
Incidence, Etiology, and Risk Factors of Clinical Mastitis in Dairy Cows under Semi-Tropical Circumstances in Chattogram, Bangladesh

 , , ,
, , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Herd Selection
2.2. Data Collection
2.3. Case Definition
2.4. Milk Sampling and Laboratory Analysis
2.4.1. Bacteriological Culture
2.4.2. MALDI-TOF Analysis, Real-Time PCR, and MIC
2.5. Statistical Analysis
2.5.1. Descriptive Statistics
2.5.2. Identification of Risk Factors for CM
3. Results
3.1. Herd Characteristics
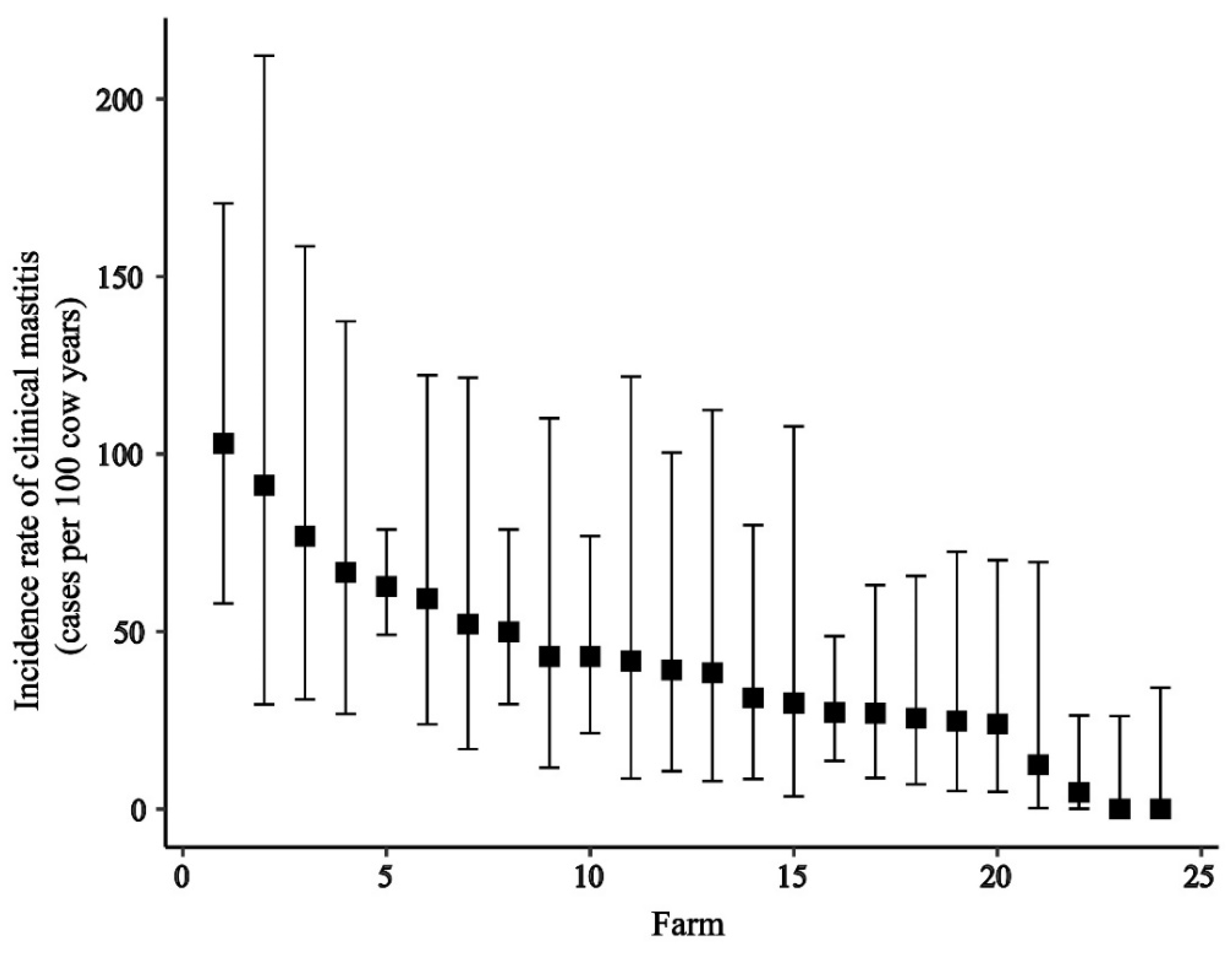
3.2. Incidence Rate of Clinical Mastitis at Different Levels
3.3. Risk Factor Analysis
3.4. Bacteriological Culture Results of Milk Samples from Clinical Mastitis
3.5. MALDI-TOF Testing of Selected Isolates
3.6. MIC Determination and Real-Time PCR
4. Discussion
4.1. Incidence Rate of Clinical Mastitis at Different Levels
4.2. Factors Associated with Clinical Mastitis
4.3. Pathogens Associated with Clinical Mastitis
4.4. Antimicrobial Resistance
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Datta, A.K.; Haider, M.Z.; Ghosh, S.K. Economic analysis of dairy farming in Bangladesh. Trop. Anim. Health Prod. 2019, 51, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Hamid, M.A.; Hossain, K.M. Role of private sector in the development of dairy industry in Bangladesh. Livest. Res. Rural Dev. 2014, 26. [Google Scholar]
- DLS. Livestock Economics Section. Available online: http://dls.portal.gov.bd/sites/default/files/files/dls.portal.gov.bd/page/ee5f4621_fa3a_40ac_8bd9_898fb8ee4700/Livestock%20Economy%20at%20a%20glance%20%20%282017-2018%29.pdf (accessed on 20 February 2020).
- FAO. G.a.I. Dairy Development’s Impact on Poverty Reduction. Available online: http://www.fao.org/3/CA0289EN/ca0289en.pdf (accessed on 20 February 2020).
- DLS. National Livestock Development Policy; Ministry of Fisheries and Livestock, Ed.; Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2007; pp. 18–23.
- Shamsuddin, M.; Ahmed, J.; Alam, M.; Modak, P. Effect of age of semen on conception rate in cattle under farm condition. Bangladesh Vet. J. 1987, 21, 51–58. [Google Scholar]
- Alam, M.G.S.; Ghosh, A. Reproductive performance in cows: Its relation to parity and season. Bangladesh Vet. J. 1988, 22, 51–61. [Google Scholar]
- Curone, G.; Filipe, J.; Cremonesi, P.; Trevisi, E.; Amadori, M.; Pollera, C.; Castiglioni, B.; Turin, L.; Tedde, V.; Vigo, D.; et al. What we have lost: Mastitis resistance in Holstein Friesians and in a local cattle breed. Res. Vet. Sci. 2018, 116, 88–98. [Google Scholar] [CrossRef]
- Islam, M.; Islam, M.; Rahman, M.; Islam, M. Prevalence of subclinical mastitis in dairy cows in selected areas of Bangladesh. Bangladesh J. Vet. Med. 2011, 9, 73–78. [Google Scholar] [CrossRef] [Green Version]
