Abstract
With the abrupt transition to observing physical distancing as a result of COVID-19, applied behavior analysts were faced with the sudden need to modify their service delivery model, while at the same time managing personal difficulties brought about by the pandemic. The present article provides a description of the impact of COVID-19 on the behavior analyst workforce currently providing clinical services in the United States. We conducted a survey to assess work conditions, burnout, and productivity of behavior analysts at various certification levels. These data provide a snapshot of the impact of COVID-19 on the workforce. Overall, one third of the participants reported experiencing job insecurity, and almost half of participants reported decreased productivity and increased burnout, with remote workers more severely affected. Taken together, these factors could compromise the ability of behavior analysts to adequately provide services to their clients. We provide recommendations for behavioral health agencies for supporting staff during extreme situations such as a pandemic.
Similar content being viewed by others


During most of the year 2020, the world was rattled by the spread of a novel coronavirus, the catalyst for the COVID-19 pandemic. Health officials urged the public to wash hands, avoid touching their face, and observe physical distancing (Centers for Disease Control & Prevention, 2021). Individuals all over the world had to adapt to rapidly changing conditions. As the virus spread through the United States in the spring, many individuals began working from home (Brenan, 2020), nonessential businesses temporarily closed (McPhillips, 2020), and teachers were forced to move all instruction online (Education Week, 2020). Effects of the pandemic itself and the demands that arose from working remotely may have health and performance implications for employees. Given the work of a behavior analyst delivering clinical services traditionally involves direct social contact with clients, it was of interest to evaluate how this rapid change in the world affected the field of behavior analysis.
In addition to determining how to provide clinical services during lockdown conditions (e.g., Behavioral Health Center of Excellence, 2020; Council for Autism Service Providers, 2020a, 2020b), behavior analysts had to grapple with concerns for their health, job security, and personal responsibilities (e.g., providing care for their children). The purpose of this article is to provide a description of the impact of COVID-19 on the workforce of behavior analysts providing clinical services in the United States. This study is of particular importance given the heightened potential for burnout among health-care workers recognized early in the pandemic (Bradley & Chahar, 2020; Launer, 2020).
Burnout in Behavior Analysis
Researchers have reported that working in some industries, such as health care and special education, can be associated with higher rates of job burnout (e.g., Brunsting et al., 2014; Hensel et al., 2015). Behavior analysts also have been reported to experience high rates of job burnout and work-related stress. Plantiveau et al. (2018) evaluated stress and burnout in 183 behavior analysts via a survey. These researchers reported that 48% of participants were not satisfied with their current work conditions, 39% experienced job dissatisfaction, and 37% and 26% of participants experienced moderate to high burnout rates, respectively. Plantiveau et al. also reported some conditions that tended to meliorate burnout and job dissatisfaction, including support at work from supervisors and peers, opportunities for professional development, and high-quality supervision. Dounavi et al. (2019) extended this research to a sample of 92 international behavior analysts. They reported that across the three dimensions of burnout, emotional exhaustion, depersonalization, and personal accomplishment, 37%, 37%, and 27%, respectively, experienced burnout. Dounavi et al. also found that, whereas excessive work demands were correlated with more burnout and supervisor support was correlated with less burnout, colleague support had mixed effects across different dimensions of burnout.
Based on a review of surveys conducted specifically with behavior technicians (i.e., direct-care providers), Novack and Dixon (2019) reported similar findings to those described by Plantiveau et al. (2018) and Dounavi et al. (2019). Novack and Dixon found four studies that provided reports of burnout from a total of 255 school- and home-based behavior technicians in the United States, the United Kingdom, and Ireland. Samples from individual studies found up to 42% of behavior technicians reported low levels of personal accomplishment (Griffith et al., 2014), 27% reported high levels of emotional exhaustion (Gibson et al., 2009), and 38% reported being highly or somewhat likely to resign (Kazemi et al., 2015). Conditions associated with lower levels of burnout included greater satisfaction with supervisor support (Gibson et al., 2009; Hurt et al., 2013) and greater levels of job satisfaction (Hurt et al., 2013).
