
Preparation and In Vivo Evaluation of a Lidocaine Self-Nanoemulsifying Ointment with Glycerol Monostearate for Local Delivery

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.2.1. Preparation and Rheological Characterization of Lidocaine Ointment
2.2.2. Physicochemical Characterization of Lidocaine Ointment
2.2.3. In Vitro Dissolution Test of Lidocaine Ointment
2.2.4. Ex Vivo Skin Permeation and Raman Mapping of Lidocaine Ointment
2.2.5. In Vivo Tail-Flick Test of Lidocaine Ointment
2.2.6. Statistical Analysis
3. Results
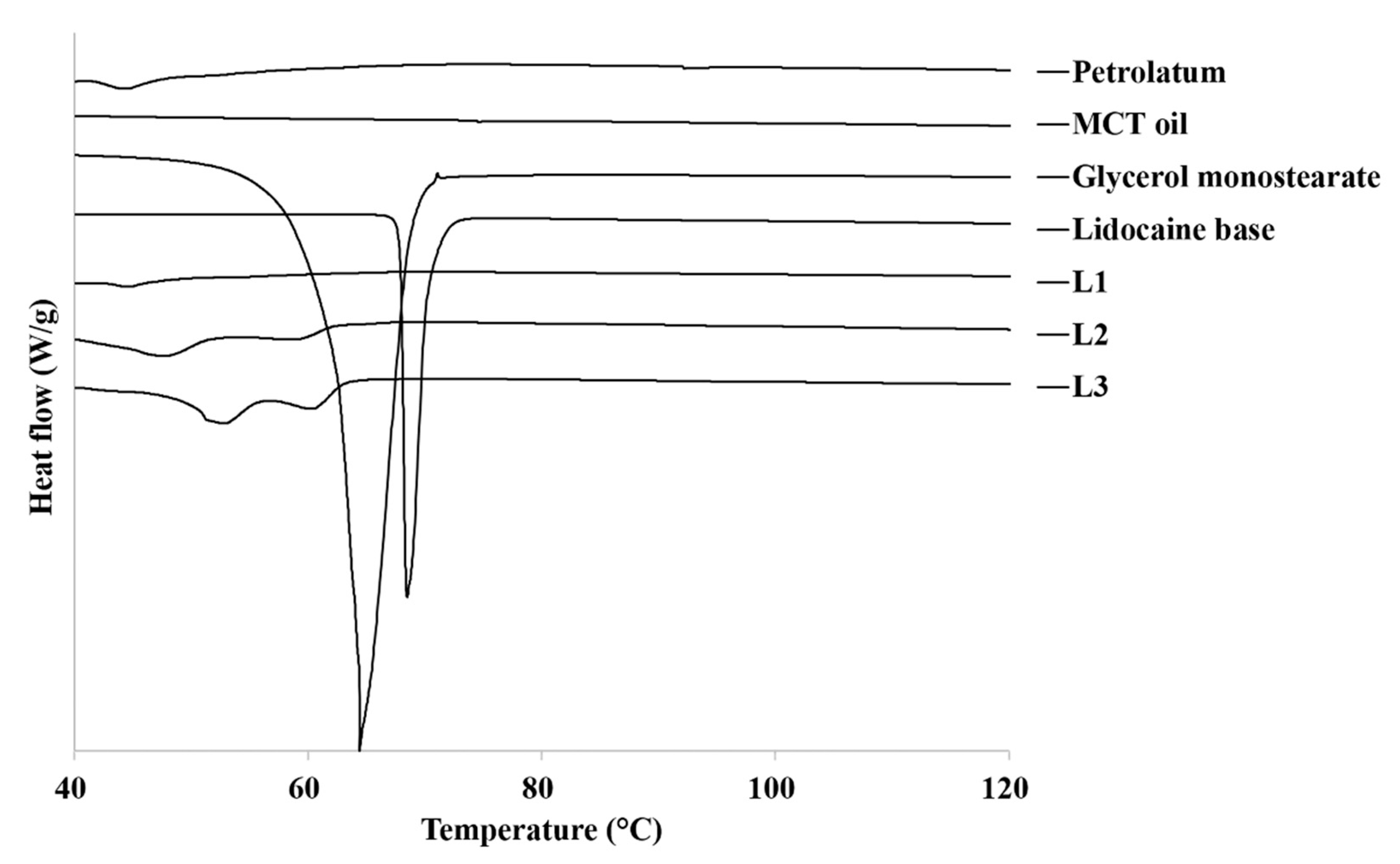
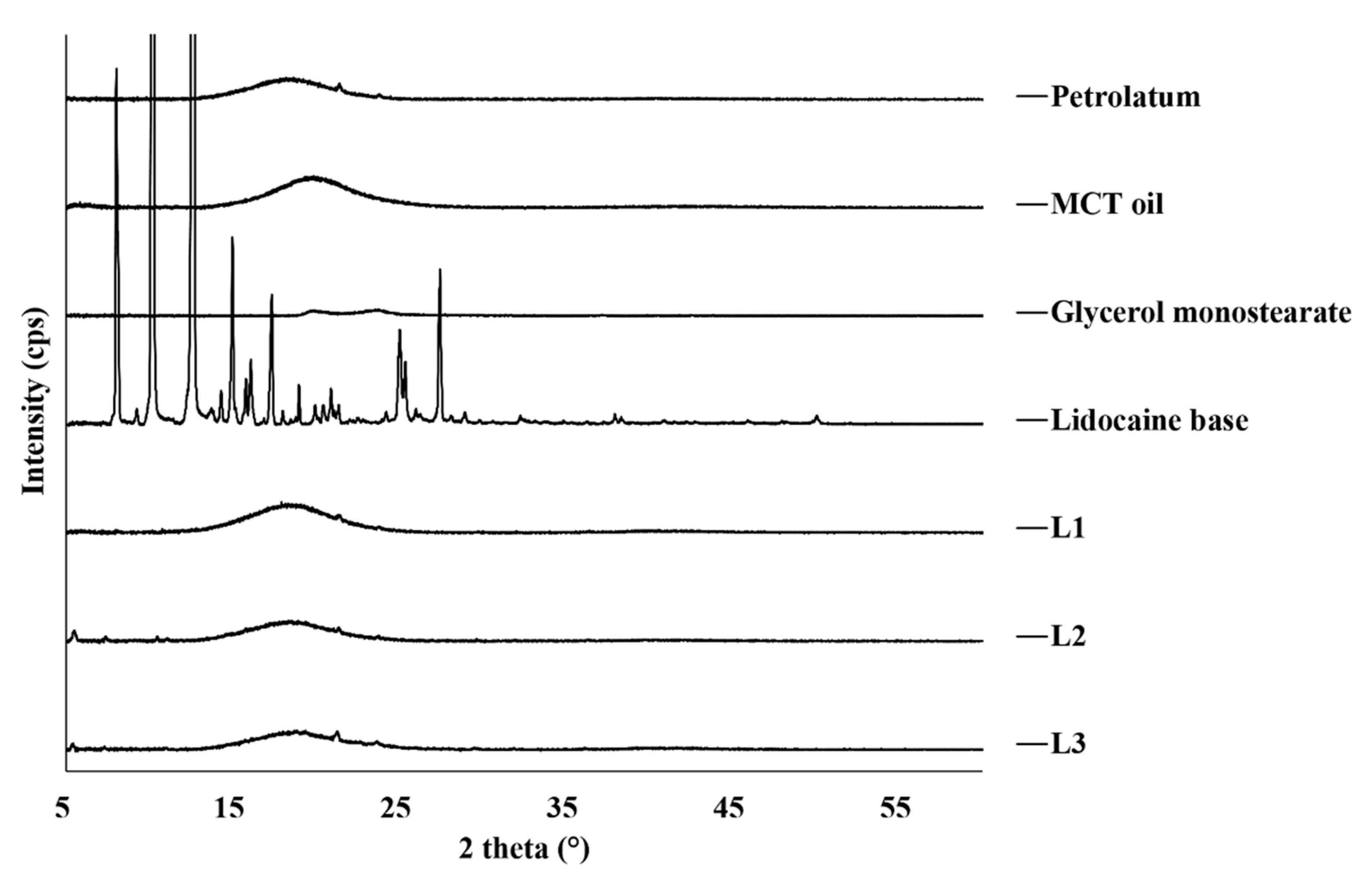
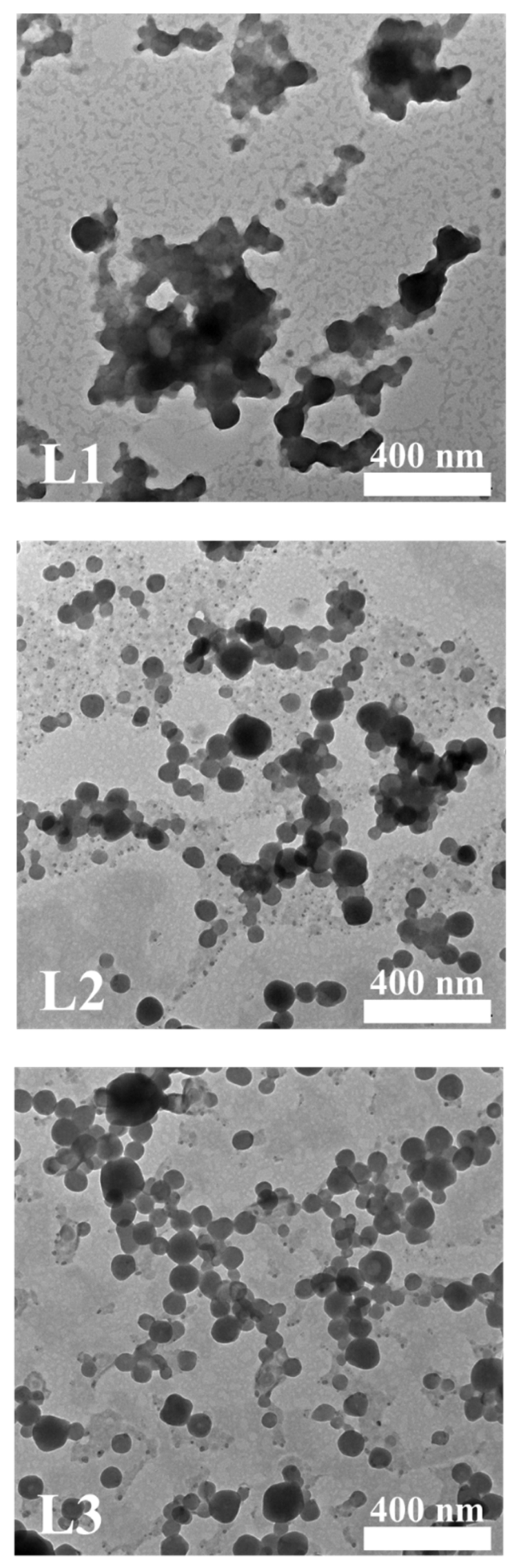
3.1. Physicochemical Characterization of Lidocaine Ointment
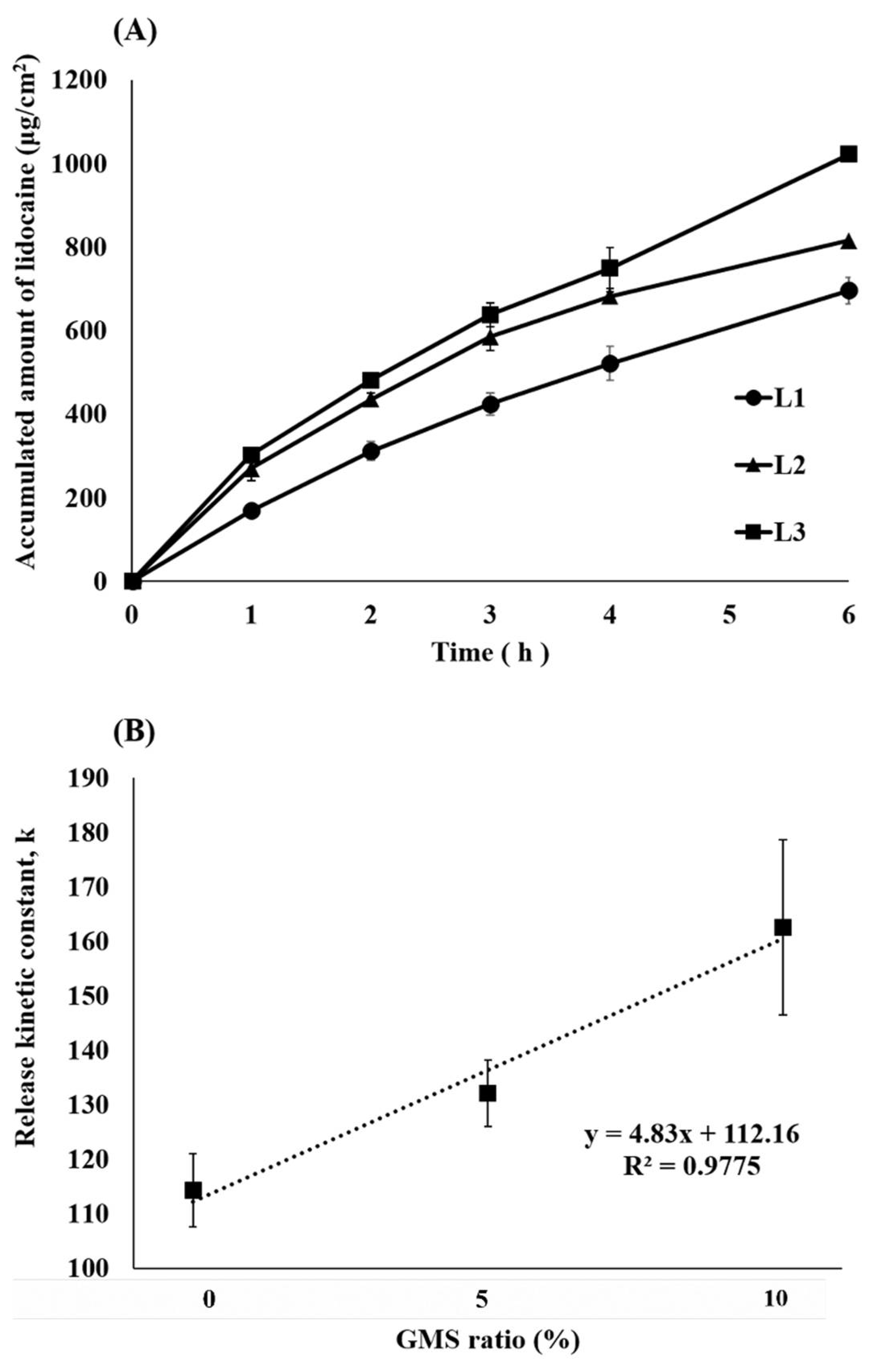
3.2. In Vitro Dissolution Test of Lidocaine Ointment
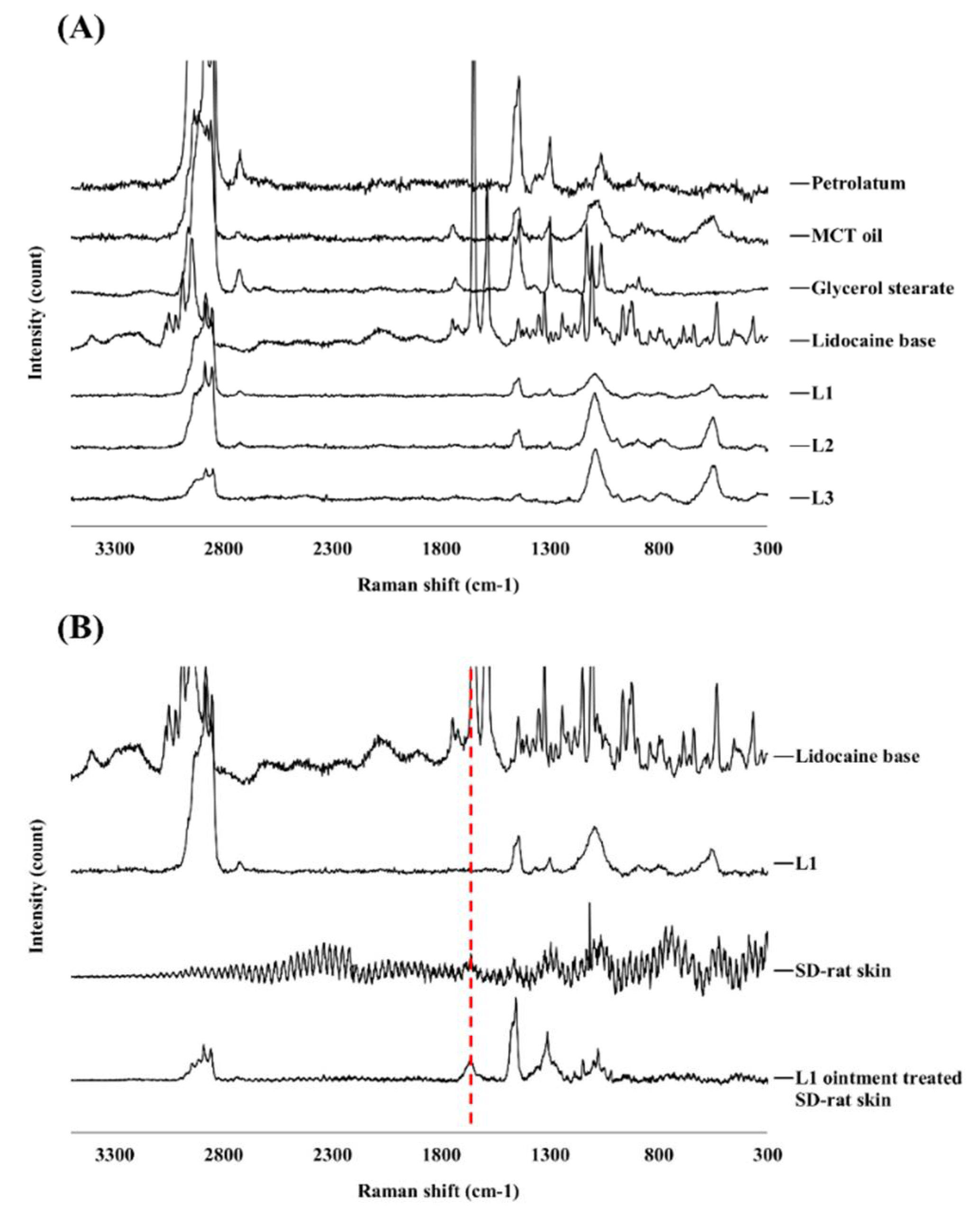
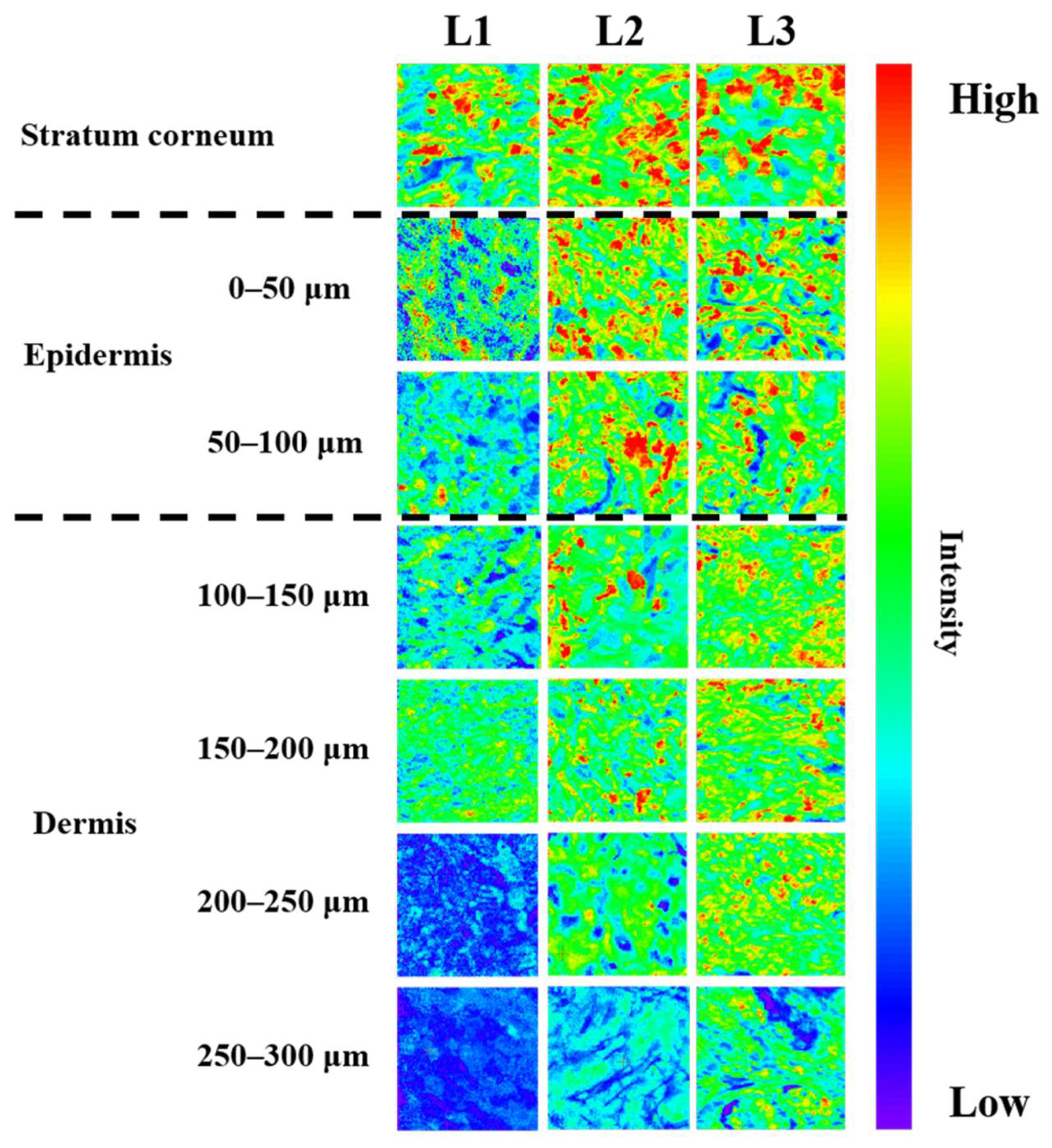
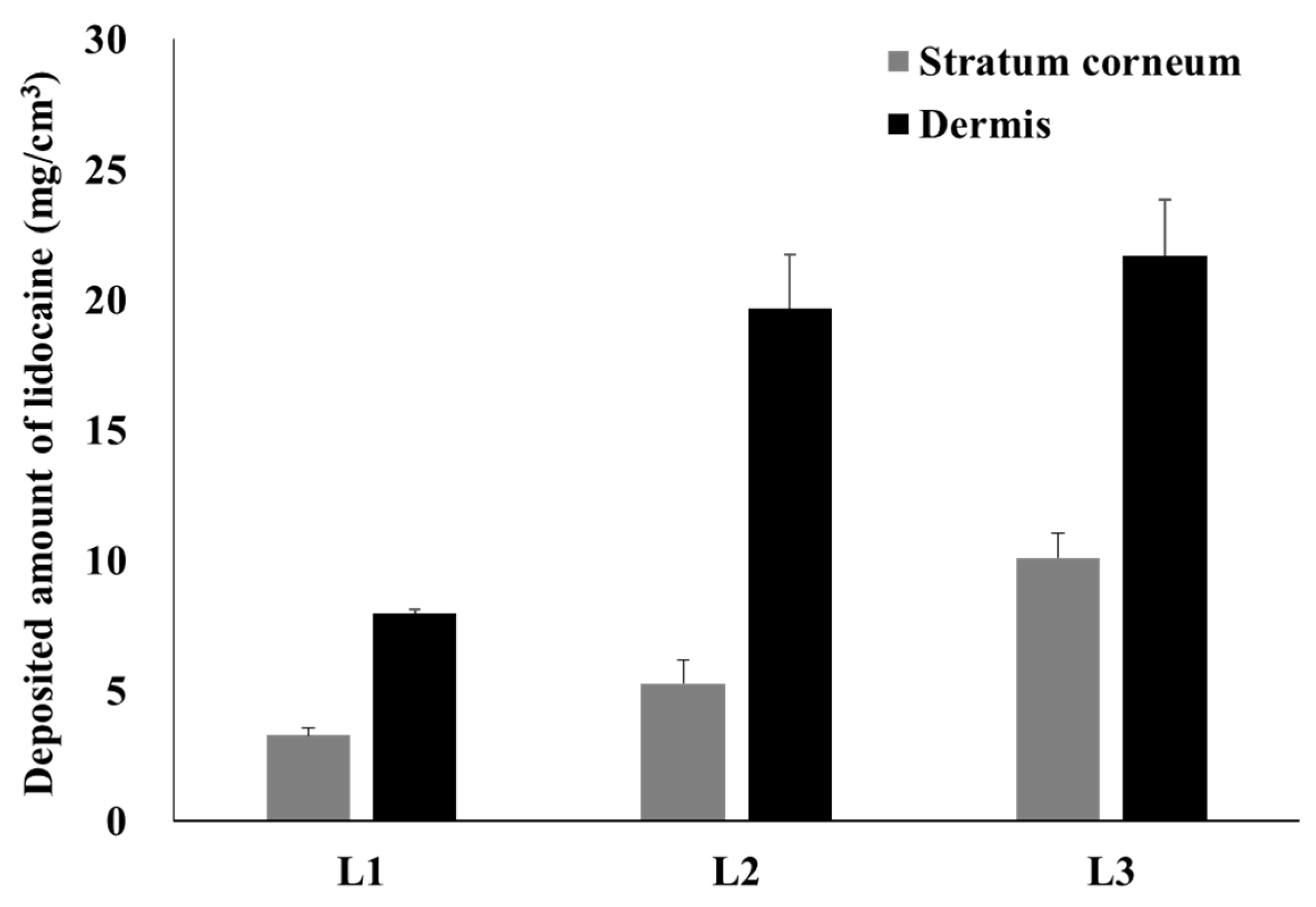
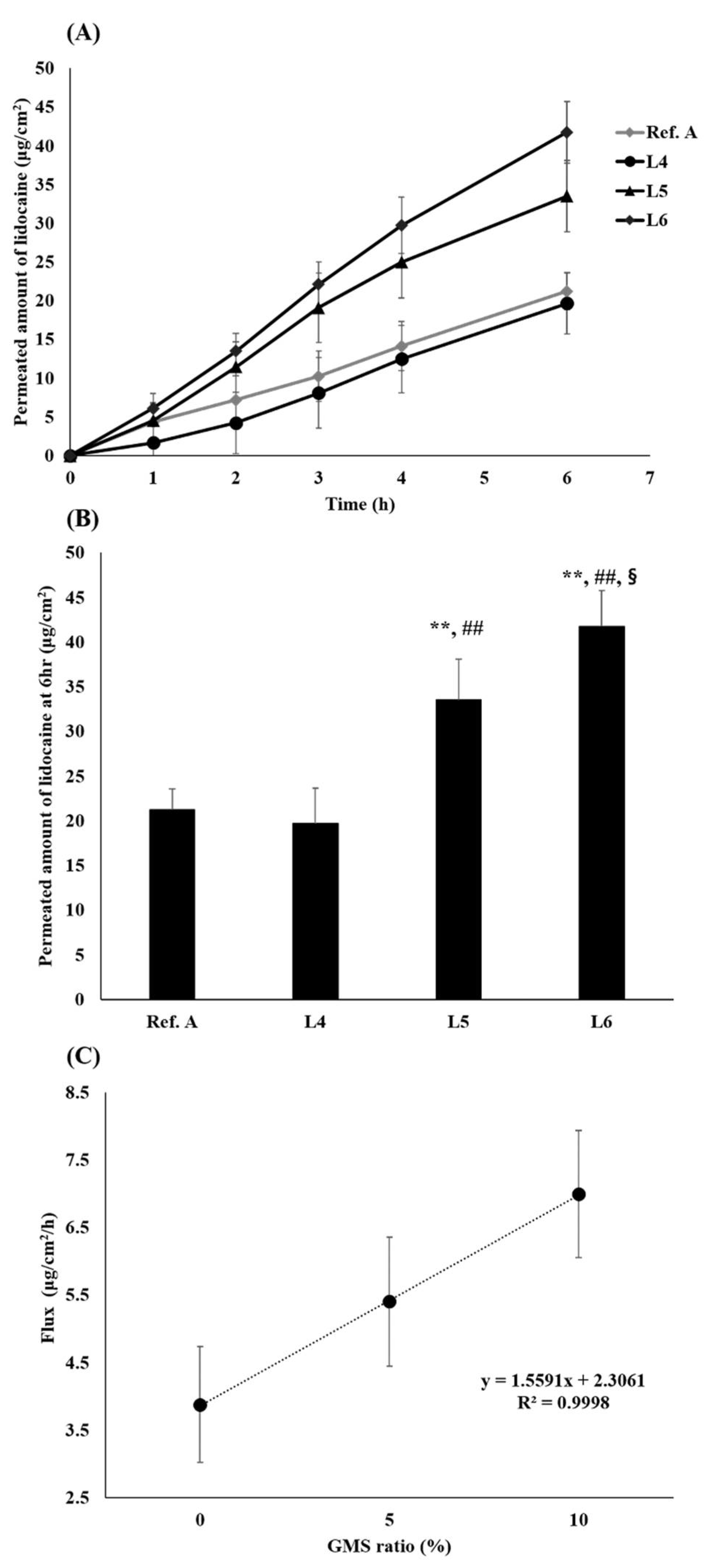
3.3. Ex Vivo Skin Permeation Test and Raman Mapping of Lidocaine Ointment
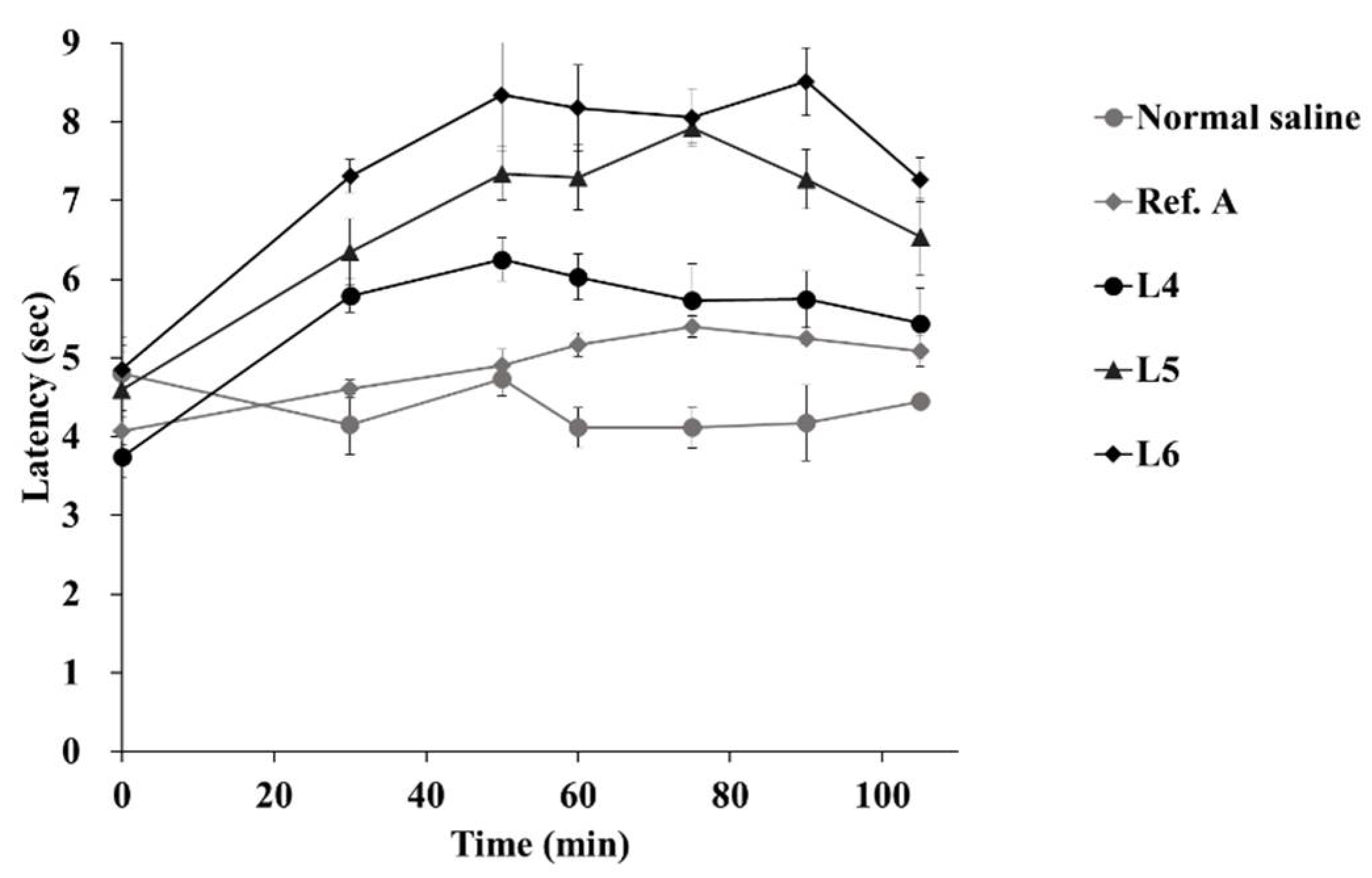
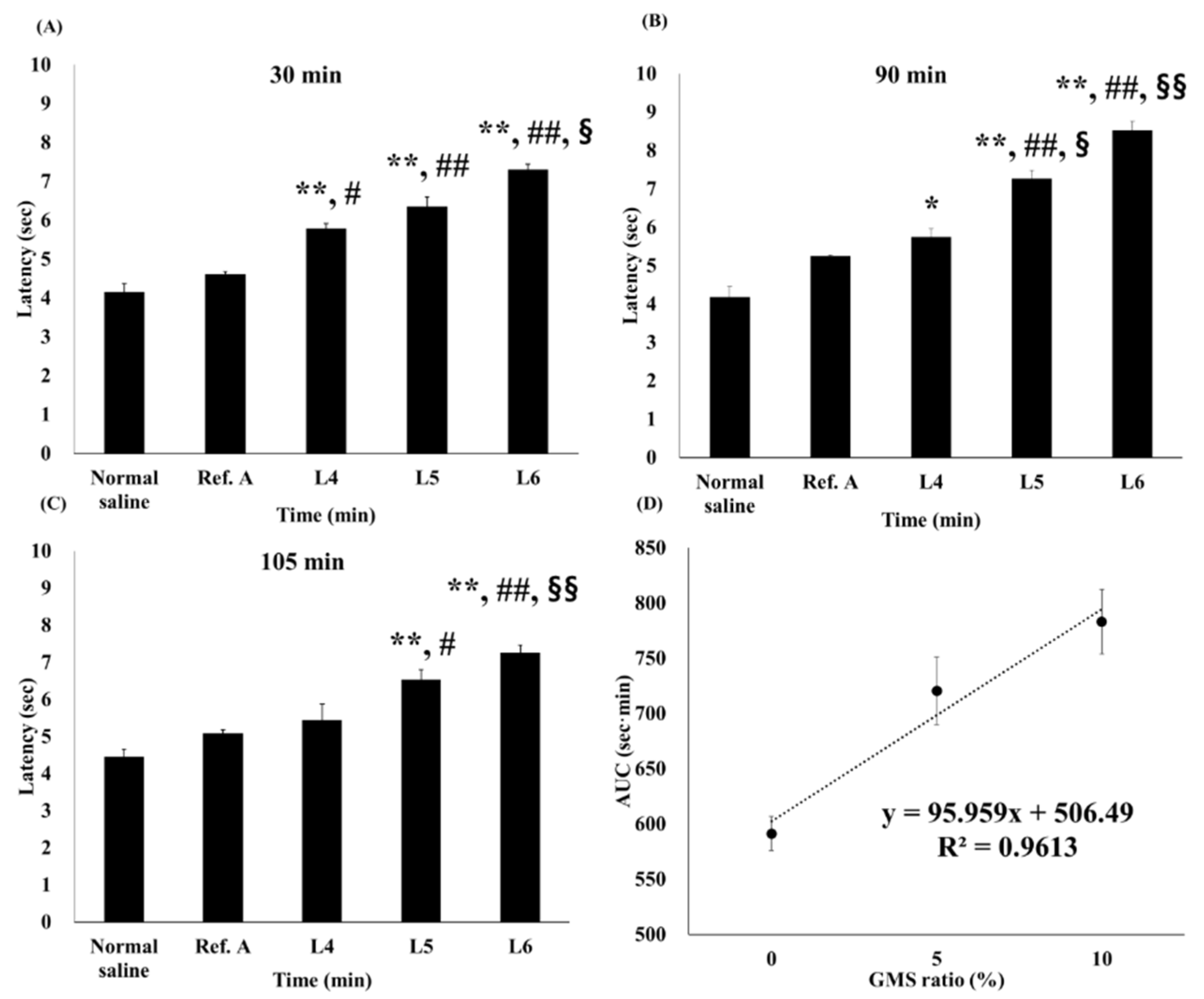
3.4. In Vivo Tail-Flick Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sun, Z.; Sun, M.J. Review of hemorrhoid disease: Presentation and management. Clin. Colon Rectal Surg. 2016, 29, 22–29. [Google Scholar]
- Johanson, J.F.; Sonnenberg, A.J.G. The prevalence of hemorrhoids and chronic constipation: An epidemiologic study. Gastroenterology 1990, 98, 380–386. [Google Scholar] [PubMed]
- Mongelli, F.; Treglia, G.; La Regina, D.; Di Giuseppe, M.; Galafassi, J.; Majno-Hurst, P.E.; Christoforidis, D. Pudendal nerve block in hemorrhoid surgery: A systematic review and meta-analysis. Dis. Colon Rectum 2021, 64, 617–631. [Google Scholar] [CrossRef] [PubMed]
- Van Tol, R.R.; Kleijnen, J.; Watson, A.J.M.; Jongen, J.; Altomare, D.F.; Qvist, N.; Higuero, T.; Muris, J.W.M.; Breukink, S.O. European society of coloproctology: Guideline for haemorrhoidal disease. Colorectal Dis. 2020, 22, 650–662. [Google Scholar] [PubMed]
