
Abstract
A growing preclinical and clinical body of work on the effects of chronic drug use and drug addiction has extended the scope of inquiry from the putative reward-related subcortical mechanisms to higher-order executive functions as regulated by the prefrontal cortex. Here we review the neuroimaging evidence in humans and non-human primates to demonstrate the involvement of the prefrontal cortex in emotional, cognitive, and behavioral alterations in drug addiction, with particular attention to the impaired response inhibition and salience attribution (iRISA) framework. In support of iRISA, functional and structural neuroimaging studies document a role for the prefrontal cortex in assigning excessive salience to drug over non-drug-related processes with concomitant lapses in self-control, and deficits in reward-related decision-making and insight into illness. Importantly, converging insights from human and non-human primate studies suggest a causal relationship between drug addiction and prefrontal insult, indicating that chronic drug use causes the prefrontal cortex damage that underlies iRISA while changes with abstinence and recovery with treatment suggest plasticity of these same brain regions and functions. We further dissect the overlapping and distinct characteristics of drug classes, potential biomarkers that inform vulnerability and resilience, and advancements in cutting-edge psychological and neuromodulatory treatment strategies, providing a comprehensive landscape of the human and non-human primate drug addiction literature as it relates to the prefrontal cortex.
Similar content being viewed by others


Introduction
The fundamentals
Drug addiction is a debilitating and chronic disease characterized by a relapsing cycle of intoxication, bingeing, withdrawal, and craving. Unlike casual use or dependence (e.g., chronic use to sustain or normalize function), drug addiction reflects a persistent cycle of drug seeking and taking that prevails despite diminished pleasure from taking the drug, as well as grave consequences on well-being and quality of life [1]. Because drugs of abuse act on the brain’s dopaminergic system, much of the focus in early drug addiction research has sought to investigate drugs’ rewarding effects via the limbic systems. Evident has been a specific focus on the mesencephalic sources of dopamine release to rewarding stimuli (e.g., ventral tegmental area and substantia nigra in the midbrain [2]), and their dopaminergic targets in the basal ganglia that are primarily associated with reward processing (e.g., nucleus accumbens [3, 4]), and action policies that are informed by reward (e.g., regulation of goal-directed and habitual behaviors) in the dorsal striatum [5, 6].
Although crucial in describing the reward-related properties of drug addiction, the mesencephalic and striatal focus overlooks the devastating effects that drugs of abuse have on the prefrontal cortex (PFC) with important implications to select emotional and cognitive functions [7]. The PFC is a cortically and subcortically interconnected region of the brain that orchestrates several higher-order executive functions. Via amygdala and striatal connections, the ventromedial PFC and orbitofrontal cortex (vmPFC/OFC; and their equivalently named regions in non-human primates) coordinate reward-related decision-making, value tracking, goal-directed control, and inhibitory control [8,9,10,11]. Specifically, the OFC regulates reward and punishment related behaviors [12], potentially by representing the value of motivationally salient outcomes [13], while human lesion studies highlight the role of the vmPFC in making advantageous [14] and goal-directed decisions (where impairment can manifest, for example, in selecting cue-triggered habitual behaviors despite unfavorable consequences) [15]. Via connections to the subthalamic nucleus and frontal motor areas, the ventrolateral PFC (vlPFC)/inferior frontal gyrus (IFG; homologous to areas 44 and 45 in non-human primates [16], although the term IFG is essentially never used in the non-human primate literature) regulates response selection and inhibition [17, 18]. Via anterior cingular and limbic connections, the dorsolateral PFC (dlPFC; homologous to areas 9 and 46 along the principal sulcus in non-human primates [19]) is involved in attention allocation, working memory, and emotional regulation [20,21,22], while via limbic and dorsal/lateral prefrontal connections, the anterior cingulate cortex (ACC; homologous to areas 24, 25, and 32 in non-human primates [23]) processes error monitoring, reward-based decisions, and emotions and their regulation [24,25,26]. A representative framework that targets these emotional, cognitive and behavioral roles of the PFC in drug addiction is the impaired Response Inhibition and Salience Attribution (iRISA) model [27, 28]. This framework posits that abnormalities in these PFC subregions underlie the core symptoms of drug addiction that manifest as hypersensitivity to drug-related cues at the expense of non-drug-related cues and reinforcers, with a concomitant impairment in the ability to suppress disadvantageous behaviors [29] (see Fig. 1 for an illustration of the affected brain networks). In this review, we will dissect the neuroimaging literature that identifies and highlights the emotional, cognitive, and behavioral bases of drug addiction, as informed by pertinent clinical and preclinical (focusing on the non-human primate) findings, specifically targeting the role of the PFC in iRISA in this disorder. We will describe alterations in PFC structure and function, their neuropsychological and behavioral manifestations, potential biomarkers that inform vulnerability and proclivity, as well as advancements in cutting-edge drug addiction treatment avenues, such as perturbations of brain structure and function. A goal of this review is to inspect the evidence that could contribute to assigning a causal role for drug use in the PFC dysfunction in iRISA in addiction. We therefore review well-controlled evidence from non-human primates, where chronic drug exposure can be studied with random group assignment and longitudinal precision (e.g., before and after exposure), in addition to longitudinal and interventional studies in humans. Specifically, we will discuss the elusive “chicken-or-egg” question in drug addiction: is the prefrontal insult observed in addicted individuals a pre-existing risk factor that accelerates drug addiction, and/or is it a direct result of chronic drug use? The unique and overlapping characteristics of substance types (e.g., tobacco, alcohol, cannabis, stimulants, opiates) will also be reviewed, providing a comprehensive landscape of the current state of the human and non-human primate drug addiction neuroimaging literature as it relates to the PFC.

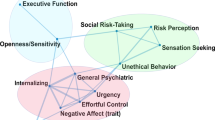
Drug addiction is associated with widespread aberrances in brain activity whereby increased task-dependent neural engagement is evident in relevant brain networks when addicted individuals are exposed to drug cues and contexts, while these same networks reflect blunted signaling during nondrug-related tasks. Adapted from Zilverstand et al. [29]. Copyright 2018 by Elsevier Inc. Adapted with permission.
To this end, we focused specifically on investigations of drug addiction (not casual drug use or sub-clinical presentations) primarily conducted using magnetic resonance imaging (MRI) that informed iRISA-related functions (e.g., reactivity to drug cues/drug-related biases in attention allocation, inhibitory control, reward-related decision-making, insight into illness) and their underpinnings (e.g., structural analyses examining PFC neuroanatomy). Because of the cytoarchitectural similarities in the PFC across humans and non-human primates [19, 30,31,32,33], we targeted studies in these species only. Because the drug addiction literature has been reviewed within the scope of the iRISA model in 2002 [27], 2011 [28], and 2018 [29], we aimed to emphasize the more recent contributions to the field herein.
Neuroanatomy
Structure: gray matter
Evidence for brain tissue differences between addicted and healthy individuals is plentiful. Although both cortical and subcortical alterations have been reported in addicted populations, the atrophy of the PFC gray matter is a reliable finding observed across substances, and most notably in the vmPFC/OFC [34,35,36]. A closer morphometric examination of drug-addicted populations yields a pattern of lower gray matter volume throughout the PFC and across several substances of abuse compared to non-addicted individuals. For instance, gray matter in the anterior PFC, dlPFC, ACC, IFG, inclusive of the vlPFC, in addition to vmPFC/OFC–regions associated with salience/value processing and/or cognitive/emotional control [13, 37,38,39,40]—is lower in tobacco [41,42,43,44], alcohol [45,46,47,48], stimulant [42, 49,50,51,52,53,54,55,56,57], and opioid use disorders [58,59,60,61,62,63,64] compared to non-addicted controls. Moreover, these PFC volume patterns show a cumulative effect for drug use, such that the longer the use, the lower the gray matter volume. Specifically, increased duration of tobacco use is associated with lower gray matter volume in the IFG [44], vlPFC [42], and the medial PFC [65]. A similar negative correlation is evident between years of use and the dlPFC in alcohol [46, 66], dlPFC, ACC, vlPFC, and vmPFC/OFC in stimulant [42, 49, 52, 54, 67], and dlPFC, IFG, and insular cortex volume in opioid use disorder [58, 60, 61, 64].
Some of these widespread patterns of lower gray matter volume in drug addiction may be reversible as suggested by cross-sectional studies reporting that the longer the abstinence, the higher the gray matter volume in nodes of the salience (e.g., ACC, insula) and the inhibitory control networks (e.g., dlPFC) [68]. Longitudinal studies examining neuroanatomical change following reduction or cessation of drug use have provided supportive evidence. For example, individuals abstaining from alcohol show increases in gray matter volume as early as 1 month after cessation, and continue to display increasing frontal gray matter volume that, by 7.5 months, meets average frontal volume in healthy controls—consistent with a recovery effect that was more pronounced in non-smoking alcohol abstainers [69]. These patterns extend to actively using cocaine-addicted individuals where decreases in cocaine use from baseline to follow-up (i.e., minimum of 6 months between time points, and at least 10% reduction in use) were associated with increased PFC (superior, middle, and inferior frontal gyri) thickness and better visual sustained attention [53]. Significant reductions/cessations in cocaine use over the same time period were also associated with enhanced reward-related decision-making in a gambling task, with parallel increases in IFG and vmPFC volume [70].
Importantly, frontal cortical structure may be a crucial predictor of sustained abstinence as suggested by significantly smaller baseline frontal gray matter volume in those who eventually relapse compared to those who continue to abstain (despite similar rates of frontal gray matter recovery over the course of abstinence) [71]. Taken together with the evidence that smaller medial frontal volume predicts earlier alcohol relapse following treatment, lower frontal gray matter volume may be an endophenotype of treatment resistance in drug addiction [72]. It may even predate the onset of addiction, predisposing individuals to early experimentation with drugs and then to the transition from occasional drug use to habitual use and finally to addiction. For instance, a study of 50 stimulant-addicted individuals and their biological siblings reported that compared to the latter, the former group displayed smaller prefrontal volume, especially in the OFC (which negatively correlated with duration of drug exposure) [35, 73]. More direct evidence is provided by a study reporting that prenatal exposure to nicotine increased the likelihood of using drugs in adolescence and that cortical OFC thickness in the prenatally exposed individuals negatively correlated with number of substances tried [74] (see [75] for similar patterns driven instead by prenatal alcohol exposure). Interestingly, individuals who were casual drug users, i.e., those who did not develop compulsive drug-use behaviors that characterize addiction, exhibited increased gray matter volume in the ACC and OFC compared to addicted individuals as well as healthy controls, suggesting that prefrontal tissue integrity may also be a marker for addiction resilience [35, 76].
Critical elements missing in the clinical studies reviewed above are true baseline measures of structure and cognitive performance prior to drug exposure, rendering the experimental control possible in longitudinal preclinical studies uniquely informative. Within-subject designs offer greater sensitivity to detect small but systematic changes within a relatively small number of subjects [see [77] for detailed discussions of sample sizes and power for longitudinal nonhuman primate imaging studies]. Using this design and to examine the structural consequences of chronic ethanol consumption, one study in rhesus macaques examined the impact of extended, voluntary ethanol consumption on volume measures of gray matter across a range of atlas-defined regions of interest [78]. A control group was not included, but individual differences in consumption were leveraged to divide the 18 animals into heavy (> 3 g/drink/day) and non-heavy drinkers. Across global cerebral cortical gray matter, significant reductions in average volume were observed following 6 and 12 months of 22 h open access to ethanol for the heavy, but not non-heavy, drinkers. Follow up correlational analyses did not show significant correlations between ethanol consumption (percent change from baseline and cumulative consumption) and the frontal (or sensory/motor) cortex (at either time point). Instead, the allocortex (hippocampus and olfactory areas), temporal, parietal, and occipital cortex showed decreases that were significantly correlated with consumption at the 6 month time point, but by the 12 month time point only changes in the allocortex were significantly correlated with consumption, potentially suggesting a unique impact of the more extended use on neurogenesis.
Including a contemporaneous control group permitting a 2 × 2 design is the best approach for longitudinal studies evaluating drug effects while controlling for the passage of time. This approach was utilized to evaluate the effects of chronic cocaine self-administration (one year, four times per week) on gray matter density (GMD) in non-human primates [79]. Similarly to findings from cross-sectional studies in human stimulant users, declines in GMD in the cocaine-exposed monkeys (relative to controls) were observed in the OFC and the insula (as well as temporal cortices, the amygdala and thalamus). Interestingly, impairments in reversal learning significantly correlated with decreased GMD in the OFC (and lateral parietal cortex) while visual working memory impairments correlated with decreased GMD in the insula (and the temporal lobe), suggesting that the structural changes observed contributed to the cognitive impairments. Importantly, by eliminating any confound of preexisting differences, these results establish causality for cocaine self-administration on generating changes in brain structure and associated cognitive functions. Crucially, in a subset of the original cohort scans were also acquired following an abstinence period of two years. As a general pattern across the whole brain, many regions that had shown decreases in GMD with 1-year of cocaine self-administration now showed clusters of increased GMD (relative to the scans obtained after self-administration). However, GMD in the insula, amygdala, and left OFC in the cocaine group, relative to the controls, did not show significant reversal with abstinence of the structural cocaine-induced impairments, suggesting a mechanism that may contribute to the risk of relapse. Taken together, longitudinal non-human primate and human studies suggest that drug addiction causes PFC damage, as evidenced by decreases in gray matter following extended drug use (see Fig. 2, panels 1–3). Importantly and in support of this causal relationship, in most regions these patterns are reversible, in that the absence of drug use results in the recovery of gray matter (see Fig. 2, panel 4 for a representation of PFC recovery).

Panel 1 depicts an at-risk PFC (saturated shading, reflecting predisposition from genetic factors, prenatal drug exposure, and early-life stress such as neglect) compared to an intact PFC (no shading). Following exposure to drugs in adolescence/adulthood in panel 2, problematic drug use (represented by distance from onset of drug exposure) and the consequential PFC impact (represented by increasing PFC saturation) are accelerated in the at-risk brain. In comparison, although also impacted by drug exposure, the intact PFC may progress more slowly towards addiction. In panel 3, chronic drug use and addiction cause further significant PFC damage (red shading) in both cases, engendering a persistent cycle of craving, intoxication, bingeing, and withdrawal. Panel 4 represents the amelioration of the addiction-induced PFC damage with substantial reduction in drug use (depicted by a less saturated shading of the PFC than the addicted state, but a more saturated shading than the pre-drug exposure state). Whether premorbid risk factors also affect speed and/or extent of recovery (e.g., is the emergence or trajectory of recovery delayed or is less consistent in those with early life PFC risk factors?) remains an open question.
