
Permeation Challenges of Drugs for Treatment of Neurological Tuberculosis and HIV and the Application of Magneto-Electric Nanoparticle Drug Delivery Systems


Abstract
:1. Introduction
2. Drug Permeation Challenges in CNS TB Treatment
2.1. Drug Permeation Challenges in CNS HIV
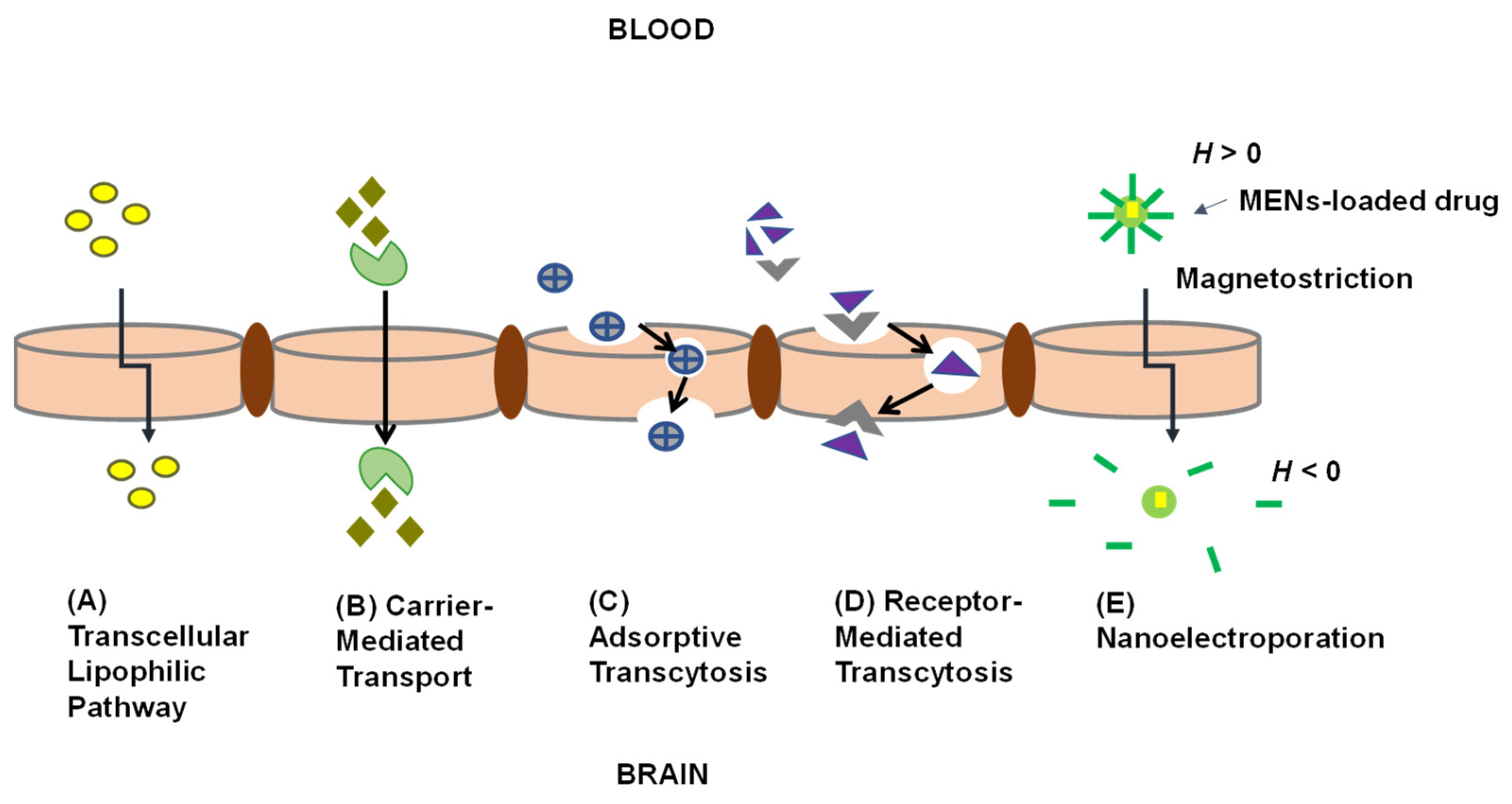
2.2. Drug Delivery across the BBB

{kind=link}
{kind=link}
{kind=link}
| Approach | Drug Delivered across the BBB | Observations | Ref. |
|---|---|---|---|
| Intranasal drug delivery | α-L-idur-onidase (IDUA) encoding adeno-associated virus serotype 9 (AAV9) vector | Intranasal administration of α-L-idur-onidase (IDUA) encoding adeno-associated virus serotype 9 (AAV9) vector results in enzyme diffusion into deeper areas of the brain and reduction of tissue glycosaminoglycans storage materials in the brain. | [68] |
| Altered drug solubility | Doxorubicin | Conjugation of doxorubicin with angiopep-2 increased delivery of doxorubicin to the brain and showed good bioavailability and lowtoxicity. | [67] |
| NP drug delivery system | Zidovudine | Zidovudine was delivered via nanostructured lipid carriers into an in vitro human brain cell line (C6) and led to a significantly higher accumulation of the drug in the brain cells. The results suggest that these NPs could be a promising delivery system to enhance the brain uptake of zidovudine and other non-nucleotide ARVs. | [69] |
| NP drug delivery system | Atazanavir | In vitro delivery of atazanavir by solid lipid NPs into a hCMEC/D3 cell line demonstrated a significantly higher drug accumulation compared to the drug aqueous solution alone. | [70] |
| Polymer drug conjugates | Ciprofloxacin | Increase in the uptake of PEGylated ciprofloxacin when the surfaces of the biologically active polymer core/shell NPs were modified with Tat peptide (TAT–PEG-b-Chol nanoparticles). | [71] |
| Peptidomimetics | HAYED peptide | A 16 lysine (K16) residue-linked low-density lipoprotein receptor-related protein (LDLR)-binding amino acid segment of apolipoprotein E (K16APoE) was used to deliver a therapeutic peptide (HAYED) into an Alzheimer’s disease mouse model brain leading to reduced necrosis. | [72] |
| Viral vectors | Gadoteridol | Gadoteridol was co-infused with adeno-associated viral type 2 vectors and results showed that infusion of therapies directly into the disease- infected regions of the human brain with convection-enhanced delivery provides an effective strategy for treating neurological disorders. | [73] |
| Trojan horse approach | HIRMAb-IDUA fusion protein | HIRMAb-IDUA fusion protein, also called valanafusp alpha has been administered to patients with mucopolysaccharidosis (MPS) I. Patients were treated with HIRMAb-IDUA weekly by IV infusion for over a year. MPS I patients treated with HIRMAb-IDUA who suffered from severe mental retardation demonstrated stability in their IQ from further decline. | [74] |
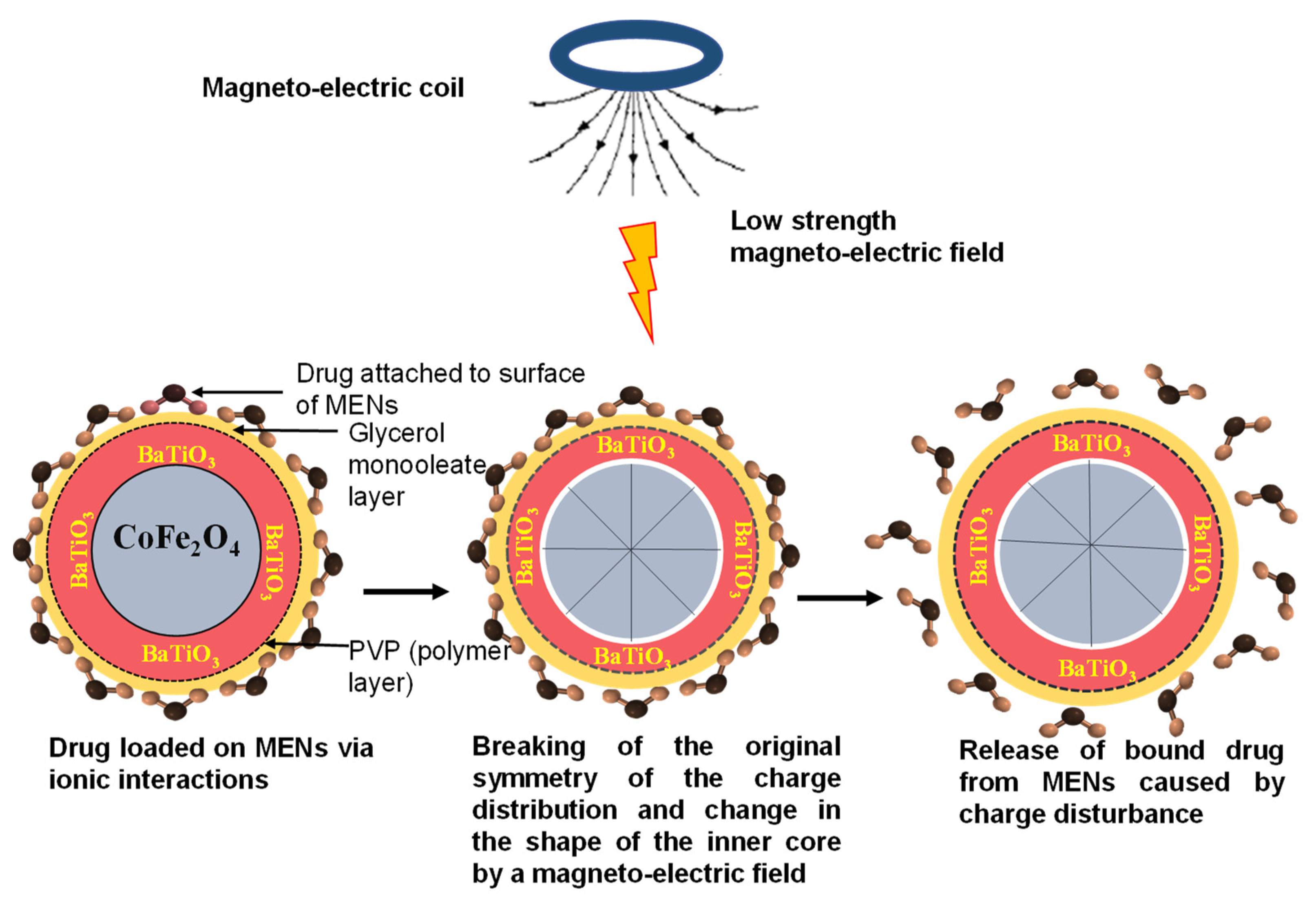
2.3. Application of MENs to Deliver Drugs across the BBB for CNS TB and HIV
3. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rodriguez-Takeuchi, S.Y.; Renjifo, M.E.; Medina, F.J. Extrapulmonary tuberculosis: Pathophysiology and imaging findings. Radiographics 2019, 39, 2023–2037. [Google Scholar] [CrossRef]
- Cherian, A.; Thomas, S.V. Central nervous system tuberculosis. Afr. Health Sci. 2011, 11, 116–127. [Google Scholar]
- Leonard, J.M. Central Nervous System Tuberculosis. In Tuberculosis and Nontuberculous Mycobacterial Infections, 7th ed.; ASM Press: Washington, DC, USA, 2017; pp. 331–341. [Google Scholar] [CrossRef]