- Hogeveen, H.; Huijps, K.; Lam, T.J. Economic aspects of mastitis: New developments. N. Z. Vet. J. 2011, 59, 16–23. [Google Scholar] [CrossRef]
- Hogeveen, H.; Østerås, O. Mastitis Management in an Economic Framework. In Proceedings of the 4th IDF International Conference, Maastricht, The Netherlands, 11–16 June 2005; pp. 41–52. [Google Scholar]
- Olde Riekerink, R.G.; Barkema, H.W.; Kelton, D.F.; Scholl, D.T. Incidence rate of clinical mastitis on Canadian dairy farms. J. Dairy Sci. 2008, 91, 1366–1377. [Google Scholar] [CrossRef] [PubMed]
- Levison, L.J.; Miller-Cushon, E.K.; Tucker, A.L.; Bergeron, R.; Leslie, K.E.; Barkema, H.W.; DeVries, T.J. Incidence rate of pathogen-specific clinical mastitis on conventional and organic Canadian dairy farms. J. Dairy Sci. 2016, 99, 1341–1350. [Google Scholar] [CrossRef]
- Tomazi, T.; Ferreira, G.C.; Orsi, A.M.; Gonçalves, J.L.; Ospina, P.A.; Nydam, D.V.; Moroni, P.; Dos Santos, M.V. Association of herd-level risk factors and incidence rate of clinical mastitis in 20 Brazilian dairy herds. Prev. Vet. Med. 2018, 161, 9–18. [Google Scholar] [CrossRef]
- Kivaria, F.M.; Noordhuizen, J.P.; Msami, H.M. Risk factors associated with the incidence rate of clinical mastitis in smallholder dairy cows in the Dar es Salaam region of Tanzania. Vet. J. 2007, 173, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Fisseha, D.; Tessema, T.S.; Birhanu, B.T.; Health, A. Aerobic bacterial isolates, incidence rate and associated risk factors of heifer and cow mastitis in and around Debre-Libanos district, Oromia, Ethiopia. J. Vet. Med. 2020, 12, 7–13. [Google Scholar]
- Horpiencharoen, W.; Thongratsakul, S.; Poolkhet, C. Risk factors associated with environmental mastitis in clinical cases at small dairies in western Thailand. Agric. Nat. Resour. 2020, 54, 190–196. [Google Scholar]
- Bradley, A.; Leach, K.A.; Breen, J.; Green, L.; Green, M. Survey of the incidence and aetiology of mastitis on dairy farms in England and Wales. Vet. Rec. 2007, 160, 253–257. [Google Scholar] [CrossRef] [Green Version]
- Santman-Berends, I.M.G.A.; Lam, T.J.G.M.; Keurentjes, J.; van Schaik, G. An estimation of the clinical mastitis incidence per 100 cows per year based on routinely collected herd data. J. Dairy Sci. 2015, 98, 6965–6977. [Google Scholar] [CrossRef] [PubMed]
- Mia, M.T.; Hossain, M.K.; Rumi, N.A.; Rahman, M.S.; Mahmud, M.S.; Das, M. Detection of bacterial species from clinical mastitis in dairy cows at Nilphamari district and their antibiogram studies. Asian J. Med. Biol. Res. 2016, 2, 656–663. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.T.; Islam, M.S.; Hasan, M. Isolation and identification of bacterial agents causing clinical mastitis in Cattle in Mymensingh and their antibiogram Profile. Microbes Health 2013, 2, 19–21. [Google Scholar] [CrossRef]