- Lorenc, Z.; Gökçe, Ö. Tribenoside and lidocaine in the local treatment of hemorrhoids: An overview of clinical evidence. Eur. Rev. Med. Pharm. Sci. 2016, 20, 2742–2751. [Google Scholar]
- Davis, B.R.; Lee-Kong, S.A.; Migaly, J.; Feingold, D.L.; Steele, S.R. The American society of colon and rectal surgeons clinical practice guidelines for the management of hemorrhoids. Dis. Colon Rectum 2018, 61, 284–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muldoon, R. Review of American society of colon and rectal surgeons clinical practice guidelines for the management of hemorrhoids. JAMA Surg. 2020, 155, 773–774. [Google Scholar] [CrossRef]
- Asteria, C.R.; Lauretta, A.; Martellucci, J.; Lucchini, G.; Chiodaroli, R.; Todaro, A.; Infantino, A. Does anaesthesia change severity of haemorrhoidal disease? A prospective and multicentre case-control study on haemorrhoidal disease assessment in two different settings: Outpatient and operating theatre. Int. J. Colorectal Dis. 2016, 31, 1529–1531. [Google Scholar] [CrossRef]
- Tarik, S.; Barazanchi, A.W.H.; Hill, A.G. Evidence-based management of pain after excisional haemorrhoidectomy surgery: A PROSPECT review update. World J. Surg. 2017, 41, 603–614. [Google Scholar]
- Barazanchi, A.W.H.; MacFater, W.S.; Rahiri, J.L.; Tutone, S.; Hill, A.G.; Joshi, G.P. Evidence-based management of pain after laparoscopic cholecystectomy: A PROSPECT review update. Br. J. Anaesth. 2018, 121, 787–803. [Google Scholar] [CrossRef] [Green Version]
- Altomare, D.F.; Giannini, I. Pharmacological treatment of hemorrhoids: A narrative review. Expert Opin. Pharm. 2013, 14, 2343–2349. [Google Scholar] [CrossRef] [PubMed]
- Zagriadskiĭ, E.A.; Bogomazov, A.M.; Golovko, E.B. Conservative treatment of hemorrhoids: Results of an observational multicenter study. Adv. Ther. 2018, 35, 1979–1992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinberg, L.; Peake, B.; Tan, C.; Nikfarjam, M. Pharmacokinetics and pharmacodynamics of lignocaine: A review. World J. Anesth. 2015, 4, 17–29. [Google Scholar] [CrossRef]