- Chakaya, J.; Khan, M.; Ntoumi, F.; Aklillu, E.; Fatima, R.; Mwaba, P.; Kapata, N.; Mfinanga, S.; Hasnain, S.E.; Katoto, P.D.M.C.; et al. Global Tuberculosis Report 2020—Reflections on the Global TB burden, treatment and prevention efforts. Int. J. Infect. Dis. 2021, in press. [Google Scholar] [CrossRef]
- Chen, W.; Huang, L.; Tang, Q.; Wang, S.; Hu, C.; Zhang, X. Progress on diagnosis and treatment of central nervous system tuberculosis. Radiol. Infect. Dis. 2020, 7, 160–169. [Google Scholar] [CrossRef]
- Picchio, V.; Cammisotto, V.; Pagano, F.; Carnevale, R.; Chimenti, I. Cell Interaction-Regulation of Immune Responses, Disease Development and Management Strategies; Intechopen: London, UK, 2020; pp. 1–15. [Google Scholar]
- Daneman, R.; Prat, A. The Blood–Brain Barrier. Cold Spring Harb. Perspect. Biol. 2015, 7, a020412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvarez-Uria, G.; Midde, M.; Pakam, R.; Naik, P.K. Initial Antituberculous Regimen with Better Drug Penetration into Cerebrospinal Fluid Reduces Mortality in HIV Infected Patients with Tuberculous Meningitis: Data from an HIV Observational Cohort Study. Tuberc. Res. Treat. 2013, 2013, 242604. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.; Meintjes, G.; Wilkinson, R.J. Treatment of Tuberculous Meningitis and Its Complications in Adults. Curr. Treat. Options Neurol. 2018, 20, 5. [Google Scholar] [CrossRef] [Green Version]
- Spudich, S.; González-Scarano, F. HIV-1 Related Central Nervous System Diseases: Current Issues in Pathogenesis, Diagnosis and Treatment. Cold Spring Harb. Perspect. Med. 2012, 2, a007120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahm, T.; Rudolph, H.; Schwerk, C.; Schroten, H.; Tenenbaum, T. Neuroinvasion and Inflammation in Viral Central Nervous System Infection. Mediat. Inflamm. 2016, 2016, 8562805. [Google Scholar] [CrossRef] [Green Version]
- Joseph, S.B.; Arrildt, K.T.; Sturdevant, C.B.; Swanstrom, R. HIV-1 targeted cells in the CNS. J. Neurovirol. 2015, 21, 276–289. [Google Scholar] [CrossRef]
- Marban, C.; Forouzanfar, F.; Ait-Ammar, A.; Fahmi, F.; Mekdad, H.E.; Daouad, F.; Rohr, O.; Schwartz, C. Targeting the brain reservoirs: Toward an HIV cure. Front. Immunol. 2016, 7, 397. [Google Scholar] [CrossRef] [Green Version]
- Wallet, C.; De Rovere, M.; Assche, J.A.; Daouad, F.; De Wit, S.; Gautier, V.; Mallon, P.W.G.; Marcello, A.; Van Lint, C.; Rohr, O.; et al. Microglial Cells: The Main HIV-1 Reservoir in the Brain. Front. Cell. Infect. Microbiol. 2019, 9, 362. [Google Scholar] [CrossRef] [Green Version]
- Valdebenito, S.; Castellano, P.; Ajasin, D.; Eugenin, E.A. Astrocytes are HIV reservoirs in the brain: A cell type with poor HIV infectivity and replication but efficient cell-to-cell viral transfer. J. Neurochem. 2021, 158, 429–443. [Google Scholar] [CrossRef]
- Osborne, O.; Peyravian, N.; Nair, M.; Daunert, S.; Toborek, M. The Paradox of HIV Blood–Brain Barrier Penetrance and Antiretroviral Drug Delivery Deficiencies. Trends Neurosci. 2020, 43, 695–708. [Google Scholar] [CrossRef] [PubMed]
- Su, J.; Sinclair, E.; Peterson, J.; Lee, E.; Kyriakides, T.C.; Li, F.; Hagberg, L.; Fuchs, D.; Price, R.W.; Gisslen, M.; et al. Progressive increase in central nervous system immune activation in untreated primary HIV-infection. J. Neuroinflamm. 2014, 11, 199. [Google Scholar]
- Wright, P.W.; Pyakurel, A.; Vaida, F.F.; Price, R.W.; Lee, E.; Peterson, J.; Fuchs, D.; Zetterberg, H.; Robertson, K.R.; Walter, R.; et al. Putamen volume and its clinical and neurological correlates in primary HIV infection. AIDS 2016, 30, 1789–1794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calcagno, A.; Perri, G.D.; Bonora, S. Treating HIV in the Central Nervous System. Drugs 2017, 77, 145–157. [Google Scholar] [CrossRef]