Structure: white matter
Drugs of abuse are neurotoxic agents with the potential to induce neuroinflammation, to which white matter connectivity is especially vulnerable [80, 81]. In humans, diffusion-weighted MRI has been primarily used to assess white matter microstructure. Fractional anisotropy (FA) reflects the coherence of water molecule diffusion along a specific orientation in white matter pathways. A low FA value represents less coherence in the main directionality of diffusion, associated with demyelination and decreased axonal integrity [82]. Mean diffusivity (MD) represents the non-directional, overall diffusivity within a given voxel, with abnormally high MD values typically suggesting structural disorganization, potentially stemming from edema [83]. Radial diffusivity (RD) quantifies the diffusion of water molecules in a direction that is perpendicular to the axon fibers, with increased RD indicating greater myelin damage [84]. Axial diffusivity (AD) reflects water molecule diffusivity that is parallel to the axonal fiber, with altered AD suggesting structural damage to the axon itself [85,86,87].
Drug-addicted individuals exhibit lower FA in numerous major white matter tracts including the corpus callosum when compared to non-addicted individuals, a consistent finding across different substance types [88]. For example, tobacco addiction is associated with lower FA in the anterior corpus callosum [89], but also in the anterior cingulum white matter [90] and pathways projecting from the nucleus accumbens, habenula, and the motor cortex to the PFC [91]—connectivity shared by functional networks implicated in exerting control over reward-driven behaviors [6]. Alcohol use is similarly associated with lower FA in widespread fronto-cingular pathways [92, 93], and in chronic cannabis use, frontal and frontotemporal pathways also evidence lower FA [94, 95]—notably those connecting to the OFC (e.g., forceps minor) [96]. Cocaine-addicted individuals have lower FA in the genu of the corpus callosum as documented by a recent meta-analysis of eight tract-based reports [97]. Current cocaine users also show deficient FA in the dlPFC, ACC, vmPFC, and OFC compared to controls [98,99,100]. Chronic methamphetamine users exhibit higher MD in the frontal (genu) of the corpus callosum as well as the frontal cingulum, where RD is also higher, suggesting edema and demyelination in these frontal white matter pathways [101]. Opiate addiction is associated with lower frontal FA [102,103,104,105,106,107] and higher RD [108] and AD [102], suggesting heroin’s destructive effects on myelin and axonal integrity, respectively. White matter microstructure abnormalities are exacerbated by duration of use (and often attenuated as a function of abstinence duration) in the IFG in alcohol [92], vmPFC/OFC and the tapetum (a fan-like radiation extending from the splenial corpus callosum, known to serve as a nexus for bilateral hippocampal connectivity) in cocaine [98, 100], and in widespread frontal pathways in heroin addiction [102, 103, 106]. In sum, the neural signature of drug addiction includes substantial microstructural damage that is potentially driven by demyelination, axonal damage, and edema in regions that regulate learning, memory, cognitive control, and optimal reward-driven behaviors [100].
In nonhuman primates, there is one report of decreased measures of myelin proteins following an extended period of chronic cocaine self-administration [109]. Specifically, levels of proteolipid and myelin basic protein (measured by western blot analysis) were reduced in regions of white matter bundles at the level of the precommissural striatum after 300 sessions (0.3 mg/kg/injection, 30 reinforcers per session, 2750 mg/kg total intake). Although significant effects were not seen in the PFC, combined with additional studies from the same lab, these observations suggest potential mechanisms for effects that may be relevant to those observed clinically in prefrontal regions. In those additional studies, a post-mortem measure of microglial activation (binding to the TSPO 18 kDA translocator protein determined with [3H]PK11195 by quantitative in vitro receptor autoradiography) was increased in 8 out of 11 white matter tracts at the level of the striatum inclusive of the cingulum bundle, the uncinate fasciculus, the superior longitudinal fasciculus, and fronto-occipital fasciculus, which could reflect altered axonal tracts from the PFC [110].
Function
The widespread neuroanatomical abnormalities in drug-addicted individuals are paralleled by alterations in brain function and concomitant behavioral impairments. When faced with drug cues, addicted individuals exhibit heightened activation in a wide-range of brain networks that regulate executive control and salience processing including reward-related decision-making, among other functions. Importantly, in the absence of drug cues, these same regions largely display hypoactivations, such that these brain networks are selectively recruited in the context of drug cue exposure [27, 29] (see Fig. 1).
Inhibitory control
Nodes of the cognitive control/executive function networks that comprise the dlPFC, ACC, and IFG [39, 111,112,113] serve as candidate regions in explaining inhibitory control impairments in various substance use disorders [28, 29]. Traditional and modified versions of classical tasks, such as the Go/No-Go [114], Stop-Signal [115], and Stroop tasks [116] have been integral in modeling inhibitory control-related performance and neural signaling in addiction. Using these inhibitory control tasks, lower activations have been reported in the dlPFC, ACC, and IFG in nicotine [117], dlPFC and ACC in cannabis [118, 119], dlPFC and IFG in alcohol [120], dlPFC, ACC, and IFG in cocaine [121,122,123,124] (which were further exacerbated by increases in task demand [125]), and ACC in heroin-addicted individuals [126, 127] compared to controls. Although some discordance in the literature exists (e.g., [128, 129]), it may be attributable to variability in task structure and analysis methods [130]. Aberrant prefrontal signaling during inhibitory control in drug-addicted individuals may underlie a vulnerability to lapses in self-control, especially when demand for inhibitory control is high, such as in the face of drug cue exposure or while craving.
There is a substantial non-human primate literature reporting links between cocaine exposure and impairments in inhibitory control. One study examined the effects of investigator administered cocaine on stimulus discrimination and reversal in vervet monkeys [131]. Consistent with an impact on OFC function [132], a specific impact only on reversal performance was observed. The effects of self-administered cocaine exposure using rhesus macaques have also been evaluated [133], showing similar results. A group (experimental vs. control) by time (pre- vs. post-cocaine) interaction showed cocaine-induced impairments in reversal performance and visual working memory (but not stimulus discrimination). Further, in a cross-sectional comparison of cognition between cocaine self-administering macaques and experimentally naive age-matched controls, the former (but not latter) group showed worse performance on multidimensional discriminations and reversal learning (but no impairments in simple discrimination) [134]. Taken together, the work from three separate groups shows striking concordance in demonstrating that repeated cocaine exposure leaves associative learning intact but produces impairments in inhibitory control.
Attention bias and cue reactivity
The pronounced drug- and drug cue-associated attentional allocation (i.e., attention bias), arousal inclusive of psychophysiological responses (i.e., cue-reactivity), and craving point to an underlying vulnerability in the way drug cues are perceived by addicted individuals [135, 136] suggesting a disproportionate amplification of drug valuation/salience that may motivate drug seeking. Attention bias towards drugs is especially evident before and during drug cue encounters and self-reported temptations, suggesting that a disruption in optimal attentional allocation may give rise to the pursuit of drugs [137]. This phenomenon of drug-dominant attention bias has been studied using modifications of classical neuropsychological tasks such as the color-word Stroop task. In this traditional task, individuals are presented with names of colors typed in congruent (same color ink) or incongruent (different color ink) colors and interference is measured as the latency caused by a conflict between the need to suppress the prepotent and fast (but task irrelevant) response of reading the word to instead respond with the slower naming of the incongruent color of the word ink [116]. In the modified version, the stimuli are altered to include drug and non-drug-related words (or other stimuli such as pictures). The attentional interference effect is tested via the latency (and/or accuracy) to respond to the drug (salient hence potentially interfering with the task at hand for the addicted individuals) as compared to non-drug (e.g., neutral) cues [138]. When behavior in cocaine-addicted individuals was matched to that of healthy controls, performance on a drug-word modified Stroop task was associated with enhanced midbrain activations to drug (as compared to neutral) words only in the addicted group, indicating that drug words may serve as motivationally salient/conditioned drug cues that potentially activate the mesencephalic dopaminergic system in human addiction [139] (although it should be noted that this fMRI BOLD study did not directly measure dopaminergic neurotransmission). The ACC recruitment during exposure to these drug words positively correlated with cocaine craving, such that the higher the craving, the higher the drug-related ACC activations (while frequency of use negatively correlated with non-drug-related ACC activation, such that the more frequent the use, the less the ACC activation to the non-drug stimuli) [140]. Thus, severity of illness may exacerbate drug cue reactivity (at the expense of non-drug cue reactivity) markers in the PFC as further supported by the effect of withdrawal symptoms on ACC hyperactivation to drug cues in cocaine users (comparing those with versus without withdrawal symptoms and healthy controls) [141]. Similar results were reported in smokers who displayed ACC hyperactivations during a line-counting task with smoking cues [142] (but see [143] for negative results) and alcohol-addicted individuals who exhibited enhanced activity in cortico-striatal regions during a visual dot probe task with alcohol images compared to neutral images [144] and higher activations in the dlPFC, vmPFC, and insula during a Go-NoGo task with alcohol compared to non-alcohol cues [145, 146]). In these studies in smokers and alcohol-addicted individuals, and in another study using a working memory load task with drug cues in cocaine-addicted individuals, higher IFG signaling correlated with less attention bias to the drug cues [147], supporting this region’s role in the suppression of cue-reactivity. Importantly, pronounced drug cue-reactivity/attentional-bias related activity in the ACC predict higher rates of drug (nicotine or cocaine) relapse following treatment—a pattern potentially marking a vulnerability for relapse in those who are unable to effectively allocate neurocognitive resources in the face of (and away from) drug cues [148,149,150].
Measuring response inhibition during exposure to salient drug reinforcers is crucial for modeling an ecologically relevant representation of the drug addiction experience—a core tenet of the iRISA framework. However, studies that directly examine the potential interaction between cue reactivity/drug salience and inhibitory control are rare [143]. In some studies, drug cue salience is conflated with response inhibition [145, 146], and in other studies the inhibitory component is absent (e.g., line-counting or dot probe tasks [142, 144]), or not directly captured while under cue reactivity (e.g., modified Stroop tasks [138]). To better understand the interaction of drug cue reactivity and response inhibition, we developed a novel emotional stop-signal task (a modification of the classic inhibitory control stop-signal task with neutral cues [115]). Here, drug and non-drug word cues prompted Go responses that required stopping when accompanied by a stop-signal, permitting a trial-by-trial modulation of drug cue-reactivity during inhibitory control. Preliminary results in cocaine-addicted individuals showed lower dlPFC activity during drug compared to non-drug reinforcers for stop success as compared to stop failure, the classical inhibitory control measure (unpublished data: Ceceli, Parvaz et al.). These deactivations are in line with dlPFC’s role in orchestrating craving-related processes whereby a drug cue context may require addicted individuals to dampen (suppress or inhibit) craving-related prefrontal signaling to meet inhibitory control demands [151, 152].
According to two preclinical studies, the OFC and ACC are both implicated in attention bias and drug cue reactivity but demonstrating separate roles. One study has explored single unit activity in the OFC and ACC in rhesus macaques during the presentation of a discriminative cue predicting cocaine availability and a discrete cue accompanying an 18 s cocaine infusion [153]. On this stimulus response task, longer response times in the presence of cocaine distractors, relative to trials in which the distractor was not associated with cocaine, indicated an attentional bias to the cocaine cues. Single unit activity was recorded during performance of this task in two animals and responses in the ACC and OFC were contrasted with activity in the dorsal and ventral striatum. Across an unbiased sample of neurons, and measuring the proportion of single units activated as well as differences in the mean population response, both the OFC and ACC (but not the striatal regions) differentiated the cocaine distractor condition. However, unlike the ACC, the OFC had a significantly greater response to the discriminative than the discrete cue. Instead, neurons in the ACC showed a prolonged engagement during the discrete cue presentation that accompanied the cocaine infusion. These direct measures of single unit activity in a primate model suggest that cortical mechanisms, especially in the OFC, are likely involved in attentional bias to cocaine associated environmental cues. The prolonged response of the ACC is instead consistent with its role in reward expectation and in guiding behavior for obtaining rewards. While this involvement of the ACC in response selection and evaluation of outcome has generally been established over short-term action outcome contingencies [154], uniquely in this report, the ACC engagement was maintained even when responses were no longer necessary (because the response contingency had been met). In sum, these results suggest that the OFC and ACC are involved in attentional bias and drug cue reactivity whereby the OFC signals drug-related attention bias (to drug availability), and the ACC sustains a response to cues associated with drug receipt.
Reward-related decision-making/choice, and insight into illness
The maladaptive engagement of brain networks that arbitrate an adaptive interaction with the environment may be a driving force in the debilitating cycle of disadvantageous behaviors and reward-related decision-making in drug addiction. In line with the suggested blunting of non-drug-related functions (and accompanying brain substrates) in drug addiction [27], addicted individuals consistently exhibit risky decisions [155,156,157] and impairments in maintaining optimal choices (that maximize monetary gain) [158]. For example, as measured by the Iowa Gambling Task [14], addicted individuals display deficits in sustaining advantageous decisions to yield net gains, with accompanying alterations in cortico-striatal function [159]. Notably, lower brain activity during and following reward-related decision-making is evident in the ACC in cannabis [158], dlPFC in alcohol [160], dlPFC, IFG, and striatum in stimulant [156, 161], and IFG in opiate use disorders [162] when compared to non-addicted controls. Reward-related decision-making difficulties in drug addiction may be the product of blunted prefrontal signaling during outcome anticipation or receipt [163,164,165], which may interfere with successful error monitoring [166] and updating of decision strategies [159].
In a preclinical study that explored the effects of cocaine on cognitive flexibility in decision-making tasks, rhesus macaques were trained on a dimensional set-shifting task similar to the Wisconsin Card Sort Task prior to any cocaine exposure [167]. Frequency of failures to follow the currently valid rule (the dimension, a stimulus attribute such as shape or color, which determined the correct response) negatively correlated with frequency of perseverative errors following a rule change. The failure to follow the rule was not attributed to distraction or memory lapse, instead indicative of an occasional deliberate violation of the correct rule in order to explore other contingencies. In support of this interpretation, learning was highest on sessions when exploration was highest, consistent with the idea that an underlying drive to learn, rather than disengagement from the task, was driving results. Following chronic cocaine exposure, these animals showed increased perseverative errors following a rule change and this inflexibility appeared to be driven by a decrease in exploratory rule breaking. Thus, compared to baseline and consistent with the other preclinical studies reviewed above indicating decreased inhibitory control, after cocaine exposure these animals followed a correct rule more rigidly, further showing impairments in their ability to shift to a new rule.
