |
| 25 | 21 | M | 0.35 | 2.66 | 2.31 | |
| 26 | 31 | M | 4.19 | 2.54 | −1.65 | |
| 27 | 24 | K | 1.25 | 1.05 | −0.20 | |
| 28 | 26 | M | 1.30 | 1.10 | −0.20 | |
| 29 | 23 | M | 1.15 | 3.80 | 2.65 | |
| 30 | 25 | M | 2.15 | 0.97 | −1.18 | |
| Control | 1 | 25 | K | 4.95 | 7.50 | 2.55 |
| 2 | 34 | M | 0.50 | 4.70 | 4.20 | |
| 3 | 25 | M | 0.30 | 0.90 | 0.60 | |
| 4 | 27 | M | 2.30 | 1.70 | −0.60 | |
| 5 | 26 | K | 1.34 | 6.30 | 4.96 | |
| 6 | 20 | K | 0.10 | 0.31 | 0.21 | |
| 7 | 26 | M | 0.75 | 2.10 | 1.35 | |
| 8 | 26 | M | 2.00 | 1.60 | −0.40 | |
| 9 | 20 | K | 0.01 | 0.21 | 0.20 | |
| 10 | 23 | K | 0.34 | 8.17 | 7.83 | |
| 11 | 26 | M | 2.12 | 1.94 | −0.18 | |
| 12 | 33 | M | 0.32 | 4.83 | 4.51 | |
| 13 | 37 | M | 0.60 | 5.03 | 4.43 | |
| 14 | 24 | M | 1.34 | 2.27 | 0.93 | |
| 15 | 25 | K | 4.95 | 7.50 | 2.55 | |
| 16 | 24 | K | 0.70 | 8.00 | 7.30 | |
| 17 | 26 | M | 0.50 | 2.00 | 1.50 | |
| 18 | 25 | M | 0.15 | 0.95 | 0.80 | |
| 19 | 25 | M | 0.50 | 1.30 | 0.80 | |
| 20 | 23 | M | 1.34 | 2.27 | 0.93 | |
| 21 | 21 | K | 1.51 | 2.49 | 0.98 | |
| 22 | 25 | K | 3.95 | 6.40 | 2.45 | |
| 23 | 25 | M | 0.20 | 0.90 | 0.70 | |
| 24 | 25 | M | 0.30 | 0.90 | 0.60 | |
| 25 | 25 | M | 0.29 | 0.80 | 0.51 | |
| 26 | 24 | M | 1.20 | 2.07 | 0.87 | |
| 27 | 26 | M | 0.45 | 2.15 | 1.70 | |
| 28 | 20 | K | 0.05 | 0.35 | 0.30 | |
| 29 | 23 | M | 2.35 | 3.25 | 0.90 | |
| 30 | 20 | K | 0.30 | 0.61 | 0.31 |
| Group | n | Mean | Median | Minimum | Maximum | SD | p TEST | |
|---|---|---|---|---|---|---|---|---|
| CRPI | Study | 30 | 1.84 | 1.5 | 0.12 | 4.98 | 1.48 | 0.083 |
| Control | 30 | 1.19 | 0.55 | 0.01 | 4.95 | 1.35 | ||
| CRP II | Study | 30 | 1.66 | 1.44 | 0.14 | 3.91 | 0.93 | 0.01 |
| Control | 30 | 2.98 | 2.08 | 0.21 | 8.18 | 2.54 | ||
| CRP ∆ | Study | 30 | 0.17 | −0.2 | −3.48 | 2.69 | 1.70 | 0.001 |
| Control | 30 | 1.79 | 0.915 | 0.60 | 7.83 | 2.15 |
| Patients Who Have Occurred | Swelling | Pain | Subjective Trismus | Redness at the Treatment Site | Dry Mouth | Burning | Dry Socket | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
| Study Group | 3 | 10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 10 |
| Control Group | 16 | 53.33% | 27 | 90% | 9 | 30% | 12 | 40% | 6 | 20% | 3 | 10% | 15 | 50% |
| Group | n | Mean | Median | Minimum | Maximum | SD | p Test | |
|---|---|---|---|---|---|---|---|---|
| Swelling | STUDY | 30 | 0.1 | 0 | 0 | 1 | 0.31 | 0.004 |
| CONTROL | 30 | 0.53 | 1 | 0 | 1 | 0.51 | ||
| Pain | STUDY | 30 | 0 | 0 | 0 | 0 | 0 | 0.000 |
| CONTROL | 30 | 0.9 | 1 | 0 | 1 | 0.30 | ||
| Subjective trismus | STUDY | 30 | 0 | 0 | 0 | 0 | 0 | 0.047 |
| CONTROL | 30 | 0.3 | 0 | 0 | 1 | 0.47 | ||
| Redness at the treatment side | STUDY | 30 | 0 | 0 | 0 | 0 | 0 | 0.008 |
| CONTROL | 30 | 0.4 | 0 | 0 | 1 | 0.50 | ||
| Dry mouth | STUDY | 30 | 0 | 0 | 0 | 0 | 0 | 0.185768 |
| CONTROL | 30 | 0.2 | 0 | 0 | 1 | 0.41 | ||
| Burning | STUDY | 30 | 0 | 0 | 0 | 0 | 0 | 0.510598 |
| CONTROL | 30 | 0.1 | 0 | 0 | 1 | 0.30 |
| Group | n | Mean | Median | Minimum | Maximum | SD | p TEST | |
|---|---|---|---|---|---|---|---|---|
| Dry Socket | Study | 30 | 0.1 | 0 | 0 | 1 | 0.31 | 0.007959 |
| Control | 30 | 0.5 | 0.5 | 0 | 1 | 0.51 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowak, J.M.; Surma, S.; Romańczyk, M.; Wojtowicz, A.; Filipiak, K.J.; Czerniuk, M.R. Assessment of the Effect of A-PRF Application during the Surgical Extraction of Third Molars on Healing and the Concentration of C-Reactive Protein. Pharmaceutics 2021, 13, 1471. https://doi.org/10.3390/pharmaceutics13091471
Nowak JM, Surma S, Romańczyk M, Wojtowicz A, Filipiak KJ, Czerniuk MR. Assessment of the Effect of A-PRF Application during the Surgical Extraction of Third Molars on Healing and the Concentration of C-Reactive Protein. Pharmaceutics. 2021; 13(9):1471. https://doi.org/10.3390/pharmaceutics13091471
Chicago/Turabian StyleNowak, Jacek M., Stanisław Surma, Monika Romańczyk, Andrzej Wojtowicz, Krzysztof J. Filipiak, and Maciej R. Czerniuk. 2021. "Assessment of the Effect of A-PRF Application during the Surgical Extraction of Third Molars on Healing and the Concentration of C-Reactive Protein" Pharmaceutics 13, no. 9: 1471. https://doi.org/10.3390/pharmaceutics13091471