Article Text

Abstract
Background and objective Weight loss and reduced fat-free mass are independent risk factors for mortality among patients with chronic obstructive pulmonary disease (COPD). These factors are important for determining diet therapy and examining the validity of assessment for energy intake (EI). We assessed the agreement of EI between a brief-type self-administered diet history questionnaire (BDHQ) and the doubly labelled water (DLW) method among male patients with stable/at risk for COPD.
Method In this cross-sectional observational study, data for 33 male patients were analysed. At the first visit, EI was estimated using a BDHQ (EIBDHQ). Total energy expenditure (TEE) was measured during 13–15 days by the DLW method, while corrected EI was calculated using the TEE and weight change during the DLW period (EIDLW). The difference between EIBDHQ and EIDLW was evaluated by the Bland-Altman method. Multiple regression analysis was used to determine the proportion of variance in the difference between EIBDHQ and EIDLW, as determined by the patient’s characteristics.
Results EIBDHQ was 2100 (95% CI: 1905 to 2295) kcal/day in the total population. A fixed bias was observed between EIBDHQ and EIDLW as −186 (95% CI: −422 to 50) kcal/day, while a proportional bias was not detected by the Bland-Altman analysis. Age, weight, anxiety and interleukin 6 were responsible for 61.7% of the variance in the difference between both EIs in a multiple regression model.
Conclusions The BDHQ underestimated EI among male patients with stable/at risk for COPD, but this estimation error was within an acceptable range compared with previous studies. EIBDHQ precision might be improved by considering common COPD traits, including inflammatory condition and mental state.
- COPD epidemiology
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
How much under-reporting of energy intake (EI) is there when assessed by a brief-type self-administered diet history questionnaire (BDHQ) among male patients with stable/at risk for chronic obstructive pulmonary disease (COPD)?
Although the BDHQ underestimated EI among male patients with stable/at risk for COPD, its precision might be improved by considering common COPD traits, including inflammatory condition and mental state.
The present results present cautionary points to be aware of when evaluating EI and contribute to helping to establish evidence for the dietary assessment of EI in patients with COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the primary causes of mortality throughout the world,1 and thus, its prevention is of great concern. Previous studies have shown that low body weight is associated with the risk of acute exacerbation and mortality,2 3 in particular, fat-free mass index is an independent predictor of mortality in patients with COPD.4 Meanwhile, cardiovascular disease and type 2 diabetes mellitus increase the risk of hospitalisation and mortality in patients with COPD.5 However, metabolic syndrome, which is known to increase the development of these metabolic diseases, is more prevalent among patients with COPDs as compared with the general population.6 In actuality, Schols et al reported that only a daily high caloric supplement and an exercise program induced body weight gain, although much of it was fat mass.7 Therefore, it is important for nutritional intervention in patients with COPD to assess energy intake (EI) by dietary assessment in addition to the evaluation of energy expenditure by devices such as an accelerometer.
However, the dietary assessment is basically a self-reported method and its accuracy is influenced by characteristics of the subjects such as dietary restraint, socioeconomic status and gender.8 Moreover, Burrows et al showed that the EI estimated by the dietary assessment method was under-reported as compared with the total energy expenditure (TEE) measured by the gold standard method, the doubly labelled water (DLW) method.9 Therefore, we need to understand the degree of estimation errors in the EI determined by the dietary assessment in order to interpret dietary data.
The brief-type self-administered diet history questionnaire (BDHQ) was originally developed to assess healthy Japanese diets. The BDHQ was validated using Japanese adults and elderly subjects, a portion of whom had chronic disease such as hypertension and hyperlipidemia, with a reasonable validity found for the questionnaire.10 11 Based on these development and validation processes, the use of the BDHQ has been expanded for use in patients with other diseases, for example, patients with liver disease, diabetes and ulcerative colitis.12–14 However, the validity of the BDHQ for estimating EI has yet to be compared with the DLW method. Furthermore, it should be noted that energy imbalance often occurs in patients with COPD as compared with healthy subjects, due to their specific traits such as dyspnoea,15 depression16 or inflammatory conditions,17 which might affect the under-reporting of EI. Therefore, it is important to specifically determine and evaluate factors related to the estimation error of EI in patients with COPD.
The present paper reports on the accuracy of EI estimated by the BDHQ among male patients with stable/at risk for COPD when using the DLW method. In addition, we also examined whether common clinical traits of COPD were related to the estimation error of EI. We expect that the present results will give indispensable information when planning to use the BDHQ for patients with COPD in Japan.
