
Abstract
Purpose
We aimed to synthesize the evidence for an association between childhood maltreatment and body image disturbances in adulthood. Information on maltreatment subtypes and mediator variables was included to gain further insights into the mechanisms of the association. In addition, we aimed to examine the role of body image disturbances in the development of negative mental health outcomes associated with childhood maltreatment.
Methods
Based on a comprehensive search strategy, eligible studies were identified in PubMed, Scopus, and Web of Science. The eligibility assessment was performed by two reviewers, and 132 articles were studied full-text. To reduce heterogeneity, only non-clinical samples were included in the meta-analysis. A meta-regression was computed to examine the influence of maltreatment subtype on body image disturbances.
Results
Our results provide evidence for a robust association between childhood maltreatment and cognitive-affective body image, both in clinical and community samples. Included studies (N = 40) indicate that body image disturbances are especially pronounced in individuals suffering from Posttraumatic Stress Disorder (PTSD) after childhood maltreatment. The meta-analysis included 12 studies with a total of 15.481 participants, and indicates a small overall effect size (r = 0.21, 95% CI = [0.16, 0.26], p < .001). Meta-regression revealed no significant impact of maltreatment subtype in non-clinical samples.
Conclusion
Childhood maltreatment should be considered as a distal risk factor for the development of a negative cognitive-affective body image. We argue for future longitudinal studies which allow a better understanding of the pathways linking childhood maltreatment, body image disturbances and associated psychopathology.
Similar content being viewed by others

Introduction
A positive body image is a crucial factor for psychosocial functioning and subjective well-being (Cash & Fleming, 2002). Seeing the own body in a positive light has been described as essential for engagement in self-care behaviors (such as physical exercise or the use of sun protection; Andrew et al., 2016; Avalos et al., 2005), self-esteem (Williams et al., 2004), interpersonal confidence and social support (Thompson et al., 1999) as well as for sexual functioning (Gillen & Markey, 2019; Satinsky et al., 2012).
Conversely, a negative body image has been linked to poorer psychological adjustment and quality of life (Annunziata et al., 2012; Bullen et al., 2012; Cash & Fleming, 2002; Cash et al., 2004b). In non-clinical samples, body image disturbances and body-related shame have been found to be associated with negative health behaviors such as smoking and binge-drinking (King et al., 2005; Nelson et al., 2009), avoidance of health care services such as cancer screening (due to felt discomfort when urged to expose the body for examination) and lack of exercise (Mensinger et al., 2018; More et al., 2019; Ridolfi & Crowther, 2013).
These findings indicate the integral role of body image in mental and physical health. Nevertheless, methodological problems presently prevent a deeper understanding of the etiopathogenetic pathways that may result from a negative body image.
A major challenge in body image research is the broad conceptualization of the construct (Thompson, 2004; Thompson et al., 2012). In the literature, body image is referred to a variety of terms (often reducing the construct to one of its components) such as body esteem, body schema, body concern, appearance evaluation, appearance orientation, size perception accuracy, body satisfaction, weight satisfaction, and drive for muscularity or thinness (Grogan, 2010; Thompson et al., 1999). As conceptualized by Slade (1994), body image is more complex and comprises the mental representation of body size and shape, body-related feelings and behaviors. Body image development is thought to be influenced by biological as well as cultural factors (Slade, 1994; Slevec & Tiggemann, 2011). Reflecting the multidimensionality of the construct, it is commonly differentiated between perceptive, cognitive-affective and behavioral components of body image (Thompson et al., 1999). The perceptive component refers to the estimation of actual body size and shape. The cognitive-affective component consists of two subcomponents: the importance attributed to weight and shape and the appraisal of one’s own appearance (Cash et al., 2004a, b). A negative self-evaluation of the own body is referred to as body dissatisfaction (Cash & Pruzinsky, 1990). Control strategies (e.g., restricted eating) and avoidance behavior (e.g., wearing loose instead of tight-fitting clothing) are subsumed under the behavioral component. In this review, we focus on the cognitive-affective component of body image.
Due to the harmful impact of a negative body image on mental and physical health, a growing body of research focuses on risk factors for the development of body dissatisfaction. Internalization of beauty ideals and appearance-related social comparison (Carlson Jones, 2004; Fuller-Tyszkiewicz et al., 2019), self-objectification (Augustus-Horvath & Tylka, 2009; Slevec & Tiggemann, 2011), exposure to idealized media images and social media use (Fardouly & Vartanian, 2016; Hargreaves & Tiggemann, 2004), low self-esteem and weight-related teasing (Ata et al., 2007; Chen et al., 2007; Valois et al., 2019), heightened body mass (Barker & Galambos, 2003; Calzo et al., 2012), and deficits in social support (Gerner & Wilson, 2005; Stice & Whitenton, 2002) have been identified as risk factors.
Early on, observations of clinicians indicated that a history of childhood sexual abuse also constitutes a risk factor for the development of body image disturbances (Arvanitakis et al., 1993; Myers, 1989; Simonds, 1992). In view of a developmental perspective, it is plausible that severe violations of body boundaries in a sensitive period for the embodiment of personal identity and integrity like those caused by several subtypes of childhood maltreatment have persisting effects on the perception of the self and the own body (Arvanitakis et al., 1993; Kearney-Cooke & Striegel-Moore, 1994; Knafo, 2016; Young, 1992).
Childhood maltreatment is commonly defined as emotional, physical and sexual abuse, and emotional and physical neglect of a minor younger than 18 years by an adult or an older adolescent with pronounced maturational difference.
Any sexual contact with a child under the age of 18 years by an authority or care-taker, and sexual acts forced by violence or trickery have been defined as childhood sexual abuse (CSA) by Finkelhor (1984). Physical abuse (CPA) is commonly described as harmful acts towards a child such as overt violence and excessive punishment (including exposure to extreme temperature or poisoning), resulting in injury or risk of injury (Kelly, 1983; Malinosky-Rummell & Hansen, 1993). Emotional abuse (CEA) can be defined as adverse parental behavior leading to impairments in the child’s psychological functioning and emotional well-being such as verbal assaults, harsh criticism, rejection and ignoring (Bernstein et al., 2003; Thompson & Kaplan, 1996). Whereas the different types of abuse are characterized by harmful actions, neglect is defined as the omission of behavior essential for the child’s healthy development (Mennen et al., 2010). Physical neglect (CPN) constitutes a lack of parental supervision which puts the child in danger, and a failure to meet basic needs by providing food, health care, and shelter (Bernstein et al., 2003). Emotional neglect (CEN) has proved to be especially difficult to define and can be understood as emotional unresponsiveness and unavailability of the care-taker violating the child’s basic need for emotional nurturance (Glaser, 2011). Different kinds of childhood maltreatment frequently co-occur (Dong et al., 2004).
Considering the overlap as well as the specific characteristics of the five childhood maltreatment subtypes, the question arises whether initial clinical observations of body image disturbances in victims of sexual abuse can be generalized to all kind of maltreatment experiences.
In the identity disruption model, Vartanian et al. (2018) focus on early adversity as a broad construct including general negative experiences and childhood trauma. According to this conceptualization, early adversity includes experiences such as growing up in an unstable family environment as well as experiences of abuse and neglect (as depicted in Fig. 1). Vartanian et al. (2018) assume that such early adversity disturbs normal identity development, and that individuals who lack well-formed personal identity and self-concept clarity are especially vulnerable to sociocultural influences as they look for external sources in order to attain a stronger sense of self. Hence, individuals with experiences of early adversities are supposed to be especially vulnerable to sociocultural pressures like beauty standards and appearance feedback, internalization of the latter and engagement in social comparisons regarding their body. Internalization of beauty ideals and engagement in body-related social comparisons are thought to be interrelated and to lead to increased body dissatisfaction. According to the identity disruption model (Vartanian et al., 2018), body dissatisfaction is associated with restrained eating, bingeing, purging and compulsive exercise.

Theoretical considerations on the association between childhood maltreatment, body image and mental health issues. Different colors depict different potential mechanisms (mediation, moderation, simple association) linking the constructs. The path between CM and body image is assumed to be more complex, for a detailed description of the Identity disruption model please see Vartanian et al. (2018)
In empirical studies, body image disturbances following childhood maltreatment were observed not only in eating disorder patients (e.g., Grilo & Masheb, 2001; Rayworth et al., 2004), but in a variety of physical and mental health conditions such as PTSD (Dyer et al., 2015; Scheffers et al., 2017), borderline personality disorder (BPD; Dyer et al., 2013a, b; Haaf et al., 2001), major depressive disorder (Andrews, 1995; Csoboth et al., 2005), poor sexual functioning (Wenninger & Heiman, 1998), and obesity (Duncan et al., 2015).