- Gudin, J.; Nalamachu, S. Utility of lidocaine as a topical analgesic and improvements in patch delivery systems. Postgrad. Med. 2020, 132, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Dangol, M.; Kang, G.; Lahiji, S.F.; Yang, H.; Jang, M.; Ma, Y.; Li, C.; Lee, S.; Kim, C.; et al. Enhanced transdermal delivery by combined application of dissolving microneedle patch on serum-treated skin. Mol. Pharm. 2017, 14, 2024–2031. [Google Scholar] [CrossRef]
- Zhao, Z.; Lian, Y.; Zhu, Y.; Ye, H.; Liu, M.; Li, J. Depot lidocaine-loaded microemulsion for prolonged local anesthesia: Different efficacy model studies. J. Drug Deliv. Sci. Technol. 2020, 55, 101404. [Google Scholar] [CrossRef]
- Tadwee, I.K.; Gore, S.; Giradkar, P. Advances in topical drug delivery system: A review. Int. J. Pharm. Res. Sci. 2012, 1, 14–23. [Google Scholar]
- Kang, J.H.; Chon, J.; Kim, Y.I.; Lee, H.J.; Oh, D.W.; Lee, H.G.; Han, C.S.; Kim, D.W.; Park, C.W. Preparation and evaluation of tacrolimus-loaded thermosensitive solid lipid nanoparticles for improved dermal distribution. Int. J. Nanomed. 2019, 14, 5381–5396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobanko, J.F.; Miller, C.J.; Alster, T.S. Topical anesthetics for dermatologic procedures: A review. Derm. Surg. 2012, 38, 709–721. [Google Scholar] [CrossRef] [PubMed]
- Oskuie, A.B.; Nasrollahi, S.A.; Nafisi, S. Design, synthesis of novel vesicular systems using turpentine as a skin permeation enhancer. J. Drug Deliv. Sci. Technol. 2018, 43, 327–332. [Google Scholar] [CrossRef]
- Lee, H.J.; Oh, D.W.; Na, M.J.; Kim, D.W.; Yuk, D.Y.; Choi, H.C.; Lee, Y.B.; Han, G.; Park, C.W. Preparation and in vivo evaluation of lecithin-based microparticles for topical delivery of minoxidil. Arch. Pharm. Res. 2017, 40, 943–951. [Google Scholar] [CrossRef]
- Mehta, D.P.; Rathod, H.J.; Shah, D.P.; Shah, C.N. A review on microemulsion based gel: A recent approach for topical drug delivery system. Res. J. Pharm. Technol. 2015, 8, 118–126. [Google Scholar] [CrossRef]
- Kim, C.K..; Kim, J.; Chi, S.; Shim, C. Effect of fatty acids and urea on the penetration of ketoprofen through rat skin. Int. J. Pharm. 1993, 99, 109–118. [Google Scholar] [CrossRef]