Methods
Subjects
A total of 37 male outpatients with stable or at risk for COPD were recruited at Saitama Medical University Hospital in the Saitama region of Japan from June 2017 to February 2018. COPD was diagnosed according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines18 and the severity was classified by the GOLD grades. None of the patients had experienced an exacerbation for at least a month prior to the examination. All at-risk patients had a smoking history of no less than 10 pack-years and had chronic respiratory symptoms without any airflow limitation (forced expiratory volume in one second (FEV1)/forced vital capacity≥0.7). Exclusion criteria included individuals who were: taking medications that affect energy balance [thyroid drugs, beta-blockers, glucagon-like peptide-1 receptor (GLP-1R) agonist]; using agents that influence the metabolism of water [diuretics, sodium-glucose cotransporter 2 (SGLT2) inhibitors]; undergoing treatment for infectious diseases, diabetes mellitus with medication, dysphagia, or other serious diseases that would interfere with their movement and who had lost more than 5% of their body weight during the previous 3 months. Out of the 37 subjects who were registered for the study, 4 were excluded from analysis due to either failure to complete the study protocol (n=1), lack of BDHQ data implemented at visit 1 (n=2) or intentional weight loss during the study period (n=1). As a result, there were 26 patients with stable COPD and 7 at-risk patients who were analysed in the present study.
Patient and public involvement
Patients and the public had no involvement in the design, conduct, reporting or dissemination plans of this research.
Protocol
The test protocol was completed in the hospital during two visits over 13–15-day periods. For both visits, subjects were evaluated after an overnight fast. At visit 1, baseline blood and urine were obtained and then, body weight and height were measured with the urinary bladder empty. Following the administration of an oral dose of DLW, the basal metabolic rate (BMR) was measured by indirect calorimetry, and the BDHQ and other questionnaires were completed by the time of the collection of the blood and urine samples that were obtained 4 hours after the administration of DLW. At visit 2, body weight was measured after emptying of the urinary bladder, followed by the last collections of the blood and urine samples. Pulmonary function tests were performed once within 3 months before or after the DLW period when the status of COPD was stable, while the 6 min walk test (6MWT) was performed within a month.
Basic characteristic measurements
Height and body weight were measured using a digital scale to the nearest 0.1 cm and 0.1 kg, respectively. Body mass index (BMI) was calculated as body weight divided by height squared (kg/m2). Pulmonary function tests were performed using a FUDAC-7 instrument (Fukuda Denshi Co., Tokyo, Japan). The predicted pulmonary function values were calculated according to the Japanese Respiratory Society guidelines.19 6MWT was performed under the direction of experienced technicians according to the American Thoracic Society guidelines. Blood samples were analysed in order to evaluate the inflammation markers.
BDHQ
The BDHQ is a four-page fixed-portion questionnaire that takes approximately 15–20 min to complete. Subjects answered questions on the consumption frequency of selected foods according to the instructions on the form, but did not provide information about the portion size. The questions were designed to estimate the dietary intake of 58 types of food and beverage items consumed during the preceding month. After filling out the entire questionnaire, a researcher checked to determine if there were any omissions and urged the subjects to fill in the blanks, if necessary. The BDHQ consists of five sections: (1) intake frequency of food and non-alcoholic beverage items, (2) daily intake of rice and miso soup, (3) frequency of drinking and amount per drink for alcoholic beverages, (4) usual cooking methods and (5) general dietary behavior. Food and beverage items contained in the BDHQ were selected from foods that are commonly consumed in Japan, which were primarily from a food list used by the National Health and Nutrition Survey of Japan.20 The standard portion sizes were derived from several recipe books for Japanese dishes.21 22 EI was estimated from the results of the nutritional value calculation (EIBDHQ).
Researchers can access the BDHQ from EBNJAPAN (Tokyo, Japan) after obtaining a license, with the calculation results available by signing a contract for use of the analysis software (DHQBOXsystem2013, Tokyo, Japan) or via outsourcing with this company. Although there is only a Japanese version of the BDHQ, a further description in English can be viewed at the following URL: http://wwwnutrepimu-tokyoacjp/english/indexhtml.