- Heaton, R.K.; Franklin, D.R., Jr.; Deutsch, R.; Letendre, S.; Ellis, R.J.; Casaletto, K.; Marquine, M.J.; Woods, S.P.; Vaida, F.; Atkinson, J.H.; et al. Neurocognitive change in the era of HIV combination antiretroviral therapy: The longitudinal CHARTER study. Clin. Infect. Dis. 2015, 60, 473–480. [Google Scholar] [CrossRef]
- Spudich, S.; Peterson, J.; Fuchs, D.; Price, R.W.; Gisslen, M. Potential for early antiretroviral therapy to reduce central nervous system HIV-1 persistence. AIDS 2019, 33, S135–S144. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.A.; Zunt, J.R. Tuberculosis of the central nervous system in immunocompromised patients: HIV infection and solid organ transplant recipients. Clin. Infect. Dis. 2011, 53, 915–926. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.; Gangwani, M.R.; Chaudhari, N.S.; Glazyrin, A.; Bhat, H.K.; Kumar, A. Neurotoxicity in the Post-HAART Era: Caution for the Antiretroviral Therapeutics. Neurotox Res. 2017, 30, 677–697. [Google Scholar] [CrossRef] [PubMed]
- Price, R.W.; Spudich, S. Antiretroviral therapy and central nervous system HIV type 1 infection. J. Infect. Dis. 2008, 197 (Suppl. 3), S294–S306. [Google Scholar] [CrossRef] [Green Version]
- Nwogu, J.N.; Ma, Q.; Babalola, C.P.; Adedeji, W.A.; Morse, G.D.; Taiwo, B. Pharmacokinetic, Pharmacogenetic, and Other Factors Influencing CNS Penetration of Antiretrovirals. AIDS Res. Treat. 2016, 2016, 2587094. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, A.; Price, R.W.; Gisslén, M. Antiretroviral drug treatment of CNS HIV-1 infection. J. Antimicrob. Chemother. 2012, 67, 299–311. [Google Scholar] [CrossRef] [Green Version]
- Kaushik, A.; Jayant, R.D.; Sagar, V.; Nair, M. The potential of magneto-electric nanocarriers for drug delivery. Expert Opin. Drug Deliv. 2014, 11, 1635–1646. [Google Scholar] [CrossRef] [PubMed]
- Rodzinski, A.; Guduru, R.; Liang, P.; Hadjikhani, A.; Stewart, T.; Stimphil, E.; Runowicz, C.D.; Cote, R.; Altman, N.; Datar, R.; et al. Targeted and controlled anticancer drug delivery and release with magnetoelectric nanoparticles. Sci. Rep. 2016, 6, 20867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, T.; Nagesetti, A.; Guduru, R.; Liang, P.; Stimphil, E.; Hadjikhani, A.; Salgueiro, L.; Horstmyer, J.; Chai, R.; Schally, A.; et al. Magneto-electric nanoparticles for delivery of antitumor peptides into glioblastoma cells by magnetic fields. Nanomedicine 2018, 13, 423–438. [Google Scholar] [CrossRef]
- Stimphil, E. Technobiology Paradigm in Nanomedicine: Treating Cancer with Magneto Electric Nanoparticles. Ph.D. Thesis, Florida International University, Miami, FL, USA, 2017; p. 58. [Google Scholar]
- Cherian, A.; Ajitha, K.C.; Iype, T.; Divya, K.P. Neurotuberculosis: An update. Acta Neurol. Belg. 2021, 121, 11–21. [Google Scholar] [CrossRef]
- Pardridge, W.M. Drug transport across the blood-brain barrier. J. Cereb. Blood Flow Metab. 2012, 32, 1959–1972. [Google Scholar] [CrossRef]
- Azarmi, M.; Maleki, H.; Nikkam, N.; Malekinejad, H. Transcellular brain drug delivery: A review on recent advancements. Int. J. Pharm. 2020, 586, 119582. [Google Scholar] [CrossRef]
- Pajouhesh, H.; Lenz, R.G. Medicinal Chemical Properties of Successful Central Nervous System Drugs. NeuroRx 2005, 2, 541–553. [Google Scholar] [CrossRef] [Green Version]
- Squibb, B.; Index, M. Isoniazid. Tuberculosis 2008, 88, 112–116. [Google Scholar] [CrossRef]
- Lakshminarayana, S.B.; Huat, T.B.; Ho, P.C.; Manjunatha, U.H.; Dartois, V.; Dick, T.; Rao, S.P.S. Comprehensive physicochemical, pharmacokinetic and activity profiling of anti-TB agents. J. Antimicrob. Chemother. 2015, 70, 857–867. [Google Scholar] [CrossRef] [PubMed]