To enhance the clinical benefits of these observations and to prevent the development of body image disturbances, it is crucial to understand the pathways linking childhood maltreatment, body image disturbances and mental health issues. As depicted in Fig. 1, body image may partially mediate (or in some cases even moderate) the association between childhood maltreatment and psychopathology, could be understood as associated symptom of specific disorders, or the association between body image and mental health could be observed simply because both constructs are negatively influenced by experiences of childhood maltreatment.
Evidence for body image alterations in individuals with a maltreatment history in non-clinical samples (e.g., Hunter, 1991; Kearney-Cooke & Ackard, 2000) supports the assumption that experiences of childhood maltreatment disturb body image development (independent of subsequent psychopathology).
In conclusion, childhood maltreatment occurs in a sensitive developmental period for the embodiment of personal identity and is supposed to disturb the latter (Krueger, 2002; Young, 1992). Individuals who lack well-formed personal identity might be especially vulnerable to sociocultural influences like beauty ideals and thus tend to develop body image disturbances (Vartanian et al., 2018). Whereas some childhood maltreatment subtypes affect the body directly (by causing pain and injury), others more prominently affect psychological functions such as the self-image and self-esteem. In empirical studies, body image alterations have been documented to occur after childhood maltreatment both in clinical and population samples. However, a systematic review of the evidence for the association between childhood maltreatment and cognitive-affective body image in adults is lacking.
The aims of this article are twofold. First, we will synthesize the present empirical evidence for the association between childhood maltreatment and cognitive-affective body image in clinical and community samples. This part of the review will especially try to answer the question whether all subtypes of childhood maltreatment are comparable in terms of their association with cognitive-affective body image or whether certain subtypes of childhood maltreatment must be considered specifically relevant in this regard. Secondly, we will analyze evidence for the potential etiopathogenetic pathways through which body image disturbances might develop and function after abuse, taking into account the methodological quality of the underlying studies. More specifically, we try to answer the question whether body image disturbances should be considered a causal factor, moderator, mediator or simply an associated symptom in pathogenetic models of the sequelae of childhood maltreatment.
Methods
This review and the including meta-analysis were performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009).
Data Sources
PubMed, Scopus, and Web of Science were searched for articles on childhood maltreatment (CM) and body image (allowing for results on associated keywords like body dissatisfaction, body esteem and bodily shame). Data bases were chosen based on relevance and coverage (Halladay et al., 2015; Visser et al., 2021). In addition, references of included studies were revised for further studies meeting the inclusion criteria.
Search Process
The data-base driven research was conducted in May and June 2019, the search term ("body image" OR "body dissatisfaction" OR "body esteem" OR "bod* shame" OR "drive for thinness" OR "drive for muscularity") AND ("child* maltreatment" OR "child* abuse") was applied. An update literature search was performed from April to May 5th 2020.
Inclusion and Exclusion Criteria
Quantitative studies on the association between cognitive-affective body image and childhood maltreatment (defined as sexual, physical or emotional abuse and emotional or physical neglect before the age of 18 years) in adults published in English between January 1990 and May 2020 were included in this review. Studies on lifetime sexual or physical abuse (including traumatic experiences in childhood and adulthood with no differentiation) were not included. Given the scarcity of research on this topic, studies primarily focusing on different outcomes of CM that also covered measures of body image (including body shame) were included as well.
Eligibility Assessment
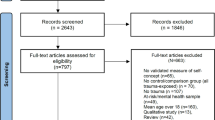
Out of 390 identified records, 131 articles were selected based on title and abstract. One additional article was selected from the reference list of one of the included articles. In the next step, the 132 selected articles were studied full-text in order to evaluate study quality and application of inclusion criteria. Each step of the eligibility assessment (screening of title and abstract, full-text analysis) was performed by two reviewers, discrepancies were resolved using consensus.
Data Extraction
Information was extracted from each included study on: (1) sample characteristics (including age, gender, diagnosis, type of childhood maltreatment and measure of the latter), (2) type of outcome measure (operationalization of body image) and (3) results of statistical analyses on the association between childhood maltreatment and body image (including further mediator or moderator variables).
Study Quality and Risk of Bias
Study quality and risk of bias were assessed independently by two reviewers applying the NIH Quality Assessment for Observational Cohort and Cross-sectional studies (National Heart Lung and Blood Institute, 2018). Discrepancies were resolved by consensus. Out of the 14 items of the NIH checklist, 9 items were applicable for the purpose of this review. Items regarding research question, sample description, participation rate, target population, sample size justification, measurement of exposure (CM) and outcome (body image), and inclusion of confounding variables were answered with yes, no, cannot determine (CD), not reported (NR) or not applicable (NA). Based on the literature, we predefined gender, age, and BMI as important confounding variables. Studies including various categories of CM received higher ratings on item 8 compared to studies focusing on one type (e.g., childhood sexual abuse). If customized measures of CM (without evidence for validity and reliability) were applied we rated item 9 as CD. Given the theoretical range of 0–9 points, we rated 7–9 points (> 80%) as good, 5,5–7 points (60–80%) as fair and less than 5,5 points (< 60%) as poor quality. This categorization is comparable with the approach of van Dalen et al. (2020).
Meta-analysis
In order to reduce heterogeneity, only studies including non-clinical samples and body dissatisfaction, body esteem or shape concerns as outcome variable were included in the meta-analysis. If data necessary for computation were missing, first authors were contacted and asked to provide additional data within four weeks (except for one study, for which author contact details could not be obtained). A total of 8 authors were contacted and response rate was 62.5%. In case of multiple assessments of body image in one study, only one result was entered into the analysis. Thereby, we focused on body dissatisfaction and shape concerns as outcome.
If necessary, effect sizes were converted based on the recommendations of the Campbell Methods Policy Note on Converting Between Effect Sizes (Polanin & Snilstveit, 2016) using the Practical Meta-Analysis Effect Size Calculator (Wilson, 2016). Publication bias was assessed by visual inspection of a funnel plot, Begg’s rank test (Begg & Mazumdar, 1994) and Egger’s regression (Egger et al., 1997). As I2-statistic indicated considerable heterogeneity with I2 = 71.7% (Melsen et al., 2014), a random-effects model was chosen. To assess whether the CM subtype influenced the association between CM and body dissatisfaction, a meta-regression with CM subtype as independent variable was computed in Stata version 15.1 by the “metareg” command (StataCorp, 2015). Due to differing assessment of CM in the included studies, 8 categories were entered in the analysis (1 = CEA, 2 = CPA, 3 = CSA, 4 = CEN, 5 = CPN, 6 = CM, 7 = CPA + CSA, 8 = neglect).
Results
Systematic Review
In total, 40 studies have been included in this review. 37 studies provide evidence for a significant association between childhood maltreatment and cognitive-affective body image and adjacent constructs such as body shame (six studies) and body esteem (four studies). The eligibility assessment is depicted in Fig. 2.

PRISMA Flow Diagram: Search and selection process
Sample Characteristics
19 of the included studies provide information on the association between childhood maltreatment and body image in non-clinical samples. These studies include community and university samples, but also focus on specific target populations such as pregnant women (Senior et al., 2005; Talmon & Ginzburg, 2019), prisoners (Milligan & Andrews, 2005), individuals with migration history (Nagaraj et al., 2019) and intimate piercings (Möller et al., 2018). 20 studies included clinical samples such as obese individuals (Grilo et al., 2006, 2005a, b; Rohde et al., 2008; Walsh et al., 2017), women diagnosed with sexual dysfunction (Kilimnik & Meston, 2016; Maseroli et al., 2018) or breast cancer (Salmon et al., 2006). In regard to mental health conditions associated with childhood maltreatment and body image disturbances, the reviewed studies mostly focus on PTSD or patients in trauma-related treatment (Borgmann et al., 2014; Dyer et al., 2015, 2013a, b; Scheffers et al., 2017; Wonderlich et al., 1996, 2001), eating disorders (Dunkley et al., 2010; Grilo & Masheb, 2001; Muehlenkamp et al., 2011; Treuer et al., 2005), and BPD (Dyer et al., 2015, 2013a, b). One study included a mixed psychiatric sample (Zlotnick et al., 1996). Bandini et al. (2011) studied individuals with male-to-female gender identity disorder (MtF GID).
In 27 of the included studies (including one study based on individuals with MtF GID), the association between childhood maltreatment and body image disturbances has been investigated in women only, and in ten of the remaining studies a balanced gender ratio could not be attained (resulting in a higher proportion of women). The three studies including balanced gender ratios point towards potential gender specific effects of CM on body image. The results of Brooke and Mussap (2013) indicate that abused men tend to develop a strong drive for thinness whereas abused women show a heightened drive for muscularity.