- Sarker, M.; Aktaruzzaman, M.; Rahman, A.; Rahman, M. Retrospective study of clinical diseases and disorders of cattle in Sirajganj district in Bangladesh. Bangladesh J. Vet. Med. 2013, 11, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Bradley, A.; Green, M. Clinical mastitis in dairy cows after’blitz’therapy. Vet. Rec. 1997, 141, 179–180. [Google Scholar]
- Bradley, A.J.; Green, M.J. Adaptation of Escherichia coli to the bovine mammary gland. J. Clin. Microbiol. 2001, 39, 1845–1849. [Google Scholar] [CrossRef] [Green Version]
- Adkins, P.R.; Middleton, J.R. Sample collection and handling. In Laboratory Handbook on Bovine Mastitis, 3rd ed.; National Mastitis Council: New Prague, MN, USA, 2017. [Google Scholar]
- Hoque, M.N.; Das, Z.C.; Rahman, A.; Haider, M.G.; Islam, M.A. Molecular characterization of Staphylococcus aureus strains in bovine mastitis milk in Bangladesh. Int. J. Vet. Sci. Med. 2018, 6, 53–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salauddin, M.; Akter, M.R.; Hossain, M.K.; Rahman, M.M. Isolation of multi-drug resistant Klebsiella spp. from bovine mastitis samples in Rangpur, Bangladesh. J. Adv. Vet. Anim. Res. 2019, 6, 362. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Abdul Baset, M.; Fouzder, S. Study of Management and Production System of Small Scale Dairy Farm in a Selective Rural Area of Bangladesh. J. Sci. Found. 2013, 8, 13–23. [Google Scholar] [CrossRef] [Green Version]
- Shamsuddoha, A.K.; Edwards, G. Dairy Industry in Bangladesh: Problems and Prospects. In Proceedings of the AARES 2000 Conference, Sydney, Australia, 23–25 January 2000. [Google Scholar]
- Bari, M.; Alam, M.; Uddin, M.R. Prevalence and associated risk factors of bovine clinical mastitis in Patiya upazila under Chittagong district of Bangladesh. Int. J. Nat. Sci. 2014, 4, 5–9. [Google Scholar] [CrossRef]
- Oliveira, C.S.; Hogeveen, H.; Botelho, A.M.; Maia, P.V.; Coelho, S.G.; Haddad, J.P. Cow-specific risk factors for clinical mastitis in Brazilian dairy cattle. Prev. Vet. Med. 2015, 121, 297–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breen, J.E.; Green, M.J.; Bradley, A.J. Quarter and cow risk factors associated with the occurrence of clinical mastitis in dairy cows in the United Kingdom. J. Dairy Sci. 2009, 92, 2551–2561. [Google Scholar] [CrossRef] [Green Version]
- Bhat, A.M.; Soodan, J.S.; Singh, R.; Dhobi, I.A.; Hussain, T.; Dar, M.Y.; Mir, M. Incidence of bovine clinical mastitis in Jammu region and antibiogram of isolated pathogens. Vet. World 2017, 10, 984–989. [Google Scholar] [CrossRef] [Green Version]
- Cheng, J.; Qu, W.; Barkema, H.W.; Nobrega, D.B.; Gao, J.; Liu, G.; De Buck, J.; Kastelic, J.P.; Sun, H.; Han, B. Antimicrobial resistance profiles of 5 common bovine mastitis pathogens in large Chinese dairy herds. J. Dairy Sci. 2019, 102, 2416–2426. [Google Scholar] [CrossRef] [Green Version]