Despite the catastrophic health, interpersonal, and legal consequences that accompany drug addiction, an alarmingly high proportion of individuals with a persistent drug use disorder (~7 in 8) do not perceive a need for substance use related treatment [168]. In support, a recent large-scale analysis of a national survey with over 40,000 responses revealed that those abusing alcohol were less likely to report a need for treatment, and this effect was amplified for the recent users [169]. There undoubtedly exists a multitude of explanatory factors related to scarcity of treatment resources [170], cultural prejudice towards treatment need and efficacy, and societal stigma [171]; however, neurocognitive impairments related to reward-related decision-making, and the awareness of one’s illness severity and decisions (i.e., insight), may further contribute to the persistent and treatment-resistant nature of addiction. Chronic cannabis users display an impaired awareness of errors during a Go/NoGo task, paralleled by decreased activations in the ACC (when subjects were unaware of errors compared to when they were aware) [172]. Behaviorally, cocaine-addicted individuals also show poor awareness of errors and impairments in post-error adjustments in Go/NoGo tasks [173]. In a decision-making task where participants were instructed to make choices to expand side-by-side-presented drug, pleasant, unpleasant, and neutral images, cocaine-addicted individuals showed a discordance between actual choice and their self-reported pleasantness ratings, such that despite rating pleasant images more favorably than drug images, compared to healthy controls they more frequently selected to visually expand the drug images over the course of the task [174], alluding to impaired insight into drug choice behaviors. In a more direct study of choice insight, cocaine-addicted individuals were categorized into intact and impaired insight groups based on the agreement between their objective preferences for viewing drug, pleasant, unpleasant, and neutral images, and their subjective report of which of these categories they thought they most frequently selected. Compared to intact-insight and control groups, those with discordant responses between actual and perceived choice (i.e., impaired insight) displayed dysfunctional error-related rostral ACC activity during an inhibitory control task (the classical Stroop task) and lower volume in this region [175]. Impaired insight was further associated with more frequent recent cocaine use [176]. In actively using cocaine-addicted individuals (i.e., assayed via cocaine-positive urine test) compared to those addicted but without recent use and healthy controls, these impairments were also evident using a metacognitive (non-drug related) accuracy task (i.e., measuring disagreement between objective visuo-perceptual dot-counting task performance and self-reported confidence in task performance [177]); the lower the metacognitive accuracy across all subjects (but driven primarily by the active users), the lower the gray matter volume in the rostral ACC [178]. This and similar tasks could be used translationally to assess parallel functions, as previously accomplished for outcome expectations, their impairment by cocaine self-administration and restoration when the mPFC/OFC were optogenetically stimulated [179]. Overall, this line of research suggests that insight-oriented treatment strategies could offer a promising avenue in tackling problematic drug use [180, 181], especially in those who exhibit these awareness deficits.
Variability across drugs (in structure/function of the PFC)
Discrepancies in behavioral and neurobiological effects of different drug types may have important treatment implications; however, to the best of our knowledge, research directly comparing neurobehavioral substrates between drug classes in non-human primates is lacking, and in humans it is sparse [182]. In recent studies in humans, gray matter volume has been contrasted between polysubstance users (encompassing cigarette, alcohol, cannabis, and cocaine); while the medial PFC volume was lower in all substance users compared to non-users, lower vlPFC volume has been specifically related to cocaine use [42]. A recent mega-analysis has teased apart substance-specific gray matter patterns and found that in addition to a substance-general effect of lower medial OFC and insula (among other non-PFC regions) volume, distinct effects of lower volume were evident in widespread PFC regions (encompassing the dlPFC, ACC, and vmPFC/OFC) in alcohol use disorder, but no specific effects in any PFC region were noted for tobacco, cannabis, cocaine, or methamphetamine users [34]. A similar effort applied to studying white matter microstructure revealed substance-specific lower frontal FA in the sagittal stratum (a bundle of white matter fibers that includes connections from the cingulate to thalamic and brain stem structures [183]) in cocaine and the genu of the corpus callosum and cingulum in methamphetamine users (unpublished data: Ottino-González et al.). Comparing stimulant and opiate-addicted individuals, commonalities were reported for frontal white matter hyperintensities (i.e., increased brightness in T2-weighted MRI potentially indicative of pathologies such as ischemia, demyelination, and vascular damage [184]), while effects in the insula were more pronounced in cocaine compared to opiate addiction [185]. Such white matter damage is potentially related to cocaine’s vasoconstrictive effects [186], to which the insula may be especially vulnerable [187]. Indeed, cocaine-addicted individuals display pronounced carotid arterial wall thickness compared to healthy controls and even those at high cardiovascular risk, and such markers for atherosclerotic insult are driven by addiction severity [188], which, taken together with the evidence above, illustrate cocaine’s widespread (neurobiological and cardiovascular) inflammatory burden.
Direct comparisons between drug classes in search of distinct brain function impairments are similarly rare. In one example, stimulant- (compared to opiate) addicted individuals made more sub-optimal decisions on the Cambridge Risk Task—a reward-based decision-making task where participants were instructed to make binary choices based on visual markers of reward probability and placed bets on the outcomes. A similar decision-making impairment was evident in patients with focal OFC (but not other PFC) lesions and in healthy controls who were experimentally depleted from serotonin (by using the serotonin precursor tryptophan) [189]. However, in another study using this task, abstinent stimulant- and opiate-addicted individuals displayed comparable reward-related decision-making and associated brain activity when directly compared (although whether these similarities are due to the cessation of drug use is an open question) [190]. An interesting comparison of the impact of different classes of drugs on uniquely modulating brain function derives from within-subject analyses, where the different drugs may show different effects in the same drug-addicted individuals. For example, those who co-abuse cocaine and heroin exhibited place-preference differences, such that they preferred to consume heroin at home and cocaine outside the home [191]. Interestingly, contextual preferences modulated brain activity when subjects imagined using drugs in these settings, in that activity in the lateral PFC and caudate increased when these individuals imagined using cocaine at home and heroin outside the home (non-preferred) compared to imagining using cocaine outside and heroin at home (preferred). This double dissociation is potentially attributable to the cognitive demand associated with the mismatch between drug use and its preferred context—a finding that is important for characterizing cue-reactivity (and other cognitive functions) between drug classes [191], further highlighting the need for substance-specific neurobiological investigations and potentially treatment applications.
Modulation and treatment
Drug addiction has largely been tackled via cognitive-behavioral, motivational, pharmacological, and neuromodulatory therapies. In cognitive-behavioral methods, the focus is on developing mechanisms that can serve to cope with symptoms such as craving. Common strategies include incentive-based behavioral adjustments (contingency management), behavioral planning for coping with high-risk scenarios (relapse prevention), and recruiting cognitive control to highlight positive aspects of abstinence and detrimental outcomes of drug use [192,193,194]. The neural investigations of these strategies for addiction have suggested a mechanism that acts on normalizing inhibitory control (via the PFC but also the subthalamic nucleus [195]) and reducing reward processing (via the ventral tegmental area of the mesencephalon [196]). For example, cigarette smokers who contemplate the consequences of use while viewing smoking cues successfully suppress craving while enhancing PFC function and decreasing striatal and ventral tegmental signaling [197]. Similarly, smokers who reinterpret drug cues to reappraise cue-induced emotional reactivity exhibit dampened craving and increased dorsal ACC activation [198]. When reinterpreting drug cues (compared to non-reinterpreted trials), alcohol-addicted individuals display relatively higher dlPFC and vlPFC and lower ventral striatal activity [199]. Cocaine-addicted individuals show decreased attention bias (measured via spontaneous gaze duration to drug over nondrug cues) following a brief, in-lab, drug cue reappraisal training, as attributed to the dlPFC in this psychophysiological study [200]. Cocaine-addicted individuals also exhibit decreases in color-word Stroop-related ACC activity following several weeks of cognitive-behavioral therapy, with and without performance improvements [201, 202], which suggests enhanced efficiency in managing the conflict demands of the task [38, 203]. These therapy-related deactivations in the ACC have also been shown to correlate with decreases in cocaine use over the course of treatment [204].
Motivational interventions have been developed to enhance the motivation to change one’s own behaviors towards treatment goals that include abstinence promotion. Relevant neuroimaging studies have capitalized on public service announcement-formatted generalized statements (originally geared towards changing large-scale public behavior) to study neural responses to potentially motivating advertisements (as well as those more personally tailored to the individual). The dorsomedial PFC (dmPFC), a node of the self-referential network that also has a role in self-awareness in addiction [205], has been primarily implicated in processing such motivation-geared manipulations to minimize subsequent drug use, with accompanying increases in the dlPFC and IFG in smokers [206,207,208,209]. It is possible that motivational interventions improve clinical outcomes by strengthening the self-relevance of treatment goals, amplifying the individual’s ability to recruit inhibitory functions (as opposed to a mechanism that relies on reward sensitivity). These findings also suggest that treatment efficacy may be maximized via the use of highly salient and self-relevant tools. However, empirical assessments of the underlying brain substrates have to date primarily been conducted in nicotine and alcohol-using populations [194], and neurobiological support for the generalizability and sustained efficacy of motivational interventions is yet to be consistently explored.
Mindfulness training provides a structured regimen whereby individuals are trained to non-judgmentally monitor, acknowledge, and accept feelings, perceptions, and thoughts as they occur, often while the individual is focused on breathing or bodily sensations [210]. In the context of addiction, the premise of these practices is to augment one’s capacity to modify emotional reactivity and exert awareness and/or control over automatic processes (i.e., reduce drug craving and enhance savoring of alternative reinforcers) [211]. Mindfulness-based interventions have been suggested to deploy cortico-striatal connectivity. For example, preliminary fMRI evidence suggests that following 8 weeks of mindfulness-based treatment, smokers exhibited lower ACC and ventral striatal signaling during exposure to cigarette compared to neutral cues, and, using a separate task, they also showed increased activation in these same regions in response to pleasant non-drug pictures [212]. In-lab mindful attention towards drug cues in smokers has similarly shown to decrease rostral ACC activation and its functional coupling with the ventral striatum [213].
Pharmacological interventions are aimed to neurochemically compete with the direct effects of drugs of abuse to ameliorate the compromised functions that are associated with drug addiction (e.g., impaired incentive salience and non-drug-related motivation) [214]. For instance, cigarette cessation treatments commonly employ varenicline, a partial nicotinic acetylcholine receptor agonist that alters the release of dopamine while also attenuating the pleasurable effects of smoking [215]. Smokers who were administered varenicline reported reduced craving, accompanied by lower OFC signaling during the passive viewing of smoking cues [216]. Bupropion increases extracellular dopamine by blocking its selective reuptake, and its regimented administration to smokers is similarly associated with decreased cigarette craving and cigarette cue-induced ACC activity [217, 218]. Similar mechanisms are utilized in tackling alcohol (via the selective GABA-B agonist baclofen or partial dopamine agonist aripiprazole), stimulant (via agonists modafinil and methylphenidate), and opiate addiction (via the agonist methadone and antagonist naltrexone) [219,220,221,222,223]. Baclofen is associated with lower OFC and ventral tegmental signaling during alcohol cue-exposure in alcohol-addicted individuals [222] (but see mixed results in the directionality of effects on the dlPFC and ACC [224, 225]; for potential use in cocaine addiction treatment, see review in [226]). Similarly, compared to placebo administration, aripiprazole significantly decreased ventral striatal signaling during cue reactivity in alcohol-addicted individuals [223]. The opposite direction of results has also been reported; the combination of aripiprazole and the selective serotonin reuptake inhibitor escitalopram in individuals with alcohol use disorder (with co-morbid major depressive disorder) hyperactivated the ACC during alcohol cue-exposure [227]. However, it also reduced craving, alluding to a potential recovery of prefrontal function following a dopaminergic and serotonergic intervention in this dual diagnosis sample [227] (see [228] for an alcohol use disorder-focused review of pharmacology and fMRI evidence). The discrepancy from the commonly reported treatment-driven ACC deactivations may be attributed to the co-morbidity with major depressive disorder, characterized by dampened pre-treatment ACC signaling [229].
In a similar fashion, methylphenidate (which blocks dopamine transporters) shows promise as a normalizing agent for drug cue neural reactivity in cocaine use disorder. Oral methylphenidate has been associated with amplified ACC activity during the drug Stroop task described above [230], with results further suggesting the normalizing of a deficient midbrain signaling during mental fatigue on this task [231]. It also improves executive function on the color-word Stroop task, decreasing errors and enhancing more careful task performance (as evidenced by post-error slowing) [232]. Interestingly, across these studies, methylphenidate was shown to affect the prefrontal regions that orchestrate executive function (e.g., dlPFC) differently for cocaine-addicted individuals as compared to healthy controls, with activation patterns reflecting altered error-related dlPFC activity with methylphenidate uniquely in the cocaine-addicted individuals [232, 233]. Finally, in naltrexone-treated opiate-addicted individuals, decreased OFC (and striatal) activity during exposure to opiate images correlated with improved withdrawal symptoms [234], of importance to further explorations of this kind in heroin addiction.
The PFC has been a common target for neuromodulation to improve treatment outcomes in addiction (see Fig. 3 for a simplified illustration of the regional directionality of effects by which targeted interventions such as neuromodulation may facilitate PFC recovery). Among the most recently employed techniques are transcranial magnetic stimulation (TMS), transcranial direct current stimulation (tDCS), fMRI neurofeedback, and the more invasive deep brain stimulation (DBS) [235]. The premise behind these strategies is stimulating the brain circuits directly to reorganize and normalize their activity to improve behavior. The most common target region for transcranial stimulation in the addicted brain has been the dlPFC, for its role in cue-reactivity and higher order executive function, its connectivity with the striatal and midbrain reward systems [236], and ease of access, reliability, and validity of signal.

Converging preliminary evidence from interventional studies suggest that cognitive reappraisal of drug cues, motivational interviewing, mindfulness meditation, pharmacological treatment, and neuromodulation may be used to diminish drug cue reactivity by decreasing ACC and OFC activity in the context of drug cues and enhance self-control by increasing dlPFC and IFG function in addicted individuals. Bidirectional arrows for the OFC and dlPFC designate their role in self-control and craving suppression, respectively.
TMS capitalizes on magnetic-field driven cortical depolarization, with high-frequency stimulation largely resulting in excitatory, and low-frequency applications resulting in inhibitory, effects [237, 238]. In smokers, high-frequency TMS of the dlPFC has revealed significant reductions in number of cigarettes smoked and cigarette cue-induced cravings [239], while low-frequency TMS has been associated with abstinence over the course of a two-week stimulation regimen [240]. Neither study reported prolonged abstinence effects as evidenced by follow-up inquiries of drug use. Similar results were reported in methamphetamine-addicted individuals who also showed improved cognitive (learning and memory) function following high-frequency dlPFC TMS [241]. Using deep TMS, where more medial brain regions (including the medial PFC) are accessible for stimulation, modest effects for long-term reductions in cocaine use were reported [242]. Although a promising method of neural perturbation, small sample sizes, variability in long-term treatment outcomes, ambiguousness in specificity of results to active versus sham stimulation, and logistic difficulties for its widespread adoption suggest that our understanding of the way TMS may be reliably utilized in addiction treatment is in its infancy.