- Mitchison, D.A. Role of individual drugs in chemotherapy of tuberculosis. Int. J. Tuberc. Lung Dis. 2000, 4, 796–806. [Google Scholar] [PubMed]
- Djukic, M.; Munz, M.; Sörgel, F.; Holzgrabe, U.; Eiffert, H.; Nau, R. Overton’s rule helps to estimate the penetration of anti-infectives into patients’ cerebrospinal fluid. Antimicrob. Agents Chemother. 2012, 56, 979–988. [Google Scholar] [CrossRef] [PubMed]
- Nau, R.; Sörgel, F.; Eiffert, H. Penetration of drugs through the blood-cerebrospinal fluid/blood-brain barrier for treatment of central nervous system infections. Clin. Microbiol. Rev. 2010, 23, 858–883. [Google Scholar] [CrossRef] [Green Version]
- Me, M. Rifampin. Tuberculosis 2008, 88, 151–154. [Google Scholar] [CrossRef]
- Sousa, M.; Pozniak, A.; Boffito, M. Pharmacokinetics and pharmacodynamics of drug interactions involving rifampicin, rifabutin and antimalarial drugs. J. Antimicrob. Chemother. 2008, 62, 872–878. [Google Scholar] [CrossRef]
- Donald, P.R. Cerebrospinal fluid concentrations of antituberculosis agents in adults and children. Tuberculosis 2010, 90, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Jenkin, G. Pyrazinamide. In Kucers the Use of Antibiotics: A Clinical Review of Antibacterial, Antifungal, Antiparasitic, and Antiviral Drugs, 7th ed.; CRC Press: Boca Raton, FL, USA, 2017; Volume 88, pp. 2361–2368. [Google Scholar] [CrossRef]
- Chiang, S.S.; Starke, J.R. Mycobacterium tuberculosis. In Principles and Practice of Pediatric Infectious Diseases, 5th ed.; Elsevier Inc.: Philadelphia, PA, USA, 2018. [Google Scholar] [CrossRef]
- Allen, L.V. Ethambutol Hydrochloride Compounded Oral Suspension USP (100mg/mL). US Pharm 2017, 42, 48–49. [Google Scholar]
- Handoko, R.; Spudich, S. Treatment of Central Nervous System Manifestations of HIV in the Current Era. Semin. Neurol. 2019, 39, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Decloedt, E.; Rosenkranz, B.; Maartens, G.; Joska, J. Central Nervous System Penetration of Antiretroviral Drugs: Pharmacokinetic, Pharmacodynamic and Pharmacogenomic Considerations. Clin. Pharmacokinet. 2015, 54, 581–598. [Google Scholar] [CrossRef]
- Psimadas, D.; Georgoulias, P.; Valotassiou, V.; Loudos, G. Molecular Nanomedicine Towards Cancer. J. Pharm. Sci. 2012, 101, 2271–2280. [Google Scholar] [CrossRef]
- Ford, J.; Khoo, S.H.; Back, D.J. The intracellular pharmacology of antiretroviral protease inhibitors. J. Antimicrob. Chemother. 2004, 54, 982–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obembe, A.O.; Umoren, E.B.; Osim, E.E. Influence of Nevirapine on Gastrointestinal Function. J. Gastrointest. Dig. Syst. 2015, 5, 2. [Google Scholar] [CrossRef] [Green Version]
- Kimulwo, M.; Okendo, J.; Aman, R.A.; Ogutu, B.R.; Kokwaro, G.O.; Ochieng, D.J.; Muigai, A.W.T.; Oloo, F.A.; Ochieng, W. Plasma nevirapine concentrations predict virological and adherence failure in Kenyan HIV-1 infected patients with extensive antiretroviral treatment exposure. PLoS ONE 2017, 12, e0172960. [Google Scholar] [CrossRef] [Green Version]
- Rojas-Celis, V.; Valiente-Echeverria, F.; Soto-Rifo, R.; Toro-Ascuy, D. New Challenges of HIV-1 Infection: How HIV-1 Attacks and Resides in the Central Nervous System. Cells 2019, 8, 1245. [Google Scholar] [CrossRef] [Green Version]
- Kasinathan, N.; Jagani, H.V.; Alex, A.T.; Volety, S.M.; Rao, J.V. Strategies for delivery to the central nervous system by systemic route. Drug Deliv. 2015, 22, 243–257. [Google Scholar] [CrossRef]
