Article Text

Abstract
Background Early access to diagnosis is crucial for effective management of any disease including tuberculosis (TB). We investigated the barriers and opportunities to maximise uptake and utilisation of molecular diagnostics in routine healthcare settings.
Methods Using the implementation of WHO approved TB diagnostics, Xpert Mycobacterium tuberculosis/rifampicin (MTB/RIF) and Line Probe Assay (LPA) as a benchmark, we evaluated the barriers and how they could be unlocked to maximise uptake and utilisation of molecular diagnostics.
Results Health officers representing 190 districts/counties participated in the survey across Kenya, Tanzania and Uganda. The survey findings were corroborated by 145 healthcare facility (HCF) audits and 11 policy-maker engagement workshops. Xpert MTB/RIF coverage was 66%, falling behind microscopy and clinical diagnosis by 33% and 1%, respectively. Stratified by HCF type, Xpert MTB/RIF implementation was 56%, 96% and 95% at district, regional and national referral hospital levels. LPA coverage was 4%, 3% below culture across the three countries. Out of 111 HCFs with Xpert MTB/RIF, 37 (33%) used it to full capacity, performing ≥8 tests per day of which 51% of these were level five (zonal consultant and national referral) HCFs. Likewise, 75% of LPA was available at level five HCFs. Underutilisation of Xpert MTB/RIF and LPA was mainly attributed to inadequate—utilities, 26% and human resource, 22%. Underfinancing was the main reason underlying failure to acquire molecular diagnostics. Second to underfinancing was lack of awareness with 33% healthcare administrators and 49% practitioners were unaware of LPA as TB diagnostic. Creation of a national health tax and decentralising its management was proposed by policy-makers as a booster of domestic financing needed to increase access to diagnostics.
Conclusion Our findings suggest higher uptake and utilisation of molecular diagnostics at tertiary level HCFs contrary to the WHO recommendation. Country-led solutions are crucial for unlocking barriers to increase access to diagnostics.
- diagnostics and tools
- health systems evaluation
- tuberculosis
Data availability statement
Data are available on reasonable request. Data available at School of Medicine Division of Infection and Global Health, WS, ws31@st-andrews.ac.uk. Requests will be reviewed by the ethics Committee to assess their compliance to confidentiality and limits of consent given by study participants.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Diagnostics are critical for effective management of disease. This is more so for tuberculosis (TB), a treatable disease but millions go undetected and untreated every year.
What are the new findings?
Contrary to WHO recommendation, implementation of Xpert MTB/RIF and Line Probe Assay is higher at tertiary, that is, regional and national healthcare levels, respectively. Despite the usual culprit (underfinancing), our study reveals that unawareness by healthcare administrators, practitioners and service users is a strong limiting factor to uptake and utilisation of diagnostics.
What do the new findings imply?
Low access to diagnosis by people living in areas served by primary healthcare facilities, which perhaps explain the 3 million TB cases that go undetected every year. Bottom-up country-led solutions are critical for increasing access to diagnostics.
Recommended solutions
Improving human resource capacity and efficiency: Considering the paucity of finances to hire and retain skilled workforce in resource limited settings, efficiency in provision of molecular diagnostic services could be improved by operating a hub system. This allows consolidation of skilled human resources at specific HCFs across the country. Secondly, providing flexible working conditions will enable staff attend training to upgrade their skills as well as attracting skilled part-time workers.
Increasing uptake of molecular diagnostics at HCF levels 1, 2, 3 and 4: some level 3 and 4 HCF can be converted into molecular diagnostics hubs serving a network of levels 1 and 2 HCFs. Each district (for Uganda and Tanzania) or subcounty (for Kenya) could have one hub receiving and processing specimens from HCFs in the area. Investing in laboratory information systems and electronic health records would ensure results feedback to respective clinics as soon as sample processing is finished.
Stability of utilities: Water and electricity are crucial for running both clinical and laboratory procedures. Investing in extension of piped water to HCFs and solar power will go a long way in ensuring consistent health service delivery.
Streamlining procurement services: Consultative approach between national-local healthcare administrators, service users and private sector will help identify efficient ways to procure supplies and ensure timely healthcare service delivery.
Increasing domestic financing of healthcare services: Based on 5-year WHO reporting prior to the study, over 50% of funding for TB services came from donor funds. Policy-makers’ suggestion of creating a health fund supported by local tax revenues is practical and will go a long way in boosting domestic funding of healthcare services.
Introduction
The COVID-19 pandemic led to worldwide shutdown and saw unprecedented uptake and utilisation of molecular diagnostics with over 500 million tests conducted in a period of 9 months (statista.com, 9 October 2020). The rapidly evolving COVID-19 is responsible 36.99 million cases and 1.1 million deaths (WHO COVID-19 Dashboard, 11 October 2020).1 The health systems have been shaken but most importantly the pandemic has raised public consciousness of the value of diagnostics and interdisciplinary approaches in the control of diseases. In contrast, tuberculosis (TB) has been a pandemic for time immemorial and a global public health emergency for over 20 years.2 3 A quarter (1.7 billion) of the world population have TB infection and in 2018, 10 million developed active disease resulting in 1.5 million deaths.4–6 Of the 10 million notified cases, 55% were bacteriologically confirmed and a small proportion of these were tested using rapid molecular tests.5 The rate of TB testing does not match incidence of TB disease and, consequently, an estimated 3 million cases go undetected every year.7
WHO approved routine use of TB molecular tests more than 10 years ago, starting with the Line Probe Assay (LPA) in 2008 and Xpert Mycobacterium tuberculosis/rifampicin (MTB/RIF) in 2010.8 9 The latter detects both TB and resistance to rifampicin in 2 hours and is the widely used molecular test for TB. By 2016, only 16 million Xpert MTB/RIF tests had been performed, translating into 3.2 million tests per year.10 While there is been steady progress in the uptake and use of Xpert MTB/RIF, the impact of using the same GeneXpert platform for testing HIV viral load and more recently COVID-19 on TB diagnosis is yet to be unravelled.11 12 There is sharp contrast in the rate of uptake of COVID-19 molecular tests compared with TB and could a leaf be borrowed from either disease on how to accelerate and maximise translation of health research innovations into policy and practice?