In contrast, tDCS is a stimulation technique that is portable and more easily administered. Neuromodulation via tDCS is accomplished by low-voltage currents that are applied to a positively charged electrode (anode), which relays the flow of current to a negatively charged electrode (cathode), with the former inducing neuronal depolarization and excitability, and the latter inducing an inhibitory effect via hyperpolarization [243]. tDCS of the dlPFC has been shown to reduce self-reported craving and number of cigarettes consumed in smokers [244, 245], and reduce alcohol craving [246], improving the likelihood of prolonged abstinence in alcohol-addicted individuals [247, 248]. tDCS of the dlPFC in cocaine addiction has also produced promising results. Groups assigned to receiving active (vs. sham) tDCS exhibited reduced craving, depression, and anxiety following stimulation over the course of 10 days [249, 250], decreased cue-reactivity related ACC signaling (assayed via electrophysiology) in those who received a single stimulation session [251], and improved daytime sleepiness and readiness to change following 15 sessions, suggesting enhanced goal-oriented behaviors [252]. However, larger sample sizes and consideration of factors such as stimulation intensity and duration, and the use of objective measures of brain function, should be considered in future efforts, as relapse rates associated with tDCS yield contradictory findings and need to be interpreted with caution [246, 247].
Neurofeedback offers an even less invasive method of neuromodulation, whereby participants can be provided with real-time indicators of their own brain activity/connectivity, for purposes of neuromodulatory training. Neurofeedback related to craving-associated brain activity and connectivity (in the ACC, mPFC, and posterior cingulate) has shown promise in the successful modulation of cigarette craving [253,254,255]. Alcohol-addicted individuals who underwent neurofeedback training to regulate activity in these regions have also reported reductions in craving [256]. To date, the PFC has not been a target of fMRI neurofeedback studies in cocaine- (or other stimulant) addicted individuals (see [257] for a recent review; for electrophysiological-based feedback studies in stimulant users see [258]; see [259, 260] for additional relevant reviews). Nevertheless, promising results show that neurofeedback of ventral tegmental activity during non-drug reward imagery resulted in successful increases in midbrain activity in cocaine-addicted individuals [261]. On the other end of the neuromodulatory invasiveness spectrum lies DBS. DBS largely involves subcortical stimulation via microelectrodes, showing success in tackling treatment-resistant major depressive disorder and movement/dopaminergic disorders such as Parkinson’s [262,263,264]. Given the need for surgically implanted electrodes, effects of DBS for the treatment of drug addiction are inferred by case studies or limited reports. Here the nucleus accumbens has been used as a target region in a majority of DBS cases [265] showing to greatly decrease craving, and decrease and/or completely resolve alcohol [266,267,268], cocaine [269], and heroin [270, 271] use disorders. DBS of the nucleus accumbens in alcohol dependence has also been reported to normalize dysfunctional error-related activity in the ACC/anterior mid-cingulate, an effect that subsides in-between stimulations [267]. However, the primary drug use curbing effects of DBS do not appear to generalize to the use of other substances in the operated individuals (here opiates, [270]), which may warrant a closer examination of the specificity of action and variability of efficacy based on substance classes, potentially in preclinical models.
Conclusions, clinical implications, and future directions
Going well beyond the confines of the mesencephalic reward pathways, growing human and non-human primate evidence highlights widespread PFC disturbances related to the iRISA syndrome in drug addiction as underlying the actual clinical symptomatology of addiction (e.g., relapse). Namely, deficits in inhibitory control are associated in humans with drug addiction with lower activity in widespread PFC regions such as the dlPFC, ACC, IFG, and OFC, with the latter also implicated in non-human primate models of drug addiction, and manifest in persistent drug use and relapse. Also characterized by the iRISA framework, excessive salience attributed to drugs and related cues over nondrug reinforcers is evident across species and associated with higher ACC and vmPFC/OFC signaling, and manifests as drug cue reactivity, attention bias, and craving. Deficits in reward-related decision-making in addicted individuals are associated with altered cortico-striatal function (e.g., lower dlPFC, IFG, and striatal activity), potentially disrupting adaptive deliberations to favor drug-biased judgements, hindering abstinence goals. Furthermore, poor insight into illness is associated with decreases in ACC activity (and volume), manifesting in disruptions in awareness of drug-seeking behaviors. Together, these emotional/cognitive/behavioral alterations related to inhibitory control, incentive salience, reward-related decision-making, and insight into illness are accompanied by structural and functional degradations in pertinent PFC regions such as the ACC, vmPFC/OFC, IFG, and dlPFC, expressing as the core clinical symptomatology in drug addiction.
Whether these PFC disturbances are the sequelae of chronic drug use or pre-morbid markers of addiction vulnerability is the elusive chicken-or-egg question, for which studies in humans can offer little causal inference. Uniquely in this review, we bridged the neurobiological studies in human drug addiction and findings revealed via randomized longitudinal prospective studies in non-human primates to infer causality as to the source of the prefrontal insult and its potential recovery (Fig. 2). By virtue of 2 × 2 non-human primate designs, whereby monkeys are randomly assigned to self-administer cocaine, followed by assessment of subsequent experimenter-guaranteed abstinence, we can conclude that cocaine self-administration reduces OFC gray matter density and that abstinence from cocaine partially reverses this effect [79]. With similar OFC patterns in drug addiction and abstinence in humans [70], we can infer that prolonged and chronic cocaine self-administration indeed causes PFC insult. Because OFC structural morphology also predicts addiction vulnerability (e.g., in those prenatally exposed to nicotine and/or alcohol [74, 75]), the relationship between PFC insult and drug addiction may be bidirectional. That is, a compromised PFC (e.g., via risk factors such as prenatal exposure to drugs and/or early life stress [74, 272]) can enhance addiction vulnerability, potentially hastening or exacerbating the PFC insult induced by the drug itself, culminating in the persistent drug addiction cycle more readily in vulnerable individuals (see Fig. 2). Additional mechanisms (e.g., connectivity of the OFC with other brain regions: see [273] where hypoconnectivity between the striatum and the OFC predicted addiction vulnerability while hyperconnectivity between the striatum and the lateral PFC predicted resilience) remain to be fully elucidated.
We reviewed numerous studies in drug-addicted individuals that have demonstrated neuropsychological impairments related to incentive salience and inhibitory control studied independently. However, very few studies have examined the interaction of these processes. Lapses in self-control may be especially pronounced during cue-reactivity, rendering this avenue most pertinent to drug-addicted individuals’ experiences outside of the laboratory setting. Modifications of well-validated tools such as the Stroop task have engendered fruitful examinations of attentional bias to drug-related cues [138], and a similar approach using other classical inhibitory control (such as the stop-signal or Go/NoGo) tasks may be effective in capturing self-control as a function of cue-reactivity ([143, 146]; unpublished data: Ceceli, Parvaz et al.). Newer tools (e.g., movie watching and/or speech sample analyses [274, 275]) and computational efforts to track the dynamic and cyclical nature of drug addiction [276] may advance the field towards more ecological validity as remains to be tested.
We have dissected the human and non-human primate drug addiction literature while considering substance-specific and substance-general effects, and it is evident that more studies are needed to elucidate the distinct contributions of different drug classes, potentially most amenable for preclinical research. Characterizing the unique and shared neurobiological anomalies driven by specific substances has important treatment implications [182]. In the human realm, such studies are restricted by the prevalence of polysubstance use and heterogeneities in substance users’ drug use patterns; [277], which, in this review, we sought to minimize by focusing only on drug addiction as opposed to recreational use or abuse (e.g., excluding non-addicted adolescents). Future studies may overcome these difficulties also by carefully tracking drug use histories and employing well-matched experimental groups (e.g., based on the primary drug of abuse). Pooled-analyses may be effective in identifying substance-specific effects, as evident in two meta/mega-analyses that have extracted the contributions of specific substances to neuroanatomical variability in drug addiction, overcoming issues of statistical power while accounting for drug use pattern variability ([34]; unpublished data: Ottino-González et al.). Compared to human research, non-human primate studies can explore more specific hypotheses by closely controlling the substance type, amount of use (to date largely impossible in the human literature), and exposure duration. Such explorations could more directly answer questions of dose, duration and other drug use effects (on brain regional variability in both structure and function) and causality (e.g., when and how occasional use becomes irreversibly detrimental).
Our understanding of neuromodulation—brain perturbation methods that have shown promising results in reducing craving and potentially improving drug use outcomes—remains in its infancy. tDCS is an especially promising tool for at-home use targeting relevant brain networks for decreasing drug craving and use; however, larger-scale studies with a focus on effective stimulation parameters and objective predictors of long-term outcomes are needed [278]. Moreover, neurofeedback studies have yet to fully account for (and potentially normalize) the PFC-driven dysfunctions in drug-addicted populations. Although such studies have utilized cortical and subcortical regions of interest as markers for functional neuromodulatory training (e.g., fMRI neurofeedback) in tobacco and alcohol-addicted individuals [253,254,255,256], the ventral tegmental area has enjoyed most of the attention, with no study to date targeting the PFC for neurofeedback training in stimulant-addicted individuals. Specific PFC sub-regions could be considered as potential neural perturbation targets. As illustrated in Fig. 3, studies using tDCS and neurofeedback can target the dlPFC while providing cognitive training to improve control over drug-related behaviors and promote adaptive decision-making. In addition, the ACC, IFG and dlPFC may serve as promising deep TMS and neurofeedback targets during exposure to drug cues, with their sustained perturbation (e.g., suppression of the ACC and dlPFC, activation of the IFG) potentially leading to curbed drug cue reactivity and attention bias, and improved self-control and abstinence outcomes.
In sum, using a cross-species approach we reviewed the neurobehavioral underpinnings of drug addiction as related to the PFC. Our unique approach allowed us to reach three main conclusions: (1) drug addiction accompanies widespread PFC disturbances related to emotional, cognitive, and behavioral functions as described in the iRISA framework, manifesting in excessive and persistent drug use. (2) The converging human and non-human primate findings permit us to assign directionality to the relationship between chronic drug use and PFC insult: drug use and addiction cause damage to PFC structure and function. Premorbid factors such as prenatal drug exposure and early life stress may also impact PFC integrity and accelerate the transition to addiction in vulnerable individuals, although the contribution of these factors need to be further interrogated preclinically. (3) The destructive impact of drug use and addiction is at least partially reversible via abstinence, yet treatment permeability requires further inquiry that would consider substance-specific neurobiological substrates and advances in neuromodulatory methods prioritizing specific PFC targets. Overall, our focus in this review on the PFC was driven by the goal to continue characterizing higher-order emotional, cognitive, and behavioral functions in drug addiction, drawing cross-species parallels and highlighting areas for future research. This PFC-based approach aims to ultimately contribute to the design of empirically-based, neuroscience-informed effective intervention and prevention efforts to minimize the catastrophic toll of the effects of drug use and addiction at the neural, behavioral, and societal levels.
References
O’Brien CP, Volkow N, Li T-K. What’s in a word? Addiction versus dependence in DSM-V. Am J Psychiatry. 2006;163:764–5.
Wise RA. Neurobiology of addiction. Curr Opin Neurobiol. 1996;6:243–51.
Knutson B, Adams CM, Fong GW, Hommer D. Anticipation of increasing monetary reward selectively recruits nucleus accumbens. J Neurosci. 2001;21:RC159–RC159.
Robinson TE, Gorny G, Mitton E, Kolb B. Cocaine self-administration alters the morphology of dendrites and dendritic spines in the nucleus accumbens and neocortex. Synapse. 2001;39:257–66.
O’Doherty JP, Dayan P, Schultz J, Deichmann R, Friston K, Dolan RJ. Dissociable roles of ventral and dorsal striatum in instrumental conditioning. Science. 2004;304:452–4.
Balleine BW, O’Doherty JP. Human and rodent homologies in action control: corticostriatal determinants of goal-directed and habitual action. Neuropsychopharmacology. 2009;35:48–69.
Volkow ND, Fowler JS. Addiction, a disease of compulsion and drive: involvement of the orbitofrontal cortex. Cereb Cortex. 2000;10:318–25.
Gläscher J, Hampton AN, O’Doherty JP. Determining a role for ventromedial prefrontal cortex in encoding action-based value signals during reward-related decision making. Cereb Cortex. 2009;19:483–95.
Pujara MS, Philippi CL, Motzkin JC, Baskaya MK, Koenigs M. Ventromedial prefrontal cortex damage is associated with decreased ventral striatum volume and response to reward. J Neurosci. 2016;36:5047–54.
Daw ND, O’Doherty JP, Dayan P, Seymour B, Dolan RJ. Cortical substrates for exploratory decisions in humans. Nature. 2006;441:876–9.
Brockett AT, Roesch MR. The ever-changing OFC landscape: what neural signals in OFC can tell us about inhibitory control. Behav Neurosci. 2021;135:129–37.
Rolls ET, Everitt BJ, Roberts A, Roberts AC, Robbins TW, Weiskrantz L. The orbitofrontal cortex. Philos Trans R Soc Lond Ser B. 1996;351:1433–44.
O’Doherty J, Kringelbach ML, Rolls ET, Hornak J, Andrews C. Abstract reward and punishment representations in the human orbitofrontal cortex. Nat Neurosci. 2001;4:95–102.
Bechara A, Tranel D, Damasio H. Characterization of the decision-making deficit of patients with ventromedial prefrontal cortex lesions. Brain. 2000;123:2189–202.
Reber J, Feinstein JS, O’Doherty JP, Liljeholm M, Adolphs R, Tranel D. Selective impairment of goal-directed decision-making following lesions to the human ventromedial prefrontal cortex. Brain. 2017;140:1743–56.
Petrides M, Tomaiuolo F, Yeterian EH, Pandya DN. The prefrontal cortex: comparative architectonic organization in the human and the macaque monkey brains. Cortex. 2012;48:46–57.
Aron AR, Behrens TE, Smith S, Frank MJ, Poldrack RA. Triangulating a cognitive control network using diffusion-weighted magnetic resonance imaging (MRI) and functional MRI. J Neurosci. 2007;27:3743–52.
Dick AS, Garic D, Graziano P, Tremblay P. The frontal aslant tract (FAT) and its role in speech, language and executive function. Cortex. 2019;111:148–63.
Sallet J, Mars RB, Noonan MP, Neubert F-X, Jbabdi S, O’Reilly JX, et al. The organization of dorsal frontal cortex in humans and macaques. J Neurosci. 2013;33:12255–74.