Please see Table S1 in the supplementary material for an overview of maltreatment subtype, body image measures, and sample characteristics of the included studies.
CM Subtypes
Multiple types of CM were assessed in 57.5% of the included studies. In the remaining studies, only one type of CM was assessed: 16 studies (40%) focused on CSA (including one study assessing incest only; Wonderlich et al., 1996) and one study assessed CEA only (Hund & Espelage, 2006). Overall, CSA was assessed most frequent in the included studies, followed by CPA and CEA and a comparatively low rate of the assessment of emotional and physical neglect (27.5%). The qualitative results indicate differing strength of association between childhood maltreatment subtypes and cognitive-affective body image.
Measures
As depicted in Table S1 in the supplementary material, included studies differ in sample size and applied measures. Whereas childhood maltreatment has been assessed mainly by the Childhood Trauma Questionnaire (CTQ; Bernstein & Fink, 1998), measures and operationalization of body image differ. Most frequently, the subscales body dissatisfaction and drive for thinness of The Eating Disorder Inventory (EDI; Garner et al., 1983), the Body Shape Questionnaire (BSQ; Cooper et al., 1987) and the subscales shape and weight concerns of the Eating Disorder Examination Questionnaire (EDE-Q; Fairburn & Beglin, 1994) have been chosen to assess aspects of cognitive-affective body image.
Study Design
In the majority of the included studies (92.5%), a cross-sectional study design was applied. Only three studies included longitudinal data. Grilo et al. (2006) compared pre- and 12 months post-operation outcomes in gastric bypass patients. Senior et al. (2005) included data from measurements at 18 and 32 weeks’ gestation to assess the influence of early traumatic experiences on maternal eating disorder symptoms. Andrews (1995) used longitudinal data to study the association between childhood maltreatment, body shame and depression.
Study Quality and Risk of Bias
The mean quality score of the included studies was 5.9 (range 3.5 – 8), which indicates a fair overall study quality. Common minor flaws were missing sample size justification, participation rate, and no specification of time period and place of recruitment. Overall, seven studies were considered of good quality, 22 of fair quality, and eleven of poor quality. The quality assessment is shown in Table S2 in the supplementary material.
Body Image as Mediator Variable
Initial support for the identity disruption model by Vartanian et al. (2018) was obtained. According to the model, early adversity leads to impaired self-concept clarity which makes individuals vulnerable to the internalization of sociocultural influences and the engagement in body comparison. This liability is assumed to lead to body dissatisfaction and associated disordered eating patterns (Vartanian et al., 2018). These assumptions are in line with the results of Preti et al. (2006), who identified body dissatisfaction as a mediator in the association between CSA and eating disorder symptoms.
According to Rohde et al. (2008) body dissatisfaction does not mediate the association between childhood maltreatment and adult obesity in middle-aged women.
Muehlenkamp et al. (2011) report an indirect effect of CM on non-suicidal self-injury (NSSI) via body dissatisfaction, low self-esteem, psychopathology, and dissociation.
Andrews (1995) found bodily shame to be a mediator between childhood maltreatment and chronic depression.
Talmon and Ginzburg (2019) suppose that the association between CM and fear of childbirth is partially mediated by self-objectification, disruption in body boundaries and body shame.
The Impact of Posttraumatic Stress Disorder (PTSD)
PTSD patients with a history of childhood maltreatment show pronounced alterations in body image, including body-related feelings of shame and disgust (Borgmann et al., 2014; Dyer et al., 2015, 2013a, b; Scheffers et al., 2017; Walsh et al., 2017). Notably, body-related emotions and impaired body experience were shown to correlate with PTSD severity, but not with trauma severity and dissociation within the PTSD group (Borgmann et al., 2014; Scheffers et al., 2017). Dyer et al. (2015) report more negative body-related feelings in PTSD patients compared to BPD patients (both with a history of CSA). According to Walsh et al. (2017), abuse survivors (CPA + CSA) suffering from PTSD report less body satisfaction compared to abuse survivors without PTSD (p = 0.015).
Meta-analysis
Study Characteristics
12 studies were included in the meta-analysis. These studies included only non-clinical samples and 15.481 participants in total, of which 95% were female. Sample size ranged from 38 to 7806, with a medium sample size of 1.290. Mean age of participants was 34.5 years with a range from 18 to 64 years. Study characteristics are described in Table 1. Please note that sample sizes mentioned above describe the sample size for which relevant data in regard to the present research question were available, whereas Table 1 depicts overall sample sizes.
Study Quality and Risk of Bias
The mean quality score of the included studies was 6 (range 3.5 – 8), which indicates a fair overall study quality. Overall, two studies were considered of good quality, eight of fair quality, and two of poor quality. The quality assessment is shown in Table 2.
Overall Effect Size
The results of the meta-analysis are depicted in Fig. 3. Results show a small overall effect size for the association between childhood maltreatment and body image (to be more precise: body esteem, body dissatisfaction or shape concerns) across included studies (r = 0.21, 95% CI = [0.16, 0.26], p < 0.001). As noted above, a high level of heterogeneity was observed (I2 = 71.7%, p < 0.001). The funnel plot was symmetric. Egger’s regression (p = 0.948) and Begg’s rank test (p = 0.166) were non-significant and indicated the absence of publication bias. Meta-regression indicated that CM subtype did not influence the association between CM and body dissatisfaction with F(7, 28) = 0.92, p = 0.5068. Sensitivity analyses were conducted by excluding OR studies (Rohde et al., 2008; Senior et al., 2005), which changed the pattern and indicated an effect of CM subtype [F(7, 21) = 4.48, p = 0.0034].

Forest plot: Results of the meta-analysis
Discussion
We systematically reviewed the literature on the association between childhood maltreatment and body image disturbances in adults. We aimed to answer the research question whether childhood maltreatment subtypes differ in their impact on body image and to analyze evidence for the potential etiopathogenetic pathways through which body image disturbances might develop and function after abuse and neglect.
Our results underline the relevance of body image disturbances in individuals with a history of childhood maltreatment. Of 40 studies included in the systematical review, 37 studies provide evidence for a significant association between childhood maltreatment and cognitive-affective body image. Meta-analysis revealed a small association between childhood maltreatment and body-related attitudes and feelings in non-clinical samples (r = 0.21, 95% CI = [0.16, 0.26], p < 0.001). Results of the meta-regression should be interpreted with caution as data might be correlated due to the frequent co-occurrence of different maltreatment subtypes (Dong et al., 2004). The cross-sectional design of the included studies impedes conclusions about etiopathogenetic pathways, though single studies indicate that body image disturbances might mediate the association between childhood maltreatment and eating disorders (Preti et al., 2006; Vartanian et al., 2018) and that PTSD is associated with pronounced alterations in body image, including body-related feelings of shame and disgust (Borgmann et al., 2014; Dyer et al., 2015, 2013a, b; Scheffers et al., 2017; Walsh et al., 2017).
Studies included in this review vary widely in terms of body image operationalization and target population. We reviewed data of individuals with physical health conditions such as obesity (Grilo et al., 2006, 2005a, b; Rohde et al., 2008; Walsh et al., 2017), sexual dysfunction (Kilimnik & Meston, 2016; Maseroli et al., 2018) and breast cancer (Salmon et al., 2006), as well as of individuals with mental health conditions such as PTSD (Borgmann et al., 2014; Dyer et al., 2015, 2013a, b; Scheffers et al., 2017; Wonderlich et al., 1996, 2001), eating disorders (Dunkley et al., 2010; Grilo & Masheb, 2001; Muehlenkamp et al., 2011; Treuer et al., 2005), and BPD (Dyer et al., 2015, 2013a, b). The non-clinical samples included community samples, but also specific samples such as pregnant women (Senior et al., 2005; Talmon & Ginzburg, 2019), prisoners (Milligan & Andrews, 2005), and individuals with migration history (Nagaraj et al., 2019) or intimate piercings (Möller et al., 2018). Evidence drawn from such diverse target populations underlines the integral role of body image in mental and physical health, and indicates its relevance beyond the field of eating disorders. Childhood maltreatment should be considered as a distal risk factor for the development of a negative cognitive-affective body image, both in clinical and community samples.
To our knowledge, this is the first review of the association between childhood maltreatment and body image disturbances in adults.
Slevec and Tiggemann (2011) reviewed risk factors for body dissatisfaction and disordered eating in middle-aged women and concluded that sexual and physical abuse are consistently associated with disordered eating, and to a lesser degree with body dissatisfaction. Overall, they identified BMI and appearance-related teasing as main risk factors for the development of body dissatisfaction. Their results also underline the relevance of aging anxiety, self-objectification, perfectionism, self-esteem and to some extent sociocultural pressures for body dissatisfaction in middle-aged women.