- Dhal, S.; Pal, K.; Giri, S. Transdermal delivery of gold nanoparticles by a soybean oil-based oleogel under iontophoresis. ACS Appl. Bio Mater. 2020, 3, 7029–7039. [Google Scholar] [CrossRef]
- Oh, D.W.; Kang, J.H.; Lee, H.J.; Han, S.D.; Kang, M.H.; Kwon, Y.H.; Jun, J.H.; Kim, D.W.; Rhee, Y.S.; Kim, J.Y.; et al. Formulation and in vitro/in vivo evaluation of chitosan-based film forming gel containing ketoprofen. Drug Deliv. 2017, 24, 1056–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, R.B.; Smith, E.R. The role percutan penetration enhancers. Adv. Drug Deliv. Rev. 1996, 18, 295–301. [Google Scholar] [CrossRef]
- Mosallam, S.; Ragaie, M.H.; Moftah, N.H.; Elshafeey, A.H.; Abdelbary, A.A. Use of novasomes as a vesicular carrier for improving the topical delivery of terconazole: In vitro characterization, in vivo assessment and exploratory clinical experimentation. Int. J. Nanomed. 2021, 16, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Vučinić-Milanković, N.; Savić, S.; Vuleta, G.; Vučinić, S. Natural surfactant-based emulsion vehicles: A correlation between colloidal structure and in vitro release of diclofenac diethylamine. J. Disp. Sci. Technol. 2010, 31, 1077–1084. [Google Scholar] [CrossRef]
- Talele, P.; Sahu, S.; Mishra, A.K. Physicochemical characterization of solid lipid nanoparticles comprised of glycerol monostearate and bile salts. Colloids Surf. B Biointerfaces 2018, 172, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.C.; Marangoni, A.G. Internal and external factors affecting the stability of glycerol monostearate structured emulsions. RSC Adv. 2015, 5, 93108–93116. [Google Scholar] [CrossRef]
- Wang, F.C.; Peyronel, F.; Marangoni, A.G. Phase diagram of glycerol monostearate and sodium stearoyl lactylate. Cryst. Growth Des. 2016, 16, 297–306. [Google Scholar] [CrossRef]
- Sone, T.; Hanamizu, T.; Ichioka, M.; Yokokura, T.; Yoshikawa, S.; Kondo-Yanai, N.; Hiraki, Y.; Esumi, K. Moisturizing effect of vesicles formed from monoglycerides on human skin. Int. J. Cosmet. Sci. 1999, 21, 23–31. [Google Scholar] [CrossRef]
