
Subscribe to RSS
DOI: 10.1055/a-1632-1777
“Novel Clinical Concepts in Thrombosis”: Integrated Care for Stroke Management—Easy as ABC

Introduction
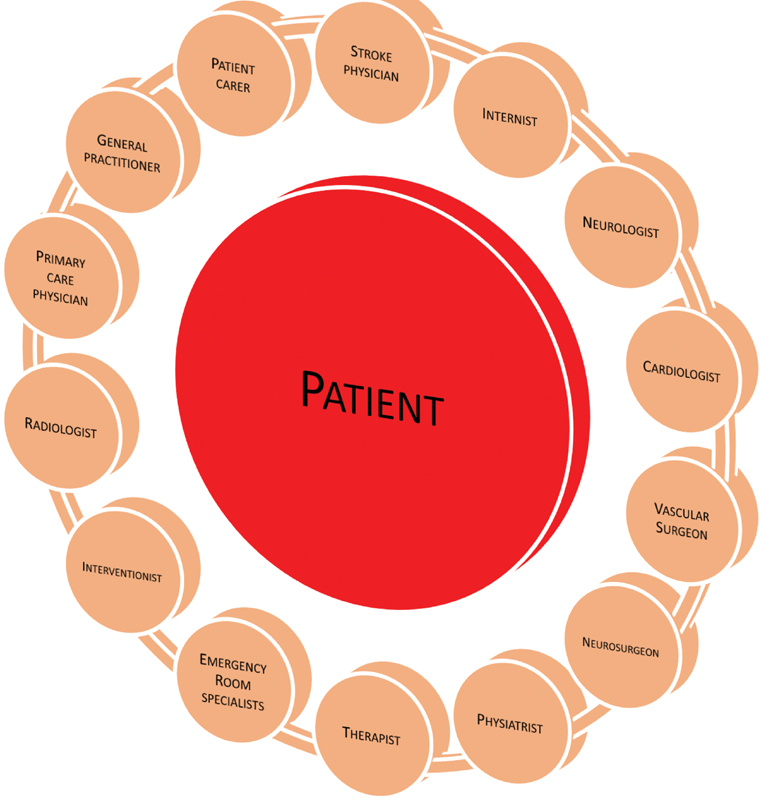
Stroke care often involves a multidisciplinary effort, including the stroke physician, internist, neurologist, interventionist, cardiologist, radiologist, vascular surgeon, neurosurgeon, emergency room physician, primary care physician, general practitioner, and rehabilitation team (including physiatrist and therapists), as well as nurses, patient carers, and next of kin ([Fig. 1]). Ultimately, the patient is central to all this, receiving information from different health care professionals. The patient “journey” requires a simple and uniform approach to the priorities of poststroke management, which can be uniformly and consistently described by different health care professionals, allowing patient (and carer) engagement and empowerment with regards to their care.
Such an “integrated care” approach has been applied in other chronic conditions. For example, the ABC (Atrial fibrillation Better Care) pathway has been proposed as an integrated approach to improve the management of patients with atrial fibrillation (AF). This has three central pillars: “A”—avoid stroke (with anticoagulants); “B”—better symptom management, with patient-centered decisions on rate or rhythm control; “C”—cardiovascular and comorbidity risk optimization.[1] This concept was first proposed to promote a streamlined approach to management that can be applicable to whether the AF patient is managed by any health care professional, the general practitioner, or the hospital-based specialist (whether cardiologist or noncardiologist).
This integrated care approach to AF management is promoted in patient pathways to improve diagnosis and management of AF patients, and would facilitate discussion and patient engagement on the principles of AF care (“easy as ABC…”) and importantly, minimizes the possibility of conflicting information from health care professionals. Such conflicting information when dealing with patients has been associated with poorer patient adherence with their management plan.[2]
The ABC pathway has been well validated in posthoc analyses of clinical trials, prospective cohort studies, and a prospective randomized trial. In a recent systematic review, AF patients treated according to the ABC pathway showed a lower risk of all-cause death (odds ratio [OR]: 0.42, 95% confidence interval [CI]: 0.31–0.56), cardiovascular death (OR: 0.37, 95% CI: 0.23–0.58), stroke (OR: 0.55, 95% CI: 0.37–0.82), and major bleeding (OR: 0.69, 95% CI: 0.51–0.94).[3] Improved clinical outcomes with ABC pathway compliance are evident, even in clinically complex patients such as those with multimorbidity, polypharmacy, and hospitalizations.[4]
The mAFA-II trial was a prospective cluster-randomized trial of patients randomized to receive usual care, or integrated care based on the ABC pathway.[5] Rates of the composite outcome of “ischemic stroke/systemic thromboembolism, death, and rehospitalization” were lower with the mAFA intervention compared with usual care (1.9 vs. 6.0%; hazard ratio [HR]: 0.39; 95% CI: 0.22–0.67; p < 0.001). Rates of rehospitalization were also lower with the mAFA intervention. In the mAFA-II trial long-term extension cohort, these beneficial effects were maintained, and there was a high adherence (>70%) and persistence (>90%) with the mAFA app-based intervention based on the ABC pathway.[6] The mAFA-II trial also reported that this holistic app-based management with dynamic risk monitoring and reassessment of the bleeding risks (using HAS-BLED score) reduced the risks of major bleeding (mAFA vs. usual care, 2.1 vs. 4.3% at 1 year) and increased total oral anticoagulation (OAC) usage from 63 to 70%.[7]
* The review process for this paper was fully handled by Christian Weber, Editor-in-Chief.