The impact of effective diagnostic testing is not only the ability to detect disease but also contribution to favourable clinical outcomes for patients. This is more likely to be achieved in a health system landscape that employs holistic approach to patient care as enshrined in the ‘WHO End TB strategy’: integrated patient-centred care and prevention to foster early diagnosis, universal drug-susceptibility testing, systematic screening of contacts and high-risk group, treatment of all people. Good governance and leadership to ensure equal access to healthcare, safe medicines and social protection to minimise impact of economic status on quality of care received. Last but not least, intensifying research and innovation to ensure discovery, development, optimisation and rapid uptake of new tools, interventions and strategies coupled with monitoring and evaluation to ascertain impact.13–15
Low-income and middle-income countries (LMICs) account for over 50% of the global TB burden.5 The scarcity of resources complicates the development of strong health systems and more so when the COVID-19 effect which is estimated to have reduced TB care delivery by 20% is taken into account.12 Models to ensure access of service by those that need them the most have been developed.16–18 For instance, Kenya used patient pathway analysis (PPA) model to assess the delivery of TB diagnostic and treatment and found more than 50% of the low-level healthcare facilities (HCFs) where majority people seek care did not have diagnostic services.19 Confronted by this finding, Kenya committed to redesigning the provision of TB services to ensure they are in places where they are most needed rather than where it is operationally convenient, such as tertiary level HCFs in urban settings. Kenya adopted this approach around the same time as our study, it will be interesting to assess the impact made on uptake and utilisation of molecular diagnostics for TB in the country.
Using the implementation of TB diagnostics as a model, we sought to understand the ways to maximise uptake and utilisation of diagnostic technologies that have regulatory approval and are supported by WHO and other expert opinion within the health systems. Our findings show higher rate of uptake and utilisation of TB diagnostics at tertiary level HCFs. In contrast to the WHO endorsement, LPA is mainly implemented at zonal—national level instead of regional HCF while Xpert MTB/RIF was more utilised at regional, zonal—national level HCFs instead of the recommended district level hospitals. These data point to hub-centralised model of implementation in order to maximise both uptake and utilisation of the diagnostics platforms. Resolving the health system, socioeconomic and cultural bottlenecks is pivotal for the effective implementation of either the PPA or centralised model of diagnostic services.
Methods
This was a mixed-methods study employing both quantitative and qualitative approaches including surveys of district/county health officers, HCF audits, in-depth one-on-one interviews, focus group discussions (FGDs) and dialogues with policy-makers. The study was conducted between September 2016 to December 2017 in Uganda, Kenya and Tanzania. At the time of the study, only Kenya was defined as a middle income country, and it has now been joined by Tanzania in this classification.20
Consortium
The study was conducted under the TWENDE consortium and comprised seven institutions: Makerere University and CPAR Uganda Ltd Uganda, Kenya Medical Research Institute (KEMRI) Kenya, Kilimanjaro Clinical Research Institute (KCRI) and National Institute for Medical Research (NIMR)—Mbeya Medical Research Centre Tanzania while the East African Community was represented by the East African Health Research Commission, and University of St Andrews, UK. TWENDE, which is Swahili word means ‘let’s go!’ is abbreviated from Tuberculosis: Working to Empower the Nations’ Diagnostic Effort.
Geography and participants
Areas of coverage were selected based on the TB diagnostics, LPA and Xpert MTB/RIF (GeneXpert) approved areas of implementation. According to the WHO, LPA and Xpert MTB/RIF are recommended for implementation at regional and district level hospitals respectively. In Uganda, regions were based on areas represented by a regional hospital while districts were taken as they are currently structured as administration units. In Tanzania, regions and districts are clearly demarcated administrative units and so were covered as such. For Kenya, regional units were counties while the subcounties were equivalent to districts in Uganda and Tanzania. Study districts, regions or counties were purposively selected to be representative of all geographical regions of the country.
Participants were healthcare administrators such as regional/county and district health (medical) officers, HCF managers and healthcare professionals of participating HCFs. Apart from managers and practitioners, patients, TB survivors, community health volunteers, opinions leaders among the HCF users, local council leaders and national policy-makers in ministry of Health and parliament were engaged. Participants were selected based on their role either as healthcare leader/manager or practitioner and/or by their status as patients with TB, caregivers or survivors. The managers and practitioners represented opinion from health system service delivery perspective while the patients, caregivers and survivors shared their lived experiences in accessing diagnosis and treatment as well as living with TB in a community.
Survey
An online survey was constructed using the University of St Andrews licensed Qualtrics survey tool (https://standrews.eu.qualtrics.com). The tool was commissioned by the University of St Andrews teaching and research ethics and complies with the European Union General Data Protection regulation EU2016/679 and the local country Ethics committees. The purpose of the survey was to obtain an overview of the challenges and opportunities confronting TB diagnostics and treatment services from the perspective of regional/county and district/sub-county health or medical officers (see online supplemental file 1). It sought to know what facility and/or service is available and if not available, what could be the underlying reasons. The survey was made compatible with all computer systems, Windows and macOS, and both Android and Apple smart phones. The opening page of the questionnaire had participant information and solicitation for consent to participate in the study.
Supplemental material
HCF audits
The rationale of the audit was to verify the responses given by survey participants and gain more insight into the implementation of TB diagnostics on ground. The audit tool was developed and teams of researchers in each country were trained to administer the tool at selected HCFs. The respondents at the HCFs were the healthcare and laboratory managers at regional/county and district/subcounty hospitals. The audit ascertained whether the facilities and services reported by the survey participants were indeed available and being used. In addition to interviews with healthcare practitioners, the auditors inspected the facilities to verify answers given. See online supplemental file 2.
Supplemental material
Policy dialogues
Workshops were organised targeting policy-makers and implementers to discuss views from the general community and construct actionable policy briefs for the national policies to implement. Participants in these were workshops were parliamentarians, technocrats from Ministries of Health, leaders from regional/county administrative units, and representatives of other disease control agencies.
‘Chatham House Rules’ were used during the FGDs and policy dialogues to promote open expression of views and opinions without fear of being vilified. The Chatham House rule states: ‘When a meeting, or part thereof, is held under the Chatham House Rule, participants are free to use the information received, but neither the identity nor the affiliation of the speaker(s), nor that of any other participant, may be revealed’. Coverage was defined as presence or absence of the diagnostic platform at HCFs as per the WHO recommendation. Utilisation was defined as the frequency of using a particular diagnostic platform as per the WHO recommendation. Presence or absence of referral network was acknowledged as an enabler but not basis of the definition.
