Article Text

Abstract
Background Growing evidence suggests that compromised lung health may be linked to cardiovascular disease. However, little is known about its association with sudden cardiac death (SCD).
Objectives We aimed to assess the link between impaired lung function, airflow obstruction and risk of SCD by race and gender in four US communities.
Methods A total of 14 708 Atherosclerosis Risk in Communities (ARIC) study participants who underwent spirometry and were asked about lung health (1987–1989) were followed. The main outcome was physician-adjudicated SCD. Fine-Gray proportional subdistribution hazard models with Firth’s penalised partial likelihood correction were used to estimate the HRs.
Results Over a median follow-up of 25.4 years, 706 (4.8%) subjects experienced SCD. The incidence of SCD was inversely associated with FEV1 in each of the four race and gender groups and across all smoking status categories. After adjusting for multiple measured confounders, HRs of SCD comparing the lowest with the highest quintile of FEV1 were 2.62 (95% CI 1.62 to 4.26) for white males, 1.80 (95% CI 1.03 to 3.15) for white females, 2.07 (95% CI 1.05 to 4.11) for black males and 2.62 (95% CI 1.21 to 5.65) for black females. The above associations were consistently observed among the never smokers. Moderate to very severe airflow obstruction was associated with increased risk of SCD. Addition of FEV1 significantly improved the predictive power for SCD.
Conclusions Impaired lung function and airflow obstruction were associated with increased risk of SCD in general population. Additional research to elucidate the underlying mechanisms is warranted.
- emphysema
- respiratory measurement
- COPD epidemiology
- critical care
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information. All data relevant to the study are included in the article or uploaded as supplementary information.
Statistics from Altmetric.com
Key messages
What is the key question?
Impaired lung function increases the risk of coronary artery disease, heart failure and ventricular arrhythmias, but is there an association between impaired lung function and sudden cardiac death?
What is the bottom line?
Baseline lung function was inversely associated with increased risk of sudden cardiac death, independent of race and gender, established cardiovascular risk factors and systemic markers of inflammation.
Why read on?
The results indicate that impaired lung function should be considered an important risk factor for sudden cardiac death.
Introduction
Sudden cardiac death (SCD) is a major health concern that constitutes 50% of cardiovascular mortality, with a currently estimated incidence of 4–5 million cases worldwide annually.1 Survival from cardiac arrest remains poor despite advances in resuscitation, hence requiring identification of predisposing factors applicable to the general population. Traditional risk factors for SCD include male sex, old age, genetic variants, history of structural heart disease, channelopathies and arrhythmogenic drug use.2 However, recent cohort studies suggest that SCD is a heterogeneous outcome that is largely unrelated to traditional risk factors and may involve multiple unrecognised aetiological pathways that directly affect cardiac function and arrhythmogenesis.3–5
COPD may be one such non-traditional risk factor for SCD. A growing body of evidence confirms strong associations between impaired lung function and cardiovascular diseases, including coronary artery disease, heart failure and ventricular arrhythmias.6 Poor lung function is also associated with increased mortality.7 8 However, few large-scale community-based cohort studies comprehensively assessed the link between subclinical or spirometry-based airflow obstruction and risk of SCD.6 9 In addition, given that smoking status is a strong potential confounding factor, an evaluation of these associations among those that never smoke is of particular importance. Finally, blacks are poorly represented in epidemiological studies from which current standards of care and treatment guidelines of SCD are derived, and this calls for studies to fill in knowledge gaps regarding SCD in blacks, who often experience higher incidence rate of SCD compared with whites.
Therefore, our objective was to assess whether impaired lung function, as assessed by reduced FEV1, and airflow obstruction, identified by self-reported diagnosis or spirometry, were independent risk factors for SCD in the general population, and whether the associations were modified by race, gender and smoking status.
Methods
Study population
The design of the Atherosclerosis Risk in Communities (ARIC) study has been described previously.10 In brief, 15 792 participants between 45 and 64 years of age were recruited from four communities across the USA (Washington County, Maryland; Forsyth County, North Carolina; Jackson, Mississippi; and suburban Minneapolis, Minnesota) between 1987 and 1989 to take part in a prospective study of cardiovascular disease. Participants underwent a standardised evaluation of cardiovascular risk factors and returned for four follow-up examinations (1990–1992, 1993–1995, 1996–1998 and 2011–2013). They continued to be followed via semiannual telephone calls to ascertain the study end point. Study population and procedures performed at the baseline and outcomes have been described previously. We obtained the cohort data sets from the NIH Biologic Specimen and Data Repository Information Coordinating Center.11 12
Assessment of lung function
ARIC conducted spirometry at visit 1 baseline using a water-sealed Collins Survey II volume displacement spirometer (Collins Survey II; Collins Medical, Braintree, Massachusetts, USA) and Pulmo-Screen II software (Pulmo-Screen; PDS Healthcare Products, Louisville, Colorado, USA). Spirometry was performed by trained and certified technicians following the American Thoracic Society (ATS) guidelines, using a standardised protocol.13 Quality control was carefully monitored throughout the study, as described previously.13 In the current study, only prebronchodilator measurements of lung function were available. The main measure of lung function was FEV1, the volume of gas that has been exhaled at the end of the first second of forced expiration. The FVC, the total volume of gas exhaled, was also examined, as well as the ratio of FEV1 to FVC. Supplemental analyses were performed with the percentage of predicted FEV1 and FVC adjusted for age, sex, race and height, obtained from equations for predicting FEV1 and FVC.14
Respiratory disease history was assessed using a standardised self-administered questionnaire by trained personnel. Subjects were also asked whether a doctor has ever told them they had asthma, chronic bronchitis or emphysema/COPD. Airflow obstruction was defined as an FEV1/FVC ratio of <0.75.15 According to ATS/European Respiratory Society criteria, abnormal spirometry was graded on the basis of FEV1% predicted: (1) mild airflow obstruction defined as FEV1% predicted >0.70 and (2) moderate/moderately severe/severe/very severe airflow obstruction defined as FEV1% predicted ≤0.70.16
Sudden cardiac death
The methods for ascertainment of SCD events have been described previously.17 In the present study, SCD was defined as an unexpected and sudden pulseless situation of presumed underlying cardiac origin because of the absence of conditions clearly unrelated to cardiac arrhythmias.18 Study participants were not classified as SCD if there was evidence of an acute non-cardiac morbidity that could account for the death and conditions clearly unrelated to cardiac arrhythmias, such as car accident, drug overdose, cancer, massive blood loss, pneumonitis, pulmonary embolism, acute respiratory failure, stroke, aortic aneurysm rupture and myocardial rupture after myocardial infarction.