Publication History
Received: 26 August 2021
Accepted: 27 August 2021
Accepted Manuscript online:
02 September 2021
Article published online:
18 October 2021
© 2021. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Lip GYH. The ABC pathway: an integrated approach to improve AF management. Nat Rev Cardiol 2017; 14 (11) 627-628
- 2 Moudallel S, van den Bemt BJF, Zwikker H. et al. Association of conflicting information from healthcare providers and poor shared decision making with suboptimal adherence in direct oral anticoagulant treatment: a cross-sectional study in patients with atrial fibrillation. Patient Educ Couns 2021; 104 (01) 155-162
- 3 Romiti GF, Pastori D, Rivera-Caravaca JM. et al. Adherence to the ‘atrial fibrillation better care’ (abc) pathway in patients with atrial fibrillation. Thromb Haemost 2022; 122 (03) 406-414
- 4 Proietti M, Romiti GF, Olshansky B, Lane DA, Lip GYH. Comprehensive management with the abc (atrial fibrillation better care) pathway in clinically complex patients with atrial fibrillation: a post hoc ancillary analysis from the affirm trial. J Am Heart Assoc 2020; 9 (10) e014932
- 5 Guo Y, Lane DA, Wang L. et al; mAF-App II Trial Investigators. Mobile health technology to improve care for patients with atrial fibrillation. J Am Coll Cardiol 2020; 75 (13) 1523-1534
- 6 Guo Y, Guo J, Shi X. et al; mAF-App II Trial investigators. Mobile health technology-supported atrial fibrillation screening and integrated care: a report from the mAFA-II trial Long-term Extension Cohort. Eur J Intern Med 2020; 82: 105-111
- 7 Guo Y, Lane DA, Chen Y, Lip GYH. mAF-App II Trial investigators. Regular bleeding risk assessment associated with reduction in bleeding outcomes: the mafa-ii randomized trial. Am J Med 2020; 133 (10) 1195-1202
- 8 Kamel H, Okin PM, Elkind MS, Iadecola C. Atrial fibrillation and mechanisms of stroke: time for a new model. Stroke 2016; 47 (03) 895-900
- 9 Chiu CC, Lin HF, Lin CH. et al. Multidisciplinary care after acute care for stroke: a prospective comparison between a multidisciplinary post-acute care group and a standard group matched by propensity score. Int J Environ Res Public Health 2021; 18 (14) 18
- 10 Hilkens NA, Algra A, Diener HC. et al; Cerebrovascular Antiplatelet Trialists' Collaborative Group. Balancing benefits and risks of long-term antiplatelet therapy in noncardioembolic transient ischemic attack or stroke. Stroke 2021; 52 (10) 3258-3265
- 11 Ntaios G, Lip GY. Difficult situations in anticoagulation after stroke: between Scylla and Charybdis. Curr Opin Neurol 2016; 29 (01) 42-48
- 12 Gargiulo G, Goette A, Tijssen J. et al. Safety and efficacy outcomes of double vs. triple antithrombotic therapy in patients with atrial fibrillation following percutaneous coronary intervention: a systematic review and meta-analysis of non-vitamin K antagonist oral anticoagulant-based randomized clinical trials. Eur Heart J 2019; 40 (46) 3757-3767
- 13 Noubiap JJ, Agbaedeng TA, Tochie JN. et al. Meta-analysis comparing the frequency of carotid artery stenosis in patients with atrial fibrillation and vice versa. Am J Cardiol 2021; 138: 72-79
- 14 Guedeney P, Collet JP. Antithrombotic therapy in acute coronary syndromes: current evidence and ongoing issues regarding early and late management. Thromb Haemost 2021; 121 (07) 854-866
- 15 Lip GYH, Collet JP, Haude M. et al; ESC Scientific Document Group. 2018 joint European consensus document on the management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous cardiovascular interventions: a joint consensus document of the European Heart Rhythm Association (EHRA), European Society of Cardiology Working Group on Thrombosis, European Association of Percutaneous Cardiovascular Interventions (EAPCI), and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS), Latin America Heart Rhythm Society (LAHRS), and Cardiac Arrhythmia Society of Southern Africa (CASSA). Europace 2019; 21 (02) 192-193