Data analysis
Quantitative data were analysed using Microsoft Excel 2016 and GraphPad Prism V.6. Percentage diagnostic coverage and utilisation was calculated per type of HCF and all HCFs combined. Analysis of variance (ANOVA) multiple comparisons test was used to assess the performance difference between HCFs. Significance was considered at p<0.05% and 95% CI.
Patient and public involvement statement
This study emerged as result of the challenges that had been experienced during implementation evaluation of new molecular diagnostic for TB in Malawi, Mozambique and Tanzania. Utilities like electricity and water were unstable and complex procurement landscape resulting in lost laboratory experiments and laboratory supplies at customs respectively. In response the researchers engaged all stakeholders to gain holistic understanding of the barriers and how they can be overcome. Participants who contributed to the discussion were Survivors of TB, carers, community opinion leaders, practitioners and policy-makers. Open FGDs were held in each region and/or county for Uganda, Tanzania and Kenya. Regional and national dialogues with policy-makers were held in each country and policy brief submitted to respective ministries of health and parliaments. Once published, the paper will be translated into lay English and local languages and publish in newspapers for access to the general public in the study countries.
Results
Participants and study area
A total of 217 survey responses received from district or county healthcare officers across the three countries. After removal of duplicate/multiple responses per district or county, 190 entries representing 27 (14%), 66 (35%) and 97 (51%) from Kenyan counties, Tanzanian and Ugandan districts, respectively, were considered for analysis. The Kenyan county was considered equivalent of Ugandan or Tanzanian region. The 27 Kenyan counties varied in size, median (range) 5 (2–17) subcounties (districts), together constituting an area of 159 subcounties and 57% of Kenyan counties. All the 14 Ugandan and 26 Tanzania mainland regions were represented in the survey. Time spent in the post by respondents ranged from less than 1 year to 16 years: 14 (7%) less than 1 year, 35 (16%) 1–2 years, 53 (24%) 3–4 years, 41 (19%) 5–6 years, 29 (13%) 7–8 years, 16 (7%) 9–10 years and 29 (13%) over 10 years. Most health officers performed a combination of more than three roles. The most and least frequently played roles were supervision of healthcare provision (97%) and paying healthcare workers’ salaries (9%). There was no unique association between particular roles and degree of implementation of diagnostic tools (table 1).
Roles performed by district and/or county health officers who participated in the survey
The on-site audits HCFs recapitulated the survey results. A total of 145 HCFs were audited, 48 (33%) each for Kenya and Uganda and 49 (34%) Tanzania. This represents 42% (112), 29% (169) and 44% (47) of the districts and counties in Uganda, Tanzania and Kenya, respectively, at the time of audit. In all the countries, government was the main TB clinical service provider, owning over 80% of the HCFs. Level 5 hospitals (national, consultant level, regional referral) were 42, level 4 (regional hospitals) 34, level 3 (district hospitals) 57, level 2 (health centre IV) 6 and level 1 (dispensary, health centre 1–3) 6. The majority, 86 of the TB laboratories were able to deliver biosafety level II (BSL II) followed by BSL I, 23 and BSL III, 6 and 4 general laboratories.
Coverage of diagnostics
At the time of the survey, smear microscopy was the most available diagnostic tool, 97% (185/190) followed by clinical diagnosis, 67% (128/190) and Xpert MTB RIF, 66% (125/190) of the districts/counties surveyed. TB culture and LPA were the least available, 7% (13/190) and 4% (8/190). Most of the districts, 89% (169) reported microscopy in combination with other diagnostics leaving only 11% (21) which had only microscopy for diagnosis. At country level, Xpert MTB/RIF test coverage was 74% (72/97) and 39% (26/66) districts in Uganda and Tanzania respectively and 42% (67/159) subcounties in Kenya (figure 1).
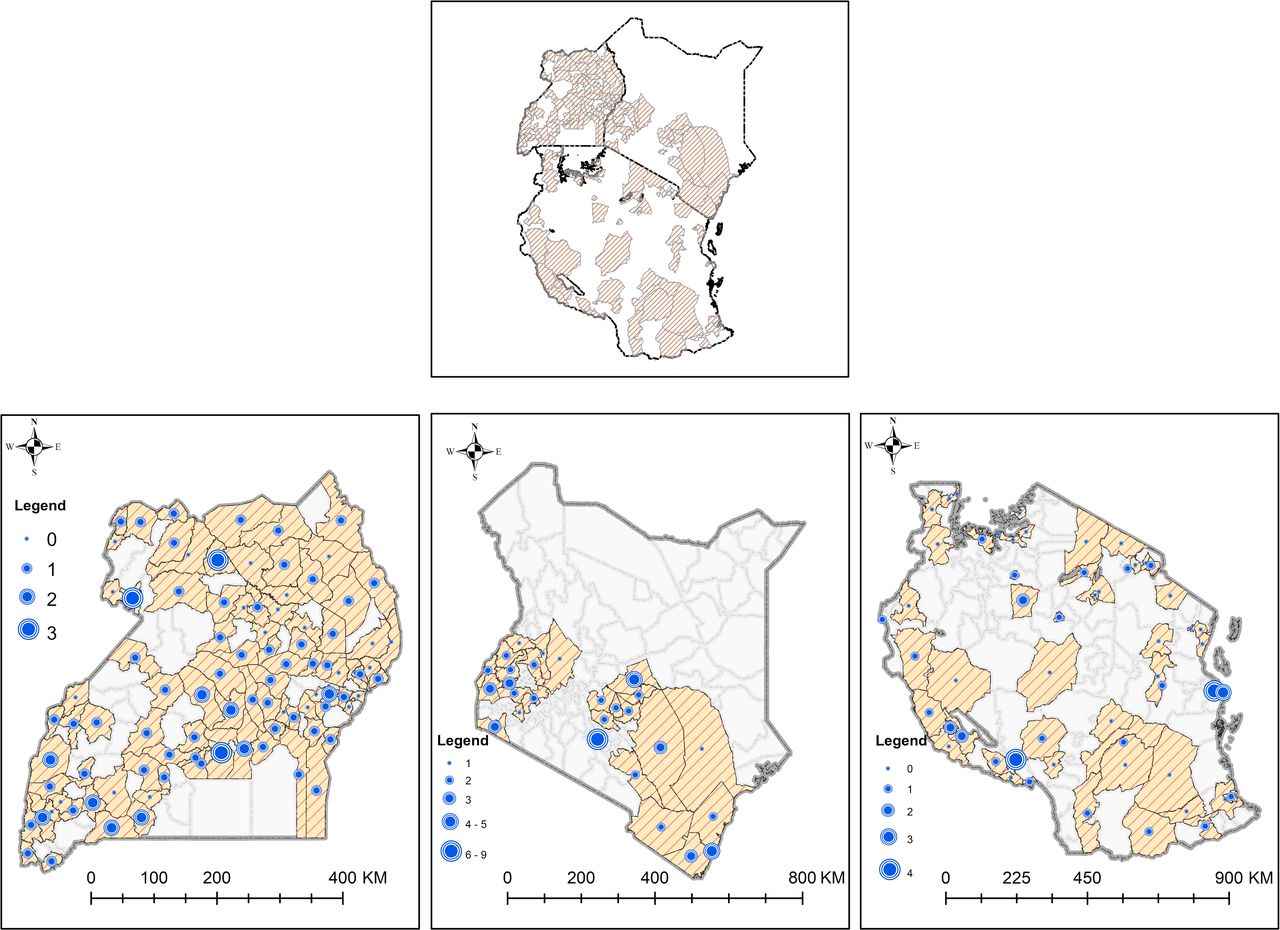
The Xpert MTB/RIF coverage in the surveyed districts and counties in Uganda, Kenya and Tanzania. The highest coverage was 3, 4 and 9 per district or county in Uganda, Tanzania and Kenya, respectively. Orange strip shading denotes districts or counties surveyed. The size of the blue circles denotes the number of the Xpert MTB/RIF machines starting from zero or no Xpert MTB/RIF machine (smallest blue circle).