- Tomazi, T.; Freu, G.; Alves, B.G.; de Souza Filho, A.F.; Heinemann, M.B.; Veiga dos Santos, M. Genotyping and antimicrobial resistance of Streptococcus uberis isolated from bovine clinical mastitis. PLoS ONE 2019, 14, e0223719. [Google Scholar] [CrossRef]
- BBS-Chattogram. District. In Agriculture; Statistics and Informatics Division, Ministry of Planning, Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2011; Volume 4, pp. 33–36. [Google Scholar]
- Edmonson, A.J.; Lean, I.J.; Weaver, L.D.; Farver, T.; Webster, G. A Body Condition Scoring Chart for Holstein Dairy Cows. J. Dairy Sci. 1989, 72, 68–78. [Google Scholar] [CrossRef]
- Tolosa, T.; Verbeke, J.; Ayana, Z.; Piepers, S.; Supré, K.; De Vliegher, S. Pathogen group specific risk factors for clinical mastitis, intramammary infection and blind quarters at the herd, cow and quarter level in smallholder dairy farms in Jimma, Ethiopia. Prev. Vet. Med. 2015, 120, 306–312. [Google Scholar] [CrossRef]
- Pinzón-Sánchez, C.; Ruegg, P.L. Risk factors associated with short-term post-treatment outcomes of clinical mastitis. J. Dairy Sci. 2011, 94, 3397–3410. [Google Scholar] [CrossRef] [Green Version]
- Koop, G.; van Werven, T.; Toft, N.; Nielen, M. Estimating test characteristics of somatic cell count to detect Staphylococcus aureus-infected dairy goats using latent class analysis. J. Dairy Sci. 2011, 94, 2902–2911. [Google Scholar] [CrossRef]
- Pichon, B.; Hill, R.; Laurent, F.; Larsen, A.R.; Skov, R.L.; Holmes, M.; Edwards, G.F.; Teale, C.; Kearns, A.M. Development of a real-time quadruplex PCR assay for simultaneous detection of nuc, Panton-Valentine leucocidin (PVL), mecA and homologue mecALGA251. J. Antimicrob. Chemother. 2012, 67, 2338–2341. [Google Scholar] [CrossRef] [Green Version]
- McDonald, R.R.; Antonishyn, N.A.; Hansen, T.; Snook, L.A.; Nagle, E.; Mulvey, M.R.; Levett, P.N.; Horsman, G.B. Development of a triplex real-time PCR assay for detection of Panton-Valentine leukocidin toxin genes in clinical isolates of methicillin-resistant Staphylococcus aureus. J. Clin. Microbiol. 2005, 43, 6147–6149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarker, S.C.; Parvin, M.S.; Rahman, A.K.; Islam, M.T. Prevalence and risk factors of subclinical mastitis in lactating dairy cows in north and south regions of Bangladesh. Trop. Anim. Health Prod. 2013, 45, 1171–1176. [Google Scholar] [CrossRef]
- Shahid, H.; Shafique, O.; Shokat, A. Dairy industry of Pakistan. Eur. J. Bus. Manag. 2012, 4, 1–4. [Google Scholar]
- Janssen, E.; Swinnen, J. Technology adoption and value chains in developing countries: Evidence from dairy in India. Food Policy 2019, 83, 327–336. [Google Scholar] [CrossRef]
- Kalmus, P.; Viltrop, A.; Aasmäe, B.; Kask, K. Occurrence of clinical mastitis in primiparous Estonian dairy cows in different housing conditions. Acta Vet. Scand. 2006, 48, 21. [Google Scholar] [CrossRef] [Green Version]