- 16 Lee SR, Rhee TM, Kang DY, Choi EK, Oh S, Lip GYH. Meta-analysis of oral anticoagulant monotherapy as an antithrombotic strategy in patients with stable coronary artery disease and nonvalvular atrial fibrillation. Am J Cardiol 2019; 124 (06) 879-885
- 17 Yasuda S, Kaikita K, Akao M. et al; AFIRE Investigators. Antithrombotic therapy for atrial fibrillation with stable coronary disease. N Engl J Med 2019; 381 (12) 1103-1113
- 18 Eikelboom JW, Connolly SJ, Bosch J. et al; COMPASS Investigators. Rivaroxaban with or without aspirin in stable cardiovascular disease. N Engl J Med 2017; 377 (14) 1319-1330
- 19 Ntaios G, Gioulekas F, Papavasileiou V, Strbian D, Michel P. ASTRAL, DRAGON and SEDAN scores predict stroke outcome more accurately than physicians. Eur J Neurol 2016; 23 (11) 1651-1657
- 20 Ntaios G, Faouzi M, Ferrari J, Lang W, Vemmos K, Michel P. An integer-based score to predict functional outcome in acute ischemic stroke: the ASTRAL score. Neurology 2012; 78 (24) 1916-1922
- 21 Papavasileiou V, Milionis H, Michel P. et al. ASTRAL score predicts 5-year dependence and mortality in acute ischemic stroke. Stroke 2013; 44 (06) 1616-1620
- 22 Liu G, Ntaios G, Zheng H. et al. External validation of the ASTRAL score to predict 3- and 12-month functional outcome in the China National Stroke Registry. Stroke 2013; 44 (05) 1443-1445
- 23 Saver JL, Chaisinanunkul N, Campbell BCV. et al; XIth Stroke Treatment Academic Industry Roundtable. Standardized nomenclature for modified Rankin scale global disability outcomes: consensus recommendations from stroke therapy academic industry roundtable XI. Stroke 2021; 52 (09) 3054-3062
- 24 Mosalski S, Shiner CT, Lannin NA. et al. Increased relative functional gain and improved stroke outcomes: a linked registry study of the impact of rehabilitation. J Stroke Cerebrovasc Dis 2021; 30 (10) 106015
- 25 Zeng YY, Wu MX, Geng DD. et al. Early-onset depression in stroke patients: effects on unfavorable outcome 5 years post-stroke. Front Psychiatry 2021; 12: 556981
- 26 Towfighi A, Ovbiagele B, El Husseini N. et al; American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; and Council on Quality of Care and Outcomes Research. Poststroke depression: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2017; 48 (02) e30-e43
- 27 Verdelho A, Wardlaw J, Pavlovic A. et al. Cognitive impairment in patients with cerebrovascular disease: a white paper from the links between stroke ESO Dementia Committee. Eur Stroke J 2021; 6 (01) 5-17
- 28 Leys D, Hénon H, Mackowiak-Cordoliani M-A, Pasquier F. Poststroke dementia. Lancet Neurol 2005; 4 (11) 752-759
- 29 Blood Pressure Lowering Treatment Trialists' Collaboration. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: an individual participant-level data meta-analysis. Lancet 2021; 397 (10285): 1625-1636
- 30 Sanders CB, Knisely K, Edrissi C. et al. Obstructive sleep apnea and stroke severity: impact of clinical risk factors. Brain Circ 2021; 7 (02) 92-103
- 31 Gill JS, Shipley MJ, Tsementzis SA. et al. Alcohol consumption–a risk factor for hemorrhagic and non-hemorrhagic stroke. Am J Med 1991; 90 (04) 489-497
- 32 Pan B, Jin X, Jun L, Qiu S, Zheng Q, Pan M. The relationship between smoking and stroke: a meta-analysis. Medicine (Baltimore) 2019; 98 (12) e14872
- 33 Lazar RM, Howard VJ, Kernan WN. et al; American Heart Association Stroke Council. A primary care agenda for brain health: a scientific statement from the American Heart Association. Stroke 2021; 52 (06) e295-e308