Measurement of energy expenditure
TEE was measured over 13–15-day periods using the DLW method (modified two-point approach).23 The details of the measurement are shown in online supplemental material 1. TEE was calculated from the carbon dioxide production.24 We used the average of the food quotient by the BDHQ as 0.86, which is the same as that reported in another Japanese elderly population.25 The corrected EI was calculated from the TEE and the change in weight during the DLW period (EIDLW) as follows: EIDLW=TEE+(Δweight×7).26 The Δweight was measured as g/day between the first and last day during the survey, and 7 (kcal/g) is the energy density of the change in weight.27 The BMR was measured by indirect calorimetry using a ventilated hood (Quark RMR, COSMED, Rome, Italy). The gas exchange measurement was initiated after the subject had rested comfortably for 30 min in a prone position, with only consistent data longer than 5 min used in the analyses. The BMR was calculated according to the Weir equation28. Physical activity level (PAL) was calculated as the TEE divided by the BMR.
Supplemental material
Questionnaires
Dyspnoea, health-related quality of life, psychological status and appetite, which were assumed to be related to the EI, were assessed using the questionnaires. Dyspnoea was evaluated using the modified Medical Research Council Dyspnea Scale,29 while the health-related quality of life was assessed using the COPD assessment test,30 in which low scores on both questionnaires indicate better condition. The Hospital Anxiety and Depression Scale (HADS) was used to measure the mental state of patients and the scores on each scale ranged from 0 to 14, with the lower scores indicating less anxiety or depression.31 Subjective appetite was evaluated by the simplified nutritional appetite questionnaire. The scores ranged from 5 to 20, with a score of 15 or more indicating high appetite.32
Statistical analysis
Statistical analyses were performed using SPSS for Windows V.26.0J (IBM Japan, Tokyo, Japan). Data are presented as the means and 95% CI. Significance was set at p=0.05. Agreement between EIBDHQ and TEE or EIDLW was assessed using the Bland-Altman plots.33 The limits of agreement were plotted, equal to 1.96 SD of the difference above and below zero. To evaluate the prevalence of underestimation or overestimation, we calculated 95% CI of EIBDHQ/TEE and EIBDHQ/EIDLW as a cut-off value, which has been proposed by Livingstone and Black.34 Subsequently, subjects with EIBDHQ/TEE and EIBDHQ/EIDLW smaller than 0.93 and 0.86 or larger than 1.07 and 1.14 were considered as underestimations or overestimations, respectively. In addition, the Lin’s concordance correlation coefficient (CCC) was used to examine the agreement between both methods.35 The relationships between each variable were determined using Pearson’s correlation. Simultaneous multiple regression analysis was used to determine the proportion of variance in the difference between the EIBDHQ and EIDLW, as explained by the patient’s characteristics if univariate correlation was significant.