Burnout during COVID-19
Some variables linked to job burnout include stress, job security, support from the organization (e.g., communication, resources), mental health personal risk factors, work-life balance, and job satisfaction (Brunsting et al., 2014; Gibson et al., 2009; Griffith et al., 2014; Hurt et al., 2013; Leiter & Maslach, 1988), all of which can be exacerbated by an event such as a worldwide pandemic. Recent studies conducted during the pandemic suggest that employees across industries faced various demands, including economic stressors, work and family conflict, and setbacks from work-related tasks (Chong et al., 2020; Sinclair et al., 2020; Sinclair et al., 2021). According to the conservation of resources theory proposed by Hobfoll (1989), when individuals experience loss of resources (e.g., decreased access to peers or support from supervisor), threats to current resources (e.g., greater demands such as job insecurity and distractions), or inadequate return on resources (e.g., decreased productivity), they may experience burnout. On the other hand, availability of resources, such as time management strategies and supervisor support, may allow individuals to engage in behaviors that build existing resources (i.e., lead to further reinforcer access), thereby reducing burnout and enhancing productivity.
The risk for heightened burnout during the pandemic is greater for health-care workers (Bradley & Chahar, 2020; Lai et al., 2020; Launer, 2020; Matsuo et al., 2020; Talaee et al., 2020). For instance, Matsuo et al. (2020) evaluated the prevalence of burnout among frontline health-care workers in Japan during the COVID-19 pandemic and found that more than 40% of nurses and 30% of radiological technologists and pharmacists met the criteria for burnout. Related to this, Khasne et al. (2020) reported that health-care workers in India experienced elevated personal (44.6%), work-related (26.9%), and pandemic-related (52.8%) burnout and suggested that support from management by improving work conditions may help meliorate the effects of the pandemic on burnout (see also Duarte et al., 2020; Serrão et al., 2021; Tan et al., 2020). Given the documented effects of this pandemic on health-care workers, the purpose of the present study was to collect data on the impact of this historic event on the behavior analytic workforce providing clinical services in the United States. Based on literature described herein, and consistent with the theory proposed by Hobfoll (1989), we hypothesized that greater burnout experienced by behavior analysts during this time would correlate with decreased access to resources, such as support from supervisors and diminished productivity, and that this effect would be more pronounced in individuals working remotely.
Method
Participants and Procedure
Participants were recruited via an email sent through the Behavior Analyst Certification Board (BACB®; 2021) email list, in which they were invited to complete an online survey. The email was sent in April 2020 to all RBT®, BCaBA®, BCBA®, and BCBA-D® certificants residing in the United States who elected to receive solicitation. The precise number of recipients is unknown because the number of those opting out of receiving notifications is not available; thus, the response rate cannot be reported. The survey was completed online via the Qualtrics website (https://www.qualtrics.com). Entry into a drawing for a $25 Amazon gift card was offered as an incentive. Within 1 week of the email being sent, there were 1,281 respondents and the survey was closed. Two respondents did not consent to participate, 68 were not eligible to participate because they were not employed at the time of their response, and 143 were not eligible to participate because they were on unpaid leave at the time of their response. Thus, 1,068 respondents answered some portion of the survey and 491 fully completed it, for a 45.97% completion rate. Only data from completed surveys are reported.
Full demographic data of the participants are presented in Table 1. The majority of respondents had BCBA® certification (62%), followed by RBT® (36%), and BCaBA® (3%) certifications. On average, participants were 33.45 years of age (SD = 8.70) and predominantly female (89%). With respect to ethnicity, approximately 84% of the participants identified as non-Latino white. Compared to data reported by the BACB® (2021), white and BCBA® individuals were overrepresented in the sample who completed this survey. A range of variables could have affected the skew in race/ethnicity and level of certification, including which BACB® certificants select to opt out of solicitations and different time constraints experienced by different groups at the time the survey was sent out.