In the ARIC study, comprehensive data were gathered on all cardiovascular-related events from hospital discharge summaries, annual phone calls, physician questionnaires, prior medical history, next-of-kin interviews, and/or witnesses, death certificates, and coroner information, where available. ARIC study events committees adjudicated the causes of death. To identify SCD, cases of death from cardiovascular cause were reviewed and adjudicated by a committee of physicians, including internists, general cardiologists and electrophysiologists. All cases of cardiovascular death that occurred in the emergency room or out of the hospital were reviewed. Each case was adjudicated independently by two reviewers and was classified as being definite SCD, possible SCD, definite non-SCD and unclassifiable. In case of divergent results, a third blinded reviewer independently reinterpreted the medical records, and a final decision on SCD classification was reached by consensus.17 For the present study, SCD was defined as an adjudicated definite or possible SCD. Percentage inter-reviewer agreement was 83.2%.
Statistical analysis
Means (SD) for continuous variables and counts with percentages for categorical variables were calculated according to quintiles of FEV1. We applied multiple imputation based on five replications and the Markov chain Monte Carlo method to account for missing data of the covariates.19 Incidence rate ratio (IRR) and 95% CIs were estimated with the use of Poisson regression models.20 As there were other types of deaths aside from SCD among the cohort participants, Fine and Gray proportional subdistribution hazard models and cumulative incidence function were used to assess the associations of FEV1 (and FVC), and airflow obstruction with the risk of SCD, with results presented as HRs and 95% CI.21 Death other than SCD was used as a competing risk.22 To minimise potential bias due to low events per variable, Firth’s penalised partial likelihood correction was applied to the hazard models.23 24 Lung function parameters were first stratified into quintiles and then evaluated as continuous variables. The median values in each quintile were used as continuous variables for trend estimation.
In the multivariate analyses, we adjusted for traditional cardiovascular risk factors, proinflammatory and procoagulability markers, including age (continuous), race, gender, education level, body mass index, systolic blood pressure, smoking status, hypertension, diabetes mellitus, history of heart failure, low-density lipoprotein cholesterol, fasting blood glucose, fibrinogen level, albumin level, von Willebrand factor and corrected QT interval (QTc) duration. We selected these confounders on the basis of their associations with the outcomes of interest or a change in effect estimate of more than 10%.25 26 FEV1 and FVC vary widely by race and gender, as do SCD rates. Therefore, further analyses used either race-specific and gender-specific FEV1 groupings or were done separately by race and gender. The potentially strong confounding due to cigarette smoking was also addressed by stratified analysis by smoking for each race and gender group.
An adjusted model using a restricted cubic spline with five knots was constructed to flexibly display the association between the hazards of developing SCD and continuous covariate of FEV1 (and FVC).27 28 We also conducted sensitivity analyses by exclusion of those with prevalent heart failure or coronary heart disease (CHD) to remove the potential for confounding as a result of these conditions and exclusion of those without airflow obstruction to remove the potential for ascertainment bias. Finally, to evaluate the incremental prognostic value of the addition of FEV1 or FVC to the basic model, we calculated the model C statistics and net reclassification improvement (NRI). Because the disease status could change over time, and receiver operating characteristic (ROC) curve as a function of time might be more appropriate for the follow-up study, we further applied the time-dependent ROC (td-ROC) curves at 25 years to evaluate the model discrimination ability.23
We used Stata V.14.0, SAS V.9.4 and R V.4.0.3 for all analyses. Statistical tests were two sided and used a significance level of p<0.05.
Results
After exclusion of 1084 subjects for whom lung function parameters were missing or incomplete, we present results for the entire source population of 14 708 individuals (45.6% male; mean age 54.3 years). The study cohort consists of 10 998 (74.8%) whites and 3710 (25.2%) blacks and no other racial groups. Baseline demographic and clinical characteristics by quintiles of FEV1 are shown in table 1, and the missing values (%) by variables are summarised in online supplemental table 1. Subjects in the lower quintiles of FEV1 were more often females, blacks and current smokers, had older age, higher body mass index, shorter stature, higher blood pressure, higher levels of proinflammatory and procoagulability markers, higher resting hear rate and longer QTc interval and were more likely to have electrocardiographic signs of left ventricular hypertrophy and to use bronchodilators than those in the higher quintiles of FEV1.