Results
Table 1 presents the characteristics of the patient population. Out of the 33 subjects, 4 (12.1%) were overweight (BMI ≥25.0 kg/m2) and 7 (21.2%) were underweight (BMI <18.5 kg/m2). Although mean body weight did not change during the DLW period (p=0.50), the range was considered to be large (−1.3–1.6 kg). Table 2 shows the energy variables and PAL.
Patients’ characteristics (n=33)
Energy intake, energy expenditure and physical activity level (n=33)
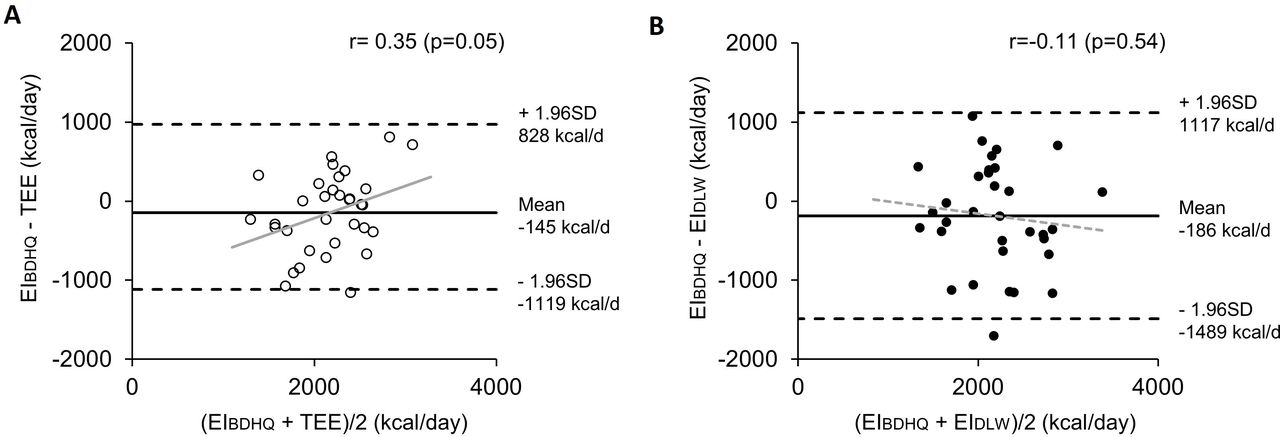
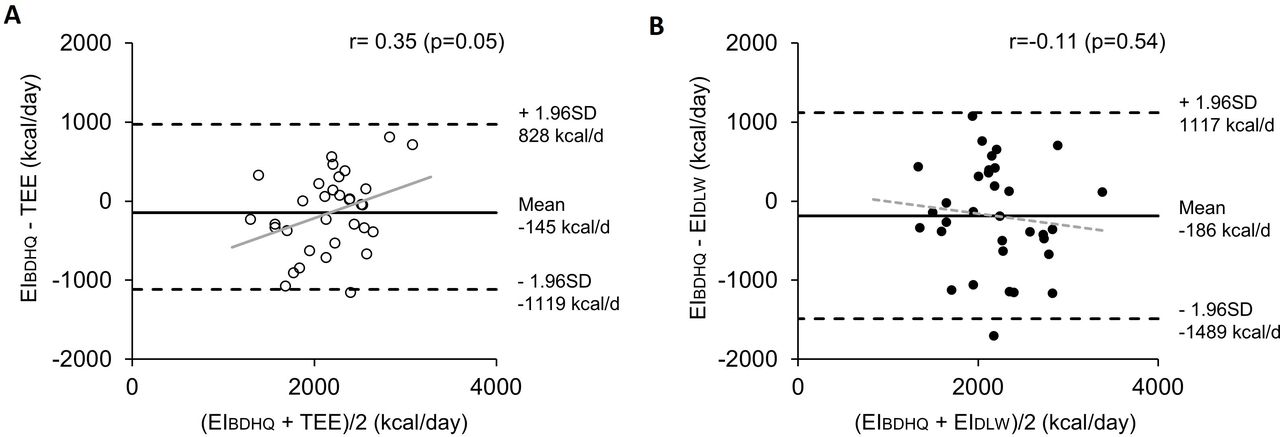
The mean differences (95% CI) between EIBDHQ and TEE or EIDLW were −145 (−321 to 31) kcal/day and −186 (−421 to 50) kcal/day, respectively. When EIBDHQ was compared with TEE and EIDLW, the EIBDHQ in 42.4% and 48.5% of the patients was considered to be underestimation and that in 30.3% and 24.2% of the patients was overestimation, respectively. EIBDHQ showed a weak correlation with TEE (r=0.49, p<0.01) and EIDLW (r=0.35, p<0.05). The difference between the EIBDHQ and TEE was weakly correlated with the average for these factors (r=0.34, p=0.05) (figure 1A), while there was no error proportional to the average of the EIBDHQ and EIDLW (r=−0.11, p=0.54) (figure 1B). In addition, Lin’s CCC was 0.491 (95% CI: 0.162 to 0.664) and 0.345 (95% CI: 0.005 to 0.587) for TEE and EIDLW, respectively.
{kind=link}
(A) Bland-Altman plots showing the difference between the EIBDHQ and TEE in relation to the average. The solid black line demonstrates the mean difference (−145 kcal/day). (B) Bland-Altman plots showing the difference between the EIBDHQ and EIDLW in relation to the average. The solid black line demonstrates the mean difference (−186 kcal/day). The grey line indicates the best-fit line. The dotted lines represent the limits of the agreement (±1.96 SD) from the mean difference. EIBDHQ, energy intake estimated by brief-type self-administered diet history questionnaire; EIDLW, energy intake calculated by doubly labelled water method; TEE, total energy expenditure.
Table 3 shows the correlation coefficients between the EI and other variables. The difference between the EIBDHQ and EIDLW was positively correlated with age, HADS—anxiety and interleukin 6 (IL-6), while negatively correlated with body weight,
Correlation coefficients between EI and each variable (n=33)
Table 4 presents the results of the simultaneous multiple regression analysis for the difference between the EIBDHQ and EIDLW. In this regression model, age, body weight, HADS—anxiety and IL-6 were responsible for 61.7% of the variance in the difference between the EIBDHQ and EIDLW. The other models are presented in the online supplemental table S1.