Participants reported being employed for an average of 34.08 hours per week (SD = 11.93) at the time of the survey. During that time, approximately 54% of participants were working remotely as a result of COVID-19. That is, a total of 266 participants were working remotely whereas 225 were working nonremotely at the time of the survey.
Measures
Participants were asked to report on a range of different variables they experienced and behaviors in which they engaged since COVID-19 began affecting local health guidelines and in-person work, approximately early to mid-March 2020. In this article, only a subset of these variables central to the hypothesis are reported and analyzed (i.e., job insecurity, partner job insecurity, distractions during work hours, supervisor social support, time management planning, information exchange, burnout, and productivity). These measures were selected given the existing literature on burnout in health-care workers, including clinical behavior analysts (e.g., Plantiveau et al., 2018), and the emerging findings of the further impact of the pandemic on stress, burnout, and ability to perform job duties (e.g., Khasne et al., 2020). Well-established and widely utilized measures from the organizational field were used to evaluate relevant variables. In cases where adequate measures were not available (e.g., distractions during work hours), the second author, who is an industrial-organizational psychologist with expertise in the area of work-related stress developed measures for the purposes of this study. Appendix A lists the individual survey items, along with their measurement scales and sources, for each of the reported variables.
Job Insecurity, Self and Partner
Ten items from Oldham et al. (1986) were used to assess job insecurity. A sample item was “My job is not a secure one.” The stem for partner job insecurity items was modified to reflect the job insecurity of one’s partner (e.g., “My partner’s job is not a secure one.”). All items were measured on a 7-point Likert scale, from 1 = “Strongly disagree” to 7 = “Strongly agree.” Cronbach’s alpha reliabilities for self and partner job insecurity were .91 and .94, respectively.
Distractions during Work Hours
Two items were developed to assess distractions during work hours. A sample item was “I get distracted by non-work-related tasks at home during work hours.” Both items were measured using a 5-point Likert scale, ranging from 1 = “Never” to 5 = “Very frequently.” Cronbach’s alpha reliability for this scale was .83 in the current study.
Supervisor Social Support
Supervisor support was assessed using a 4-item scale (Beehr et al., 1990). A sample item was “My immediate supervisor is willing to listen to my personal problems.” All items were rated on a 5-point Likert scale, ranging from 1 = “Never” to 5 = “Very frequently.” Cronbach’s alpha reliability was .92 for this scale in the present study.
Time Management Planning
Five items from Parke et al. (2018) were used to assess time management planning. A sample item from this scale was “Since the coronavirus, do you make a list of things that you have to do?” All items were rated on a 5-point Likert scale, from 1 = “Never” to 5 = “Very frequently.” Cronbach’s alpha reliability for this scale was .83.
Information Exchange
Eight items developed for this study were used to measure frequency and quality of information exchange between the participant and other members of their work team (e.g., peers, supervisor). A sample item was “The information my colleagues share with me is valuable and of high quality.” All items were measured on 5-point Likert scale, from 1 = “Never” to 5 = “Very frequently.” Cronbach’s alpha reliability for this measure was .89.
Burnout
We measured burnout using nine items from Shirom and Melamed’s (2006) burnout scale. A sample item included, “I feel physically drained.” All items were rated on a 7-point Likert scale, ranging from 1 = “Strongly disagree” to 7 = “Strongly agree.” Cronbach’s alpha reliability for this measure in the current study was .94.
Productivity
Two survey items were developed to assess productivity related to work duties. A sample item was “I can finish a large number of work-related tasks daily.” Both items were measured on a 7-point Likert scale, from 1 = “Strongly disagree” to 7 = “Strongly agree.” Cronbach’s alpha reliability for this measure was .70.