Kane MJ, Engle RW. The role of prefrontal cortex in working-memory capacity, executive attention, and general fluid intelligence: an individual-differences perspective. Psychonomic Bull Rev. 2002;9:637–71.
Goldin PR, McRae K, Ramel W, Gross JJ. The neural bases of emotion regulation: reappraisal and suppression of negative emotion. Biol Psychiatry. 2008;63:577–86.
Barbey AK, Koenigs M, Grafman J. Dorsolateral prefrontal contributions to human working memory. Cortex. 2013;49:1195–205.
Paus T. Primate anterior cingulate cortex: where motor control, drive and cognition interface. Nat Rev Neurosci. 2001;2:417–24.
Carter CS, Braver TS, Barch DM, Botvinick MM, Noll D, Cohen JD. Anterior cingulate cortex, error detection, and the online monitoring of performance. Science. 1998;280:747–9.
Bush G, Vogt BA, Holmes J, Dale AM, Greve D, Jenike MA, et al. Dorsal anterior cingulate cortex: a role in reward-based decision making. PNAS. 2002;99:523–8.
Etkin A, Egner T, Kalisch R. Emotional processing in anterior cingulate and medial prefrontal cortex. Trends Cogn Sci. 2011;15:85–93.
Goldstein RZ, Volkow ND. Drug addiction and its underlying neurobiological basis: neuroimaging evidence for the involvement of the frontal cortex. Am J Psychiatry. 2002;159:1642–52.
Goldstein RZ, Volkow ND. Dysfunction of the prefrontal cortex in addiction: neuroimaging findings and clinical implications. Nat Rev Neurosci. 2011;12:652–69.
Zilverstand A, Huang AS, Alia-Klein N, Goldstein RZ. Neuroimaging impaired response inhibition and salience attribution in human drug addiction: a systematic review. Neuron. 2018;98:886–903.
Roberts AC, Clarke HF. Why we need nonhuman primates to study the role of ventromedial prefrontal cortex in the regulation of threat- and reward-elicited responses. PNAS. 2019;116:26297–304.
Barbas H, Pandya DN. Architecture and intrinsic connections of the prefrontal cortex in the rhesus monkey. J Comp Neurol. 1989;286:353–75.
Öngür D, Price JL. The organization of networks within the orbital and medial prefrontal cortex of rats, monkeys and humans. Cereb Cortex. 2000;10:206–19.
Yeterian EH, Pandya DN, Tomaiuolo F, Petrides M. The cortical connectivity of the prefrontal cortex in the monkey brain. Cortex. 2012;48:58–81.
Mackey S, Allgaier N, Chaarani B, Spechler P, Orr C, Bunn J, et al. Mega-analysis of gray matter volume in substance dependence: general and substance-specific regional effects. Am J Psychiatry. 2019;176:119–28.
Ersche KD, Williams GB, Robbins TW, Bullmore ET. Meta-analysis of structural brain abnormalities associated with stimulant drug dependence and neuroimaging of addiction vulnerability and resilience. Curr Opin Neurobiol. 2013;23:615–24.
Tanabe J, Tregellas JR, Dalwani M, Thompson L, Owens E, Crowley T, et al. Medial orbitofrontal cortex gray matter is reduced in abstinent substance-dependent individuals. Biol Psychiatry. 2009;65:160–4.
Menon V, Uddin LQ. Saliency, switching, attention and control: a network model of insula function. Brain Struct Funct. 2010;214:655–67.
MacDonald AW, Cohen JD, Stenger VA, Carter CS. Dissociating the role of the dorsolateral prefrontal and anterior cingulate cortex in cognitive control. Science. 2000;288:1835–8.
Levy BJ, Wagner AD. Cognitive control and right ventrolateral prefrontal cortex: reflexive reorienting, motor inhibition, and action updating. Ann N Y Acad Sci. 2011;1224:40–62.
Kovach CK, Daw ND, Rudrauf D, Tranel D, O’Doherty JP, Adolphs R. Anterior prefrontal cortex contributes to action selection through tracking of recent reward trends. J Neurosci. 2012;32:8434–42.
Fritz H-C, Wittfeld K, Schmidt CO, Domin M, Grabe HJ, Hegenscheid K, et al. Current smoking and reduced gray matter volume-a voxel-based morphometry study. Neuropsychopharmacology. 2014;39:2594–2600.
Kaag AM, Schulte MHJ, Jansen JM, van Wingen G, Homberg J, van den Brink W, et al. The relation between gray matter volume and the use of alcohol, tobacco, cocaine and cannabis in male polysubstance users. Drug Alcohol Depend. 2018;187:186–94.
Sutherland MT, Riedel MC, Flannery JS, Yanes JA, Fox PT, Stein EA, et al. Chronic cigarette smoking is linked with structural alterations in brain regions showing acute nicotinic drug-induced functional modulations. Behav Brain Funct. 2016;12:16.
Stoeckel LE, Chai XJ, Zhang J, Whitfield-Gabrieli S, Evins AE. Lower gray matter density and functional connectivity in the anterior insula in smokers compared with never smokers. Addict Biol. 2016;21:972–81.
Rosenthal A, Beck A, Zois E, Vollstädt-Klein S, Walter H, Kiefer F, et al. Volumetric prefrontal cortex alterations in patients with alcohol dependence and the involvement of self-control. Alcohol Clin Exp Res. 2019;43:2514–24.
Fortier CB, Leritz EC, Salat DH, Venne JR, Maksimovskiy AL, Williams V, et al. Reduced cortical thickness in abstinent alcoholics and association with alcoholic behavior. Alcohol Clin Exp Res. 2011;35:2193–201.
Wiers CE, Gawron CK, Gröpper S, Spengler S, Stuke H, Lindenmeyer J, et al. Decreased gray matter volume in inferior frontal gyrus is related to stop-signal task performance in alcohol-dependent patients. Psychiatry Res. 2015;233:125–30.
Wang J, Fan Y, Dong Y, Ma M, Ma Y, Dong Y, et al. Alterations in brain structure and functional connectivity in alcohol dependent patients and possible association with impulsivity. PLoS One. 2016;11:e0161956.
Alia-Klein N, Parvaz MA, Woicik PA, Konova AB, Maloney T, Shumay E, et al. Gene x disease interaction on orbitofrontal gray matter in cocaine addiction. Arch Gen Psychiatry. 2011;68:283–94.
Hall MG, Alhassoon OM, Stern MJ, Wollman SC, Kimmel CL, Perez-Figueroa A, et al. Gray matter abnormalities in cocaine versus methamphetamine-dependent patients: a neuroimaging meta-analysis. Am J Drug Alcohol Abus. 2015;41:290–9.
Franklin TR, Acton PD, Maldjian JA, Gray JD, Croft JR, Dackis CA, et al. Decreased gray matter concentration in the insular, orbitofrontal, cingulate, and temporal cortices of cocaine patients. Biol Psychiatry. 2002;51:134–42.
Yip SW, Worhunsky PD, Xu J, Morie KP, Constable RT, Malison RT, et al. Gray-matter relationships to diagnostic and transdiagnostic features of drug and behavioral addictions. Addict Biol. 2018;23:394–402.
Hirsiger S, Hänggi J, Germann J, Vonmoos M, Preller KH, Engeli EJE, et al. Longitudinal changes in cocaine intake and cognition are linked to cortical thickness adaptations in cocaine users. Neuroimage Clin. 2019;21:101652.
Smith DG, Jones PS, Williams GB, Bullmore ET, Robbins TW, Ersche KD. Overlapping decline in orbitofrontal gray matter volume related to cocaine use and body mass index. Addict Biol. 2015;20:194–6.
Matuskey D, Bhagwagar Z, Planeta B, Pittman B, Gallezot J-D, Chen J, et al. Reductions in brain 5-HT1B receptor availability in primarily cocaine-dependent humans. Biol Psychiatry. 2014;76:816–22.
Konova AB, Moeller SJ, Tomasi D, Parvaz MA, Alia-Klein N, Volkow ND, et al. Structural and behavioral correlates of abnormal encoding of money value in the sensorimotor striatum in cocaine addiction. Eur J Neurosci. 2012;36:2979–88.
Moreno-López L, Catena A, Fernández-Serrano MJ, Delgado-Rico E, Stamatakis EA, Pérez-García M, et al. Trait impulsivity and prefrontal gray matter reductions in cocaine dependent individuals. Drug Alcohol Depend. 2012;125:208–14.
Wollman SC, Alhassoon OM, Hall MG, Stern MJ, Connors EJ, Kimmel CL, et al. Gray matter abnormalities in opioid-dependent patients: a neuroimaging meta-analysis. Am J Drug Alcohol Abus. 2017;43:505–17.
Liu H, Hao Y, Kaneko Y, Ouyang X, Zhang Y, Xu L, et al. Frontal and cingulate gray matter volume reduction in heroin dependence: optimized voxel-based morphometry. Psychiatry Clin Neurosci. 2009;63:563–8.
Yuan Y, Zhu Z, Shi J, Zou Z, Yuan F, Liu Y, et al. Gray matter density negatively correlates with duration of heroin use in young lifetime heroin-dependent individuals. Brain Cogn. 2009;71:223–8.
Shi H, Liang Z, Chen J, Li W, Zhu J, Li Y, et al. Gray matter alteration in heroin-dependent men: an atlas-based magnetic resonance imaging study. Psychiatry Res Neuroimaging. 2020;304:111150.
Wang X, Li B, Zhou X, Liao Y, Tang J, Liu T, et al. Changes in brain gray matter in abstinent heroin addicts. Drug Alcohol Depend. 2012;126:304–8.
Lin H-C, Wang P-W, Wu H-C, Ko C-H, Yang Y-H, Yen C-F. Altered gray matter volume and disrupted functional connectivity of dorsolateral prefrontal cortex in men with heroin dependence. Psychiatry Clin Neurosci. 2018;72:435–44.
Li M, Tian J, Zhang R, Qiu Y, Wen X, Ma X, et al. Abnormal cortical thickness in heroin-dependent individuals. Neuroimage. 2014;88:295–307.
Hanlon CA, Owens MM, Joseph JE, Zhu X, George MS, Brady KT, et al. Lower subcortical gray matter volume in both younger smokers and established smokers relative to non-smokers. Addict Biol. 2016;21:185–95.
Fein G, Di Sclafani V, Cardenas VA, Goldmann H, Tolou-Shams M, Meyerhoff DJ. Cortical gray matter loss in treatment-naïve alcohol dependent individuals. Alcohol Clin Exp Res. 2002;26:558–64.
Barrós-Loscertales A, Garavan H, Bustamante JC, Ventura-Campos N, Llopis JJ, Belloch V, et al. Reduced striatal volume in cocaine-dependent patients. Neuroimage. 2011;56:1021–6.
Connolly CG, Bell RP, Foxe JJ, Garavan H. Dissociated grey matter changes with prolonged addiction and extended abstinence in cocaine users. PLoS One. 2013;8:e59645.
Durazzo TC, Mon A, Gazdzinski S, Yeh P-H, Meyerhoff DJ. Serial longitudinal magnetic resonance imaging data indicate non-linear regional gray matter volume recovery in abstinent alcohol-dependent individuals. Addict Biol. 2015;20:956–67.
Parvaz MA, Moeller SJ, d’Oleire Uquillas F, Pflumm A, Maloney T, Alia-Klein N, et al. Prefrontal gray matter volume recovery in treatment-seeking cocaine-addicted individuals: a longitudinal study. Addict Biol. 2017;22:1391–401.
Durazzo TC, Mon A, Gazdzinski S, Meyerhoff DJ. Regional brain volume changes in alcohol-dependent individuals during early abstinence: associations with relapse following treatment. Addict Biol. 2017;22:1416–25.
Rando K, Hong K-I, Bhagwagar Z, Li C-SR, Bergquist K, Guarnaccia J, et al. Association of frontal and posterior cortical gray matter volume with time to alcohol relapse: a prospective study. Am J Psychiatry. 2011;168:183–92.
Ersche KD, Jones PS, Williams GB, Turton AJ, Robbins TW, Bullmore ET. Abnormal brain structure implicated in stimulant drug addiction. Science. 2012;335:601–4.
Lotfipour S, Ferguson E, Leonard G, Perron M, Pike B, Richer L, et al. Orbitofrontal cortex and drug use during adolescence: role of prenatal exposure to maternal smoking and BDNF genotype. Arch Gen Psychiatry. 2009;66:1244.
Kühn S, Witt C, Banaschewski T, Barbot A, Barker GJ, Büchel C, et al. From mother to child: orbitofrontal cortex gyrification and changes of drinking behaviour during adolescence. Addiction Biol. 2016;21:700–8.
Ersche KD, Jones PS, Williams GB, Smith DG, Bullmore ET, Robbins TW. Distinctive personality traits and neural correlates associated with stimulant drug use versus familial risk of stimulant dependence. Biol Psychiatry. 2013;74:137–44.
Song X, García-Saldivar P, Kindred N, Wang Y, Merchant H, Meguerditchian A, et al. Strengths and challenges of longitudinal non-human primate neuroimaging. NeuroImage. 2021;236:118009.
Kroenke CD, Rohlfing T, Park B, Sullivan EV, Pfefferbaum A, Grant KA. Monkeys that voluntarily and chronically drink alcohol damage their brains: a longitudinal MRI study. Neuropsychopharmacology. 2014;39:823–30.
Jedema HP, Song X, Aizenstein HJ, Bonner AR, Stein EA, Yang Y, et al. Long-term cocaine self-administration produces structural brain changes that correlate with altered cognition. Biol Psychiatry. 2021;89:376–85.
Carvalho M, Carmo H, Costa VM, Capela JP, Pontes H, Remião F, et al. Toxicity of amphetamines: an update. Arch Toxicol. 2012;86:1167–231.
Kousik SM, Napier TC, Carvey PM. The effects of psychostimulant drugs on blood brain barrier function and neuroinflammation. Front Pharmacol. 2012;3:121.
De Erausquin GA, Alba-Ferrara L. What does anisotropy measure? Insights from increased and decreased anisotropy in selective fiber tracts in schizophrenia. Front Integr Neurosci. 2013;7:9.
Soares J, Marques P, Alves V, Sousa N. A hitchhiker’s guide to diffusion tensor imaging. Front Neurosci. 2013;7:31.
Song S-K, Yoshino J, Le TQ, Lin S-J, Sun S-W, Cross AH, et al. Demyelination increases radial diffusivity in corpus callosum of mouse brain. Neuroimage. 2005;26:132–40.
Loy DN, Kim JH, Xie M, Schmidt RE, Trinkaus K, Song S-K. Diffusion tensor imaging predicts hyperacute spinal cord injury severity. J Neurotrauma. 2007;24:979–90.
Winklewski PJ, Sabisz A, Naumczyk P, Jodzio K, Szurowska E, Szarmach A. Understanding the physiopathology behind axial and radial diffusivity changes—what do we know? Front Neurol. 2018;9:92.