Supplemental material
Baseline characteristics of the study population across quintiles of FEV1s
Lung function test and the risk of SCD
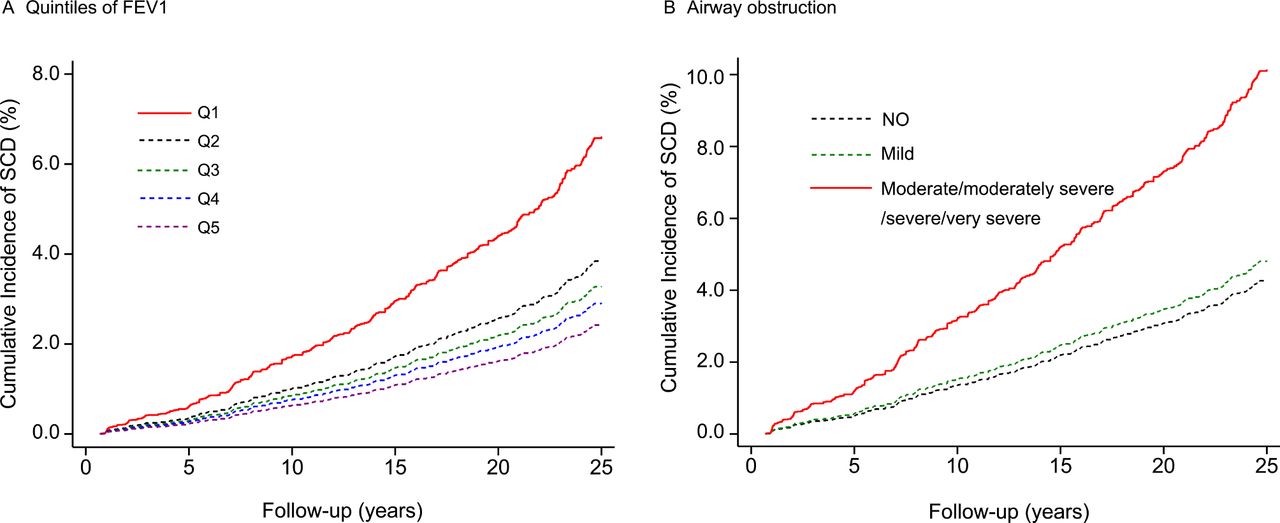
During a median follow-up of 25.4 (IQR: 19.9–25.6) years, 5045 subjects died. The median survival time for those who died was 15.9 (IQR: 10.0–20.1) years. Of these deaths, 706 were adjudicated as SCD (incidence rate=2.22 per 1000 person-years). Table 2 and online supplemental table 2 present unadjusted and multivariate-adjusted HRs of SCD associated with FEV1, FVC and other risk factors. In unadjusted analysis, subjects in the lowest (Q1) quintile of FEV1 and FVC showed significantly higher risk for SCD than those in the highest (Q5) quintile, with unadjusted HRs for the lowest (vs the highest) quintile of FEV1 and FVC were 2.05 (95% CI 1.63 to 2.58) and 1.74 (95% CI 1.39 to 2.48), respectively. Adjustment for multiple confounding risk factors seems to strengthen these associations. In the fully adjusted model, the corresponding HRs of SCD comparing subjects in the lowest quintile with the highest quintile were 2.72 (95% CI 2.03 to 3.64) for FEV1 and 2.59 (95% CI 1.87 to 3.58) for FVC. Of note, males compared with females (adjusted HR: 3.47 (95% CI 2.80 to 4.30)) and blacks compared with whites (adjusted HR: 1.23 (95% CI 1.01 to 1.45)) experienced increased risk of SCD. However, use of bronchodilators or inhaled corticosteroids (ICS) did not seem to be associated with risk of SCD. Cumulative incidence functions also revealed a monotonic association between FEV1 and risk of SCD throughout the study period (figure 1A).

Cumulative incidence of sudden cardiac death by quintiles of FEV1 (A) and by airflow obstruction defined by spirometry data (B). Q1 is the lowest quintile, and Q5 is the highest quintile. Curves were estimated using competing risk analysis. Adjusted for age (continuous), race, gender, education level, body mass index, systolic blood pressure, smoking status, hypertension, diabetes mellitus, history of heart failure, low-density lipoprotein cholesterol, fasting blood glucose, fibrinogen level, albumin level, von Willebrand factor and QTc duration.
HRs (95% CIs) of SCD according to quintiles of FEV1 and FVC*
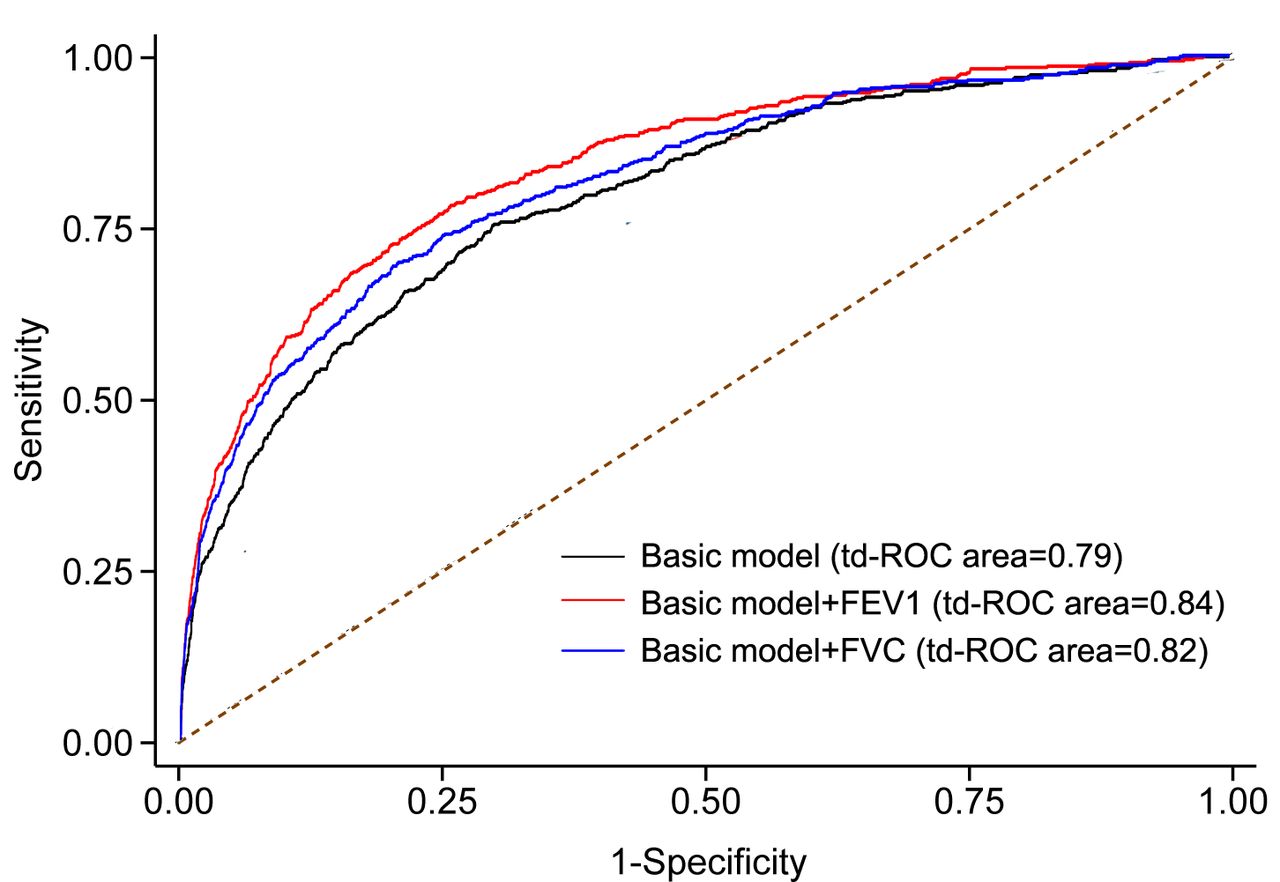
On receiver operating characteristic curve analysis, the model for SCD had a significantly higher predictive value when FEV1 was included (C statistic: 0.77 (95% CI 0.75 to 0.79)) compared with when it was not (C statistic: 0.74 (95% CI 0.72 to 0.76); p<0.001). The reclassification analysis also yielded a significant continuous NRI as 40.7% (95% CI 32.3% to 49.2%; p<0.001) (table 3). In addition, inclusion of FEV1 to the baseline model displayed a significantly higher td-ROC than baseline model only (td-ROC area: 0.84 (95% CI 0.82 to 0.86) vs 0.79 (95% CI 0.77 to 0.82), p<0.001). Similar results were observed for FVC (figure 2).