The number of Xpert MTB/RIF test machines (GeneXpert) was not consistent with the number of subcounties (districts) per county in Kenya. Some counties had less than the number of the subcounties and vice versa (online supplemental figure 1).
Supplemental material
Supplemental material
The coverage results were replicated in the on-site audit of 145 HCFs: smear microscopy availability 142 (98%), Xpert MTB/RIF 111 (76%), Culture 5 (4%) and LPA 4 (3%). Number of available of Xpert MTB/RIF instruments increased with increasing level of HCF. Out of the 111 HCFs possessing Xpert MTB/RIF, 1 (0.9%), 5 (5%), 32 (29%), 33 (30%) and 40 (36%) were level 1, 2, 3, 4 and 5 HCFs, respectively. Availability within the HCF type, level 4 and 5 had the highest, 97% and 95% coverage of Xpert MTB/RIF instruments followed by level 2, 83%, level 3 (56%) and level 1, 17% (figure 2).

Xpert MTB/RIF coverage. (A) Percentage HCFs with Xpert MTB/RIF proportional to the total number of HCFs in possession of Xpert MTB/RIF (n=111). (B) Xpert MTB/RIF coverage in proportion to the HCF type. HCFs, healthcare facilities.
Out the four HCFs in possession of LPA, three were L5 (one national, one zonal referral and one consultant hospital) and only one was L4 (regional). This implies out of 34 audited regional hospitals, only one had LPA service as per WHO recommendation. All the five HCFs with culture were L5 (two national referral, two consultant and one zonal referral hospitals).
Utilisation of diagnostics
Smear microscopy
Taken together, number of smears performed per month by HCFs with microscopy services (142) were median (range) 56 (0.8–460). The number of smears performed increased with the HCF level, 26 (17–75), 18 (1.3–60), 46 (0.8–460), 48 (1.3–400) and 89 (5–311) at HCF level 1, 2, 3, 4 and 5, respectively. Only HCF level 5 performed above median number of smears per month. Of the 142 HCFs that performed microscopy, 96% (137) used it for diagnosis and treatment follow-up. The most frequent use of smear microscopy was treatment follow-up, 50% (68) followed by combination of primary diagnosis and treatment follow-up, 40% (55). The proportion of using microscopy as a primary diagnostic tool was high, 33% in level one (L1) HCFs vs 10% in L5 HCFs, and 67% vs 26% for using microscopy for both primary diagnosis and treatment follow-up (table 2).
Utilisation of smear microscopy in audited HCFs
Xpert MTB/RIF
Like coverage, utilisation of Xpert MTB/RIF increased with level of HCF, median (IQR) 0 (0–4), 90 (33–390), 120 (55–170), 200 (110–240), 228 (110–320) tests per month at level 1, 2, 3, 4 and 5 HCF, respectively, linear regression p=0.002. The ordinary one-way ANOVA multiple comparisons test showed significant difference of tests performed at different HCFs, F=5.4, p=0.0005. However, the difference was driven by tests at level 4 and 5 which were significantly higher than level 1 and both level 1 and 3 HCFs, respectively. Out of the 111 sites with Xpert MTB/RIF test instruments, only 37 (33%) used the instruments to full capacity, performing at least 8 tests per day or 240 tests per month. Of the HCFs using Xpert MTB/RIF to full capacity, 8% (3), 14% (5), 27% (10) and 51% (19) of these HCFs were level 2, 3, 4 and 5 respectively. None of the level 1 HCFs performed Xpert MTB/RIF to capacity (figure 3A,B).

Utilisation of Xpert MTB/RIF at different HCF level. (A) The number of Xpert MTB/RIF tests conducted per HCF. (B) The number of HCFs that performed 240 and above tests per month or eight tests per day recommended by WHO for full capacity use of Xpert MTB/RIF. In both level, five hospitals performed more tests than lower level HCFs. HCFs, healthcare facilities.
All Xpert MTB/RIF test machines except 2 (1.8%) were operated in designated laboratory space and not at point-of-care (consultation room) or ward. Most HCFs prescribed Xpert MTB/RIF test to all presumptive TB cases, 86% (95/111). Where Xpert MTB/RIF was not prescribed to all, these groups of cases were prioritised, ‘health workers, prisoners, children (0–14 years), diabetic mothers, HIV positive clients who are coughing and on retreatment, contacts of drug-resistant TB patients, retreatment cases, treatment absconders, relapse cases, retreatment cases, refugees and expecting mothers’. It is important to note that by the end of 2019, Kenya, Tanzania and Uganda had updated their national TB control guidelines recommending Xpert MTB/RIF test to all presumptive cases hence more HCFs are currently having the Xpert MTB/RIF machines. Xpert MTB/RIF machine operational condition and reagent procurement were assessed and showed 87% (96/111) of the HCFs had their machines calibrated, 89% (99/111) had stable supply of cartridges and 76% (85/111) received the cartridges on time. The magnitude of effect by each factor varied from HCF-to-HCF with a trend to better service at high HCF level (figure 4A–F).