Analytic Strategy
Independent samples t-tests across remote and nonremote behavior analysts were conducted to ascertain whether there were differences with respect to job insecurity, partner job insecurity, distractions during work hours, supervisor social support, time management planning, information exchange, burnout, and productivity. Considering that multiple t-tests can inflate the probability of observing a significant effect even when none exist, Bonferroni corrections (i.e., p < .006) to control for Type I errors were applied. Next, bivariate correlations among all variables for remote versus nonremote workers were computed.
Results
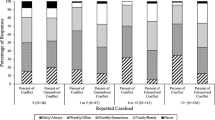
Overall, 31.6% of the participants experienced job insecurity at the time of this study. In addition, 45.4% of participants indicated they experienced burnout and 42.6% of participants reported reduced productivity at the time of completing the survey. Table 2 presents the means scores on Likert scales, standard deviations, t-tests, and correlations among all study variables for remote and nonremote participants. Results indicated significant differences in distraction and information exchange at p < .006 value. In particular, participants working remotely (M = 3.65, SD = 1.05) experienced significantly greater distractions compared to nonremote workers (M = 3.01, SD = 1.21), t(489) = 6.26, p = .00. Likewise, remote workers (M = 4.17, SD = 0.74) perceived significantly greater information exchange compared to nonremote workers (M = 3.77, SD = 0.90), t(489) = 5.31, p = .00. Although time management and productivity were different between remote and nonremote workers, the mean difference occurred at the p = .02 level, and therefore was not considered a significant difference. There were no significant differences in job insecurity, partner job insecurity, supervisor support, or burnout among remote versus nonremote behavior analysts.
Correlation results indicated that across both remote and nonremote participants, job insecurity was positively associated with burnout and negatively related to productivity. Although distractions were negatively related to productivity in both remote and nonremote participants, there was only a positive association between distractions and burnout among those participants that were working remotely. Lastly, supervisor support, time management, and information exchange were positively associated with productivity and negatively correlated with burnout across both groups of participants. There was no relationship between partner’s job insecurity and burnout or productivity for either remote or nonremote employees.
Discussion
The present study sought to characterize the impact of COVID-19 on the behavior analysis workforce. Results of the present survey revealed that almost half of all respondents reported high levels of burnout and decreased productivity, and a third of respondents experienced job insecurity. The number of respondents reporting burnout was higher than previously reported by Plantiveau et al. (2018) and Dounavi et al. (2019), which could be in part due to the additional challenges resulting from the pandemic. Compounding the baseline challenges of the behavior analysts’ job (Plantiveau et al., 2018) with the effects of the pandemic could hinder the behavior analysts’ ability to effectively perform their jobs, which is of great concern because behavior analysts often work with vulnerable populations. Therefore, behavioral health providers may consider developing antecedent strategies to curb the effects of sudden stressors (e.g., large-scale weather or public health-related events, individual acute life events) on the burnout experienced by behavior analysts delivering clinical services. Some antecedent strategies to consider include establishing specific protocols to follow when local, national, or global health or weather emergencies occur. For instance, providers could create a decision tree to help determine the needs of clients during emergency situations that disrupt services (Colombo et al., 2020), create a contingency plan for potential disruption of service (e.g., assessment of appropriateness of telehealth services for clients, system for rapidly and efficiently communicating with staff and clients), create a system to obtain requisite approvals or coverage to deliver remote services (e.g., insurance authorizations for telehealth services), establish procedures and trainings on reallocation of workflow (e.g., train staff to deliver services remotely instead of in-person service delivery to client), assign staff in advance to address specific issues that may arise (e.g., clinician unavailable due to emergency, tornado warning) and empower them to act accordingly (e.g., assign different clinician to client, communicate disruption of services to relevant parties).