- Verbeke, J.; Piepers, S.; Supré, K.; De Vliegher, S. Pathogen-specific incidence rate of clinical mastitis in Flemish dairy herds, severity, and association with herd hygiene. J. Dairy Sci. 2014, 97, 6926–6934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rainard, P.; Cunha, P.; Gilbert, F.B. Innate and Adaptive Immunity Synergize to Trigger Inflammation in the Mammary Gland. PLoS ONE 2016, 11, e0154172. [Google Scholar] [CrossRef] [PubMed]
- Sordillo, L.M. Mammary Gland Immunobiology and Resistance to Mastitis. Vet. Clin. N. Am. Food Anim. Pract. 2018, 34, 507–523. [Google Scholar] [CrossRef] [PubMed]
- Green, M.J.; Bradley, A.J.; Medley, G.F.; Browne, W.J. Cow, farm, and management factors during the dry period that determine the rate of clinical mastitis after calving. J. Dairy Sci. 2007, 90, 3764–3776. [Google Scholar] [CrossRef]
- Jamali, H.; Barkema, H.W.; Jacques, M.; Lavallée-Bourget, E.M.; Malouin, F.; Saini, V.; Stryhn, H.; Dufour, S. Invited review: Incidence, risk factors, and effects of clinical mastitis recurrence in dairy cows. J. Dairy Sci. 2018, 101, 4729–4746. [Google Scholar] [CrossRef] [PubMed]
- Rathore, A.K.; Sheldrake, R.F. Teat orifice stretchability associated with teat diameter gradient and milk yield in lactating cows. Anim. Sci. 1977, 24, 215–220. [Google Scholar] [CrossRef]
- Klaas, I.C.; Enevoldsen, C.; Ersbøll, A.K.; Tölle, U. Cow-related risk factors for milk leakage. J. Dairy Sci. 2005, 88, 128–136. [Google Scholar] [CrossRef]
- Schukken, Y.H.; Grommers, F.J.; van de Geer, D.; Erb, H.N.; Brand, A. Risk factors for clinical mastitis in herds with a low bulk milk somatic cell count. 2. Risk factors for Escherichia coli and Staphylococcus aureus. J. Dairy Sci. 1991, 74, 826–832. [Google Scholar] [CrossRef]
- Szyda, J.; Mielczarek, M.; Frąszczak, M.; Minozzi, G.; Williams, J.L.; Wojdak-Maksymiec, K. The genetic background of clinical mastitis in Holstein-Friesian cattle. Animal 2019, 13, 2156–2163. [Google Scholar] [CrossRef] [Green Version]
- Bun, C.; Watanabe, Y.; Uenoyama, Y.; Inoue, N.; Ieda, N.; Matsuda, F.; Tsukamura, H.; Kuwahara, M.; Maeda, K.-I.; Ohkura, S.; et al. Evaluation of heat stress response in crossbred dairy cows under tropical climate by analysis of heart rate variability. J. Vet. Med Sci. 2018, 80, 181–185. [Google Scholar] [CrossRef] [Green Version]
- Mandour, M.; Al-Shami, S.; Al-Eknah, M. Body Condition Scores at Calving and Their Association with Dairy Cow Performance and Health in Semiarid Environment Under Two Cooling Systems. Ital. J. Anim. Sci. 2015, 14. [Google Scholar] [CrossRef] [Green Version]
- Burton, J.L.; Madsen, S.A.; Yao, J.; Sipkovsky, S.S.; Coussens, P.M. An immunogenomics approach to understanding periparturient immunosuppression and mastitis susceptibility in dairy cows. Acta Vet. Scand. 2003, 44, S71. [Google Scholar] [CrossRef] [Green Version]