Mostly, review articles in the field do not include childhood maltreatment but focus on other risk factors for the development of body dissatisfaction. Meta-analytical findings indicate small overall effect-sizes for thin media exposure in both genders, ranging from r = 0.03 to r = 0.17 (Ferguson, 2013; Grabe et al., 2008; Groesz et al., 2002; Levine & Murnen, 2009). Fat talk (r = 0.34), weight-related teasing (r = 0.39) and appearance-related teasing (r = 0.32) seem to be especially relevant to body dissatisfaction development in adults (Menzel et al., 2010; Mills & Fuller-Tyszkiewicz, 2017). Interestingly, the association between fat talk and later body dissatisfaction becomes trivial (r = 0.08) in longitudinal studies (Mills & Fuller-Tyszkiewicz, 2017).
Our meta-analytical findings are limited, as we only included non-clinical samples. However, the influence of childhood maltreatment on body dissatisfaction seems to be comparable to other known risk factors such as thin media exposure and is observed despite the time gap between maltreatment and body image assessment. We know little about intervening processes, but our results indicate that the link between childhood maltreatment and body image disturbances in adulthood may not be close and direct, but rather calls for a more differentiated view.
When interpreting our results, the complexity of prolonged trauma sequelae should be kept in mind. We suppose body image disturbances to be a meaningful yet slightly understudied factor, but only one among many to influence the association between childhood maltreatment and mental and physical health. Family environment, emotion regulation and impulsivity have been proven to play an important role in the development of negative mental and physical health conditions in individuals with a history of childhood maltreatment (Bhandari et al., 2011; Brown et al., 2017; Michopoulos et al., 2015). In addition, the influential role of neurobiological mechanisms like alterations in HPA axis functioning in the aftermath of early traumatic experiences remains unquestioned (Heim et al., 2008; Tarullo & Gunnar, 2006; Teicher et al., 2003).
During the conduction of this review and meta-analysis, we faced several challenges that might be familiar to researchers in the field of body image research. First, the multidimensionality of the construct and the variety of terms body image is referred to in the literature represent a challenge in the synthesizing of findings (Grogan, 2010; Thompson et al., 1999). Whereas we chose a broad approach for the systematic review by including adjacent constructs such as body shame, we focused on only one facet of body image in the meta-analysis in order to enhance comparability of results. While the association between body image disturbances and childhood maltreatment is robust when both constructs are considered in their broadest sense, the specificity of the association between diverse aspects of body image and subtypes of childhood maltreatment remains unclear and calls for a more fine-grained scientific analysis. Second, a gold standard for the assessment of body image is lacking and as research in this area has been growing in the last decade, so has the variety of instruments (Thompson, 2004; Thompson et al., 2012). For example, Kling et al. (2019) identified 150 different body images measures applied in recent years.
Synthesizing data from studies that vary strongly in sample characteristics, body image operationalization and assessment instruments is challenging and might limit the validity of our results. For future research, we support claims for a consensus on measurement choices in the field of body image research (Cash & Pruzinsky, 2002; Krawczyk et al., 2012).
It is also important to note that gender ratio was unbalanced and resulted in a higher proportion of women in the vast majority of reviewed studies. The results of the remaining studies indicate that the association between childhood maltreatment and body image might be gender-specific. Whereas our conclusions are mainly based on female samples, the inclusion of men would be desirable for future research on the topic.
Despite the afore-mentioned limitations, our results argue for the relevance of body image disturbances in those having undergone childhood maltreatment, a notion that has implications not only in terms of future research perspectives but also for clinical intervention. It is noteworthy that the majority of frequently applied evidence-based trauma therapies do not include work on body image – even though body image seems to be susceptible to therapeutic change (Farrell et al., 2006; Guest et al., 2019; Scheffers et al., 2017). Not surprisingly, body image alterations were identified among the residual symptoms of evidence-based, trauma-focused psychotherapies by Larsen et al. (2019). First results on the efficacy of body-related therapy adjacent to trauma-focused psychotherapy in women with a history of childhood sexual abuse are promising (Price, 2005). Body-related interventions seem to enhance the frequently reported low self-care of traumatized patients (Felitti et al., 1998); potentially leading to more health-conscious behaviors. Given the influential role of body image on quality of life and psychosocial functioning (Cash et al., 2004a, b; Scheffers et al., 2017), we suggest to include work on body image in therapeutic approaches focusing on maltreatment survivors.
References
Andrew, R., Tiggemann, M., & Clark, L. (2016). Positive body image and young women’s health: Implications for sun protection, cancer screening, weight loss and alcohol consumption behaviours. Journal of Health Psychology, 21(1), 28–39. https://doi.org/10.1177/1359105314520814
Andrews, B. (1995). Bodily shame as a mediator between abusive experiences and depression. Journal of Abnormal Psychology, 104, 277–285.
Annunziata, M. A., Giovannini, L., & Muzzatti, B. (2012). Assessing the body image: Relevance, application and instruments for oncological settings. Supportive Care in Cancer, 20(5), 901–907. https://doi.org/10.1007/s00520-011-1339-x
Arvanitakis, K., Jodoin, R. M., Lester, E. P., Lussier, A., & Robertson, B. M. (1993). Early sexual abuse and nightmares in the analysis of adults. The Psychoanalytic Quarterly, 62(4), 572–587.
Ata, R. N., Ludden, A. B., & Lally, M. M. (2007). The effects of gender and family, friend, and media influences on eating behaviors and body image during adolescence. Journal of Youth and Adolescence, 36(8), 1024–1037. https://doi.org/10.1007/s10964-006-9159-x
Augustus-Horvath, C. L., & Tylka, T. L. (2009). A test and extension of objectification theory as it predicts disordered eating: Does women’s age matter? Journal of Counseling Psychology, 56(2), 253–265. https://doi.org/10.1037/a0014637
Avalos, L., Tylka, T. L., & Wood-Barcalow, N. (2005). The Body Appreciation Scale: Development and psychometric evaluation. Body Image, 2(3), 285–297. https://doi.org/10.1016/j.bodyim.2005.06.002
Bandini, E., Fisher, A. D., Ricca, V., Ristori, J., Meriggiola, M. C., Jannini, E. A., & Maggi, M. (2011). Childhood maltreatment in subjects with male-to-female gender identity disorder. International Journal of Impotence Research, 23(6), 276–285. https://doi.org/10.1038/ijir.2011.39
Barker, E. T., & Galambos, N. L. (2003). Body dissatisfaction of adolescent girls and boys: Risk and resource factors. The Journal of Early Adolescence, 23(2), 141–165. https://doi.org/10.1177/0272431603023002002
Begg, C. B., & Mazumdar, M. (1994). Operating characteristics of a rank correlation test for publication bias. Biometrics, 50(4), 1088–1101.
Bernstein, D. P., & Fink, L. (1998). Childhood Trauma Questionnaire: A retrospective self-report. Psychological Corporation.
Bernstein, D. P., Stein, J. A., Newcomb, M. D., Walker, E., Pogge, D., Ahluvalia, T., & Zule, W. (2003). Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse & Neglect, 27(2), 169–190. https://doi.org/10.1016/s0145-2134(02)00541-0
Bhandari, S., Winter, D., Messer, D., & Metcalfe, C. (2011). Family characteristics and long-term effects of childhood sexual abuse. British Journal of Clinical Psychology, 50(4), 435–451. https://doi.org/10.1111/j.2044-8260.2010.02006.x
Bifulco, A., Bernazzani, O., Moran, P. M., & Jacobs, C. (2005). The childhood experience of care and abuse questionnaire (CECA.Q): Validation in a community series. British Journal of Clinical Psychology, 44(4), 563–581. https://doi.org/10.1348/014466505X35344
Borgmann, E., Kleindienst, N., Vocks, S., & Dyer, A. S. (2014). Standardized mirror confrontation: Body-related emotions, cognitions and level of dissociation in patients with Posttraumatic Stress Disorder after childhood sexual abuse. Borderline Personality Disorder and Emotion Dysregulation, 1, 10. https://doi.org/10.1186/2051-6673-1-10
Brooke, L., & Mussap, A. J. (2013). Brief report: Maltreatment in childhood and body concerns in adulthood. Journal of Health Psychology, 18(5), 620–626. https://doi.org/10.1177/1359105312454036
Brown, S., Mitchell, T. B., Fite, P. J., & Bortolato, M. (2017). Impulsivity as a moderator of the associations between child maltreatment types and body mass index. Child Abuse & Neglect, 67, 137–146. https://doi.org/10.1016/j.chiabu.2017.02.029
Brown, T. A., Cash, T. F., & Mikulka, P. J. (1990). Attitudinal body-image assessment: Factor analysis of the Body-Self Relations Questionnaire. Journal of Personality Assessment, 55(1–2), 135–144. https://doi.org/10.1080/00223891.1990.9674053
Bullen, T. L., Sharpe, L., Lawsin, C., Patel, D. C., Clarke, S., & Bokey, L. (2012). Body image as a predictor of psychopathology in surgical patients with colorectal disease. Journal of Psychosomatic Research, 73(6), 459–463. https://doi.org/10.1016/j.jpsychores.2012.08.010
Calzo, J. P., Sonneville, K. R., Haines, J., Blood, E. A., Field, A. E., & Austin, S. B. (2012). The development of associations among body mass index, body dissatisfaction, and weight and shape concern in adolescent boys and girls. Journal of Adolescent Health, 51(5), 517–523. https://doi.org/10.1016/j.jadohealth.2012.02.021
Carlson Jones, D. (2004). Body image among adolescent girls and boys: A longitudinal study. Developmental Psychology, 40(5), 823–835. https://doi.org/10.1037/0012-1649.40.5.823
Cash, T. F., & Fleming, E. C. (2002). The impact of body image experiences: Development of the body image quality of life inventory. International Journal of Eating Disorders, 31(4), 455–460. https://doi.org/10.1002/eat.10033
Cash, T. F., Melnyk, S. E., & Hrabosky, J. I. (2004a). The assessment of body image investment: An extensive revision of the Appearance Schemas Inventory. International Journal of Eating Disorders, 35(3), 305–316. https://doi.org/10.1002/eat.10264
Cash, T. F., & Pruzinsky, T. (1990). Body images: Development, deviance, and change. Guilford Press.