Although behavior analysts working remotely and nonremotely during this time did not differ in their reported level of burnout, there was a notable difference between the two groups in terms of productivity. In particular, remote workers reported lower productivity. Likewise, the two groups differed significantly in the frequency and quality of information exchanged between the participant and other members of their work team and in distractions during work hours. Despite receiving more information from their teams and engaging in more planning activities, remote workers experienced decreased productivity. This could be due to the difficulties of separating work tasks from personal tasks while working from home. It also could be the result of competing activities hindering or precluding work productivity (e.g., more time spent on administrative tasks creating or learning COVID-19 procedures instead of implementing services to clients). Additional distractions experienced during this time negatively affected the productivity of both remote and nonremote workers, but only increased burnout in remote workers. During the uncertain times of COVID-19, all behavior analysts have had to balance the needs of their clients with their own needs, as well as the needs and well-being of staff they may supervise. Working remotely may have challenged behavior analysts to bring additional familial and household needs into this balance as well.
The pandemic affected individuals differently based on their personal circumstances. For instance, it is possible that behavior analysts who are at high risk for contracting COVID-19, or who have caregiver responsibilities, may experience continuing to work in person with clients differently than individuals who do not have health concerns or are not the primary caregivers for small children. Matsuo et al. (2020) noted it is important for team leaders and peers to demonstrate support and reinforce the effort of healthcare workers during the pandemic. Consistent with Plantiveau et al. (2018) and Dounavi et al. (2019), results from this study suggest that support from supervisors protects workers from experiencing burnout. Related to this, clear and timely communication from supervisors with their staff, providing prompt and easy access to resources (e.g., personal protective equipment, mental health support) and relevant information (e.g., COVID-19 policies and procedures, relevant training, relevant local information) during the transition to remote work may help alleviate uncertainty and increase reported support from supervisors. According to findings from the present study, information exchange was correlated with higher productivity and lower burnout for both remote and nonremote workers. This finding is consistent with reports that when staff perceive greater personal and professional support from supervisors, they report less burnout (Hurt et al., 2013). For instance, supervisors could use mass text apps such as GroupMe (https://groupme.com) or platforms such as Basecamp (https://basecamp.com) or Slack (https://slack.com) to easily disseminate information, resources, and maintain communication among the team.
When presented with circumstances such as rapidly pivoting to remote work, supervisors may consider providing additional supervision to ensure proper training and support of staff. In addition to considering the financial implications for the organization, supervisors have an ethical obligation to consider the implications, for their staff and clients, of drastically changing their service delivery model. To be better prepared in advance of unforeseen circumstances that necessitate major and immediate shifts, such as the present pandemic, organizations may consider building a part-time backup service delivery model into their existing structure. For example, an agency providing only center-based services may begin including 1 or 2 hr a month of parent training provided through telehealth. Doing so would ameliorate at least some ethical concerns, having staff who are already trained in implementing those alternative service models. If there is one lesson to learn from the current pandemic, it is that we may face unforeseen circumstances and find ourselves wholly unprepared for the challenge. Therefore, organizations should strive to develop policies and procedures for addressing challenges presented by unexpected events, such as natural disasters or a pandemic, and should train staff to engage in their work tasks under varying conditions. Likewise, supervisors may develop a process for addressing conflicts between ethical code elements, such as when trying to balance the best interest of clients by continuing to deliver in-person services and the well-being of staff who may not feel comfortable or well-prepared to do so under uncertain conditions (see Rosenberg & Schwartz, 2019, for a decision tree for ethical decision making).
For the long-term well-being of behavior analytic service providers and their workforce, agencies should aim to collect internal data on job satisfaction, staff perception of available resources and support, personal and professional barriers for completing tasks, contingencies governing staff behavior, and how each of these variables may be affected by current environmental conditions. Tools such as the Performance Diagnostic Checklist-Human Services proposed by Carr et al. (2013; see Cymbal et al., 2020, for review) can be useful for this purpose. Practitioners also may consider adapting such tools to the specific needs of the provider organization and to include any unique environmental conditions (e.g., COVID-19). This would allow service providers to preemptively address issues that may arise in the workforce that could be aggravated in the presence of drastic circumstances such as a global pandemic or natural disaster. This pandemic has posed many challenges, and this article provides only a brief snapshot of the impact it had on the behavior analytic workforce. A third of the participants of this study reported experiencing job insecurity and almost half reported decreased productivity and increased burnout, with remote workers more severely affected during the early months of the COVID-19 pandemic. All of these factors could hinder the ability of behavior analysts to deliver high-quality clinical services to their clients during this time. The time is ripe for service providers and practitioners to convert lessons learned and prepare for future unforeseen situations.