- Gundelach, Y.; Kalscheuer, E.; Hamann, H.; Hoedemaker, M. Risk factors associated with bacteriological cure, new infection, and incidence of clinical mastitis after dry cow therapy with three different antibiotics. J. Vet. Sci. 2011, 12, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Fadlelmoula, A.; Yousif, I.A.; Nikhaila, A.M. Lactation Curve and Persistency of Crossbred Dairy Cows in the Sudan. J. Appl. Sci. Res. 2007, 3, 1127–1133. [Google Scholar]
- Valckenier, D.; Piepers, S.; Schukken, Y.H.; De Visscher, A.; Boyen, F.; Haesebrouck, F.; De Vliegher, S. Longitudinal study on the effects of intramammary infection with non-aureus staphylococci on udder health and milk production in dairy heifers. J. Dairy Sci. 2021, 104, 899–914. [Google Scholar] [CrossRef]
- Putz, E.J.; Palmer, M.V.; Ma, H.; Casas, E.; Reinhardt, T.A.; Lippolis, J.D. Case report: Characterization of a persistent, treatment-resistant, novel Staphylococcus aureus infection causing chronic mastitis in a Holstein dairy cow. BMC Vet. Res. 2020, 16, 336. [Google Scholar] [CrossRef]
- Rossi, B.F.; Bonsaglia, E.C.R.; Castilho, I.G.; Dantas, S.T.A.; Salina, A.; Langoni, H.; Pantoja, J.C.F.; Budri, P.E.; Fitzgerald-Hughes, D.; Júnior, A.F.; et al. Genotyping of long term persistent Staphylococcus aureus in bovine subclinical mastitis. Microb. Pathog. 2019, 132, 45–50. [Google Scholar] [CrossRef]
- Salih, R.R.M. Bovine mastitis caused by Bacillus spp. in Khartoum State, Sudan. J. Vet. Med. Anim. Prod. 2011; 2, 25–32. [Google Scholar]
- Horpiencharoen, W.; Thongratsakul, S.; Poolkhet, C. Risk factors of clinical mastitis and antimicrobial susceptibility test results of mastitis milk from dairy cattle in western Thailand: Bayesian network analysis. Prev. Vet. Med. 2019, 164, 49–55. [Google Scholar] [CrossRef]
- Rafiullah, R.; Khan, M.A.; Shafee, M.; Akbar, A.; Ali, A.; Shoaib, M.; Ashraf, F.; Khan, N. Occurrence of mastitis and associated pathogens with antibiogram in animal population of Peshawar, Pakistan. Thai J. Vet. Med. 1970, 47, 103–108. [Google Scholar]
- Naccache, S.N.; Callan, K.; Burnham, C.A.; Wallace, M.A.; Westblade, L.F.; Dien Bard, J. Evaluation of Oxacillin and Cefoxitin Disk Diffusion and Microbroth Dilution Methods for Detecting mecA-Mediated β-Lactam Resistance in Contemporary Staphylococcus epidermidis Isolates. J. Clin. Microbiol. 2019, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Level | Status | IRCM 1 per 100 Quarter-Years | 95% CI | Level | Status | IRCM 1 per 100 Cows per Year | 95% CI |
|---|---|---|---|---|---|---|---|
| Quarter level | Overall | 11.6 | 10.2 to 13.3 | Animal level | Overall | 43.9 | 38.2 to 50.5 |
| Grade-1 | 2.8 | 2.1 to 3.6 | Grade-1 | 10.5 | 7.9 to 14.0 | ||
| Grade-2 | 6.5 | 5.5 to 7.8 | Grade-2 | 25.5 | 21.3 to 30.7 | ||