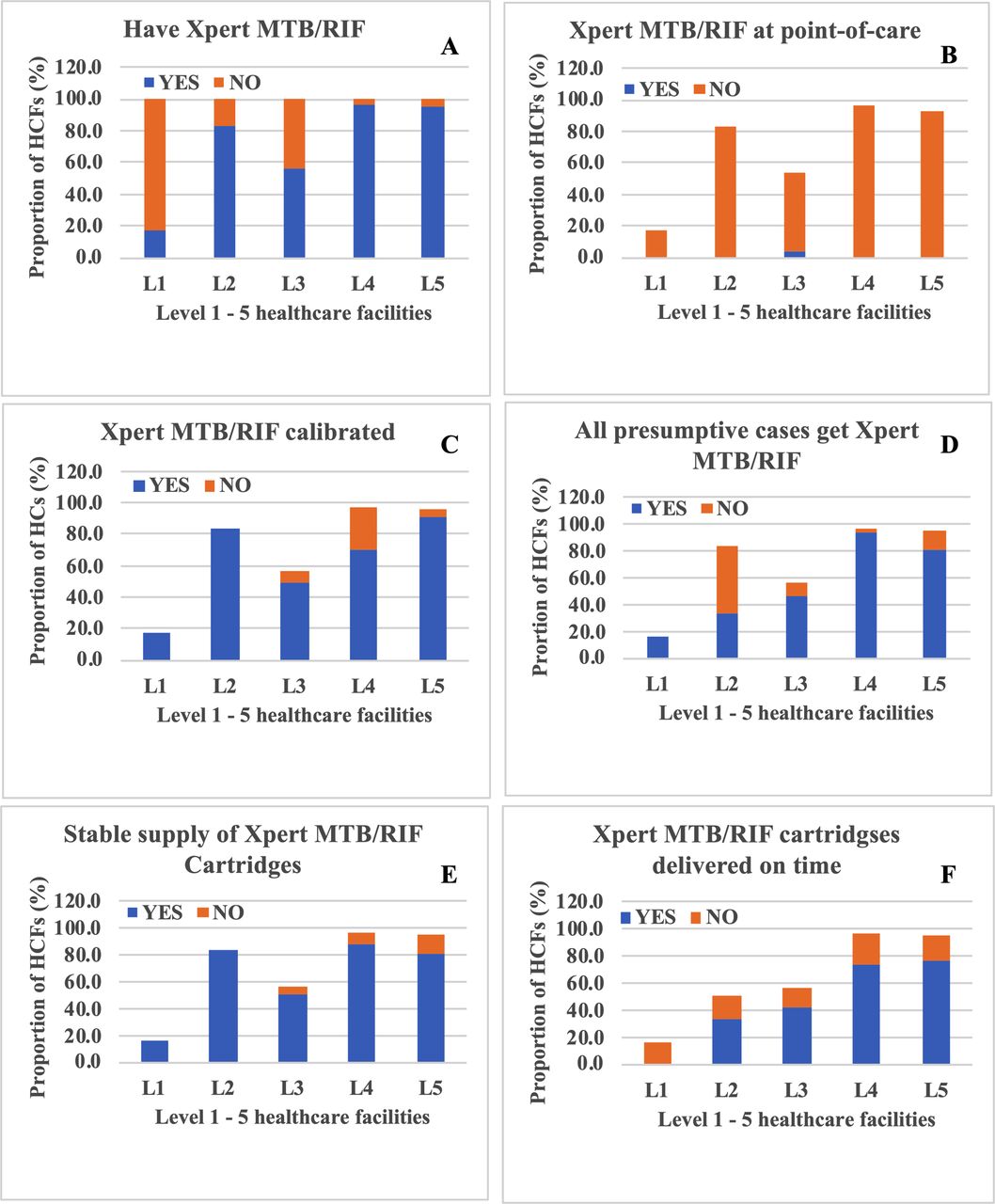
Availability, utilisation, calibration and procurement issues of Xpert MTB/RIF machines. Participants answered yes (blue bars) or no (orange bars) to (A) possession of Xpert MTB/RIF test instruments, (B) use of the instrument at point-of-care, (C) instrument calibration, (D) prescription of Xpert MTB/RIF test to all presumptive MTB/RIF cases, (E) stable supply of Xpert MTB/RIF reagent cartridges and (F) if these cartridges were delivered on time. There was a trend to better performances in all parameters at higher healthcare facility levels. HCFs, healthcare facilities.
Line Probe Assay
Utilisation of the LPA was quite irregular. Out of the four HCFs that had an established LPA service, one performed it on request, 64 tests per month, the second was twice a month, 24 tests per month and the third performed only the day they were trained and since then never performed it again. When asked what the limiting factor was for not performing LPA again, they said, ‘can’t tell, a team came here trained us on LPA and left, since then we have never done anything, we actually don’t remember what we learned’ Laboratory manager at a Regional Hospital. The fourth HCF gave no answer on how they used their LPA service. Of the four HCFs that had LPA, three (75%) were level 5 and one (25%) was level 4.
Underlying limitations for underutilisation or absence of Xpert MTB/RIF and LPA services
Some HCFs that had Xpert MTB/RIF attributed underutilisation of the service to inadequate human resource 22% (24/111), procurement difficulties, 12% (13/111), poor electricity and water supply, 12% (24/111) and 6% (7/111), respectively. The lack of Xpert MTB/RIF and LPA services was mainly attributed to insufficient finance at both district/county level (91% and 55%), and at the HCF level (56% and 21%), respectively. Lack of awareness was a second limiting factor to financing revealing 33% and 49% of the district/county health officers and healthcare practitioners were unaware of the LPA as a diagnostic test for TB. Inadequate human resource (24%), lack of water (26%) and electricity (26%) were also considered substantial limitation of implementation of Xpert MTB/RIF by practitioners at their HCFs (table 3). A total of 6%–9% reported procurement difficulties for the two diagnostics, which included reagent stockouts and delayed payment of requisitions by the healthcare management. ‘Failed procurement is not necessarily due to distant (overseas) sources of laboratory supplies, in most cases it is due to bureaucracy associated with releasing payments, sometimes taking up to 9 months to honour requisition or pay an invoice yet we have a stock of LPA kits here in Nairobi’, Kenyan Hain Life sciences officer.