Cash, T. F., & Pruzinsky, T. (2002). Future challenges for body image theory, research, and clinical practice. In T. F. Cash & T. Pruzinsky (Eds.), Body Images: A handbook of Theory, Research, and Clinical Practice (pp. 509–516). Guilford Press.
Cash, T. F., Thériault, J., & Annis, N. M. (2004b). Body image in an interpersonal context: Adult attachment, fear of intimacy, and social anxiety. Journal of Social and Clinical Psychology, 23(1), 89–103. https://doi.org/10.1521/jscp.23.1.89.26987
Chen, H., Gao, X., & Jackson, T. (2007). Predictive models for understanding body dissatisfaction among young males and females in China. Behaviour Research and Therapy, 45(6), 1345–1356. https://doi.org/10.1016/j.brat.2006.09.015
Cooper, P. J., Taylor, M. J., Cooper, Z., & Fairburn, C. G. (1987). The development and validation of the Body Shape Questionnaire. International Journal of Eating Disorders, 6(4), 485–494.
Csoboth, C. T., Birkás, E., & Purebl, G. (2005). Living in fear of experiencing physical and sexual abuse is associated with severe depressive symptomatology among young women. Journal of Women’s Health, 14(5), 441–448. https://doi.org/10.1089/jwh.2005.14.441
Derogatis, L. R., & Melisaratos, N. (1979). The DSFI: A multidimensional measure of sexual functioning. Journal of Sex & Marital Therapy, 5(3), 244–281. https://doi.org/10.1080/00926237908403732
Dong, M., Anda, R. F., Felitti, V. J., Dube, S. R., Williamson, D. F., Thompson, T. J., & Giles, W. H. (2004). The interrelatedness of multiple forms of childhood abuse, neglect, and household dysfunction. Child Abuse & Neglect, 28(7), 771–784. https://doi.org/10.1016/j.chiabu.2004.01.008
Duncan, A. E., Sartor, C. E., Jonson-Reid, M., Munn-Chernoff, M. A., Eschenbacher, M. A., Diemer, E. W., & Heath, A. C. (2015). Associations between body mass index, post-traumatic stress disorder, and child maltreatment in young women. Child Abuse & Neglect, 45, 154–162. https://doi.org/10.1016/j.chiabu.2015.02.007
Dunkley, D. M., Masheb, R. M., & Grilo, C. M. (2010). Childhood maltreatment, depressive symptoms, and body dissatisfaction in patients with binge eating disorder: The mediating role of self-criticism. International Journal of Eating Disorders, 43(3), 274–281. https://doi.org/10.1002/eat.20796
Dyer, A. S., Borgmann, E., Feldmann, R. E., Kleindienst, N., Priebe, K., Bohus, M., & Vocks, S. (2013a). Body image disturbance in patients with borderline personality disorder: Impact of eating disorders and perceived childhood sexual abuse. Body Image, 10(2), 220–225. https://doi.org/10.1016/j.bodyim.2012.12.007
Dyer, A. S., Borgmann, E., Kleindienst, N., Feldmann, R. E., Vocks, S., & Bohus, M. (2013b). Body image in patients with posttraumatic stress disorder after childhood sexual abuse and co-occurring eating disorder. Psychopathology, 46(3), 186–191. https://doi.org/10.1159/000341590
Dyer, A. S., Feldmann, R. E., & Borgmann, E. (2015). Body-related emotions in posttraumatic stress disorder following childhood sexual abuse. Journal of Child Sexual Abuse, 24(6), 627–640. https://doi.org/10.1080/10538712.2015.1057666
Egger, M., Smith, G. D., Schneider, M., & Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. BMJ, 315(7109), 629–634. https://doi.org/10.1136/bmj.315.7109.629
Eubanks, J. R., Kenkel, M. Y., & Gardner, R. M. (2006). Body-size perception, body-esteem, and parenting history in college women reporting a history of child abuse. Perceptual and Motor Skills, 102(2), 485–497. https://doi.org/10.2466/pms.102.2.485-497
Fairburn, C. G., & Beglin, S. J. (1994). Assessment of eating disorders: Interview or self-report questionnaire? International Journal of Eating Disorders, 16(4), 363–370.
Fardouly, J., & Vartanian, L. R. (2016). Social media and body image concerns: Current research and future directions. Current Opinion in Psychology, 9, 1–5. https://doi.org/10.1016/j.copsyc.2015.09.005
Farrell, C., Shafran, R., & Lee, M. (2006). Empirically evaluated treatments for body image disturbance: A review. European Eating Disorders Review, 14(5), 289–300. https://doi.org/10.1002/erv.693
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/s0749-3797(98)00017-8
Ferguson, C. J. (2013). In the eye of the beholder: Thin-ideal media affects some, but not most, viewers in a meta-analytic review of body dissatisfaction in women and men. Psychology of Popular Media Culture, 2(1), 20–37. https://doi.org/10.1037/a0030766
Finkelhor, D. (1984). Child Sexual Abuse: New Theory and Research. Free Press.
Franzoi, S. L., & Shields, S. A. (1984). The Body Esteem Scale: Multidimensional structure and sex differences in a college population. Journal of Personality Assessment, 48(2), 173–178. https://doi.org/10.1207/s15327752jpa4802_12
Fuller-Tyszkiewicz, M., Chhouk, J., McCann, L. -A., Urbina, G., Vuo, H., Krug, I., & Richardson, B. (2019). Appearance comparison and other appearance-related influences on body dissatisfaction in everyday life. Body Image, 28, 101–109. https://doi.org/10.1016/j.bodyim.2019.01.002
Garner, D. M. (1991). The Eating Disorder Inventory-2: Professional manual. Odessa, FL: Psychological Assessment Resources.
Garner, D. M. (2004). The Eating Disorder Inventory-3: Professional manual. Odessa, FL: Psychological Assessment Resources.