Multiple regression analysis for predicting the difference between EIBDHQ and EIDLW (n=33)
Discussion
This study examined the accuracy of the EI estimated by the BDHQ among male patients with stable/at risk for COPD as compared with the corrected EI when using the DLW method. Results indicated that the BDHQ underestimated the EI among the present population. In addition, this is the first study that has examined factors related to the error of the estimated EI in patients with COPD, with the discrepancy between the EIBDHQ and EIDLW found to be independently influenced by age, body weight, inflammatory condition and mental state.
The present subjects showed that PAL (95% CI) was 1.79 (1.72 to 1.86), which seemed to be a little higher than that observed for the elderly population in Western countries. However, Yamada et al evaluated the TEE and BMR measured using DLW and indirect calorimetry in community-dwelling male older adults without sporting habits (73±9 years).25 PALDLW calculated by them was 1.85±0.23. Furthermore, Morino et al reported the PALDLW of patients without diabetes mellitus (67.1±4.7 years)23 and their PALDLW (95% CI) was 1.81 (1.72 to 1.91). With regard to these results, the subjects in our study had similar PAL as compared with other populations in Japan.
The Academy of Nutrition and Dietetics revised the COPD evidence-based nutrition practice guideline in 2019.36 In accordance with this guideline, the recommendation level of estimated energy requirement in patients with COPD was weak as there was little evidence on TEE for them. In addition, this guideline also proposed using the 30 kcal/kg body weight to estimate the TEE for non-obese adults with COPD. However, the present study results showed that the average of the TEE kcal/kg was 38 kcal/kg, which was higher than the energy estimates proposed by this guideline. Moreover, Farooqi et al combined and then re-examined their previous results37–39 and reported finding that the average of TEE kcal/kg was approximately 33 kcal/kg among 44 patients with COPD, even though these subjects were from a relatively more severe population (GOLD2, n=10; GOLD3, n=21; GOLD4, n=10) as compared with our subjects.40 Therefore, an additional study that determines the energy requirement among patients with COPD will need to be conducted in the future.
Energy requirement is the amount of food energy needed to balance the energy expenditure in order to maintain the body size.41 The present results demonstrated that EIBDHQ was significantly lower (−145 (95% CI: −321 to 31) kcal/day (p<0.01)) than TEE. However, the range of body weight change during the DLW period (−1.3–1.6 kg) was larger than we expected, which indicated the energy balance was not stable during that period. Thus, we also calculated the EIDLW as the actual EI during the DLW period and explored the factors associated with the difference between EIBDHQ and EIDLW. Our multiple regression analysis showed that older age, worse mental status and inflammatory conditions were related to the over-reporting of the BDHQ, while being larger body weight led to under-reporting.
McKenzie et al performed a systemic review and meta-analysis and found that the mean estimation error (95% CI) of EI by a food frequency questionnaire (FFQ) was −421 (−546 to –297) kcal/day in a male population evaluated by the results of a pool analysis (n=178).42 In contrast, the present results showed that the estimation error of EI by the BDHQ was −186 (−422 to 50), which is a smaller and narrower range as compared with the previous studies.
The present degree of under-reporting (8.1%) seemed to be a little smaller as compared with that which has been shown in previous studies. Under-reporting of EI estimated by FFQ tended to increase with obesity index such as BMI.43 The subjects in the present study were generally leaner compared with the previous studies with subjects of similar age mainly conducted in Western countries. Therefore, this was probably the main reason why the degree of under-reporting of the present study was a little smaller.
Meanwhile, the degree of under-reporting decreased according to the increase in age within the subjects of the present study. EIBDHQ in the older subjects seems to be slightly less under-reported. The previous study10 showed that median EIBDHQ in very old subjects (1642 kcal/day, median age was 87 years old, men and women together) was a little small as those expected from the mean EIBDHQ in middle-aged subjects11 (1923 kcal/day, mean age was 50 years old, men and women together). However, it is yet unknown this was due to smaller portion sizes of foods, or less frequent intake of foods, or both.
Watanabe et al reported the estimation error of EI by FFQ in healthy elderly men that had a similar age (73.5±6.0 years) and weight (61.6±8.6) as our subjects.44 Their estimation error (−463 (95% CI: −612 to –314) kcal/day) was larger than that found in our present study. However, the dietary assessment questionnaire used was different between the two studies. The subjects were also different: they were apparently healthy community-dwelling older persons in the previous study. Therefore, we could not explain the reason of this difference whether it was due to the difference of questionnaires used, difference of subject characteristics such as mental status and physical activity or some other unknown factors.