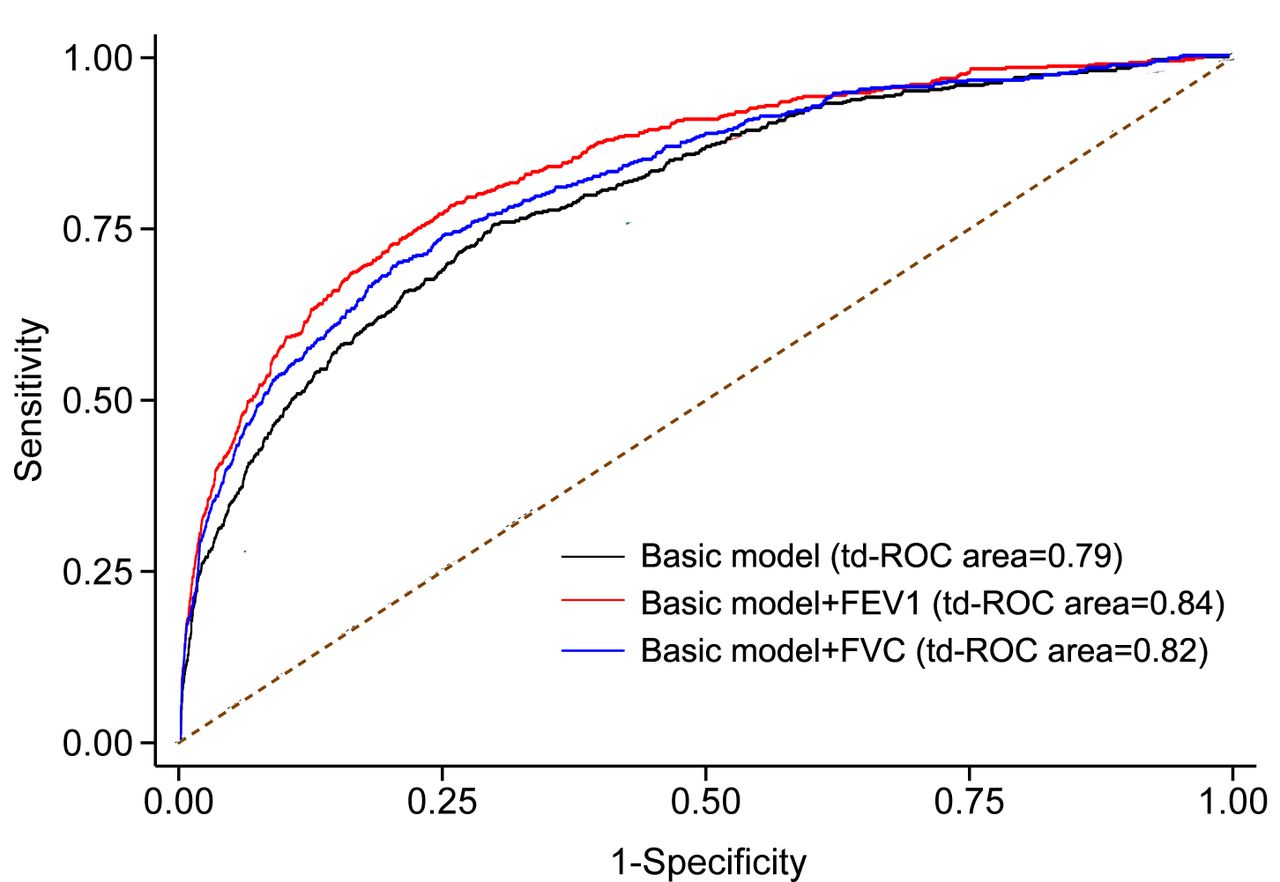
Comparison of time-dependent receiver operating characteristic (td-ROC) curve area at 25 years for sudden cardiac death between the full model without and with FEV1 or FVC.