Della Nave R, Ginestroni A, Diciotti S, Salvatore E, Soricelli A, Mascalchi M. Axial diffusivity is increased in the degenerating superior cerebellar peduncles of Friedreich’s ataxia. Neuroradiology. 2011;53:367–72.
Hampton WH, Hanik IM, Olson IR. Substance abuse and white matter: findings, limitations, and future of diffusion tensor imaging research. Drug Alcohol Depend. 2019;197:288–98.
Lin F, Wu G, Zhu L, Lei H. Heavy smokers show abnormal microstructural integrity in the anterior corpus callosum: a diffusion tensor imaging study with tract-based spatial statistics. Drug Alcohol Depend. 2013;129:82–87.
Baeza-Loya S, Velasquez KM, Molfese DL, Viswanath H, Curtis KN, Thompson-Lake DGY, et al. Anterior cingulum white matter is altered in tobacco smokers. Am J Addict. 2016;25:210–4.
Savjani RR, Velasquez KM, Thompson-Lake DGY, Baldwin PR, Eagleman DM, De La Garza R, et al. Characterizing white matter changes in cigarette smokers via diffusion tensor imaging. Drug Alcohol Depend. 2014;145:134–42.
Fortier CB, Leritz EC, Salat DH, Lindemer E, Maksimovskiy AL, Shepel J, et al. Widespread effects of alcohol on white matter microstructure. Alcohol Clin Exp Res. 2014;38:2925–33.
Jansen JM, van Holst RJ, van den Brink W, Veltman DJ, Caan MWA, Goudriaan AE. Brain function during cognitive flexibility and white matter integrity in alcohol-dependent patients, problematic drinkers and healthy controls. Addict Biol. 2015;20:979–89.
Ashtari M, Cervellione K, Cottone J, Ardekani BA, Kumra S. Diffusion abnormalities in adolescents and young adults with a history of heavy cannabis use. J Psychiatr Res. 2009;43:189–204.
Gruber SA, Silveri MM, Dahlgren MK, Yurgelun-Todd D. Why so impulsive? White matter alterations are associated with impulsivity in chronic marijuana smokers. Exp Clin Psychopharmacol. 2011;19:231–42.
Filbey FM, Aslan S, Calhoun VD, Spence JS, Damaraju E, Caprihan A, et al. Long-term effects of marijuana use on the brain. Proc Natl Acad Sci USA. 2014;111:16913–8.
Suchting R, Beard CL, Schmitz JM, Soder HE, Yoon JH, Hasan KM, et al. A meta-analysis of tract-based spatial statistics studies examining white matter integrity in cocaine use disorder. Addiction Biol. 2021;26:e12902.
He Q, Li D, Turel O, Bechara A, Hser Y-I. White matter integrity alternations associated with cocaine dependence and long-term abstinence: preliminary findings. Behavioural Brain Res. 2020;379:112388.
Romero MJ, Asensio S, Palau C, Sanchez A, Romero FJ. Cocaine addiction: diffusion tensor imaging study of the inferior frontal and anterior cingulate white matter. Psychiatry Res. 2010;181:57–63.
van Son D, Wiers RW, Catena A, Perez-Garcia M, Verdejo-García A. White matter disruptions in male cocaine polysubstance users: associations with severity of drug use and duration of abstinence. Drug Alcohol Depend. 2016;168:247–54.
Lederer K, Fouche J-P, Wilson D, Stein DJ, Uhlmann A. Frontal white matter changes and aggression in methamphetamine dependence. Metab Brain Dis. 2016;31:53–62.
Bora E, Yücel M, Fornito A, Pantelis C, Harrison BJ, Cocchi L, et al. White matter microstructure in opiate addiction. Addict Biol. 2012;17:141–8.
Wollman SC, Alhassoon OM, Stern MJ, Hall MG, Rompogren J, Kimmel CL, et al. White matter abnormalities in long-term heroin users: a preliminary neuroimaging meta-analysis. Am J Drug Alcohol Abus. 2015;41:133–8.
Wang Y, Li W, Li Q, Yang W, Zhu J, Wang W. White matter impairment in heroin addicts undergoing methadone maintenance treatment and prolonged abstinence: a preliminary DTI study. Neurosci Lett. 2011;494:49–53.
Li W, Zhu J, Li Q, Ye J, Chen J, Liu J, et al. Brain white matter integrity in heroin addicts during methadone maintenance treatment is related to relapse propensity. Brain Behav. 2016;6:e00436.
Liu H, Li L, Hao Y, Cao D, Xu L, Rohrbaugh R, et al. Disrupted white matter integrity in heroin dependence: a controlled study utilizing diffusion tensor imaging. Am J Drug Alcohol Abus. 2008;34:562–75.
Wang X, Yu R, Zhou X, Liao Y, Tang J, Liu T, et al. Reversible brain white matter microstructure changes in heroin addicts: a longitudinal study. Addict Biol. 2013;18:727–8.
Li W, Li Q, Zhu J, Qin Y, Zheng Y, Chang H, et al. White matter impairment in chronic heroin dependence: a quantitative DTI study. Brain Res. 2013;1531:58–64.
Smith HR, Beveridge TJR, Nader MA, Porrino LJ. Regionally-specific alterations in myelin proteins in nonhuman primate white matter following prolonged cocaine self-administration. Drug Alcohol Depend. 2014;137:143–7.
Smith HR, Beveridge TJR, Nader SH, Nader MA, Porrino LJ. Regional elevations in microglial activation and cerebral glucose utilization in frontal white matter tracts of rhesus monkeys following prolonged cocaine self-administration. Brain Struct Funct. 2019;224:1417–28.
Aron AR, Poldrack RA. Cortical and subcortical contributions to stop signal response inhibition: role of the subthalamic nucleus. J Neurosci. 2006;26:2424–33.
Cole MW, Schneider W. The cognitive control network: Integrated cortical regions with dissociable functions. NeuroImage. 2007;37:343–60.
Garavan H, Ross TJ, Murphy K, Roche RAP, Stein EA. Dissociable executive functions in the dynamic control of behavior: inhibition, error detection, and correction. Neuroimage. 2002;17:1820–9.
Gomez P, Ratcliff R, Perea M. A model of the Go/No-Go task. J Exp Psychol Gen. 2007;136:389–413.
Verbruggen F, Logan GD. Response inhibition in the stop-signal paradigm. Trends Cogn Sci. 2008;12:418–24.
Jensen AR, Rohwer WD. The stroop color-word test: a review. Acta Psychol. 1966;25:36–93.
Luijten M, Veltman DJ, Hester R, Smits M, Nijs IMT, Pepplinkhuizen L, et al. The role of dopamine in inhibitory control in smokers and non-smokers: a pharmacological fMRI study. Eur Neuropsychopharmacol. 2013;23:1247–56.
Eldreth DA, Matochik JA, Cadet JL, Bolla KI. Abnormal brain activity in prefrontal brain regions in abstinent marijuana users. Neuroimage. 2004;23:914–20.
Kober H, DeVito EE, DeLeone CM, Carroll KM, Potenza MN. Cannabis abstinence during treatment and one-year follow-up: relationship to neural activity in men. Neuropsychopharmacology. 2014;39:2288–98.
Li C-SR, Luo X, Yan P, Bergquist K, Sinha R. Altered impulse control in alcohol dependence: neural measures of stop signal performance. Alcohol Clin Exp Res. 2009;33:740–50.
Kaufman JN, Ross TJ, Stein EA, Garavan H. Cingulate hypoactivity in cocaine users during a GO-NOGO task as revealed by event-related functional magnetic resonance imaging. J Neurosci. 2003;23:7839–43.
Li CR, Huang C, Yan P, Bhagwagar Z, Milivojevic V, Sinha R. Neural correlates of impulse control during stop signal inhibition in cocaine-dependent men. Neuropsychopharmacology. 2008;33:1798–806.
Moeller SJ, Froböse MI, Konova AB, Misyrlis M, Parvaz MA, Goldstein RZ, et al. Common and distinct neural correlates of inhibitory dysregulation: Stroop fMRI study of cocaine addiction and intermittent explosive disorder. J Psychiatr Res. 2014;0:55–62.
Barrós-Loscertales A, Bustamante J-C, Ventura-Campos N, Llopis J-J, Parcet M-A, Ávila C. Lower activation in the right frontoparietal network during a counting Stroop task in a cocaine-dependent group. Psychiatry Res. 2011;194:111–8.
Hester R, Garavan H. Executive dysfunction in cocaine addiction: evidence for discordant frontal, cingulate, and cerebellar activity. J Neurosci. 2004;24:11017–22.
Fu L, Bi G, Zou Z, Wang Y, Ye E, Ma L, et al. Impaired response inhibition function in abstinent heroin dependents: an fMRI study. Neurosci Lett. 2008;438:322–6.
Lee TMC, Zhou W, Luo X, Yuen KSL, Ruan X, Weng X. Neural activity associated with cognitive regulation in heroin users: a fMRI study. Neurosci Lett. 2005;382:211–6.
Luijten M, O’Connor DA, Rossiter S, Franken IHA, Hester R. Effects of reward and punishment on brain activations associated with inhibitory control in cigarette smokers. Addiction. 2013;108:1969–78.
Hu S, Ide JS, Zhang S, Sinha R, Li CR. Conflict anticipation in alcohol dependence — a model-based fMRI study of stop signal task. NeuroImage Clin. 2015;8:39–50.
Luijten M, Machielsen MWJ, Veltman DJ, Hester R, de Haan L, Franken IHA. Systematic review of ERP and fMRI studies investigating inhibitory control and error processing in people with substance dependence and behavioural addictions. J Psychiatry Neurosci. 2014;39:149–69.
Jentsch JD, Olausson P, De La Garza R, Taylor JR. Impairments of reversal learning and response perseveration after repeated, intermittent cocaine administrations to monkeys. Neuropsychopharmacology. 2002;26:183–90.
Butter CM. Perseveration in extinction and in discrimination reversal tasks following selective frontal ablations in Macaca mulatta. Physiol Behav. 1969;4:163–71.
Porter JN, Olsen AS, Gurnsey K, Dugan BP, Jedema HP, Bradberry CW. Chronic cocaine self-administration in rhesus monkeys: impact on associative learning, cognitive control, and working memory. J Neurosci. 2011;31:4926–34.
Gould RW, Gage HD, Nader MA. Effects of chronic cocaine self-administration on cognition and cerebral glucose utilization in rhesus monkeys. Biol Psychiatry. 2012;72:856–63.
Field M, Cox WM. Attentional bias in addictive behaviors: a review of its development, causes, and consequences. Drug Alcohol Depend. 2008;97:1–20.
Onken LS, Blaine JD, Boren JJ. Behavioral treatments for drug abuse and dependence. U.S. Department of Health and Human Services, Public Health Service, National Institutes of Health, National Institute on Drug Abuse; 1993.
Waters AJ, Marhe R, Franken IHA. Attentional bias to drug cues is elevated before and during temptations to use heroin and cocaine. Psychopharmacology. 2012;219:909–21.
Smith DG, Ersche KD. Using a drug-word Stroop task to differentiate recreational from dependent drug use. CNS Spectr. 2014;19:247–55.
Goldstein RZ, Tomasi D, Alia-Klein N, Carrillo JH, Maloney T, Woicik PA, et al. Dopaminergic response to drug words in cocaine addiction. J Neurosci. 2009;29:6001–6.
Goldstein RZ, Alia-Klein N, Tomasi D, Carrillo JH, Maloney T, Woicik PA, et al. Anterior cingulate cortex hypoactivations to an emotionally salient task in cocaine addiction. Proc Natl Acad Sci USA. 2009;106:9453–8.
Denomme WJ, Shane MS. History of withdrawal modulates drug- and food-cue reactivity in cocaine dependent participants. Drug Alcohol Depend. 2020;208:107815.
Luijten M, Veltman DJ, van den Brink W, Hester R, Field M, Smits M, et al. Neurobiological substrate of smoking-related attentional bias. Neuroimage. 2011;54:2374–81.
Gilman JM, Radoman M, Schuster RM, Pachas G, Azzouz N, Fava M, et al. Anterior insula activation during inhibition to smoking cues is associated with ability to maintain tobacco abstinence. Addict Behav Rep. 2018;7:40–46.
Vollstädt‐Klein S, Loeber S, Richter A, Kirsch M, Bach P, Goltz Cvonder, et al. Validating incentive salience with functional magnetic resonance imaging: association between mesolimbic cue reactivity and attentional bias in alcohol-dependent patients. Addiction Biol. 2012;17:807–16.
Ames SL, Wong SW, Bechara A, Cappelli C, Dust M, Grenard JL, et al. Neural correlates of a Go/NoGo task with alcohol stimuli in light and heavy young drinkers. Behav Brain Res. 2014;0:382–9.
Czapla M, Baeuchl C, Simon JJ, Richter B, Kluge M, Friederich H-C, et al. Do alcohol-dependent patients show different neural activation during response inhibition than healthy controls in an alcohol-related fMRI go/no-go-task? Psychopharmacology. 2017;234:1001–15.
Hester R, Garavan H. Neural mechanisms underlying drug-related cue distraction in active cocaine users. Pharm Biochem Behav. 2009;93:270–7.
Marhe R, Luijten M, van de Wetering BJM, Smits M, Franken IHA. Individual differences in anterior cingulate activation associated with attentional bias predict cocaine use after treatment. Neuropsychopharmacology. 2013;38:1085–93.
Allenby C, Falcone M, Wileyto EP, Cao W, Bernardo L, Ashare RL, et al. Neural cue reactivity during acute abstinence predicts short-term smoking relapse. Addict Biol. 2019. https://doi.org/10.1111/adb.12733.
Janes AC, Pizzagalli DA, Richardt S, deB Frederick B, Chuzi S, Pachas G, et al. Brain reactivity to smoking cues prior to smoking cessation predicts ability to maintain tobacco abstinence. Biol Psychiatry. 2010;67:722–9.
George O, Koob GF. Control of craving by the prefrontal cortex. Proc Natl Acad Sci USA. 2013;110:4165–6.
Hayashi T, Ko JH, Strafella AP, Dagher A. Dorsolateral prefrontal and orbitofrontal cortex interactions during self-control of cigarette craving. Proc Natl Acad Sci USA. 2013;110:4422–7.
Baeg EH, Jackson ME, Jedema HP, Bradberry CW. Orbitofrontal and anterior cingulate cortex neurons selectively process cocaine-associated environmental cues in the rhesus monkey. J Neurosci. 2009;29:11619–27.
Shidara M, Richmond BJ. Anterior cingulate: single neuronal signals related to degree of reward expectancy. Science. 2002;296:1709–11.