Garner, D. M., Olmsted, M. P., Bohr, Y., & Garfinkel, P. E. (1982). The Eating Attitudes Test: Psychometric features and clinical correlates. Psychological Medicine, 12(4), 871–878. https://doi.org/10.1017/s0033291700049163
Garner, D. M., Olmstead, M. P., & Polivy, J. (1983). Development and validation of a multidimensional Eating Disorder Inventory for anorexia nervosa and bulimia. International Journal of Eating Disorders, 2(2), 15–34. https://doi.org/10.1002/1098-108X(198321)2:2%3c15::AID-EAT2260020203%3e3.0.CO;2-6
Gerner, B., & Wilson, P. H. (2005). The relationship between friendship factors and adolescent girls’ body image concern, body dissatisfaction, and restrained eating. International Journal of Eating Disorders, 37(4), 313–320. https://doi.org/10.1002/eat.20094
Gillen, M. M., & Markey, C. H. (2019). A review of research linking body image and sexual well-being. Body Image, 31, 294–301. https://doi.org/10.1016/j.bodyim.2018.12.004
Glaser, D. (2011). How to deal with emotional abuse and neglect: Further development of a conceptual framework (FRAMEA). Child Abuse & Neglect, 35(10), 866–875. https://doi.org/10.1016/j.chiabu.2011.08.002
Grabe, S., Ward, L. M., & Hyde, J. S. (2008). The role of the media in body image concerns among women: A meta-analysis of experimental and correlational studies. Psychological Bulletin, 134(3), 460–476. https://doi.org/10.1037/0033-2909.134.3.460
Grilo, C. M., & Masheb, R. M. (2001). Childhood psychological, physical, and sexual maltreatment in outpatients with binge eating disorder: Frequency and associations with gender, obesity, and eating-related psychopathology. Obesity Research, 9(5), 320–325. https://doi.org/10.1038/oby.2001.40
Grilo, C. M., Masheb, R. M., Brody, M., Burke-Martindale, C. H., & Rothschild, B. S. (2005a). Binge eating and self-esteem predict body image dissatisfaction among obese men and women seeking bariatric surgery. International Journal of Eating Disorders, 37(4), 347–351. https://doi.org/10.1002/eat.20130
Grilo, C. M., Masheb, R. M., Brody, M., Toth, C., Burke-Martindale, C. H., & Rothschild, B. S. (2005b). Childhood maltreatment in extremely obese male and female bariatric surgery candidates. Obesity Research, 13(1), 123–130. https://doi.org/10.1038/oby.2005.16
Grilo, C. M., White, M. A., Masheb, R. M., Rothschild, B. S., & Burke-Martindale, C. H. (2006). Relation of childhood sexual abuse and other forms of maltreatment to 12-month postoperative outcomes in extremely obese gastric bypass patients. Obesity Surgery, 16(4), 454–460. https://doi.org/10.1381/096089206776327288
Groesz, L. M., Levine, M. P., & Murnen, S. K. (2002). The effect of experimental presentation of thin media images on body satisfaction: A meta-analytic review. International Journal of Eating Disorders, 31(1), 1–16. https://doi.org/10.1002/eat.10005
Grogan, S. (2010). Promoting positive body image in males and females: Contemporary issues and future directions. Sex Roles, 63(9–10), 757–765. https://doi.org/10.1007/s11199-010-9894-z
Guest, E., Costa, B., Williamson, H., Meyrick, J., Halliwell, E., & Harcourt, D. (2019). The effectiveness of interventions aiming to promote positive body image in adults: A systematic review. Body Image, 30, 10–25. https://doi.org/10.1016/j.bodyim.2019.04.002
Haaf, B., Pohl, U., Deusinger, I. M., & Bohus, M. (2001). Examination of body concept of female patients with borderline personality disorder. Psychotherapie, Psychosomatik, Medizinische Psychologie, 51(6), 246–254. https://doi.org/10.1055/s-2001-14302
Halladay, C. W., Trikalinos, T. A., Schmid, I. T., Schmid, C. H., & Dahabreh, I. J. (2015). Using data sources beyond PubMed has a modest impact on the results of systematic reviews of therapeutic interventions. Journal of Clinical Epidemiology, 68(9), 1076–1084.
Hargreaves, D. A., & Tiggemann, M. (2004). Idealized media images and adolescent body image: “Comparing” boys and girls. Body Image, 1(4), 351–361. https://doi.org/10.1016/j.bodyim.2004.10.002
Heim, C., Newport, D. J., Mletzko, T., Miller, A. H., & Nemeroff, C. B. (2008). The link between childhood trauma and depression: Insights from HPA axis studies in humans. Psychoneuroendocrinology, 33(6), 693–710. https://doi.org/10.1016/j.psyneuen.2008.03.008
Hund, A. R., & Espelage, D. L. (2006). Childhood emotional abuse and disordered eating among undergraduate females: Mediating influence of alexithymia and distress. Child Abuse & Neglect, 30(4), 393–407. https://doi.org/10.1016/j.chiabu.2005.11.003
Hunter, J. A. (1991). A comparison of the psychosocial maladjustment of adult males and females sexually molested as children. Journal of Interpersonal Violence, 6(2), 205–217. https://doi.org/10.1177/088626091006002005
Jenkins, P. E., Meyer, C., & Blissett, J. M. (2013). Childhood abuse and eating psychopathology: The mediating role of core beliefs. Journal of Aggression, Maltreatment & Trauma, 22(3), 248–261. https://doi.org/10.1080/10926771.2013.741665
Kearney-Cooke, A., & Ackard, D. M. (2000). The effects of sexual abuse on body image, self-image, and sexual activity of women. Journal of Gender-Specific Medicine, 3(6), 54–60.
Kearney-Cooke, A., & Striegel-Moore, R. H. (1994). Treatment of childhood sexual abuse in anorexia nervosa and bulimia nervosa: A feminist psychodynamic approach. International Journal of Eating Disorders, 15(4), 305–319. https://doi.org/10.1002/eat.2260150402
Kelly, J. A. (1983). Treating child-abusive families: Intervention based on skills-training principles. Plenum Press.
Kilimnik, C. D., & Meston, C. M. (2016). Role of body esteem in the sexual excitation and inhibition responses of women with and without a history of childhood sexual abuse. The Journal of Sexual Medicine, 13(11), 1718–1728. https://doi.org/10.1016/j.jsxm.2016.09.004
King, T. K., Matacin, M., White, K. S., & Marcus, B. H. (2005). A prospective examination of body image and smoking cessation in women. Body Image, 2(1), 19–28. https://doi.org/10.1016/j.bodyim.2005.01.003
Kleindienst, N., Priebe, K., Borgmann, E., Cornelisse, S., Krüger, A., Ebner-Priemer, U., & Dyer, A. (2014). Body Self-Evaluation and Physical Scars in Patients with Borderline Personality Disorder: An Observational Study. Borderline Personality Disorder and Emotional Dysregulation, 1, 2. https://doi.org/10.1186/2051-6673-1-2
Kling, J., Kwakkenbos, L., Diedrichs, P. C., Rumsey, N., Frisén, A., Brandão, M. P., & Fitzgerald, A. (2019). Systematic review of body image measures. Body Image, 30, 170–211. https://doi.org/10.1016/j.bodyim.2019.06.006
Knafo, H. (2016). The development of body image in school-aged girls: A review of the literature from sociocultural, social learning theory, psychoanalytic, and attachment theory perspectives. The New School Psychology Bulletin, 13(2), 1–16.
Krawczyk, R., Menzel, J., & Thompson, J. K. (2012). Methodological issues in the study of body image and appearance. In N. Rumsey & D. Harcourt (Eds.), The Oxford handbook of the psychology of appearance (pp. 605–619). Oxford University Press.
Krueger, D. W. (2002). Psychodynamic perspectives on body image. In T. F. Cash & T. Pruzinsky (Eds.), Body image: A handbook of theory, research, and clinical practice (pp. 30–37). Guilford Press.
Larsen, S. E., Fleming, C. J. E., & Resick, P. A. (2019). Residual symptoms following empirically supported treatment for PTSD. Psychological Trauma: Theory, Research, Practice and Policy, 11(2), 207–215. https://doi.org/10.1037/tra0000384
Levine, M. P., & Murnen, S. K. (2009). “Everybody knows that mass media are/are not [pick one] a cause of eating disorders”: A critical review of evidence for a causal link between media, negative body image, and disordered eating in females. Journal of Social and Clinical Psychology, 28(1), 9–42. https://doi.org/10.1521/jscp.2009.28.1.9
Mahtani, S., Hasking, P., & Melvin, G. A. (2019). Shame and Non-suicidal Self-injury: Conceptualization and Preliminary Test of a Novel Developmental Model among Emerging Adults. Journal of Youth and Adolescence, 48(4), 753–770. https://doi.org/10.1007/s10964-018-0944-0
Malinosky-Rummell, R., & Hansen, D. J. (1993). Long-term consequences of childhood physical abuse. Psychological Bulletin, 114(1), 68–79. https://doi.org/10.1037/0033-2909.114.1.68
Maseroli, E., Scavello, I., Campone, B., Di Stasi, V., Cipriani, S., Felciai, F., & Vignozzi, L. (2018). Psychosexual Correlates of Unwanted Sexual Experiences in Women Consulting for Female Sexual Dysfunction According to Their Timing Across the Life Span. Journal of Sexual Medicine, 15(12), 1739–1751. https://doi.org/10.1016/j.jsxm.2018.10.004
McCreary, D. R. (2007). The drive for muscularity scale: Description, psychometrics, and research findings. In J. K. Thompson & G. Cafri (Eds.), The Muscular Ideal: Psychological, Social, and Medical Perspectives (pp. 87–106). American Psychological Association.