Incremental prognostic value of the addition of FEV1 or FVC to the basic model for SCD
Stratified analysis by gender and race
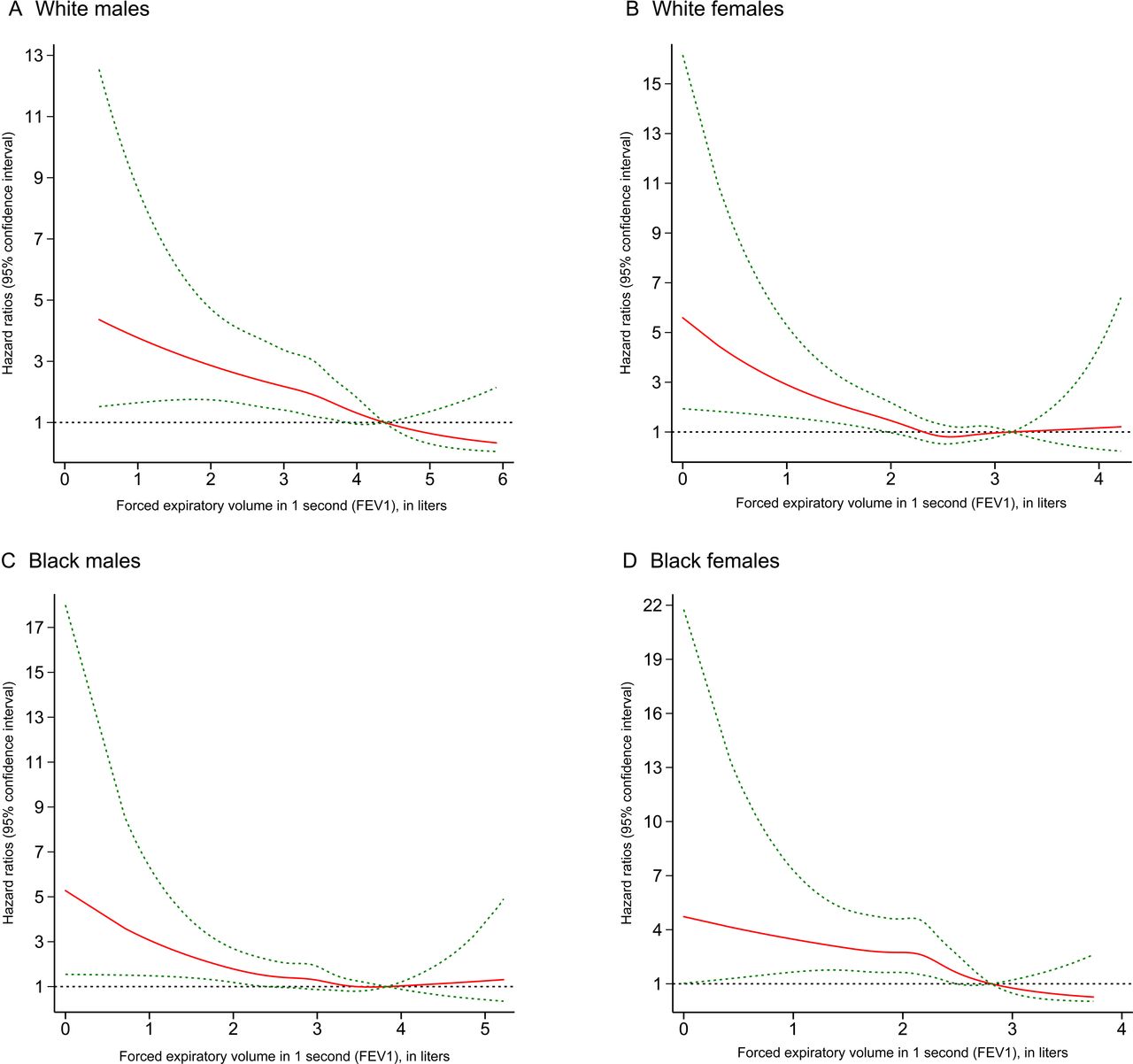
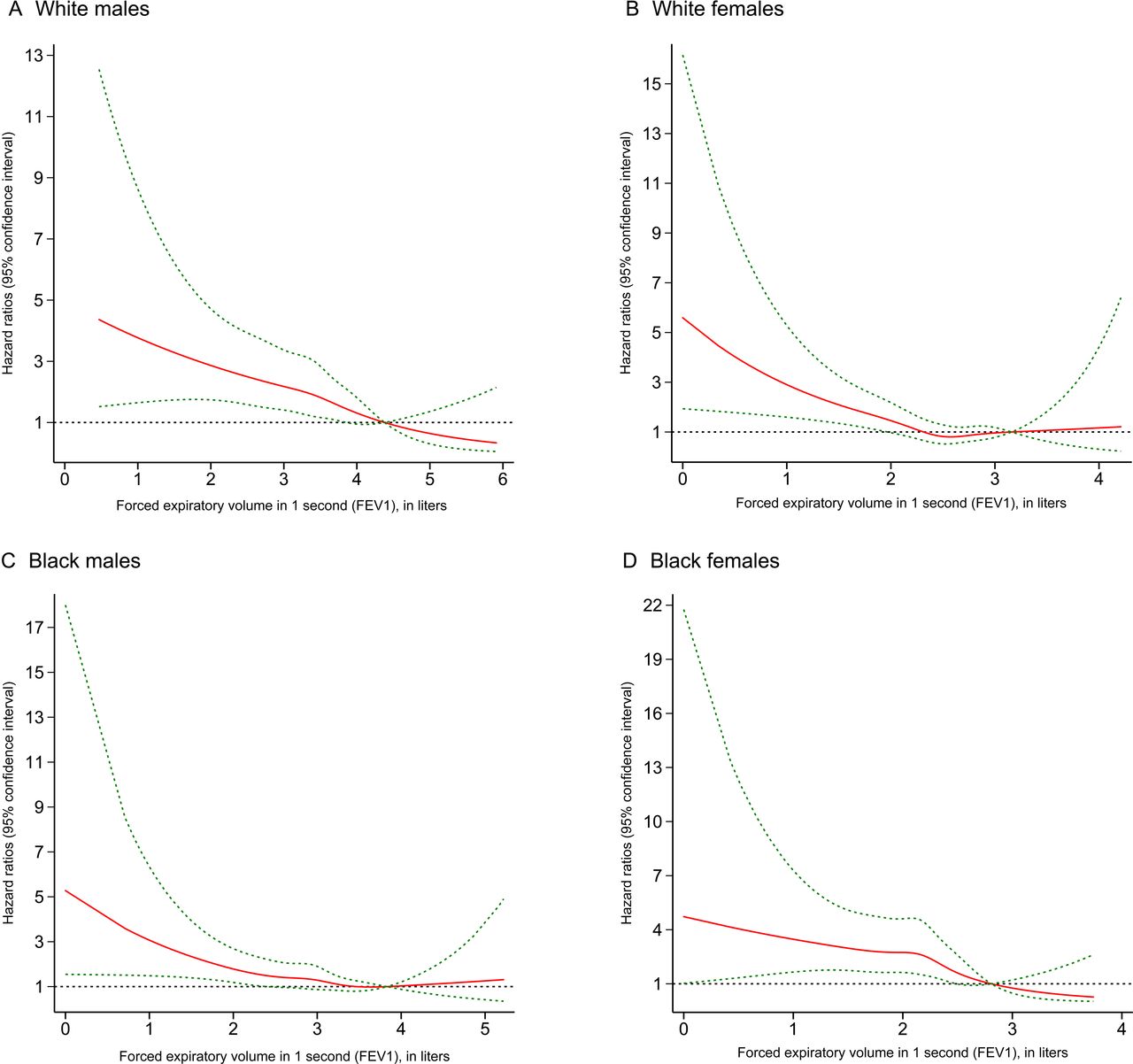
Figure 3 is a boxplot graph showing the distribution of FEV1 and FVC in each race-specific and gender-specific group. The baseline FEV1 and FVC were higher in whites than in blacks for both genders (p<0.001). The incidence rate of SCD decreased monotonically and inversely with higher FEV1 quintiles after adjusting for age and height for both genders in each race group. The adjusted average incidence rates of SCD per 1000 person-years were (from the lowest to highest quintile) 4.67, 3.34, 2.79, 2.17 and 1.05 for white males; 2.46, 1.07, 0.74, 0.62 and 0.43 for white females; 10.19, 4.94, 5.83, 3.26 and 2.81 for black males; and 4.58, 4.17, 3.28, 1.58 and 0.95 for black females (table 4). In subdistribution hazard models adjusted for multiple confounding risk factors, the risk for SCD increased inversely and monotonically by quintiles of FEV1, in white males, white females and black males (figure 4). The adjusted HRs comparing those in the lowest quintile of FEV1 with those in the highest for SCD were 2.62 (95% CI 1.62 to 4.26) among white males, 1.80 (95% CI 1.03 to 3.15) among white females, 2.07 (95% CI 1.05 to 4.11) among black males and 2.62 (95% CI 1.21 to 5.65) among black females. No statistical interaction by race or gender was present, though magnitudes of effect tended to be larger in white males than in black males and in black females than in white females (table 4). In the adjusted restricted cubic spline models, the HR also decreased monotonically in