- Paul, A.; Zhang, B.; Mohapatra, S.; Li, G.; Li, Y.; Gazit, E.; Segal, D. Novel mannitol-based small molecules for inhibiting aggregation of α-synuclein amyloids in Parkinson’s disease. Front. Mol. Biosci. 2019, 6, 16. [Google Scholar] [CrossRef] [Green Version]
- Dong, X. Current strategies for brain drug delivery. Theranostics 2018, 8, 1481–1493. [Google Scholar] [CrossRef] [PubMed]
- Le, T.N.; Blakley, B.W. Mannitol and the blood-labyrinth barrier. J. Otolaryngol. Head Neck Surg. 2017, 46, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, F.Y.; Wong, T.T.; Teng, M.C.; Liu, R.S.; Lu, M.; Liang, H.F.; Wei, M.C. Focused ultrasound and interleukin-4 receptor-targeted liposomal doxorubicin for enhanced targeted drug delivery and antitumor effect in glioblastoma multiforme. J. Control. Release 2012, 160, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Rosenblatt, R.B.; Frank, J.A.; Burks, S.R. Cytosolic Ca2+ transients during pulsed focused ultrasound generate reactive oxygen species and cause DNA damage in tumor cells. Theranostics 2020, 11, 602–613. [Google Scholar] [CrossRef]
- McMahon, D.; Hynynen, K. Acute inflammatory response following increased blood-brain barrier permeability induced by focused ultrasound is dependent on microbubble dose. Theranostics 2017, 7, 3989–4000. [Google Scholar] [CrossRef] [PubMed]
- Bellettato, C.M.; Scarpa, M. Possible strategies to cross the blood–brain barrier. Ital. J. Pediatr. 2018, 44 (Suppl. 2), 127–133. [Google Scholar] [CrossRef]
- Das, M.K.; Chakraborty, T. Progress in brain delivery of Anti-HIV drugs. J. Appl. Pharm. Sci. 2015, 5, 154–164. [Google Scholar] [CrossRef] [Green Version]
- Harikishore, A.; Yoon, H.S. Immunophilins: Structures, Mechanisms and Ligands. Curr. Mol. Pharmacol. 2015, 9, 37–47. [Google Scholar] [CrossRef]
- Hamilton, G.S. Immunophilin ligands for the treatment of neurological disorders. Expert Opin. Ther. Pat. 1998, 8, 1109–1124. [Google Scholar] [CrossRef]
- Deb, P.K.; Al-Attraqchi, O.; Chandrasekaran, B.; Paradkar, A.; Tekade, R.K. Protein/Peptide Drug Delivery Systems: Practical Considerations in Pharmaceutical product Development. In Basic Fundamentals of Drug Delivery; Academic Press: Cambridge, MA, USA, 2019; pp. 651–684. [Google Scholar] [CrossRef]
- Jain, K.K. Nanobiotechnology-based drug delivery to the central nervous system. Neurodegener. Dis. 2007, 4, 287–291. [Google Scholar] [CrossRef]
- Curley, S.M.; Cady, N.C. Biologically-derived nanomaterials for targeted therapeutic delivery to the brain. Sci. Prog. 2018, 101, 273–292. [Google Scholar] [CrossRef]
- Ren, J.; Shen, S.; Wang, D.; Xi, Z.; Guo, L.; Pang, Z.; Qian, Y.; Sun, X.; Jiang, X. The targeted delivery of anticancer drugs to brain glioma by PEGylated oxidized multi-walled carbon nanotubes modified with angiopep-2. Biomaterials 2012, 33, 3324–3333. [Google Scholar] [CrossRef] [PubMed]
- Belur, L.R.; Temme, A.; Podetz-Pedersen, K.M.; Riedl, M.; Vulchanova, L.; Robinson, N.; Hanson, L.R.; Kozarsky, K.F.; Orchard, P.J.; Freyll, W.H.; et al. Intranasal adeno-associated virus mediated gene delivery and expression of human iduronidase in the central nervous system: A noninvasive and effective approach for prevention of neurologic disease in mucopolysaccharidosis type I. Hum. Gene Ther. 2017, 28, 576–587. [Google Scholar] [CrossRef]
- Joshy, K.S.; Sharma, C.P. Blood compatible nanostructured lipid carriers for the enhanced delivery of azidothymidine to brain. Adv. Sci. Lett. 2012, 6, 47–55. [Google Scholar] [CrossRef]