Melsen, W. G., Bootsma, M. C. J., Rovers, M. M., & Bonten, M. J. M. (2014). The effects of clinical and statistical heterogeneity on the predictive values of results from meta-analyses. Clinical Microbiology and Infection, 20(2), 123–129. https://doi.org/10.1111/1469-0691.12494
Mendelson, B. K., & White, D. R. (1982). Relation between body-esteem and self-esteem of obese and normal children. Perceptual and Motor Skills, 54(3), 899–905. https://doi.org/10.2466/pms.1982.54.3.899
Mennen, F. E., Kim, K., Sang, J., & Trickett, P. K. (2010). Child neglect: Definition and identification of youth’s experiences in official reports of maltreatment. Child Abuse & Neglect, 34(9), 647–658. https://doi.org/10.1016/j.chiabu.2010.02.007
Mensinger, J. L., Tylka, T. L., & Calamari, M. E. (2018). Mechanisms underlying weight status and healthcare avoidance in women: A study of weight stigma, body-related shame and guilt, and healthcare stress. Body Image, 25, 139–147. https://doi.org/10.1016/j.bodyim.2018.03.001
Menzel, J. E., Schaefer, L. M., Burke, N. L., Mayhew, L. L., Brannick, M. T., & Thompson, J. K. (2010). Appearance-related teasing, body dissatisfaction, and disordered eating: A meta-analysis. Body Image, 7(4), 261–270. https://doi.org/10.1016/j.bodyim.2010.05.004
Michopoulos, V., Powers, A., Moore, C., Villarreal, S., Ressler, K. J., & Bradley, B. (2015). The mediating role of emotion dysregulation and depression on the relationship between childhood trauma exposure and emotional eating. Appetite, 91, 129–136. https://doi.org/10.1016/j.appet.2015.03.036
Milligan, R. -J., & Andrews, B. (2005). Suicidal and other self-harming behaviour in offender women: The role of shame, anger and childhood abuse. Legal and Criminological Psychology, 10(1), 13–25. https://doi.org/10.1348/135532504x15439
Mills, J., & Fuller-Tyszkiewicz, M. (2017). Fat talk and body image disturbance: A systematic review and meta-analysis. Psychology of Women Quarterly, 41(1), 114–129. https://doi.org/10.1177/0361684316675317
Milner, J. S., Robertson, K. R., & Rogers, D. L. (1990). Childhood history of abuse and adult child abuse potential. Journal of Family Violence, 5(1), 15–34. https://doi.org/10.1007/BF00979136
Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Annals of Internal Medicine, 151(4), 264–269. https://doi.org/10.7326/0003-4819-151-4-200908180-00135
Möller, J., Peregrinova, L., Badde, S., Oddo, S., Unterhorst, K., & Stirn, A. (2018). Childhood abuse and neglect in intimately pierced individuals. International Journal of Culture and Mental Health, 11(3), 237–247. https://doi.org/10.1080/17542863.2017.1362448
More, K. R., Phillips, L. A., & Eisenberg Colman, M. H. (2019). Evaluating the potential roles of body dissatisfaction in exercise avoidance. Body Image, 28, 110–114. https://doi.org/10.1016/j.bodyim.2019.01.003
Muehlenkamp, J. J. (2012). Body regard in nonsuicidal self-injury: Theoretical explanations and treatment directions. Journal of Cognitive Psychotherapy, 26(4), 331–347. https://doi.org/10.1891/0889-8391.26.4.331
Muehlenkamp, J. J., Claes, L., Smits, D., Peat, C. M., & Vandereycken, W. (2011). Non-suicidal self-injury in eating disordered patients: A test of a conceptual model. Psychiatry Research, 188(1), 102–108. https://doi.org/10.1016/j.psychres.2010.12.023
Myers, M. F. (1989). Men sexually assaulted as adults and sexually abused as boys. Archives of Sexual Behavior, 18(3), 203–215. https://doi.org/10.1007/BF01543195
Nagaraj, N. C., Vyas, A. N., & McDonnell, K. A. (2019). Is There a Link Between Childhood Family Violence and Adult Health? Understanding Family Violence Amongst South Asian American Women. Journal of Immigrant and Minority Health, 21(5), 978–1003. https://doi.org/10.1007/s10903-018-0829-z
National Heart Lung and Blood Institute (NIH) (2018). Study quality assessment tools. Retrieved from https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
Nelson, M. C., Lust, K., Story, M., & Ehlinger, E. (2009). Alcohol use, eating patterns, and weight behaviors in a university population. American Journal of Health Behavior, 33(3), 227–237. https://doi.org/10.5993/ajhb.33.3.1
Nijenhuis, E. R. S., Van der Hart, O., & Kruger, K. (2002). The psychometric characteristics of the Traumatic Experiences Checklist (TEC): First findings among psychiatric outpatients. Clinical Psychology & Psychotherapy, 9(3), 200–210. https://doi.org/10.1002/cpp.332
Pöhlmann, K., Thiel, P., & Joraschky, P. (2008). Development and validation of the Dresden Body Image Inventory (Dresdner Körperbildfragebogen; DKB-35). In P. Joraschky, H. Lausberg, K. Pöhlmann, & F. Röhricht (Eds.), Body-Orientated Diagnostic and Psychotherapy in Patients with Eating Disorders (pp. 57–72). Psychosozial-Verlag.
Polanin, J. R., & Snilstveit, B. (2016). Campbell Methods Policy Note on Converting Between Effect Sizes. The Campbell Collaboration.
Preti, A., Incani, E., Camboni, M. V., Petretto, D. R., & Masala, C. (2006). Sexual abuse and eating disorder symptoms: The mediator role of bodily dissatisfaction. Comprehensive Psychiatry, 47(6), 475–481. https://doi.org/10.1016/j.comppsych.2006.03.004
Price, C. J. (2005). Body-oriented therapy in recovery from child sexual abuse: An efficacy study. Alternative Therapies in Health and Medicine, 11(5), 46–57.
Probst, M., Vandereycken, W., van Coppenolle, H., & Vanderlinden, J. (1995). The Body Attitude Test for patients with an eating disorder: Psychometric characteristics of a new questionnaire. Eating Disorders, 3(2), 133–144. https://doi.org/10.1080/10640269508249156
Rayworth, B. B., Wise, L. A., & Harlow, B. L. (2004). Childhood abuse and risk of eating disorders in women. Epidemiology, 15(3), 271–278. https://doi.org/10.1097/01.ede.0000120047.07140.9d
Ridolfi, D. R., & Crowther, J. H. (2013). The link between women’s body image disturbances and body-focused cancer screening behaviors: A critical review of the literature and a new integrated model for women. Body Image, 10(2), 149–162. https://doi.org/10.1016/j.bodyim.2012.11.003
Rohde, P., Ichikawa, L., Simon, G. E., Ludman, E. J., Linde, J. A., Jeffery, R. W., & Operskalski, B. H. (2008). Associations of child sexual and physical abuse with obesity and depression in middle-aged women. Child Abuse & Neglect, 32(9), 878–887. https://doi.org/10.1016/j.chiabu.2007.11.004
Rosen, J. C., Srebnik, D., Saltzberg, E., & Wendt, S. (1991). Development of a body image avoidance questionnaire. Psychological Assessment: A Journal of Consulting and Clinical Psychology, 3(1), 32–37. https://doi.org/10.1037/1040-3590.3.1.32
Salmon, P., Hill, J., Krespi, R., Clark, L., Fisher, J., & Holcombe, C. (2006). The role of child abuse and age in vulnerability to emotional problems after surgery for breast cancer. European Journal of Cancer, 42(15), 2517–2523. https://doi.org/10.1016/j.ejca.2006.05.024
Sanders, B., & Becker-Lausen, E. (1995). The measurement of psychological maltreatment: Early data on the child abuse and trauma scale. Child Abuse & Neglect, 19(3), 315–323. https://doi.org/10.1016/s0145-2134(94)00131-6
Satinsky, S., Reece, M., Dennis, B., Sanders, S., & Bardzell, S. (2012). An assessment of body appreciation and its relationship to sexual function in women. Body Image, 9(1), 137–144. https://doi.org/10.1016/j.bodyim.2011.09.007
Schaaf, K. K., & McCanne, T. R. (1994). Childhood abuse, body image disturbance, and eating disorders. Child Abuse & Neglect, 18(8), 607–615. https://doi.org/10.1016/0145-2134(94)90011-6
Scheffers, M., Van Busschbach, J. T., Bosscher, R. J., Aerts, L. C., Wiersma, D., & Schoevers, R. A. (2017). Body image in patients with mental disorders: Characteristics, associations with diagnosis and treatment outcome. Comprehensive Psychiatry, 74, 53–60. https://doi.org/10.1016/j.comppsych.2017.01.004
Senior, R., Barnes, J., Emberson, J. R., & Golding, J. (2005). Early experiences and their relationship to maternal eating disorder symptoms, both lifetime and during pregnancy. British Journal of Psychiatry, 187, 268–273. https://doi.org/10.1192/bjp.187.3.268
Simonds, S. L. (1992). Sexual abuse and body image: Approaches and implications for treatment. The Arts in Psychotherapy, 19(4), 289–293. https://doi.org/10.1016/0197-4556(92)90007-B
Slade, P. D. (1994). What is body image? Behavior Research and Therapy, 32(5), 497–502. https://doi.org/10.1016/0005-7967(94)90136-8
Slade, P. D., Dewey, M. E., Newton, T., Brodie, D., & Kiemle, G. (1990). Development and preliminary validation of the body satisfaction scale (BSS). Psychology & Health, 4(3), 213–220. https://doi.org/10.1080/08870449008400391
Slevec, J. H., & Tiggemann, M. (2011). Predictors of body dissatisfaction and disordered eating in middle-aged women. Clinical Psychology Review, 31(4), 515–524. https://doi.org/10.1016/j.cpr.2010.12.002
StataCorp. (2015). Stata Statistical Software: Release 14. StataCorp.