References
Beehr, T. A., King, L. A., & King, D. W. (1990). Social support and occupational stress: Talking to supervisors. Journal of Vocational Behavior, 36(1), 61–81. https://doi.org/10.1016/0001-8791(90)90015-T.
Behavior Analyst Certification Board. (2021). BACB certificant data. https://www.bacb.com/bacb-certificant-data/
Behavioral Health Center of Excellence. (2020). COVID-19 FAQs for ABA providers. https://bhcoe.org/resources/covid-19-faqs-for-aba-providers/
Bradley, M., & Chahar, P. (2020). Burnout of healthcare providers during COVID-19. Cleveland Clinic Journal of Medicine. Advance online publication. https://doi.org/10.3949/ccjm.87a.ccc051
Brenan, M. (2020). COVID-19 and remote work: An update. Gallup. https://news.gallup.com/poll/321800/covid-remote-work-update.aspx
Brunsting, N. C., Sreckovic, M. A., & Lane, K. L. (2014). Special education teacher burnout: Asynthesis of research from 1979 to 2013. Education & Treatment of Children, 37, 681–711.
Carr, J. E., Wilder, D. A., Majdalany, L., Mathisen, D., & Strain, L. A. (2013). An assessment-based solution to a human-service employee performance problem: An initial evaluation of the performance diagnostic checklist—Human services. Behavior Analysis in Practice, 6(1), 16–32. https://doi.org/10.1007/BF03391789.
Centers for Disease Control & Prevention. (2021). Things to know about the COVID-19 pandemic. https://www.cdc.gov/coronavirus/2019-ncov/your-health/need-to-know.html
Chong, S., Huang, Y., & Chang, C. H. D. (2020). Supporting interdependent telework employees: A moderated-mediation model linking daily COVID-19 task setbacks to next-day work withdrawal. Journal of Applied Psychology, 105(12), 1408–1422. https://doi.org/10.1037/apl0000843.
Colombo, R. A., Wallace, M., & Taylor, R. (2020). An essential service decision model for ABA providers during crisis. Behavior Analysis in Practice, 13, 306–311. https://doi.org/10.1007/s40617-020-00432-z.
Council for Autism Service Providers. (2020a). Coronavirus resources. https://casproviders.org/coronavirus-resources/
Council for Autism Service Providers. (2020b). Practice parameters for telehealth ABA. https://casproviders.org/practice-parameters-for-telehealth/?fbclid=IwAR2wUUPuFj908_lW5sG0SATp3RUW6q3kP dWFE6fS_wslOytxl7Bv8a71ik
Cymbal, D., Wilder, D. A., Thomas, R., & Ertel, H. (2020). Further evaluation of the validity and reliability of the performance diagnostic checklist-human services. Journal of Organizational Behavior Management, 40(3–4), 249–257. https://doi.org/10.1080/01608061.2020.1792027.
Dounavi, K., Fennell, B., & Early, E. (2019). Supervision for certification in the field of applied behaviour analysis: Characteristics and relationship with job satisfaction, burnout, work demands, and support. International Journal of Environmental Research & Public Health, 16(12), 2098. https://doi.org/10.3390/ijerph16122098.
Duarte, I., Teixeira, A., Castro, L., Marina, S., Ribeiro, C., Jácome, C., Martins, V., Ribeiro-Vaz, I., Pinheiro, H. C., Silva, A. R., Ricou, M., Sousa, B., Alves, C., Oliveira, A., Silva, P., Nunes, R., & Serrão, C. (2020). Burnout among Portuguese healthcare workers during the COVID-19 pandemic. BMC Public Health, 20(1), 1885. https://doi.org/10.1186/s12889-020-09980-z.