| Grade-3 | 2.4 | 1.8 to 3.2 | Grade-3 | 7.8 | 5.6 to 10.9 | ||
| Quarter position | Front right | 10.8 | 8.3 to 14.2 | ||||
| Front left | 14.2 | 11.1 to 18.0 | |||||
| Hind right | 13.1 | 10.2 to 16.8 | |||||
| Hind left | 8.5 | 6.3 to 11.6 | |||||
| Quarter position | Front | 12.5 | 10.4 to 15.0 | ||||
| Hind | 10.8 | 8.9 to 13.1 |
| Factors | Categories | N 2 | IRCM 3/100 Cows/y | 95% CI (IRCM) | Odds Ratio | 95% CI (OR) | p |
|---|---|---|---|---|---|---|---|
| Body condition score | ≤3 | 427 | 34.9 | 26.5 to 45.9 | Ref | ||
| 3.25 | 488 | 45.7 | 36.0 to 58.0 | 1.3 | 0.9–1.9 | 0.2 | |
| ≥3.5 | 468 | 51.0 | 40.8 to 63.7 | 1.5 | 1.0–2.2 | 0.04 | |
| Parity | 1 | 364 | 42.1 | 31.9 to 55.6 | Ref | ||
| 2 | 354 | 42.9 | 32.4 to 56.8 | 1.1 | 0.7–1.7 | 0.7 | |
| 3 | 279 | 37.5 | 26.9 to 52.2 | 1.1 | 0.7–1.7 | 0.7 | |
| 4 | 214 | 51.8 | 37.2 to 72.1 | 1.3 | 0.8–2.0 | 0.3 | |
| ≥5 | 172 | 51.4 | 35.3 to 75.0 | 1.1 | 0.7–1.9 | 0.7 | |
| Milk yield (L/d) | 10 or less | 462 | 30.8 | 23.0 to 41.3 | Ref | ||
| 10.1–13 | 266 | 38.6 | 27.6 to 54.0 | 1.4 | 0.9–2.3 | 0.1 | |
| 13.1–17 | 328 | 38.8 | 28.8 to 52.4 | 1.4 | 0.9–2.2 | 0.1 | |
| >17 | 327 | 73.0 | 58.1 to 91.7 | 2.8 | 1.9–4.1 | <0.001 | |
| Days in milk | 27 or less | 354 | 51.4 | 38.1 to 69.3 | 1.4 | 0.9–2.2 | 0.2 |
| 28–90 | 392 | 56.2 | 44.9 to 70.4 | 2.1 | 1.3–3.2 | 0.001 | |
| 91–185 | 292 | 38.3 | 28.3 to 51.8 | 1.5 | 0.9–2.4 | 0.1 | |
| >185 | 345 | 29.7 | 21.3 to 41.4 | Ref |
| Factors | Categories | N 2 | Odds Ratio | 95% CI (OR) | p |
|---|---|---|---|---|---|
| Body condition score | ≤3 | 427 | Ref | ||
| 3.25 | 488 | 1.3 | 0.8 to 1.9 | 0.2 | |
| ≥3.5 | 468 | 1.4 | 1.0 to 2.2 | 0.08 | |
| Milk yield (L/d) | 10 or less | 462 | Ref | ||
| 10.1–13 | 266 | 1.3 | 0.8 to 2.1 | 0.3 | |
| 13.1–17 | 328 | 1.4 | 0.9 to 2.2 | 0.2 | |
| >17 | 327 | 2.4 | 1.6 to 3.8 | <0.001 | |
| Days in milk | 27 or less | 354 | 1.1 | 0.7 to 1.8 | 0.7 |
| 28–90 | 392 | 1.6 | 1.0 to 2.7 | 0.03 | |
| 91–185 | 292 | 1.3 | 0.8 to 2.2 | 0.2 | |
| >185 | 345 | Ref |
| Name of Pathogens | n = 153 | % |
|---|---|---|
| Streptococcus spp. | 35 | 22.9 |
| NAS 1 | 31 | 20.3 |
| Bacillus spp. | 29 | 19.0 |
| NGN 2 | 13 | 8.5 |
| E. coli | 11 | 7.2 |
| Staphylococcus aureus | 4 | 2.6 |
| Culture negative | 28 | 18.3 |
| Contaminated | 2 | 1.3 |
| Test Agent | Species | Resistance 1 % (95% CI) | Distribution (n of MICs (µg/mL) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0.03 | 0.06 | 0.12 | 0.25 | 0.5 | 1 | 2 | 4 | 8 | 16 | 32 | 64 | |||
| Penicillin | S. aureus | 66.7 (9.4 to 99.2) | 1 | 2 | ||||||||||
| NAS 2 | 69.2 (52.4 to 83.0) | 4 | 2 | 1 | 5 | 2 | 25 | |||||||
| Cefalotin | S. aureus | 0 (0 to 70.8) | 2 | 1 | ||||||||||
| NAS 2 | 0 (0 to 9.0) | 18 | 9 | 12 | ||||||||||
| Oxacillin + 2% NaCl | S. aureus | 66.7 (9.4 to 99.2) | 1 | 2 | ||||||||||
| NAS2 | 97.4 (86.5 to 99.9) | 1 | 38 | |||||||||||