- Wang, F.C.; Marangoni, A.G. Advances in the application of food emulsifier α-gel phases: Saturated monoglycerides, polyglycerol fatty acid esters, and their derivatives. J. Colloid Interface Sci. 2016, 483, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Hadgraft, J. Modulation of the barrier function of the skin. Ski. Pharmacol. Physiol. 2001, 14, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Dąbrowska, A.K.; Spano, F.; Derler, S.; Adlhart, C.; Spencer, N.D.; Rossi, R.M. The relationship between skin function, barrier properties, and body-dependent factors. Ski. Res. Technol. 2018, 24, 165–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Z.; Liu, C.; Wan, X.; Fang, L. Development of aw/o emulsion using ionic liquid strategy for transdermal delivery of anti-aging component α–lipoic acid: Mechanism of different ionic liquids on skin retention and efficacy evaluation. Eur. J. Pharm. Sci. 2020, 141, 105042. [Google Scholar] [CrossRef]
- Singh, B.; Beg, S.; Khurana, R.K.; Sandhu, P.S.; Kaur, R.; Katare, O.P. Recent advances in self-emulsifying drug delivery systems (SEDDS). Crit. Rev. Ther. Drug Carrier Syst. 2014, 31, 121–185. [Google Scholar] [CrossRef] [PubMed]
- Ponto, T.; Latter, G.; Luna, G.; Leite-Silva, V.R.; Wright, A.; Benson, H.A.E. Novel self-nano-emulsifying drug delivery systems containing astaxanthin for topical skin delivery. Pharmaceutics 2021, 13, 649. [Google Scholar] [CrossRef]
- Van Staden, D.; Du Plessis, J.; Viljoen, J.J.P. Development of a self-emulsifying drug delivery system for optimized topical delivery of clofazimine. Pharmaceutics 2020, 12, 523. [Google Scholar] [CrossRef]
- Badran, M.M.; Taha, E.I.; Tayel, M.M.; Al-Suwayeh, S.A. Ultra-fine self nanoemulsifying drug delivery system for transdermal delivery of meloxicam: Dependency on the type of surfactants. J. Mol. Liq. 2014, 190, 16–22. [Google Scholar] [CrossRef]
- El Maghraby, G.M. Self-microemulsifying and microemulsion systems for transdermal delivery of indomethacin: Effect of phase transition. Colloids Surf. B Biointerfaces 2010, 75, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Alonso, C.; Larburu, I.; Bon, E.; González, M.M.; Iglesias, M.T.; Urreta, I.; Emparanza, J.I. Efficacy of petrolatum jelly for the prevention of diaper rash: A randomized clinical trial. J. Spec. Pediatr. Nurs. 2013, 18, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Fujii, M.; Nakamura, T.; Fukuno, S.; Mizutani, N.; Nabe, T.; Kohno, S. Ethanol aggravates itch-related scratching in hairless mice developing atopic dermatitis. Eur. J. Pharmacol. 