Education Week. (2020). The coronavirus spring: The historic closing of U.S. schools (A timeline). https://www.edweek.org/leadership/the-coronavirus-spring-the-historic-closing-of-u-s-schools-a-timeline/2020/07
Gibson, J. A., Grey, I. M., & Hastings, R. P. (2009). Supervisor support as a predictor of burnout and therapeutic self-efficacy in therapists working in ABA schools. Journal of Autism & Developmental Disorders, 39, 1024–1030. https://doi.org/10.1007/s10803-009-0709-4.
Griffith, G., Barbakou, A., & Hastings, R. (2014). Coping as a predictor of burnout and general health in therapists working in ABA schools. European Journal of Special Needs Education, 29, 548–558. https://doi.org/10.1080/08856257.2014.952915.
Hensel, J. M., Lunsky, Y., & Dewa, C. S. (2015). Exposure to aggressive behaviour and burnout in direct support providers: The role of positive work factors. Research in Developmental Disabilities, 36, 404–412. https://doi.org/10.1016/j.ridd.2014.10.033.
Hobfoll, S. E. (1989). Conservation of resources: A new attempt at conceptualizing stress. American Psychologist, 44(3), 513–524.
Hurt, A. A., Grist, C. L., Malesky Jr., L. A., & McCord, D. M. (2013). Personality traits associated with occupational “burnout” in ABA therapists. Journal of Applied Research in Intellectual Disabilities, 26, 299–308. https://doi.org/10.1111/jar.12043.
Kazemi, E., Shapiro, M., & Kavner, A. (2015). Predictors of intention to turnover in behavior technicians working with individuals with autism spectrum disorder. Research in Autism Spectrum Disorder, 17, 106–115. https://doi.org/10.1016/j.rasd.2015.06.012.
Khasne, R. W., Dhakulkar, B. S., Mahajan, H. C., & Kulkarni, A. P. (2020). Burnout among healthcare workers during COVID-19 pandemic in India: Results of a questionnaire-based Survey. Indian Journal of Critical Care Medicine, 24, 664–671. https://doi.org/10.5005/jp-journals-10071-23518.
Lai, J., Ma, S., Wang, Y., Cai, Z., Hu, J., Wei, N., Wu, J., Du, H., Chen, T., Li, R., Tan, H., Kang, L., Yao, L., Huang, M., Wang, H., Wang, G., Liu, Z., & Hu, S. (2020). Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Network Open, 3(3), e203976. https://doi.org/10.1001/jamanetworkopen.2020.3976.
Launer, J. (2020). Burnout in the age of COVID-19. Postgraduate Medical Journal, 96, 367–368. https://doi.org/10.1136/postgradmedj-2020-137980.
Leiter, M. P., & Maslach, C. (1988). The impact of interpersonal environment on burnout and organizational commitment. Journal of Organizational Behavior, 9(4), 297–308. https://doi.org/10.1002/job.4030090402.
Matsuo, T., Kobayashi, D., Taki, F., Sakamoto, F., Uehara, Y., Mori, N., & Fukui, T. (2020). Prevalence of health care worker burnout during the coronavirus disease 2019 (COVID-19) pandemic in Japan. JAMA Network Open, 3(8), e2017271. https://doi.org/10.1001/jamanetworkopen.2020.17271.
McPhillips, D. (2020). The statistical support for closing non-essential businesses. U.S. News. https://www.usnews.com/news/articles/2020-05-18/the-statistical-support-for-closing-non-essential-businesses-during-the-coronavirus-pandemic
Novack, M. N., & Dixon, D. R. (2019). Predictors of burnout, job satisfaction, and turnover in behavior technicians working with individuals with autism spectrum disorder. Review Journal of Autism & Developmental Disorders, 6, 413–421. https://doi.org/10.1007/s40489-019-00171-0.