The factors underlying lack of Xpert MTB/RIF and LPA services at district/county level and healthcare facility level
Inadequate space and test complexity were also identified as reasons for underutilisation of LPA. In principle conducting LPA requires three rooms (pre-PCR, PCR and post-PCR) to perform, ‘Very few HCFs in the country have such space and person time to perform LPA’, Tanzanian senior laboratory scientist.
Culture
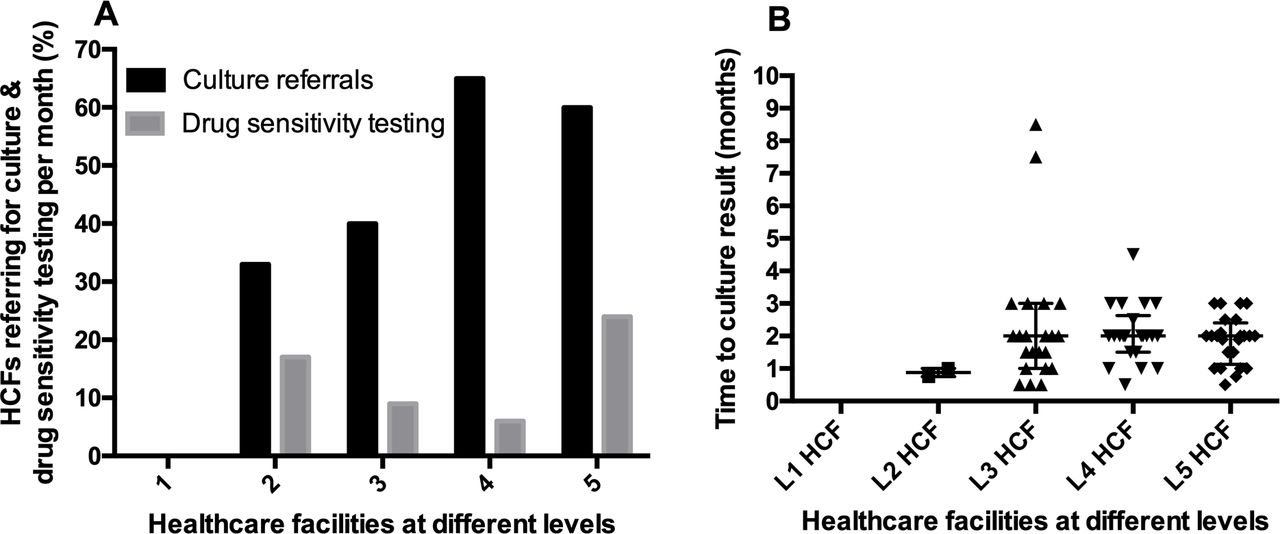
Like LPA, culture was a less used diagnostic, 49.6% (72/145) of the facilities that we audited. The median (range) of culture testing was 1 (0–347) test per month. While no culture test was prescribed by HCF level one, L2, L3, L4 and L5 prescribed 0.1 (0–0.2), 0.3 (0–36), 0.4 (0–13) and 10 (0–347) cultures per month, respectively. Utilisation improved with HCF level, 0% (0/6), 33% (2/6), 40% (23/57), 65% (22/34) and 60% (25/42) level 1, 2, 3, 4 and 5 HCFs referring samples for culture. Where culture was prescribed, the percentage referral for drug sensitivity testing (DST) was 25% (18/72) overall and varied across HCF levels, 17% (1/6), 9% (5/57), 6% (2/34) and 24% (10/42) at different HCF level 2–5, respectively. Time to culture restult was on average 2 month for all HCF (figure 5A,B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Healthcare facilities that referred samples for (A) culture (black bars) and drug sensitivity testing (grey bars). (B) Time to culture result across different healthcare facilities. Level 5 HCFs performed substantially more DST than lower level HCFs. The less median time-to-result by level 2 HCFs is because there were only two HCFs that referred samples for culture, insufficient to compute meaningful median. DST, drug sensitivity testing; HCFs, healthcare facilities.
Monitoring response to anti-TB therapy
Most of the 145 audited HCFs, 79% (114) used microscopy as the only tool for monitoring treatment. This included 83% (5/6), 50% (3/6), 82 (47/57), 88% (30/34) and 69% (29/42) level 1, 2, 3, 4 and 5 HCFs, respectively. Other treatment monitoring methods used alone were clinical assessment, 2% (3) and Xpert MTB/RIF 0.7% (1). One of each level 2, 3 and 5 HCF used clinical assessment only while one level 3 HCF used Xpert MTB/RIF. Some HCFs used a combination of monitoring methods, 3% (4), 4% (5), 4% (5), 1.4% (2) and 0.7% (1) for microscopy-clinical assessment, microscopy-Xpert MTB/RIF, Xpert MTB/RIF-culture and microscopy-Xpert MTB/RIF-chest X-ray, respectively. Combination of microscopy and culture was available at two level 4- and three level 5- HCFs only. Microscopy-Xpert MTB/RIF was present at one level 1 and two of each level 3 and 5 HCFs while microscopy-Xpert MTB-chest X-ray was available at one level 3 hospital.
Human resource capacity
All HCFs employed certificate and diploma level laboratory technicians and medically qualified staff with highest proportion (100%) at level 1 and 2 HCFs, respectively. There was no bachelor degree qualified laboratory staff at level 1 HCFs. The highest proportion of master’s degree holders, 38% and clerical staff, 75% was found at level 5 HCFs (table 4).
Human resource capacity at different HCF levels
Diagnostic choice making
With a subset of healthcare practitioners (N=22), we explored the qualities they would consider when choosing a diagnostic test for their practice. A total of 95% and 82% of the practitioners preferred an expensive but more accurate and harder to perform but shorter time-to-result diagnostic to a low cost—less accurate and longer time-to-result test, respectively (table 5).
Qualities that inform choice of diagnostic test by practitioners
Policy-makers’ engagement
Policy-makers were engaged at the initiation—during and after completion—of the study. Prestudy engagement gave policy-makers’ perspective on the important matters the study should focus on and the channels through which findings can be communicated to policy-making organs. A total of 11 policy-makers engagement workshops were held, three each in Kenya and Tanzania and five in Uganda. Dialogues ranged from ways to make research to policy making to sustainable uptake and utilisation of diagnostic technologies for better health outcomes. Policy-makers were keen to be involved in research right from inception to the end in order to increase translation of outputs into policy and practice. Demonstrating research outcomes and impact at county (region) level before scale-up to national level was particularly recommended as the best way to increase uptake of health research innovations. Creating a national health tax and permitting county-regional governments to invest a percent of local collected revenues was proposed as means of increasing domestic financing and ensure sustainable uptake and utilisation of health technologies.