each race-specific and gender-specific group. The FEV1 values under the cutoffs of 3.85 L for white males, 1.96 L for white females, 2.40 L for black males and 2.49 L for black females were associated with significantly increased risks of SCD (figure 5). The above-mentioned associations were observed across all smoking status categories for white males. Of note, in analyses restricted to never smokers for all race and gender groups, significant inverse associations between lung function and SCD were observed (table 5).
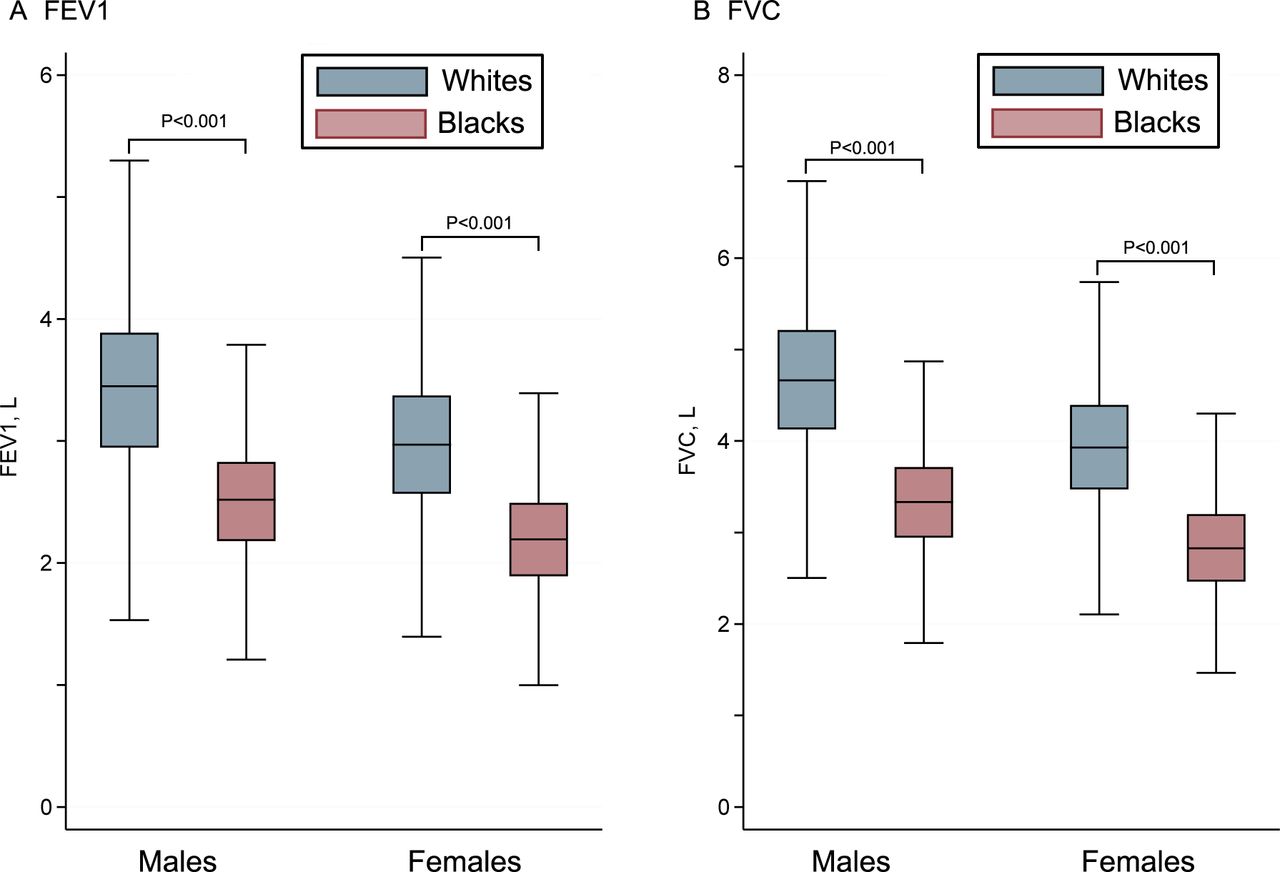
Boxplot graph of the distribution of FEV1 and FVC for each gender and race.

Estimated adjusted HRs (95% CIs) of sudden cardiac death for the quintiles of FEV1 for each gender and race. The y axis is plotted on a log scale. Adjusted for age (continuous), race, gender, education level, body mass index, systolic blood pressure, smoking status, hypertension, diabetes mellitus, history of heart failure, low-density lipoprotein cholesterol, fasting blood glucose, fibrinogen level, albumin level, von Willebrand factor and QTc duration.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The adjusted HRs (solid line) with 95% CIs(dotted lines) of sudden cardiac death by FEV1 in white males (A), white females (B), black males (C) and black females (D). The curves are plotted using restricted cubic splines with multiple knots. Adjusted for age (continuous), education level, body mass index, systolic blood pressure, smoking status, hypertension, diabetes mellitus, history of heart failure, low-density lipoprotein cholesterol, fasting blood glucose, fibrinogen level, albumin level, von Willebrand factor and QTc duration.