- Chattopadhyay, N.; Zastre, J.; Wong, H.L.; Wu, X.Y.; Bendayan, R. Solid lipid nanoparticles enhance the delivery of the HIV protease inhibitor, atazanavir, by a human brain endothelial cell line. Pharm. Res. 2008, 25, 2262–2271. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Guo, K.; Lu, J.; Venkatraman, S.S.; Luo, D.; Ng, K.C.; Ling, E.; Moochhala, S.; Yang, Y. Biologically active core/shell nanoparticles self-assembled from cholesterol-terminated PEG-TAT for drug delivery across the blood-brain barrier. Biomaterials 2008, 29, 1509–1517. [Google Scholar] [CrossRef]
- Zou, Z.; Shen, Q.; Pang, Y.; Li, X.; Chen, Y.; Wang, X.; Luo, X.; Wu, Z.; Bao, Z.; Zhang, J.; et al. The synthesized transporter K16APoE enabled the therapeutic HAYED peptide to cross the blood-brain barrier and remove excess iron and radicals in the brain, thus easing Alzheimer’s disease. Drug Deliv. Transl. Res. 2019, 9, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Su, X.; Kells, A.P.; Salegio, E.A.; Richardson, R.M.; Hadaczek, P.; Beyer, J.; Bringas, J.; Pivirotto, P.; Forsayeth, J.; Bankiewicz, K.S. Real-time MR imaging With Gadoteridol Predicts Distribution of Transgenes After Convection-enhanced Delivery of AAV2 Vectors. Mol. Ther. 2010, 18, 1490–1495. [Google Scholar] [CrossRef] [PubMed]
- Giugliani, R.; Giugliani, L.; Poswar, F.; Donis, K.C.; Corte, A.D.; Schmidt, M.; Boado, R.J.; Nestrasil, I.; Nguyen, C.; Chen, S.; et al. Neurocognitive and somatic stabilization in pediatric patients with severe Mucopolysaccharidosis Type i after 52 weeks of intravenous brain-penetrating insulin receptor antibody-iduronidase fusion protein (valanafusp alpha): An open label phase 1-2 trial. Orphanet J. Rare Dis. 2018, 13, 110. [Google Scholar] [CrossRef]
- Małkiewicz, M.A.; Szarmach, A.; Sabisz, A.; Cubala, W.J.; Szurowska, E.; Winklewski, P.J. Blood-brain barrier permeability and physical exercise. J. Neuroinflammation 2019, 16, 15. [Google Scholar] [CrossRef]
- Abdulkhaleq, L.A.; Assi, M.A.; Abdullah, R.; Zamri-Saad, M.; Taufiq-Yap, Y.H.; Hezmee, M.N.M. The crucial roles of inflammatory mediators in inflammation: A review. Vet. World 2018, 11, 627–635. [Google Scholar] [CrossRef] [Green Version]
- Emerich, D.F.; Dean, R.L.; Osborn, C.; Bartus, R.T. The Development of the Bradykinin Agonist Labradimil as a Means to Increase the Permeability of the Blood-Brain Barrier: From Concept to Clinical Evaluation. Clin. Pharmacokinet. 2001, 40, 105–123. [Google Scholar] [CrossRef] [PubMed]
- Balla, A.; Goli, D. Formulation & evaluation of PLGA nanoparticles of ropinirole HCl for targeting brain. Indian J. Pharm. Sci. 2020, 82, 622–631. [Google Scholar] [CrossRef]
- Fisher, D.; Mentor, S. Are claudin-5 tight-junction proteins in the blood-brain barrier porous? Neural Regen. Res. 2020, 15, 1838–1839. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.A.; Bauer, J.; Flick, M.J.; Sikorski, S.L.; Nuriel, T.; Lassmann, H.; Degen, J.L.; Akassoglou, K. The fibrin-derived γ377-395 peptide inhibits microglia activation and suppresses relapsing paralysis in central nervous system autoimmune disease. J. Exp. Med. 2007, 204, 571–582. [Google Scholar] [CrossRef] [PubMed]
- Luo, S.; Ma, C.; Zhu, M.; Ju, W.; Yang, Y.; Wang, X. Application of Iron Oxide Nanoparticles in the Diagnosis and Treatment of Neurodegenerative Diseases With Emphasis on Alzheimer’s Disease. Front. Cell. Neurosci. 2020, 14, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otani, T.; Furuse, M. Tight Junction Structure and Function Revisited. Trends Cell Biol. 2020, 30, 805–817. [Google Scholar] [CrossRef]
- Pardridge, W.M. Treatment of alzheimer’s disease and blood–brain barrier drug delivery. Pharmaceuticals 2020, 13, 394. [Google Scholar] [CrossRef]
- Islam, Y.; Leach, A.G.; Smith, J.; Pluchino, S.; Coxonl, C.R.; Sivakumaran, M.; Downing, J.; Fatokun, A.A.; Teixido, M.; Ehtezazi, T. Peptide based drug delivery systems to the brain. Nano Express 2020, 1, 012002. [Google Scholar] [CrossRef]