Oldham, G. R., Kulik, C. T., Stepina, L. P., & Ambrose, M. L. (1986). Relations between situational factors and the comparative referents used by employees. Academy of Management Journal, 29(3), 599–608. https://doi.org/10.5465/256226.
Parke, M. R., Weinhardt, J. M., Brodsky, A., Tangirala, S., & DeVoe, S. E. (2018). When daily planning improves employee performance: The importance of planning type, engagement, and interruptions. Journal of Applied Psychology, 103(3), 300–312. https://doi.org/10.1037/apl0000278.
Plantiveau, C., Dounavi, K., & Virués-Ortega, J. (2018). High levels of burnout among early-career board-certified behavior analysts with low collegial support in the work environment. European Journal of Behavior Analysis, 19(2), 195–207. https://doi.org/10.1080/15021149.2018.1438339.
Rosenberg, N. E., & Schwartz, I. S. (2019). Guidance or compliance: What makes an ethical behavior analyst. Behavior Analysis in Practice, 12(2), 473–482. https://doi.org/10.1007/s40617-018-00287-5.
Serrão, C., Duarte, I., Castro, L., & Teixeira, A. (2021). Burnout and depression in Portuguese healthcare workers during the COVID-19 pandemic-the mediating role of psychological resilience. International Journal of Environmental Research & Public Health, 18(2), 636. https://doi.org/10.3390/ijerph18020636.
Shirom, A., & Melamed, S. (2006). A comparison of the construct validity of two burnout measures in two groups of professionals. International Journal of Stress Management, 13(2), 176–200. https://doi.org/10.1037/1072-5245.13.2.176.
Sinclair, R. R., Allen, T., Barber, L., Bergman, M., Britt, T., Butler, A., Ford, M., Hammer, L., Kath, L., Probst, T., & Yuan, Z. (2020). Occupational health science in the time of COVID-19: Now more than ever. Editorial/Commentary for Occupational Health Science, 4, 1–22. https://doi.org/10.1007/s41542-020-00064-3.
Sinclair, R. R., Probst, T., Watson, G. P., & Bazzoli, A. (2021). Caught between Scylla and Charybdis: How economic stressors and occupational risk factors influence workers’ occupational health reactions to COVID-19. Applied Psychology: An International Review, 70, 85–119. https://doi.org/10.1111/apps.12301.
Talaee, N., Varahram, M., Jamaati, H., Salimi, A., Attarchi, M., Kazempour Dizaji, M., Sadr, M., Hassani, S., Farzanegan, Z., Monjazebi, F., & Seyedmehdi, S. M. (2020). Stress and burnout in health care workers during COVID-19 pandemic: Validation of a questionnaire. Journal of Public Health, 1–6. Advance online publication. https://doi.org/10.1007/s10389-020-01313-z
Tan, B., Kanneganti, A., Lim, L., Tan, M., Chua, Y. X., Tan, L., Sia, C. H., Denning, M., Goh, E. T., Purkayastha, S., Kinross, J., Sim, K., Chan, Y. H., & Ooi, S. (2020). Burnout and associated factors among health care workers in Singapore during the COVID-19 pandemic. Journal of the American Medical Directors Association, 21(12), 1751–1758.e5. https://doi.org/10.1016/j.jamda.2020.09.035.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The authors have no conflicts of interest to declare that are relevant to the content of this article.
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Auburn University Institutional Review Board for the Protection of Human Subjects in Research (IRB protocol #20-177, 04/07/2020).
The approved IRB protocol included a waiver of consent given all data were collected electronically and without identifying information.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix A
Appendix A
Rights and permissions
About this article

Cite this article
Jimenez-Gomez, C., Sawhney, G. & Albert, K.M. Impact of COVID-19 on the Applied Behavior Analysis Workforce: Comparison across Remote and Nonremote Workers. Behav Analysis Practice 14, 873–882 (2021). https://doi.org/10.1007/s40617-021-00625-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40617-021-00625-0