Arcurio LR, Finn PR, James TW. Neural mechanisms of high-risk decisions-to-drink in alcohol-dependent women. Addiction Biol. 2015;20:390–406.
Gowin JL, May AC, Wittmann M, Tapert SF, Paulus MP. Doubling down: increased risk-taking behavior following a loss by individuals with cocaine use disorder is associated with striatal and anterior cingulate dysfunction. Biol Psychiatry Cogn Neurosci Neuroimaging. 2017;2:94–103.
Yamamoto DJ, Reynolds J, Krmpotich T, Banich MT, Thompson L, Tanabe J. Temporal profile of fronto-striatal-limbic activity during implicit decisions in drug dependence. Drug Alcohol Depend. 2014;136:108–14.
Wesley MJ, Hanlon CA, Porrino LJ. Poor decision-making by chronic marijuana users is associated with decreased functional responsiveness to negative consequences. Psychiatry Res. 2011;191:51–59.
Tanabe J, Reynolds J, Krmpotich T, Claus E, Thompson LL, Du YP, et al. Reduced neural tracking of prediction error in substance-dependent individuals. Am J Psychiatry. 2013;170:1356–63.
Beylergil SB, Beck A, Deserno L, Lorenz RC, Rapp MA, Schlagenhauf F, et al. Dorsolateral prefrontal cortex contributes to the impaired behavioral adaptation in alcohol dependence. Neuroimage Clin. 2017;15:80–94.
Stewart JL, May AC, Poppa T, Davenport PW, Tapert SF, Paulus MP. You are the danger: attenuated insula response in methamphetamine users during aversive interoceptive decision-making. Drug Alcohol Depend. 2014;0:110–9.
Gradin VB, Baldacchino A, Balfour D, Matthews K, Steele JD. Abnormal brain activity during a reward and loss task in opiate-dependent patients receiving methadone maintenance therapy. Neuropsychopharmacology. 2014;39:885–94.
Balodis IM, Potenza MN. Anticipatory reward processing in addicted populations: a focus on the monetary incentive delay task. Biol Psychiatry. 2015;77:434–44.
Nestor LJ, Suckling J, Ersche KD, Murphy A, McGonigle J, Orban C, et al. Disturbances across whole brain networks during reward anticipation in an abstinent addiction population. NeuroImage Clin. 2020;27:102297.
Claus ED, Shane MS. dACC response to presentation of negative feedback predicts stimulant dependence diagnosis and stimulant use severity. Neuroimage Clin. 2018;20:16–23.
Li CR, Milivojevic V, Kemp K, Hong K, Sinha R. Performance monitoring and stop signal inhibition in abstinent patients with cocaine dependence. Drug Alcohol Depend. 2006;85:205–12.
Ebitz RB, Sleezer BJ, Jedema HP, Bradberry CW, Hayden BY. Tonic exploration governs both flexibility and lapses. PLoS Comput Biol. 2019;15:e1007475.
Moeller SJ, Platt JM, Wu M, Goodwin RD. Perception of treatment need among adults with substance use disorders: longitudinal data from a representative sample of adults in the United States. Drug Alcohol Depend. 2020;209:107895.
Moeller SJ, Goodwin RD, Sullivan RM, Verdejo-Garcia A. Chapter 26 - Drug use and self-awareness of treatment need: an exemplar of how population-based survey studies can address questions relevant to the neuroscience of insight. In: Verdejo-Garcia A, editor. Cognition and Addiction, London: Academic Press; 2020. p. 351–64.
McLellan AT, Meyers K. Contemporary addiction treatment: A review of systems problems for adults and adolescents. Biol Psychiatry. 2004;56:764–70.
Gopalkrishnan N, Babacan H. Cultural diversity and mental health. Australas Psychiatry. 2015;23:6–8.
Hester R, Nestor L, Garavan H. Impaired error awareness and anterior cingulate cortex hypoactivity in chronic cannabis users. Neuropsychopharmacology. 2009;34:2450–8.
Hester R, Simões-Franklin C, Garavan H. Post-error behavior in active cocaine users: poor awareness of errors in the presence of intact performance adjustments. Neuropsychopharmacology. 2007;32:1974–84.
Moeller SJ, Maloney T, Parvaz MA, Dunning JP, Alia-Klein N, Woicik PA, et al. Enhanced choice for viewing cocaine pictures in cocaine addiction. Biol Psychiatry. 2009;66:169–76.
Moeller SJ, Konova AB, Parvaz MA, Tomasi D, Lane RD, Fort C, et al. Functional, structural, and emotional correlates of impaired insight in cocaine addiction. JAMA Psychiatry. 2014;71:61–70.
Moeller SJ, Maloney T, Parvaz MA, Alia-Klein N, Woicik PA, Telang F, et al. Impaired insight in cocaine addiction: laboratory evidence and effects on cocaine-seeking behaviour. Brain. 2010;133:1484–93.
Fleming SM, Weil RS, Nagy Z, Dolan RJ, Rees G. Relating introspective accuracy to individual differences in brain structure. Science. 2010;329:1541–3.
Moeller SJ, Fleming SM, Gan G, Zilverstand A, Malaker P, d’Oleire Uquillas F, et al. Metacognitive impairment in active cocaine use disorder is associated with individual differences in brain structure. Eur Neuropsychopharmacol. 2016;26:653–62.
Lucantonio F, Takahashi Y, Hoffman AF, Chang CY, Chaudhary S, Shaham Y, et al. Orbitofrontal activation restores insight lost after cocaine use. Nat Neurosci. 2014;17:1092–9.
Steptoe A, Wardle J, Smith H, Kopp M, Skrabski A, Vinck J, et al. Tobacco smoking in young adults from 21 European countries: association with attitudes and risk awareness. Addiction. 1995;90:571–82.
Kim JS, Park BK, Kim GJ, Kim SS, Jung JG, Oh MK, et al. The role of alcoholics’ insight in abstinence from alcohol in male Korean alcohol dependents. J Korean Med Sci. 2007;22:132–7.
Badiani A, Belin D, Epstein D, Calu D, Shaham Y. Opiate versus psychostimulant addiction: the differences do matter. Nat Rev Neurosci. 2011;12:685–700.
Schmahmann JD, Pandya D. Fiber pathways of the brain. Oxford University Press, New York, USA; 2009.
Wardlaw JM, Valdés Hernández MC, Muñoz-Maniega S. What are white matter hyperintensities made of? J Am Heart Assoc. 2015;4:e001140.
Lyoo IK, Streeter CC, Ahn KH, Lee HK, Pollack MH, Silveri MM, et al. White matter hyperintensities in subjects with cocaine and opiate dependence and healthy comparison subjects. Psychiatry Res. 2004;131:135–45.
Kaufman MJ. Cocaine-induced cerebral vasoconstriction detected in humans with magnetic resonance angiography. JAMA. 1998;279:376.
Bartzokis G, Goldstein IB, Hance DB, Beckson M, Shapiro D, Lu PH, et al. The incidence of T2-weighted MR imaging signal abnormalities in the brain of cocaine-dependent patients is age-related and region-specific. AJNR Am J Neuroradiol. 1999;20:1628–35.
Bachi K, Mani V, Kaufman AE, Alie N, Goldstein RZ, Fayad ZA, et al. Imaging plaque inflammation in asymptomatic cocaine addicted individuals with simultaneous positron emission tomography/magnetic resonance imaging. World J Radiol. 2019;11:62–73.
Rogers RD, Everitt BJ, Baldacchino A, Blackshaw AJ, Swainson R, Wynne K, et al. Dissociable deficits in the decision-making cognition of chronic amphetamine abusers, opiate abusers, patients with focal damage to prefrontal cortex, and tryptophan-depleted normal volunteers: evidence for monoaminergic mechanisms. Neuropsychopharmacology. 1999;20:322–39.
Ersche KD, Fletcher PC, Lewis SJG, Clark L, Stocks-Gee G, London M, et al. Abnormal frontal activations related to decision-making in current and former amphetamine and opiate dependent individuals. Psychopharmacology. 2005;180:612–23.
De Pirro S, Galati G, Pizzamiglio L, Badiani A. The affective and neural correlates of heroin versus cocaine use in addiction are influenced by environmental setting but in opposite directions. J Neurosci. 2018;38:5182–95.
Dutra L, Stathopoulou G, Basden SL, Leyro TM, Powers MB, Otto MW. A meta-analytic review of psychosocial interventions for substance use disorders. AJP. 2008;165:179–87.
Carroll KM. A cognitive-behavioral approach: treating cocaine addiction. U.S. Department of Health and Human Services, National Institutes of Health, National Institute on Drug Abuse, Maryland, USA; 1998.
Zilverstand A, Parvaz MA, Moeller SJ, Goldstein RZ. Chapter 13—Cognitive interventions for addiction medicine: understanding the underlying neurobiological mechanisms. In: Ekhtiari H, Paulus MP, editors. Progress in Brain Research, vol. 224, Amsterdam: Elsevier; 2016. p. 285–304.
Bari A, Robbins TW. Inhibition and impulsivity: Behavioral and neural basis of response control. Prog Neurobiol. 2013;108:44–79.
Everitt BJ, Robbins TW. Neural systems of reinforcement for drug addiction: from actions to habits to compulsion. Nat Neurosci. 2005;8:1481–9.
Kober H, Mende-Siedlecki P, Kross EF, Weber J, Mischel W, Hart CL, et al. Prefrontal–striatal pathway underlies cognitive regulation of craving. PNAS. 2010;107:14811–6.
Zhao L-Y, Tian J, Wang W, Qin W, Shi J, Li Q, et al. The role of dorsal anterior cingulate cortex in the regulation of craving by reappraisal in smokers. PLOS One. 2012;7:e43598.
Suzuki S, Mell MM, O’Malley SS, Krystal JH, Anticevic A, Kober H. Regulation of craving and negative emotion in alcohol use disorder. Biol Psychiatry Cogn Neurosci Neuroimaging. 2020;5:239–50.
Parvaz MA, Malaker P, Zilverstand A, Moeller SJ, Alia-Klein N, Goldstein RZ. Attention bias modification in drug addiction: enhancing control of subsequent habits. PNAS. 2021;118:23.
DeVito EE, Worhunsky PD, Carroll KM, Rounsaville BJ, Kober H, Potenza MN. A preliminary study of the neural effects of behavioral therapy for substance use disorders. Drug Alcohol Depend. 2012;122:228–35.
DeVito EE, Dong G, Kober H, Xu J, Carroll KM, Potenza MN. Functional neural changes following behavioral therapies and disulfiram for cocaine dependence. Psychol Addict Behav. 2017;31:534–47.
Carter CS, van Veen V. Anterior cingulate cortex and conflict detection: an update of theory and data. Cogn Affect Behav Neurosci. 2007;7:367–79.
DeVito EE, Kober H, Carroll KM, Potenza MN. fMRI Stroop and behavioral treatment for cocaine-dependence: preliminary findings in methadone-maintained individuals. Addictive Behav. 2019;89:10–14.
Moeller SJ, Goldstein RZ. Impaired self-awareness in human addiction: deficient attribution of personal relevance. Trends Cogn Sci. 2014;18:635–41.
Wang A-L, Ruparel K, Loughead JW, Strasser AA, Blady SJ, Lynch KG, et al. Content matters: neuroimaging investigation of brain and behavioral impact of televised anti-tobacco public service announcements. J Neurosci. 2013;33:7420–7.
Chua HF, Liberzon I, Welsh RC, Strecher VJ. Neural correlates of message tailoring and self-relatedness in smoking cessation programming. Biol Psychiatry. 2009;65:165–8.
Chua HF, Ho SS, Jasinska AJ, Polk TA, Welsh RC, Liberzon I, et al. Self-related neural response to tailored smoking-cessation messages predicts quitting. Nat Neurosci. 2011;14:426–7.
Wilson SJ, Sayette MA, Fiez JA. Neural correlates of self-focused and other-focused strategies for coping with cigarette cue exposure. Psychol Addictive Behav. 2013;27:466–76.
Garland EL, Howard MO. Mindfulness-based treatment of addiction: current state of the field and envisioning the next wave of research. Addiction Sci Clin Pract. 2018;13:14.
Baer RA, Smith GT, Hopkins J, Krietemeyer J, Toney L. Using self-report assessment methods to explore facets of mindfulness. Assessment. 2006;13:27–45.
Froeliger B, Mathew AR, McConnell PA, Eichberg C, Saladin ME, Carpenter MJ, et al. Restructuring reward mechanisms in nicotine addiction: a pilot fMRI study of mindfulness-oriented recovery enhancement for cigarette smokers. Evid Based Complement Altern Med. 2017;2017:7018014.
Westbrook C, Creswell JD, Tabibnia G, Julson E, Kober H, Tindle HA. Mindful attention reduces neural and self-reported cue-induced craving in smokers. Soc Cogn Affect Neurosci. 2013;8:73–84.
Volkow ND, Li T-K. Drug addiction: the neurobiology of behaviour gone awry. Nat Rev Neurosci. 2004;5:963–70.
Cahill K, Lindson-Hawley N, Thomas KH, Fanshawe TR, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2016;5:CD006103.
Franklin T, Wang Z, Suh JJ, Hazan R, Cruz J, Li Y, et al. Effects of varenicline on smoking cue–triggered neural and craving responses. Arch Gen Psychiatry. 2011;68:516–26.
Culbertson CS, Bramen J, Cohen MS, London ED, Olmstead RE, Gan JJ, et al. Effect of bupropion treatment on brain activation induced by cigarette-related cues in smokers. Arch Gen Psychiatry. 2011;68:505.
Brody AL, Mandelkern MA, Lee G, Smith E, Sadeghi M, Saxena S, et al. Attenuation of cue-induced cigarette craving and anterior cingulate cortex activation in bupropion-treated smokers: a preliminary study. Psychiatry Res. 2004;130:269–81.
Johansson BA, Berglund M, Lindgren A. Efficacy of maintenance treatment with naltrexone for opioid dependence: a meta-analytical review. Addiction. 2006;101:491–503.
Srisurapanont M, Jarusuraisin N. Naltrexone for the treatment of alcoholism: a meta-analysis of randomized controlled trials. Int J Neuropsychopharmacol. 2005;8:267–80.
Dackis CA, Kampman KM, Lynch KG, Pettinati HM, O’Brien CP. A double-blind, placebo-controlled trial of modafinil for cocaine dependence. Neuropsychopharmacology. 2005;30:205–11.
Beck A, Pelz P, Lorenz RC, Charlet K, Geisel O, Heinz A, et al. Effects of high-dose baclofen on cue reactivity in alcohol dependence: a randomized, placebo-controlled pharmaco-fMRI study. Eur Neuropsychopharmacol. 2018;28:1206–16.