- Viscusi, E.R.; Viscusi, A.R. Blood-brain barrier: Mechanisms governing permeability and interaction with peripherally acting μ-opioid receptor antagonists. Reg. Anesth. Pain Med. 2020, 45, 688–695. [Google Scholar] [CrossRef]
- Betzer, O.; Shilo, M.; Opochinsky, R.; Barnoy, E.; Motiei, M.; Okun, E.; Yadid, G.; Popovtzer, R. The effect of nanoparticle size on the ability to cross the blood-brain barrier: An in vivo study. Nanomedicine 2017, 12, 1533–1546. [Google Scholar] [CrossRef]
- Teleanu, D.M.; Chircov, C.; Grumezescu, A.M.; Volceanov, A.; Teleanu, R.I. Blood-brain delivery methods using nanotechnology. Pharmaceutics 2018, 10, 269. [Google Scholar] [CrossRef] [Green Version]
- Roth, C.C.; Barnes, R.A.; Ibey, B.L.; Beier, H.T.; Mimun, L.C.; Maswadi, S.M.; Shadaram, M.; Glickman, R.D. Characterization of pressure transients generated by nanosecond electrical pulse (nsEP) exposure. Sci. Rep. 2015, 5, 15063. [Google Scholar] [CrossRef] [Green Version]
- Sridhara, V.; Joshi, R.P. Numerical study of lipid translocation driven by nanoporation due to multiple high-intensity, ultrashort electrical pulses. Biochim. Biophys. Acta—Biomembr. 2014, 1838, 902–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pakhomov, A.G.; Bowman, A.M.; Ibey, B.L.; Andre, F.M.; Pakhomova, O.N.; Schoenbach, K.H. Analysis ofconductance ofinward-rectifyingmembrane pores induced by nanosecond electric pulses inGH3 (murine pituitary) and CHO-K1 cells. Biochem. Biophys. Res. Commun. 2009, 385, 181–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, V.; Kesharwani, P.; Amin, M.C.I.M.; Iyer, A. (Eds.) Nanotechnology-Based Approaches for Targeting and Delivery of Drugs and Genes; Academic Press: Cambridge, MA, USA, 2017; p. 506. [Google Scholar]
- Moen, E.K.; Ibey, B.L.; Beier, H.T.; Armani, A.M. Quantifying pulsed electric field-induced membrane nanoporation in single cells. Biochim. Biophys. Acta—Biomembr. 2016, 1858, 2795–2803. [Google Scholar] [CrossRef] [PubMed]
- Lungu, M.; Neculae, A.; Bunoiu, M.; Biris, C. Nanoparticles’ Promises and Risks: Characterization, Manipulation, and Potential Hazards to Humanity and the Environment; Springer: Cham, Switzerland, 2015; pp. 1–355. [Google Scholar] [CrossRef]
- Shen, Z.; Fisher, A.; Liu, W.K.; Li, Y. 1—PEGylated “stealth” nanoparticles and liposomes. In Engineering of Biomaterials for Drug Delivery Systems; Woodhead Publishing: Sawston, UK, 2018; pp. 1–26. [Google Scholar]
- Dube, A. Nanomedicines for infectious diseases. Pharm. Res. 2019, 36, 63. [Google Scholar] [CrossRef] [Green Version]
- Patra, J.K.; Das, G.; Fraceto, L.F.; Campos, E.V.R.; Rodriguez-Torres, M.P.; Acosta-Torres, L.S.; Diaz-Torres, L.A.; Grillo, R.; Swamy, M.K.; Sharma, S.; et al. Nano based drug delivery systems: Recent developments and future prospects. J. Nanobiotechnol. 2018, 16, 71. [Google Scholar] [CrossRef] [Green Version]
- Hadjikhani, A.; Rodzinski, A.; Wang, P.; Nagesetti, A.; Guduru, R.; Liang, P.; Runowicz, C.; Shahbazmohamadi, S.; Khizroev, S. Biodistribution and clearance of magnetoelectric nanoparticles for nanomedical applications using energy dispersive spectroscopy. Nanomedicine 2017, 12, 1801–1822. [Google Scholar] [CrossRef]
- Pandey, P.; Ghimire, G.; Garcia, J.; Rubfiaro, A.; Wang, X.; Tomitaka, A.; Nair, M.; Kaushik, A.; He, J. Single-Entity Approach to Investigate Surface Charge Enhancement in Magnetoelectric Nanoparticles Induced by AC Magnetic Field Stimulation. ACS Sens. 2020, 6, 340–347. [Google Scholar] [CrossRef]