Farooqi et al examined the validity of diet history for estimating EI using DLW method in women with COPD.45 The underestimation of EI was 28% as compared with TEE but EIDLW was not shown in the study. The BMI of the subjects was 24.5±3.5 kg/m2, which is larger as compared with that observed in our subjects (21.7 (95% CI: 20.6 to 22.9) kg/m2). Thus, this may be one of the reasons that underestimation of EI was larger in the previous study as compared with the present results, as under-reporting of the EI has been shown to be associated with a higher BMI.46 In addition, it has been demonstrated that the under-reporting of the EI when using a FFQ or diet history was larger in women versus men.43 47 48 These findings appear to confirm why there was a larger underestimation of the EI in the previous COPD women versus the present male patients. Moreover, Farooqi et al also conducted 7-day food diaries during the DLW period. When these types of dietary surveys are conducted, subjects often eat less than usual, as they find that recording the amount of food consumed is troublesome. Therefore, it is possible in the previous study that actual food intake during dietary survey was smaller as compared with a usual diet due to undereating by the subjects. If they compared with EIDLW instead of TEE, underestimation of EI might have been smaller.
In addition to the factors examined in the present study, food choice also affects the results of the under-reporting of EI because this could differ in patients with COPD as compared with the healthy counterparts. One previous study in Italy reported a significantly lower intake of cereals, potatoes, meats and fish, which are the main sources of energy and protein in the country.49 In contrast, patients reported a significantly higher intake of dairy products and non-alcoholic beverages. Although this study unfortunately used a FFQ that was developed for healthy individuals rather than for patients with COPD, this finding does suggest that there may be some different food choices among patients with COPD as compared with healthy controls. A further study will need to be conducted to clarify the effect of food choice on the estimation error of EI between COPD and control subjects.
The present study had several limitations. First, a small sample size could have made the regression model unstable and thus, a more stable model will need to be reconsidered by increasing new subjects in order to use the present model in a clinical setting. Second, only male subjects were evaluated in this study due to the fact the prevalence of COPD in Japan is higher in men than in women50 and because there were fewer female patients who met the inclusion criteria at our hospital. Since the validity of the dietary assessment depends on the sex difference, the present results only apply to male patients. Third, this study included only two patients with very severe COPD (GOLD stage 4), as they often had comorbidities that met our exclusion criteria. In the present population, there was no significant correlation for the %FEV1 and the difference between the EIBDHQ and EIDLW. Fourth, the period surveyed by the BDHQ took place before and did not overlap with the DLW period. However, Okubo et al have suggested that dietary behaviour could be influenced by either an intentional or non-intentional intervention effect when the DHQ is conducted during the DLW period.51 Thus, to avoid this issue, potential bias, such as influencing the dietary behaviour, was kept to a minimum in the present study. Fifth, TEE was calculated with the food quotient as a constant, as the other dietary assessments were not conducted in the present study. Sixth, foods that should be listed in the BDHQ, especially for patients with COPD, and the food portion size have not yet been surveyed. Therefore, we will need to conduct a study that includes details on the weighed dietary records or dietary recalls in order to determine the foods and the portion sizes that should be listed in the BDHQ for patients with COPD. Seventh, the present study did not include control subjects and thus, the effect of the food choice difference between control subjects and patients with COPD could not be examined.
In conclusion, although EI estimated by the BDHQ was lower than that by the DLW method among male patients with stable/at risk for COPD, the estimation error was within an acceptable range as compared with that reported in previous studies. The precision of the EI could potentially be improved by taking into consideration the inflammatory condition and mental state of COPD.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Ethics approval
The study protocol was approved by the Ethics Committee of the Saitama Medical University (approval number 16-003-1), Keio University (approval number 2015-03) and the National Institutes of Biomedical Innovation, Health and Nutrition (approval number NIBIOHN29), in accordance with the Declaration of Helsinki. All participants gave written informed consent after being informed of the study procedures.
Acknowledgments
The authors would like to thank Azusa Sasaki, Hitoshi Miyazawa and Akiko Sakata for their technical assistance. The authors are also grateful to all of the subjects and hospital personnel for their dedication.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors YN contributed to data collection, analysis and interpretation of data and wrote the manuscript. HN contributed to the study design and conduct, data collection, analysis and interpretation of the data and manuscript review and editing. SS, YY, ST and FK contributed to the study design and the interpretation of the data. TS, HS, SY and SN contributed to data collection and interpretation of data. HN, ST and FK take responsibility for the integrity of the data and the accuracy of the data analysis. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This work was supported by the Japan Agency for Medical Research and Development (grant numbers JP17ek0210045 and JP20ek0210112).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.