Stice, E., & Whitenton, K. (2002). Risk factors for body dissatisfaction in adolescent girls: A longitudinal investigation. Developmental Psychology, 38(5), 669–678. https://doi.org/10.1037//0012-1649.38.5.669
Strauß, B. & Richter-Appelt, H. (1996). Fragebogen zur Beurteilung des eigenen Körpers (FBeK). Göttingen: Hogrefe.
Talmon, A., & Ginzburg, K. (2018). “Body self” in the shadow of childhood sexual abuse: The long-term implications of sexual abuse for male and female adult survivors. Child Abuse & Neglect, 76, 416–425. https://doi.org/10.1016/j.chiabu.2017.12.004
Talmon, A., & Ginzburg, K. (2019). Chased by the Past: The Relation Between Childhood Maltreatment and Fear of Childbirth. Sex Roles, 81(3–4), 223–234. https://doi.org/10.1007/s11199-018-0984-7
Tarullo, A. R., & Gunnar, M. R. (2006). Child maltreatment and the developing HPA axis. Hormones and Behavior, 50(4), 632–639. https://doi.org/10.1016/j.yhbeh.2006.06.010
Taylor, S. E., Lerner, J. S., Sage, R. M., Lehman, B. J., & Seeman, T. E. (2004). Early environment, emotions, responses to stress, and health. Journal of Personality, 72(6), 1365–1393. https://doi.org/10.1111/j.1467-6494.2004.00300.x
Teicher, M. H., Andersen, S. L., Polcari, A., Anderson, C. M., Navalta, C. P., & Kim, D. M. (2003). The neurobiological consequences of early stress and childhood maltreatment. Neuroscience & Biobehavioral Reviews, 27(1–2), 33–44. https://doi.org/10.1016/S0149-7634(03)00007-1
Thompson, A. E., & Kaplan, C. A. (1996). Childhood emotional abuse. The British Journal of Psychiatry, 168(2), 143–148. https://doi.org/10.1192/bjp.168.2.143
Thompson, J. K. (2004). The (mis) measurement of body image: Ten strategies to improve assessment for applied and research purposes. Body Image, 1(1), 7–14. https://doi.org/10.1016/S1740-1445(03)00004-4
Thompson, J. K., Burke, N. L., & Krawczyk, R. (2012). Measurement of body image in adolescence and adulthood. In T. F. Cash (Ed.), Encyclopedia of Body Image and Human Appearance (Vol. 2) (pp. 512–520). San Diego, CA: Academic Press/Elsevier.
Thompson, J. K., Heinberg, L. J., Altabe, M., & Tantleff-Dunn, S. (1999). Exacting beauty: Theory, assessment, and treatment of body image disturbance. American Psychological Association.
Thompson, T., Dinnel, D. L., & Dill, N. J. (2003). Development and validation of a Body Image Guilt and Shame Scale. Personality and Individual Differences, 34(1), 59–75. https://doi.org/10.1016/S0191-8869(02)00026-0
Treuer, T., Koperdák, M., Rózsa, S., & Füredi, J. (2005). The impact of physical and sexual abuse on body image in eating disorders. European Eating Disorders Review, 13(2), 106–111. https://doi.org/10.1002/erv.616
Valois, D. D., Davis, C. G., Buchholz, A., Obeid, N., Henderson, K., Flament, M., & Goldfield, G. S. (2019). Effects of weight teasing and gender on body esteem in youth: A longitudinal analysis from the REAL study. Body Image, 29, 65–73. https://doi.org/10.1016/j.bodyim.2019.02.009
van Dalen, M., Dierckx, B., Pasmans, S. G. M. A., Aendekerk, E. W. C., Mathijssen, I. M. J., Koudstaal, M. J., & Okkerse, J. M. E. (2020). Anxiety and depression in adolescents with a visible difference: A systematic review and meta-analysis. Body Image, 33, 38–46. https://doi.org/10.1016/j.bodyim.2020.02.006
Vartanian, L. R., Hayward, L. E., Smyth, J. M., Paxton, S. J., & Touyz, S. W. (2018). Risk and resiliency factors related to body dissatisfaction and disordered eating: The identity disruption model. International Journal of Eating Disorders, 51(4), 322–330. https://doi.org/10.1002/eat.22835
Visser, M., van Eck, N. J., & Waltman, L. (2021). Large-scale comparison of bibliographic data sources: Scopus, Web of Science, Dimensions, Crossref, and Microsoft Academic. Quantitative Science Studies, 2(1), 20–41.
Walsh, E., Rosenstein, L., Dalrymple, K., Chelminski, I., & Zimmerman, M. (2017). The Importance of Assessing for Childhood Abuse and Lifetime PTSD in Bariatric Surgery Candidates. Journal of Clinical Psychology in Medical Settings, 24(3–4), 341–354. https://doi.org/10.1007/s10880-017-9518-7
Watson, L. B., Matheny, K. B., Gagné, P., Brack, G., & Ancis, J. R. (2013). A Model Linking Diverse Women’s Child Sexual Abuse History With Sexual Risk Taking. Psychology of Women Quarterly, 37(1), 22–37. https://doi.org/10.1177/0361684312454535
Wenninger, K., & Heiman, J. R. (1998). Relating body image to psychological and sexual functioning in child sexual abuse survivors. Journal of Traumatic Stress, 11(3), 543–562. https://doi.org/10.1023/A:1024408830159
Williams, E. F., Cash, T. F., & Santos, M. T. (2004). Positive and negative body image: Precursors, correlates, and consequences. Paper presented at the meeting of the Association for Advancement of Behavior Therapy.
Wilson, D. B. (2016). Practical Meta-Analysis Effect Size Calculator [Online calculator]. Retrieved from https://campbellcollaboration.org/research-resources/effect-size-calculator.html
Wonderlich, S. A., Crosby, R. D., Mitchel, J. E., Thompson, K. M., Redlin, J., Demuth, G., & Haseltine, B. (2001). Eating disturbance and sexual trauma in childhood and adulthood. International Journal of Eating Disorders, 30(4), 401–412. https://doi.org/10.1002/eat.1101
Wonderlich, S. A., Donaldson, M. A., Carson, D. K., Staton, D., Gertz, L., Leach, L. R., & Johnson, M. (1996). Eating disturbance and incest. Journal of Interpersonal Violence, 11(2), 195–207. https://doi.org/10.1177/088626096011002004
Young, L. (1992). Sexual abuse and the problem of embodiment. Child Abuse & Neglect, 16(1), 89–100. https://doi.org/10.1016/0145-2134(92)90010-o
Zlotnick, C., Hohlstein, L. A., Shea, M. T., Pearlstein, T., Recupero, P., & Bidadi, K. (1996). The relationship between sexual abuse and eating pathology. International Journal of Eating Disorders, 20(2), 129–134.
Funding
Open Access funding enabled and organized by Projekt DEAL. This research was supported by the German Federal Ministry of Education and Research (BMBF), funding code 01KR1801A. Responsibility for the content of this publication rests with the authors.
Author information
Authors and Affiliations
Contributions
Christine Bödicker was involved in the conceptualization and administration of the project, investigation (search term, study selection, data extraction and risk of bias assessment), writing (original draft) and visualization. Jonas Reinckens was involved in investigation (study selection, data extraction, risk of bias assessment), and visualization. Michael Höfler was involved in the formal analysis (conduction of the meta-analysis). Jürgen Hoyer was involved in supervision. All authors provided approval for submission of the contents for publication, and agreed to be accountable for the accuracy and integrity of the project.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bödicker, C., Reinckens, J., Höfler, M. et al. Is Childhood Maltreatment Associated with Body Image Disturbances in Adulthood? A Systematic Review and Meta-Analysis. Journ Child Adol Trauma 15, 523–538 (2022). https://doi.org/10.1007/s40653-021-00379-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40653-021-00379-5