Race-specific and gender-specific HRs (95% CIs) of SCD according to quintiles of FEV1*
Race-specific and gender-specific HR (95% CI) of SCD according to quintiles of FEV1 by smoking status*
In sensitivity analysis, we excluded subjects with prevalent CHD or chronic heart failure and found that the risk estimates seemed to be higher than the main findings. Further analyses by restricting to those without prevalent airflow obstruction also demonstrated a somewhat greater risk than the overall population (online supplemental table 3). Additional analyses based on the continuous variable were also performed, as the relations between FEV1 with risk of SCD appear to be approximately monotonic. The adjusted HRs of race and gender-specific 1-SD decreases of FEV1 were 1.34 (95% CI 1.17 to 1.54) among white males, 1.42 (95% CI 1.09 to 1.85) among white females, 1.26 (95% CI 1.01 to 1.57) among black males and 1.37 (95% CI 1.12 to 1.67) among black females (online supplemental table 4).
Similar patterns were also observed for FVC, FEV1% predicted and FVC% predicted quintiles in subanalyses. In multivariable models adjusted for cardiovascular risk factors, the HRs comparing the lowest with the highest quintile of FVC were only significant in white males, and an inverse association was still significant for both genders in each race group. The adjusted HRs for the lowest versus highest quintile of FEV1% predicted were 2.08 (95% CI 1.36 to 3.17) for white males, 1.82 (95% CI 1.01 to 3.29) for white females, 2.21 (95% CI 1.20 to 4.06) for black males and 2.03 (95% CI 1.06 to 3.90) for black females (online supplemental table 5). Similarly, FVC% predicted was associated with increased risk of SCD. However, the outcome did not differ significantly by race or by gender.
Of note, the multivariate-adjusted HRs comparing subjects in the lowest quintile of FEV1/FVC ratio with subjects in the highest quintile were 1.50 (95% CI 1.04 to 2.16) for white males, 2.71 (95% CI 1.50 to 4.93) for white females, 1.40 (95% CI 0.80 to 2.46) for black males and 1.84 (95% CI 1.01 to 3.36) for black females. The cut points for quintile FEV1/FVC ratio were 0.67, 0.72, 0.76 and 0.79 for white males; 0.70, 0.74, 0.78 and 0.80 for white females; 0.69, 0.74, 0.78 and 0.81 for black males; and 0.72, 0.77, 0.80 and 0.83 for black females. The boundary of FEV1/FVC ratio quintile was approximately 0.70 for most race–gender groups, and subjects with a value below the boundary had a log-linear increase in risk of SCD (online supplemental table 5).
Airflow obstruction and risk of sudden cardiac death
In multivariable adjusted models, moderate to very severe airflow obstruction as defined by spirometry (adjusted HR: 2.37 (95% CI 1.86 to 3.01)) was associated with risk of SCD but not mild airflow obstruction (adjusted HR: 1.13 (95% CI 0.96 to 1.33)). Cumulative incidence functions also suggested a monotonic association between moderate to very severe airflow obstruction and SCD (figure 1B). Of note, 85.6% of the subjects with self-reported history of emphysema or COPD, and 60.0% of the subjects with self-reported history of bronchitis had airflow obstruction. However, the significant association with SCD was only observed in subjects with self-reported physician diagnosis of emphysema or COPD (adjusted HR: 1.82 (95% CI 1.09 to 3.03)) but not in those with self-reported physician diagnosis of bronchitis (adjusted HR: 0.85 (95% CI 0.63 to 1.14)) or asthma (adjusted HR: 0.81 (95% CI 0.57 to 1.15)). In addition, use of bronchodilators (adjusted HR: 0.67 (95% CI 0.32 to 1.41)) or ICS (adjusted HR: 0.48 (95% CI 0.77 to 3.41)) were not significantly associated with risk of SCD in subjects with airflow obstruction.
In the stratified analysis, as compared with those without airflow obstruction, the HRs of moderate to very severe airflow obstruction were 1.92 (95% CI 1.35 to 2.73) for white males, 4.97 (95% CI 2.92 to 8.45) for white females, 2.27 (95% CI 1.32 to 3.92) for black males and 1.52 (95% CI 0.76 to 3.05) for black females. On testing the associations of several definitions of respiratory disease with SCD, a self-reported physician diagnosis of emphysema or COPD had significant association with SCD in black males and white females but not among any other groups. However, self-reported physician diagnosis of bronchitis or asthma did not seem to be associated with risk of SCD in all groups (table 6).
Race-specific and gender-specific incidence rate and HR (95% CIs) of SCD for airflow obstruction*
Discussion
In this biracial, bigender community-based sample of 14 708 participants followed for approximately 25 years, we observed an inverse association between baseline lung function and SCD, and a monotonic, direct association between impaired lung function or airflow obstruction and SCD across groups defined by race and gender, independent of established cardiovascular risk factors and systemic markers of inflammation. Of note, the associations persisted even after adjusting for smoking status and were observed in never smokers, suggesting the results are not primarily confounded by smoking status. Overall, the predictive model showed that addition of FEV1 or FVC significantly improved the predictive power for SCD.