2009, 611, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Al-Ghabeish, M.; Krishnaiah, Y.S.; Rahman, Z.; Khan, M.A. Kinetics of drug release from ointments: Role of transient-boundary layer. Int. J. Pharm. 2015, 494, 31–39. [Google Scholar] [CrossRef]
- Whitworth, C.W.; Asker, A.F. Effect of small-scale preparation techniques on diffusion of salicylic acid from various ointment bases. J. Pharm. Sci. 1974, 63, 1618–1620. [Google Scholar] [CrossRef]
- Bhagurkar, A.M.; Angamuthu, M.; Patil, H.; Tiwari, R.V.; Maurya, A.; Hashemnejad, S.M.; Kundu, S.; Murthy, S.N.; Repka, M.A. Development of an ointment formulation using hot-melt extrusion technology. AAPS Pharm. Sci. Tech. 2016, 17, 158–166. [Google Scholar] [CrossRef]
- Omar, M.M.; Hasan, O.A.; El Sisi, A.M. Preparation and optimization of lidocaine transferosomal gel containing permeation enhancers: A promising approach for enhancement of skin permeation. Int. J. Nanomed. 2019, 14, 1551. [Google Scholar] [CrossRef] [Green Version]
- López-Iglesias, C.; Quílez, C.; Barros, J.; Velasco, D.; Alvarez-Lorenzo, C.; Jorcano, J.L.; Moteiro, F.; Garcia-González, C. Lidocaine-loaded solid lipid microparticles (slmps) produced from gas-saturated solutions for wound applications. Pharmaceutics 2020, 12, 870. [Google Scholar] [CrossRef]
- Lee, H.J.; Kwon, Y.B.; Kang, J.H.; Oh, D.W.; Park, E.S.; Rhee, Y.S.; Kim, J.Y.; Shin, D.H.; Kim, D.W.; Park, C.W. Inhaled bosentan microparticles for the treatment of monocrotaline-induced pulmonary arterial hypertension in rats. J. Control Release 2021, 329, 468–481. [Google Scholar] [CrossRef] [PubMed]