Discussion
Early diagnosis of TB is essential because it shortens time to appropriate treatment, prevents severe morbidity and mortality.15 21 Using implementation of TB diagnostics as a model and benchmarking on the WHO recommendations, we assessed the barriers and opportunities to overcome them for maximal uptake and utilisation of diagnostic tools into policy and practice in in LMIC setting. At the time of research, 2016–2017 the WHO implementation recommendation was district and regional hospital level for Xpert MTB/RIF and LPA, respectively.8 9 Full capacity use of Xpert MTB/RIF was set at a minimum of eight tests per day while no utilisation limit was set for LPA. It is important to note that the actual impact of WHO recommendation is realised by customisation into country specific policy guidelines.
In the study countries, use of Xpert MTB/RIF and LPA was not universal for all presumptive TB. Xpert MTB/RIF was recommended for HIV positive cases or those who have been in contact with drug resistant case.22–24 LPA was modelled along the use of culture recommendation, that is, referral for culture and DST for smear positive cases at 2 or 3 months of anti-TB treatment. We note that the algorithm for Xpert MTB/RIF has since changed to cover all presumptive TB cases and future studies should test whether this has improved the rate of utilisation.
Irrespective of the TB testing algorithm, our findings show that there are fundamental health system and socioeconomic—cultural barriers that hinder maximal uptake and utilisation of health technologies. In this paper, we focus on health system challenges and show that uptake and utilisation of molecular and microbiological (culture) diagnostics in LMIC setting is still below expectation. Low uptake of diagnostics was mainly attributed to underfinancing of healthcare followed by lack of awareness by both district health officers and practitioners at HCFs. Procurement difficulties, inadequate human resource and utilities such as water and electricity were highlighted as underlying suboptimal utilisation of molecular diagnostics hereby referred as Xpert MTB/RIF and LPA.
While the private sector plays a major role in providing healthcare in the studied countries, government was found to be the main TB service provider, giving over 80% of diagnostic and treatment services. This could be due to the complexity of managing TB that deters private healthcare providers from investing in it. In this case, the importance of government in expanding access of diagnosis and treatment services cannot be more emphasised. This makes public servants like district/county health officers even more important. Our findings show that the health officers were well informed of the state of health services in their areas of jurisdiction because their survey responses were corroborated by healthcare practitioners at the HCFs. However, there was no correlation between the roles they performed and degree of implementation of diagnostic tools.
Despite its technical limitations, smear microscopy was widely implemented and utilised diagnostic for TB at all levels of the healthcare system in Kenya, Tanzania and Uganda.25 26 We believe low-acquisition cost, space and energy requirements make the microscope more attractive for HCFs to implement.27 Furthermore, the microscope is a multipurpose platform often serving other functions such as diagnosis of malaria, helminths and other bacterial infections in low-income countries. Technical limitations such as low sensitivity and specificity for diagnosing TB have less impact on the choice of diagnostic methodology. Technical challenges notwithstanding, for example, the low sensitivity of smear microscopy revealed by the 2016 Kenya TB prevalence survey where smear microscopy only detected 46% cases compared with 78% by Xpert MTB/RIF,28 a device that serves other diagnostic needs at the HCF makes more economic sense when deciding technologies to purchase. Therefore, investing in open rather than closed systems will go a long way in maximising uptake of new health technologies into policy and practice.
WHO approved Xpert MTB/RIF for implementation up to district hospital level.9 29 Our results show that, out of the 57 level 3 (district/subcounty) hospitals, only 56% had the Xpert MTB/RIF instruments and only 14% used the instruments to capacity, that is, performing eight or more tests per day. There was, instead, higher, close to 100% coverage at level 4 and 5 HCFs with corresponding high full capacity utilisation of 27% and 51%, respectively. It is, therefore, not clear the model followed in allocating the Xpert MTB/RIF instruments. For instance, in Kenya some counties had more than one Xpert MTB/RIF instruments per subcounty while others had two instruments serving over 10 subcounties. In line with this observation Oliwa et al found variability in spatial distribution of diagnostic services in Kenya suggesting a non-need driven allocation of diagnostic platforms.30
Only two (1.4%) of the audited HCFs used the Xpert MTB/RIF at point-of-care (in consultation room). In most cases, Xpert MTB/RIF results were not available in the same day, which means the speed advantage of Xpert MTB/RIF is not being realised. It is also not clear whether both doctor consultation and Xpert MTB/RIF testing were going on in the same room. The higher the HCF was in the health system hierarchy the higher the utilisation of Xpert MTB/RIF instruments. Limitations such as procurement, inadequacy of utilities and human resources were less frequent at higher level HCFs. In line with Pooran et al, our findings show that a hub system with an effective sample referral network may be more cost-effective than placing Xpert MTB/RIF machine at every HCF.31 With this approach, Xpert MTB/RIF may no longer qualify as near point-of-care test, but its utilisation will be more cost-effective. It has been suggested, however, that decentralisation of Xpert MTB/RIF can be cost-effective if the testing volumes are high in peripheral HCFs32 and there is good flow of funds to ensure availability of consumables. The high testing volume—decentralisation model contradicts the novel battery powered single module point-of-care GeneXpert OMNI because it would require 16 hours to test eight samples thus increasing turn-around-time and cost more to implement in high TB burden settings.33 34
The LPA was the least implemented diagnostic test, yet it is the only approved rapid DST diagnostic for multidrug-resistant TB.35 Although approved for implementation at regional (L4) hospital, only 1/34 (3%) reported possession of LPA platform, which they were unfortunately unable to execute since they were trained by the test manufacturers. Lack of awareness emerged as the second main factor limiting the implementation of LPA. Surprisingly, almost 50% of health administrators and practitioners were not aware of LPA as a diagnostic for TB. Without awareness, there is no chance that such a diagnostic could be on the list of diagnostics to acquire by either HCF or district health administration. Furthermore, lack of awareness by practitioners is most likely to limit referrals for a given test and thus hindering its utilisation. Space intensiveness and laboriousness were highlighted as limitations for high utilisation by HCFs who had the LPA service. This is an eye opener for health technology developers to make technologies that are compatible with the available infrastructure as well as investing in increasing awareness and accessibility of these technologies especially in high TB burden settings.