We found two observational reports that also assessed the association of COPD with the risk of SCD in the general population.6 9 However, none of these studies evaluated the impact of impaired lung function quantitatively or conducted stratified analyses by race, gender and smoking status. In consistent with the findings from both the Rotterdam study and Oregon Sudden Unexpected Death Study, our results also indicate that COPD is an independent risk factor for SCD. However, our results add incremental values as compared with the previous reports. First, lung function measurements were performed in all participants at baseline in our study, which makes the diagnosis of airflow obstruction more accurate than previous studies that defined COPD based on medical records. In our study, 14.4% of the subjects with self-reported physician diagnosis of emphysema or COPD did not have airflow obstruction, while 60.0% of the subjects with self-reported physician diagnosis of bronchitis had airflow obstruction. This suggests defining airflow obstruction based on medical records might introduce recall bias or detection bias. We found only moderate to very severe airflow obstruction, rather than mild airflow obstruction conferred increased risk. Second, we extended the results to a biracial population and established its independence from smoking by analysing the never smokers separately. We also found an association of SCD with self-reported physician diagnosis of emphysema or COPD in black males and white females. Third, our study demonstrated that objective measures including FEV1, FVC, FEV1% predicted, FVC% predicted and FEV1/FVC ratio were all inversely associated with risk of SCD. Of note, the risk magnitude between reduced FEV1 and SCD seems to be greater after the exclusion of participants with prevalent airflow obstruction. These indicate that population without COPD or airflow obstruction but with impaired lung function were also at high risk of SCD. Fourth, although bronchodilators such as xanthines, beta-agonists or anticholinergics are potentially arrhythmogenic, while ICS might have a protective role on cardiovascular events in COPD patients, we found their use was not associated with risk of SCD and their adjustment did not appreciably alter the putative relationship.
The underlying mechanisms involved in the association between impaired lung function and SCD remain uncertain, but several plausible explanations have been suggested. First, impaired lung function could cause cardiac autonomic dysfunction that might ultimately translate into SCD.29–31 Our results suggest that reduced FEV1 level was associated with prolongation of the QTc interval, which represents the duration of ventricular repolarisation and a well-established ECG-derived risk indicator for SCD. In addition, impaired lung function is associated with increased resting heart rate in our study. Tachycardia could result in increased myocardial oxygen demand, a situation that may lead to myocardial ischaemia and potentially dysrhythmic consequences.32 Other studies also demonstrated that impaired lung function could also cause abnormalities of baroreceptor sensitivity, heart rate variability and muscle sympathetic nerve activity, which were indicators of increased sympathetic tone or reduced vagal tone.33
Second, an increased risk of SCD in individuals with impaired lung function may also be explained by systemic hypoxaemia.34 The prolonged oxygen desaturations could trigger ventricular ectopy by deterioration of gas composition and pulmonary hypertension, leading to elevation of ventricular pressure and change of the electrophysiological properties of ventricular tissues, which in turn trigger SCD.35 Individuals with impaired lung function also have an increase in coagulability. Platelet activation and aggregation are increased, fibrinogen levels are increased and fibrinolytic activity is decreased due to hypoxaemia and hypercapnia.32 In consistent with this, our data demonstrated that concentrations of fibrinogen and von Willebrand’s factor were inversely proportional to the baseline lung function.
Third, chronic systemic inflammation and endothelial dysfunction could provide other mechanisms through which SCD is caused. Both our data and previous evidence suggest that those with low lung volumes seem to have higher levels of systemic markers of inflammation.36 Wedzicha and Seemungal37 also reported that systemic inflammation during COPD exacerbations may lead to increase of cardiac death which is collaborated by other evidence that concentrations of non-specific markers of inflammation such as C reactive protein and interleukin-6 were increased following COPD exacerbations.38 C reactive protein is strongly linked to increased cardiovascular risk in general, and SCD and impaired lung function specifically.39
Our study has several strengths and some limitations. First, we have included a large sample size and diverse population, which enabled the estimation of precise incidence rates, stratification by race, gender and smoking status, and a comprehensive assessment of potential confounders. Second, SCD was validated by physicians blinded to the lung function of the subject. Third, the data on SCD events and covariates were prospectively gathered, reducing the risk of potential recall bias. A first limitation is that unmeasured and residual confounding of the relationship between lung function and SCD could not be completely addressed by multivariate modelling, owing to the observational nature of the study. Second, ARIC study included only middle-aged adults of white or black race; therefore, these findings may not apply to younger adults or other races. Third, autopsies and electrocardiography were rarely performed at the time of death, limiting the assessment of exact causes of death. Nevertheless, The SCD events were rigorously adjudicated using multiple sources of information, which might provide a more accurate diagnosis of SCD than is often available in epidemiological studies. Fourth, as noted, FEV1 and FVC were not measured postbronchodilation, which is critical in cases of COPD. In addition, bronchodilator reversibility testing and other tests, which are warranted to confirm the diagnosis of asthma, were not performed. These precluded further subgroup analyses according to the precise diagnosis of COPD and asthma.40 Instead, we used self-reported history of asthma and COPD when possible. Fifth, limited data available may preclude exploring in depth the role of other variables, such as disease control, access to adequate pharmacotherapy and socioeconomic status that may also influence the risk of SCD. For example, ICS might theoretically have a protective role on cardiovascular events in patients with COPD. However, given the smaller number of subjects taking ICS in our study, we only found a non-significant reduction of SCD risk associated with ICS.
In summary, reduced lung function was independently associated with an increased risk of SCD in the general population. These findings were consistent in race and gender-based subgroups and persisted after controlling for traditional cardiovascular risk factors. These findings should encourage ongoing research of the mechanisms of SCD in individuals with impaired lung function, as well as the development of clinical trials of lung function improvement for prevention of SCD.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the institutional review board at all participating institutions, and all participants provided written informed consent at enrolment.
Acknowledgments
The authors would like to thank the staff and participants of the Atherosclerosis Risk in Communities (ARIC) study and Biologic Specimen and Data Repository Information Coordinating Center for their important contributions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Y-JC, Z-GC and F-JY contributed equally.
Contributors S-HW and Y-JC conceived the overall idea and all authors designed the study. F-JY performed the statistical analyses, and Z-GC and Y-JC wrote the first draft of the manuscript. All revised the manuscript critically. All have given their final approval of the version to be published.
Funding The ARIC study is carried out as a collaborative study supported by National Heart, Lung, and Blood Institute contracts. The study was also financially supported by the grants from National Natural Science Foundation of China (81600260, 81370285 and 81970206), Guangdong Natural Science Foundation (2016A030313210 and 2019A1515010269), Guangzhou City Science and Technology key Programme (201508020057), Guangdong Basic and Applied Basic Research Foundation (2021A1515010405), the project of Guangdong Province Science and Technology Plan (2017A020215174), the Fundamental Research Funds for the Central Universities in Sun Yat-Sen University (18ykpy08), the project of Kelin new star of the First Affiliated Hospital of Sun Yat-Sen University (Y50186) and the clinical research plan of the Eastern Hospital of the First Affiliated Hospital of Sun Yat-Sen University (2019007).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.