- Bakonyi, M.; Gácsi, A.; Kovács, A.; Szűcs, M.B.; Berkó, S.; Csányi, E. Following-up skin penetration of lidocaine from different vehicles by Raman spectroscopic mapping. J. Pharm. Biomed. 2018, 154, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Muniz, B.V.; Baratelli, D.; Di Carla, S.; Serpe, L.; da Silva, C.B.; Guilherme, V.A.; Ribeiro, L.N.M.; Cereda, C.M.S.; Paula, E.; Volpato, M.C.; et al. Hybrid hydrogel composed of polymeric nanocapsules co-loading lidocaine and prilocaine for topical intraoral anesthesia. Sci. Rep. 2018, 8, 17972. [Google Scholar] [CrossRef] [PubMed]
- Wijaya, W.; Zheng, H.; Zheng, T.; Su, S.; Patel, A.R.; Van der Meeren, P.; Huang, Q. Improved bioaccessibility of polymethoxyflavones loaded into high internal phase emulsions stabilized by biopolymeric complexes: A dynamic digestion study via TNO’s gastrointestinal model. Curr. Res. Nutr. Food Sci. 2020, 2, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Sweed, N.M.; Fayez, A.M.; El-Emam, S.Z.; Dawoud, M.H. Response surface optimization of self nano-emulsifying drug delivery system of rosuvastatin calcium for hepatocellular carcinoma. Int. J. Pharm. Investig. 2021, 51, 85–101. [Google Scholar] [CrossRef]
- Tran, P.; Park, J.S. Recent trends of self-emulsifying drug delivery system for enhancing the oral bioavailability of poorly water-soluble drugs. Int. J. Pharm. Investig. 2021, 1–25. [Google Scholar]
- Lee, H.J.; Kang, J.H.; Lee, H.G.; Kim, D.W.; Rhee, Y.S.; Kim, J.Y.; Park, E.S.; Park, C.W. Preparation and physicochemical characterization of spray-dried and jet-milled microparticles containing bosentan hydrate for dry powder inhalation aerosols. Drug Des. Dev. Ther. 2016, 10, 4017–4030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, C.W.; Lee, H.J.; Oh, D.W.; Kang, J.H.; Han, C.S.; Kim, D.W. Preparation and in vitro/in vivo evaluation of PLGA microspheres containing norquetiapine for long-acting injection. Drug Des. Dev. Ther. 2018, 12, 711–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, N.A.; Oh, H.K.; Lee, J.C.; Choi, Y.H.; Jeong, S.H. Comparison of solubility enhancement by solid dispersion and micronized butein and its correlation with in vivo study. Int. J. Pharm. Investig. 2021, 51, 53–60. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Excipient | L1 | L2 | L3 | L4 | L5 | L6 |
|---|---|---|---|---|---|---|