- Corral-Flores, V.; Bueno-Baqués, D.; Ziolo, R.F. Synthesis and characterization of novel CoFe2O4-BaTiO3 multiferroic core-shell-type nanostructures. Acta Mater. 2010, 58, 764–769. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, S.; Xiao, Z.; Liu, X.; Wu, C.; Wu, K.; Liu, A.; Wei, D.; Sun, J.; Zhou, L.; et al. Magnetoelectric Nanoparticles Incorporated Biomimetic Matrix for Wireless Electrical Stimulation and Nerve Regeneration. Adv. Healthc. Mater. 2021, 10, 2100695. [Google Scholar] [CrossRef] [PubMed]
- Khizroev, S.; Nair, M.; Liang, P.; Runowicz, C.; Guduru, R. On-Demand Release Using Magneto-Electric Nanoparticles. U.S. Patent 9895549B2, 20 February 2018. [Google Scholar]
- Guduru, R.; Liang, P.; Runowicz, C.; Nair, M.; Atluri, V.; Khizroev, S. Magneto-electric Nanoparticles to Enable Field-controlled High-Specificity Drug Delivery to Eradicate Ovarian Cancer Cells. Sci. Rep. 2013, 3, 2953. [Google Scholar] [CrossRef] [PubMed]
- Napotnik, T.B.; Miklavčič, D. In vitro electroporation detection methods—An overview. Bioelectrochemistry 2018, 120, 166–182. [Google Scholar] [CrossRef]
- Nair, M.; Guduru, R.; Liang, P.; Hong, J.; Sagar, V.; Khizroev, S. Externally on-demand release of anti-HIV drug using magneto-electric nanoparticles as carriers. Nat. Commun. 2013, 4, 1707. [Google Scholar] [CrossRef]
- Kaushik, A.; Nikkhah-Moshaie, R.N.; Bhardwaj, V.; Atluri, V.; Jayant, R.D.; Yndart, A.; Kateb, B.; Pala, N.; Nair, M. Investigation of ac-magnetic field stimulated nanoelectroporation of magneto-electric nano-drug-carrier inside CNS cells. Sci. Rep. 2017, 7, 45663. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, M.; Kaushik, A.; Lapierre, J.; Dever, S.M.; El-Hage, N.; Nair, M. Electro-Magnetic Nano-Particle Bound Beclin1 siRNA Crosses the Blood–Brain Barrier to Attenuate the Inflammatory Effects of HIV-1 Infection in Vitro. J. Neuroimmune Pharmacol. 2017, 12, 120–132. [Google Scholar] [CrossRef] [Green Version]
- Kamran, M.; Ullah, A.; Mehmood, Y.; Nadeem, K.; Krenn, H. Role of SiO2 coating in multiferroic CoCr2O4 nanoparticles. AIP Adv. 2017, 7, 025011. [Google Scholar] [CrossRef] [Green Version]
- Biehl, P.; von der Lühe, M.; Dutz, S.; Schacher, F.H. Synthesis, characterization, and applications of magnetic nanoparticles featuring polyzwitterionic coatings. Polymers 2018, 10, 91. [Google Scholar] [CrossRef] [Green Version]
- Kaushik, A.; Yndart, A.; Atluri, V.; Tiwari, S.; Tomitaka, A.; Jayant, R.D.; Gupta, P.; Alvarez-Carbonell, D.; Khalili, K.; Nair, M. Magnetically guided non-invasive CRISPR-Cas9/gRNA delivery across blood-brain barrier to eradicate latent HIV-1 infection. Sci. Rep. 2019, 9, 3928. [Google Scholar] [CrossRef] [Green Version]
- Soriano, V.; Barreiro, P.; de Mendoza, C. Making 2D topological polymers a reality. Nat. Mater. 2020, 19, 823–824. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mhambi, S.; Fisher, D.; Tchokonte, M.B.T.; Dube, A. Permeation Challenges of Drugs for Treatment of Neurological Tuberculosis and HIV and the Application of Magneto-Electric Nanoparticle Drug Delivery Systems. Pharmaceutics 2021, 13, 1479. https://doi.org/10.3390/pharmaceutics13091479
Mhambi S, Fisher D, Tchokonte MBT, Dube A. Permeation Challenges of Drugs for Treatment of Neurological Tuberculosis and HIV and the Application of Magneto-Electric Nanoparticle Drug Delivery Systems. Pharmaceutics. 2021; 13(9):1479. https://doi.org/10.3390/pharmaceutics13091479
Chicago/Turabian StyleMhambi, Sinaye, David Fisher, Moise B. Tchoula Tchokonte, and Admire Dube. 2021. "Permeation Challenges of Drugs for Treatment of Neurological Tuberculosis and HIV and the Application of Magneto-Electric Nanoparticle Drug Delivery Systems" Pharmaceutics 13, no. 9: 1479. https://doi.org/10.3390/pharmaceutics13091479