Culture, the gold-standard diagnostic for TB36 was only found at a 5% implementation level across the three countries. All culture laboratories were associated with level 5 HCFs (national, consultant or zonal referral hospitals). On average culture laboratories serve 20 million or more people. Level 5 hospitals were more likely to perform culture and DST than lower HCFs which did not have the facilities. The presence of a culture laboratory at a facility did not change the time-to-culture-result, 2 months at level 3, 4 and 5 HCFs. An extended time-to-result could discourage clinicians from referring samples for culture since the results would not come in time to inform their clinical decisions. The limited availability of culture labs and very low referrals for culture shows the three countries are not on course to achieve the universal DST access target of 100% by 2020 (WHO framework of indicators and targets). While culture is relatively easy to perform and cheaper, practitioners indicated they would spend a little more money for a hard to perform, expensive but accurate test with shorter time-to-result diagnostic technology. The underutilisation of culture could also be attributed to the WHO algorithm because the recommendation at the time of the study suggested a culture be performed if the patient sputum is smear positive at month two or three of treatment.26 37
The low degree of coverage and utilisation of molecular and culture tests revealed by our study is an indication that TB is most likely underdiagnosed in the region and more so, drug resistant TB. Global estimates show 3 million TB cases go undetected every year.7 Our findings also indicate that universal DST as recommended by WHO is currently unachievable until such a time when the countries have developed required diagnostic capabilities.38 Treatment response monitoring needs of drug susceptible TB in the region are largely met due to wide coverage of smear microscopy but not drug resistant TB which requires a combination of microscopy and culture to monitor.37 39 Challenges associated with microscopy and culture for monitoring treatment response led the WHO to recognise the University of St Andrews developed TB Molecular Bacterial Load Assay (TB-MBLA) as a candidate to replace the two tests for monitoring TB treatment response.40 41 Like other molecular diagnostics, maximising uptake and utilisation of TB-MBLA requires addressing the barriers highlighted in this paper.
In the same trend, human resources capacity increased with the level of HCF, which partly explains higher uptake and utilisation of diagnostic services at these healthcare centres. Higher level HCFs are more likely to be in the urban centres with many social amenities attractive to professionals to come work and stay. Deliberate efforts must be made by national governments to ensure appointment and retention of healthcare practitioners in rural areas.
Health budgets in the study countries are largely donor dependent and thus any economic downturns in donor countries have ripple effect on the delivery of diagnostic and treatment services in LMIC settings. This is more so in the era of the COVID-19 pandemic that has ravaged global economy with traditional donor countries experiencing up to 10% or more shrinking of their economies.12 It is more prudent to state that LMICs probably need to address the need to increase domestic funding for healthcare including TB control services if the End TB Strategy has to be realised.
Engaging policy-makers unravelled valuable ideas on how to practically increase research impact and domestic financing to sustain uptake of health technologies and ensure quality healthcare. A Health tax on particular goods and services to build revenue base for funding healthcare programmes, research and innovation was recommended as the best way to go. The views from policy-makers clearly demonstrate how an invaluable partner they are in research and its translation to policy and practice. Response to COVID-19 is a good example where in most countries scientists and policy-makers have worked hand-in-hand to use available knowledge and tools to save lives while searching for more effective medical remedies goes on.
Conclusion
Our results have revealed that the health system set up favours maximal uptake and utilisation of both molecular and microbiological diagnostics at tertiary rather than lower healthcare levels. They point to a hub-centralised model of implementation as the most effective for maximising uptake and utilisation of molecular diagnostics. It is important to note, however, that the success of a centralised system also requires unlocking the health system barriers to increase awareness, smoothen sample referral path and shorten results turn-around-time.42 Centralised system may mean low access to diagnostic services by people in rural and hard to reach areas, thus innovative ways to ensure access by such communities are crucial. The findings also show low diagnostic capacity for drug resistant TB in the region, which means they are far from achieving the universal DST recommended by WHO. This paper further emphasises that health system bottlenecks are multifactorial and thus call for multisectoral interdisciplinary approach to address them.14
Data availability statement
Data are available on reasonable request. Data available at School of Medicine Division of Infection and Global Health, WS, ws31@st-andrews.ac.uk. Requests will be reviewed by the ethics Committee to assess their compliance to confidentiality and limits of consent given by study participants.
Ethics statements
Ethics approval
The study gained ethical approval from respective institutional and national ethics committees represented in the consortium. In the UK, approval was obtained from University Teaching and Research Ethics Committee of University of St Andrews (MD12073), Uganda: Makerere University Institutional Research Ethics Board (IRB) and National Council of Science and Technology (HS 2129), Kenya: KEMRI Scientific and Ethics Review Unit (KEMRI/RES/7/3/1) and Tanzania: KCRI and Mbeya and southern highlands zonal IRBs and National Health Research Ethics Committee (NatHREC) at NIMR headquarters (NIMR/HQ/R.8a/vol.IX/1317). In addition to ethics approvals, access permissions were sought and obtained from local government authorities and healthcare facilitie involved in the study.
Acknowledgments
The authors acknowledge the contributions of Dr Ewan Chirnside and Professor Gibson Kibiki in the initial study conception, design and implementation of the study. Professor Kibiki also played a big role in linking the TWENDE consortium to East African Health Research Commission (EAHRC). As a result of his effort, EAHRC officially adopted TWENDE as a research consortium for generating evidence needed for translation of health technologies to policy and practice in the East African Community. Special thanks to the members of the community, healthcare administrators and practitioners, and policy-makers who participated in the study and gave important insights that make the basis of this paper.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Senjuti Saha
Twitter @dkomics, @Infection_StAnd
Contributors WS, NEN, EA, MJ and SHG: Conceived and designed the study; WS, FO, IM, AL, FN, KK, BM, EFM, ES, HM, DK, SM and BTM: Developed the research tools and collected the data; FO, IM, FN, WO, LM, NEN and WS: led database cleaning and data analysis; NEN and WS: drafted the manuscript; WS and AA: drew the figures and maps; all authors: reviewed the manuscript and SHG: proofread the manuscript.
Funding The study was funded by the European and Developing Countries Clinical Trials Partnership (EDCTP), grant TWENDE-EDCTP-CSA-2014-283.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.