| Petrolatum | 95.00 | 91.00 | 86.00 | 91.95 | 86.45 | 81.45 |
| MCT oil | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Glycerol monostearate | - | 5.00 | 10.00 | - | 5.00 | 10.00 |
| Vitamin E-acetate | - | - | - | 3.00 | 3.00 | 3.00 |
| Lidocaine base | 3.00 | 3.00 | 3.00 | 3.00 | 3.00 | 3.00 |
| Allantoin | - | - | - | 1.00 | 1.00 | 1.00 |
| Prednisolone acetate | - | - | - | 0.05 | 0.05 | 0.05 |
| dl-Methylephedrine HCl | - | - | - | - | 0.5 | 0.5 |
| pH | 8.4 | 8.4 | 8.5 | 8.5 | 8.5 | 8.5 |
| Viscosity (×103 cP) | - | - | - | 23.5 ± 0.5 | 41.9 ± 0.8 | 95.2 ± 0.9 |
| Minimum extrusion force (N) | - | - | - | 19.5 ± 0.2 | 25.2 ± 0.8 | 54.9 ± 0.9 |
| Ointment | Droplet Size (nm) | PDI |
|---|---|---|
| L1 | 1132.0 ± 118.8 | 0.22 ± 0.11 |
| L2 | 117.0 ± 0.3 | 0.28 ± 0.01 |
| L3 | 108.0 ± 1.4 | 0.30 ± 0.02 |
| Normal Saline | Ref. A | L4 | L5 | L6 | |
|---|---|---|---|---|---|
| AUC (sec × min) | 439.8 ± 32.6 | 512.3 ± 7.2 * | 583.0 ± 14.3 **, # | 706.1 ± 24.9 **, ##, §§ | 778.9 ± 26.3 **, ##, §§, † |
| Effect fold compared to Normal saline | 1.00 | 1.16 | 1.33 | 1.61 | 1.77 |
| Effect fold compared to Ref. A | 0.86 | 1.00 | 1.14 | 1.38 | 1.52 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, J.-H.; Yoo, K.-H.; Park, H.-Y.; Hyun, S.-M.; Han, S.-D.; Kim, D.-W.; Park, C.-W. Preparation and In Vivo Evaluation of a Lidocaine Self-Nanoemulsifying Ointment with Glycerol Monostearate for Local Delivery. Pharmaceutics 2021, 13, 1468. https://doi.org/10.3390/pharmaceutics13091468
Kang J-H, Yoo K-H, Park H-Y, Hyun S-M, Han S-D, Kim D-W, Park C-W. Preparation and In Vivo Evaluation of a Lidocaine Self-Nanoemulsifying Ointment with Glycerol Monostearate for Local Delivery. Pharmaceutics. 2021; 13(9):1468. https://doi.org/10.3390/pharmaceutics13091468
Chicago/Turabian StyleKang, Ji-Hyun, Kwang-Hwi Yoo, Hyo-Young Park, Seung-Min Hyun, Sang-Duk Han, Dong-Wook Kim, and Chun-Woong Park. 2021. "Preparation and In Vivo Evaluation of a Lidocaine Self-Nanoemulsifying Ointment with Glycerol Monostearate for Local Delivery" Pharmaceutics 13, no. 9: 1468. https://doi.org/10.3390/pharmaceutics13091468