Myrick H, Li X, Randall PK, Henderson S, Voronin K, Anton RF. The effect of aripiprazole on cue-induced brain activation and drinking parameters in alcoholics. J Clin Psychopharmacol. 2010;30:365–72.
Logge WB, Morris RW, Baillie AJ, Haber PS, Morley KC. Baclofen attenuates fMRI alcohol cue reactivity in treatment-seeking alcohol dependent individuals. Psychopharmacology. 2019. https://doi.org/10.1007/s00213-019-05192-5.
Holla B, Karthik S, Biswal J, Viswanath B, Jayarajan D, Bharath RD, et al. Brain functional magnetic resonance imaging cue-reactivity can predict baclofen response in alcohol use disorders. Clin Psychopharmacol Neurosci. 2018;16:290–301.
Volkow ND, Fowler JS, Wang G-J. The addicted human brain viewed in the light of imaging studies: brain circuits and treatment strategies. Neuropharmacology. 2004;47:3–13.
Han DH, Kim SM, Choi JE, Min KJ, Renshaw PF. Adjunctive aripiprazole therapy with escitalopram in patients with co-morbid major depressive disorder and alcohol dependence: clinical and neuroimaging evidence. J Psychopharmacol. 2013;27:282–91.
Grodin EN, Ray LA. The use of functional magnetic resonance imaging to test pharmacotherapies for alcohol use disorder: a systematic review. Alcohol: Clin Exp Res. 2019;43:2038–56.
Liotti M, Mayberg HS. The role of functional neuroimaging in the neuropsychology of depression. J Clin Exp Neuropsychol. 2001;23:121–36.
Goldstein RZ, Woicik PA, Maloney T, Tomasi D, Alia-Klein N, Shan J, et al. Oral methylphenidate normalizes cingulate activity in cocaine addiction during a salient cognitive task. PNAS. 2010;107:16667–72.
Moeller SJ, Tomasi D, Honorio J, Volkow ND, Goldstein RZ. Dopaminergic involvement during mental fatigue in health and cocaine addiction. Transl Psychiatry. 2012;2:e176.
Moeller SJ, Honorio J, Tomasi D, Parvaz MA, Woicik PA, Volkow ND, et al. Methylphenidate enhances executive function and optimizes prefrontal function in both health and cocaine addiction. Cereb Cortex. 2014;24:643–53.
Moeller SJ, Konova AB, Tomasi D, Parvaz MA, Goldstein RZ. Abnormal response to methylphenidate across multiple fMRI procedures in cocaine use disorder: feasibility study. Psychopharmacology. 2016;233:2559–69.
Shi Z, Wang A-L, Jagannathan K, Fairchild VP, O’Brien CP, Childress AR, et al. Effects of extended-release naltrexone on the brain response to drug-related stimuli in patients with opioid use disorder. J Psychiatry Neurosci. 2018;43:254–61.
Luigjes J, Segrave R, de Joode N, Figee M, Denys D. Efficacy of invasive and non-invasive brain modulation interventions for addiction. Neuropsychol Rev. 2019;29:116–38.
Yuan K, Yu D, Bi Y, Wang R, Li M, Zhang Y, et al. The left dorsolateral prefrontal cortex and caudate pathway: new evidence for cue-induced craving of smokers. Hum Brain Mapp. 2017;38:4644–56.
Chen R, Classen J, Gerloff C, Celnik P, Wassermann EM, Hallett M, et al. Depression of motor cortex excitability by low‐frequency transcranial magnetic stimulation. Neurology. 1997;48:1398–403.
Siebner HR, Peller M, Willoch F, Minoshima S, Boecker H, Auer C, et al. Lasting cortical activation after repetitive TMS of the motor cortex: a glucose metabolic study. Neurology. 2000;54:956–63.
Amiaz R, Levy D, Vainiger D, Grunhaus L, Zangen A. Repeated high-frequency transcranial magnetic stimulation over the dorsolateral prefrontal cortex reduces cigarette craving and consumption. Addiction. 2009;104:653–60.
Trojak B, Meille V, Achab S, Lalanne L, Poquet H, Ponavoy E, et al. Transcranial magnetic stimulation combined with nicotine replacement therapy for smoking cessation: a randomized controlled trial. Brain Stimul. 2015;8:1168–74.
Su H, Zhong N, Gan H, Wang J, Han H, Chen T, et al. High frequency repetitive transcranial magnetic stimulation of the left dorsolateral prefrontal cortex for methamphetamine use disorders: a randomised clinical trial. Drug Alcohol Depend. 2017;175:84–91.
Bolloni C, Panella R, Pedetti M, Frascella AG, Gambelunghe C, Piccoli T, et al. Bilateral transcranial magnetic stimulation of the prefrontal cortex reduces cocaine intake: a pilot study. Front Psychiatry. 2016;7:133.
Nitsche MA, Paulus W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J Physiol. 2000;527:633–9.
Boggio PS, Liguori P, Sultani N, Rezende L, Fecteau S, Fregni F. Cumulative priming effects of cortical stimulation on smoking cue-induced craving. Neurosci Lett. 2009;463:82–86.
Fecteau S, Agosta S, Hone-Blanchet A, Fregni F, Boggio P, Ciraulo D, et al. Modulation of smoking and decision-making behaviors with transcranial direct current stimulation in tobacco smokers: a preliminary study. Drug Alcohol Depend. 2014;140:78–84.
da Silva MC, Conti CL, Klauss J, Alves LG, do Nascimento Cavalcante HM, Fregni F, et al. Behavioral effects of transcranial Direct Current Stimulation (tDCS) induced dorsolateral prefrontal cortex plasticity in alcohol dependence. J Physiol Paris. 2013;107:493–502.
Klauss J, Penido Pinheiro LC, Silva Merlo BL, Correia Santos G, de A, Fregni F, et al. A randomized controlled trial of targeted prefrontal cortex modulation with tDCS in patients with alcohol dependence. Int J Neuropsychopharmacol. 2014;17:1793–803.
Klauss J, Anders QS, Felippe LV, Nitsche MA, Nakamura-Palacios EM. Multiple sessions of transcranial direct current stimulation (tDCS) reduced craving and relapses for alcohol use: a randomized placebo-controlled trial in alcohol use disorder. Front Pharmacol. 2018;9:716.
Batista EK, Klauss J, Fregni F, Nitsche MA, Nakamura-Palacios EM A Randomized Placebo-Controlled Trial of Targeted Prefrontal Cortex Modulation with Bilateral tDCS in Patients with Crack-Cocaine Dependence. Int J Neuropsychopharmacol. 2015;18:pyv066.
de Almeida Ramos R, Taiar I, Trevizol AP, Shiozawa P, Cordeiro Q. Effect of a ten-day prefrontal transcranial direct current stimulation protocol for crack craving: a proof-of-concept trial. J ECT. 2016;32:e8.
Conti CL, Nakamura-Palacios EM. Bilateral transcranial direct current stimulation over dorsolateral prefrontal cortex changes the drug-cued reactivity in the anterior cingulate cortex of crack-cocaine addicts. Brain Stimul. 2014;7:130–2.
Gaudreault P-O, Sharma A, Datta A, Nakamura-Palacios EM, King S, Malaker P, et al. A double-blind sham-controlled phase 1 clinical trial of tDCS of the dorsolateral prefrontal cortex in cocaine inpatients: craving, sleepiness, and contemplation to change. Eur J Neurosci. 2021. https://doi.org/10.1111/ejn.15172.
Kim D-Y, Yoo S-S, Tegethoff M, Meinlschmidt G, Lee J-H. The inclusion of functional connectivity information into fMRI-based neurofeedback improves its efficacy in the reduction of cigarette cravings. J Cogn Neurosci. 2015;27:1552–72.
Canterberry M, Hanlon CA, Hartwell KJ, Li X, Owens M, LeMatty T, et al. Sustained reduction of nicotine craving with real-time neurofeedback: exploring the role of severity of dependence. Nicotine Tob Res. 2013;15:2120–4.
Hanlon CA, Hartwell KJ, Canterberry M, Li X, Owens M, LeMatty T, et al. Reduction of cue-induced craving through realtime neurofeedback in nicotine users: the role of region of interest selection and multiple visits. Psychiatry Res. 2013;213:79–81.
Karch S, Keeser D, Hümmer S, Paolini M, Kirsch V, Karali T, et al. Modulation of craving related brain responses using real-time fMRI in patients with alcohol use disorder. PLOS One. 2015;10:e0133034.
Martz ME, Hart T, Heitzeg MM, Peltier SJ. Neuromodulation of brain activation associated with addiction: a review of real-time fMRI neurofeedback studies. NeuroImage Clin. 2020;27:102350.
Corominas-Roso M, Ibern I, Capdevila M, Ramon R, Roncero C, Ramos-Quiroga JA. Benefits of EEG-neurofeedback on the modulation of impulsivity in a sample of cocaine and heroin long-term abstinent inmates: a pilot study. Int J Offender Ther Comp Criminol. 2020;64:1275–98.
Stewart JL, May AC, Paulus MP. Bouncing back: brain rehabilitation amid opioid and stimulant epidemics. NeuroImage Clin. 2019;24:102068.
Sokhadze TM, Cannon RL, Trudeau DL. EEG biofeedback as a treatment for substance use disorders: review, rating of efficacy, and recommendations for further research. Appl Psychophysiol Biofeedback. 2008;33:1–28.
Kirschner M, Sladky R, Haugg A, Stämpfli P, Jehli E, Hodel M, et al. Self-regulation of the dopaminergic reward circuit in cocaine users with mental imagery and neurofeedback. EBioMedicine. 2018;37:489–98.
Mayberg HS, Lozano AM, Voon V, McNeely HE, Seminowicz D, Hamani C, et al. Deep brain stimulation for treatment-resistant depression. Neuron. 2005;45:651–60.
Schlaepfer TE, Bewernick BH. Deep brain stimulation for major depression. Handb Clin Neurol. 2013;116:235–43.
Benabid AL. Deep brain stimulation for Parkinson’s disease. Curr Opin Neurobiol. 2003;13:696–706.
Wang TR, Moosa S, Dallapiazza RF, Elias WJ, Lynch WJ. Deep brain stimulation for the treatment of drug addiction. Neurosurg Focus. 2018;45:E11.
Heinze H-J, Heldmann M, Voges J, Hinrichs H, Marco-Pallares J, Hopf J-M, et al. Counteracting incentive sensitization in severe alcohol dependence using deep brain stimulation of the nucleus accumbens: clinical and basic science aspects. Front Hum Neurosci. 2009;3:22.
Kuhn J, Gründler TOJ, Bauer R, Huff W, Fischer AG, Lenartz D, et al. Successful deep brain stimulation of the nucleus accumbens in severe alcohol dependence is associated with changed performance monitoring. Addict Biol. 2011;16:620–3.
Müller UJ, Sturm V, Voges J, Heinze H-J, Galazky I, Heldmann M, et al. Successful treatment of chronic resistant alcoholism by deep brain stimulation of nucleus accumbens: first experience with three cases. Pharmacopsychiatry. 2009;42:288–91.
Gonçalves-Ferreira A, Couto FS, do, Campos AR, Neto LPL, Gonçalves-Ferreira D, Teixeira J. Deep brain stimulation for refractory cocaine dependence. Biol Psychiatry. 2016;79:e87–e89.
Kuhn J, Möller M, Treppmann JF, Bartsch C, Lenartz D, Gruendler TOJ, et al. Deep brain stimulation of the nucleus accumbens and its usefulness in severe opioid addiction. Mol Psychiatry. 2014;19:145–6.
Valencia-Alfonso C-E, Luigjes J, Smolders R, Cohen MX, Levar N, Mazaheri A, et al. Effective deep brain stimulation in heroin addiction: a case report with complementary intracranial electroencephalogram. Biol Psychiatry. 2012;71:e35–e37.
Wakeford AGP, Morin EL, Bramlett SN, Howell LL, Sanchez MM. A review of nonhuman primate models of early life stress and adolescent drug abuse. Neurobiol Stress. 2018;9:188–98.
Ersche KD, Meng C, Ziauddeen H, Stochl J, Williams GB, Bullmore ET, et al. Brain networks underlying vulnerability and resilience to drug addiction. Proc Natl Acad Sci USA. 2020;117:15253–61.
Nastase SA, Goldstein A, Hasson U. Keep it real: rethinking the primacy of experimental control in cognitive neuroscience. NeuroImage 2020;222:117254.
Agurto C, Norel R, Pietrowicz M, Parvaz M, Kinreich S, Bachi K, et al. Speech markers for clinical assessment of cocaine users. 2019 IEEE International Conference on Acoustics Speech and Signal Processing. 2019;2019:6391–4.
Gueguen MC, Schweitzer EM, Konova AB. Computational theory-driven studies of reinforcement learning and decision-making in addiction: what have we learned? Curr Opin Behav Sci. 2021;38:40–48.
Crummy EA, O’Neal TJ, Baskin BM, Ferguson SM. One is not enough: understanding and modeling polysubstance use. Front Neurosci. 2020;14:569.
Ekhtiari H, Tavakoli H, Addolorato G, Baeken C, Bonci A, Campanella S, et al. Transcranial electrical and magnetic stimulation (tES and TMS) for addiction medicine: A consensus paper on the present state of the science and the road ahead. Neurosci Biobehav Rev. 2019;104:118–40.
Funding
RZG is supported by grants from the National Institute on Drug Abuse (R01DA048301, R01DA041528, R01DA047851, 271201800035C) and the National Center for Complementary and Integrative Health (R01AT010627). CWB is supported by the National Institute on Drug Abuse Intramural Research Program.
Author information
Authors and Affiliations
Contributions
AOC, CWB, and RZG wrote the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ceceli, A.O., Bradberry, C.W. & Goldstein, R.Z. The neurobiology of drug addiction: cross-species insights into the dysfunction and recovery of the prefrontal cortex. Neuropsychopharmacol. 47, 276–291 (2022). https://doi.org/10.1038/s41386-021-01153-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41386-021-01153-9
This article is cited by
-
Incubation of methamphetamine craving in punishment-resistant individuals is associated with activation of specific gene networks in the rat dorsal striatum
Molecular Psychiatry (2024)
-
Assessment of rTMS treatment effects for methamphetamine addiction based on EEG functional connectivity
Cognitive Neurodynamics (2024)
-
Whole-brain white matter abnormalities in human cocaine and heroin use disorders: association with craving, recency, and cumulative use
Molecular Psychiatry (2023)
-
Addictive and other mental disorders: a call for a standardized definition of dual disorders
Translational Psychiatry (2022)
-
Prefrontal fNIRS-based clinical data analysis of brain functions in individuals abusing different types of drugs
Journal of Biomedical Semantics (2021)