| Cefoxitin | S. aureus | 33.3 (0.8 to 90.6) | 1 | 1 | 1 | |||||||||
| NAS 2 | - | 3 | 2 | 3 | 5 | 10 | 16 | |||||||
| Enrofloxacin | S. aureus | 0 (0 to 70.8) | 2 | 1 | ||||||||||
| NAS 2 | 25.6 (13.0 to 42.1) | 18 | 11 | 10 | ||||||||||
| Fusidic acid | S. aureus | 33.3 (0.8 to 90.6) | 2 | 1 | ||||||||||
| NAS 2 | 0 (0 to 9.0) | 19 | 7 | 13 | ||||||||||
| Erythromycin | S. aureus | 0 (0 to 70.8) | 3 | |||||||||||
| NAS 2 | 66.7 (49.8 to 80.9) | 13 | 4 | 22 | ||||||||||
| Clindamycin | S. aureus | 0 (0 to 70.8) | 3 | |||||||||||
| NAS 2 | 43.6 (27.8 to 60.4) | 22 | 7 | 10 | ||||||||||
| Gentamycin | S. aureus | 66.7 (9.4 to 99.2) | 1 | 2 | ||||||||||
| NAS 2 | 30.8 (17.0 to 47.6) | 18 | 9 | 12 | ||||||||||
| Nitrofurantoin | S. aureus | 0 (0 to 70.8) | 3 | |||||||||||
| NAS 2 | 5.1 (0.6 to 17.3) | 35 | 1 | 2 | ||||||||||
| Tetracycline | S. aureus | 33.3 (0.8 to 90.6) | 1 | 1 | 1 | |||||||||
| NAS 2 | 43.6 (27.8 to 60.4) | 11 | 7 | 3 | 1 | 17 | ||||||||
| Distribution (n) of MICs (mg/L) | ||||||||||||||
| 0.25/4.75 | 0.5/9.5 | 1/19 | 2/38 | 4/76 | ||||||||||
| Trimethoprim + Sulfamethoxazole | S. aureus | 0 (0 to 70.8) | 2 | 1 | ||||||||||
| NAS 2 | 0 (0 to 9.0) | 13 | 5 | 5 | 4 | 12 | ||||||||
| Incidence Rate (100 Cows/Year) | Quarter Level (100 Quarters/Year) | Number of Cows | Period of the Study | Country | Reference |
|---|---|---|---|---|---|
| 23.3 | - | 12296 | 12 months | Canada | Olde Riekerink et al., 2008 [12] |
| 23.7 | - | 5395 | 14 months | Canada | Levison et al., 2016 [13] |
| - | 35.8 | 4374 | 15 months | Brazil | Tomazi et al., 2018 [14] |
| 43.3 | 38.4 | 317 | 18 months | Tanzania | Kivaria et al., 2007 [15] |
| 32.2 | - | 4947 | 12 months | Netherlands | Santman-Berends et al., 2015 [19] |
| 41.6 | - | 810 | 12 months | UK | Bradley and Green, 2001 [24] |
| 43.9 | 11.6 | 1383 | 6 months | Bangladesh | The present study |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singha, S.; Koop, G.; Persson, Y.; Hossain, D.; Scanlon, L.; Derks, M.; Hoque, M.A.; Rahman, M.M. Incidence, Etiology, and Risk Factors of Clinical Mastitis in Dairy Cows under Semi-Tropical Circumstances in Chattogram, Bangladesh. Animals 2021, 11, 2255. https://doi.org/10.3390/ani11082255
Singha S, Koop G, Persson Y, Hossain D, Scanlon L, Derks M, Hoque MA, Rahman MM. Incidence, Etiology, and Risk Factors of Clinical Mastitis in Dairy Cows under Semi-Tropical Circumstances in Chattogram, Bangladesh. Animals. 2021; 11(8):2255. https://doi.org/10.3390/ani11082255
Chicago/Turabian StyleSingha, Shuvo, Gerrit Koop, Ylva Persson, Delower Hossain, Lauren Scanlon, Marjolein Derks, Md. Ahasanul Hoque, and Md. Mizanur Rahman. 2021. "Incidence, Etiology, and Risk Factors of Clinical Mastitis in Dairy Cows under Semi-Tropical Circumstances in Chattogram, Bangladesh" Animals 11, no. 8: 2255. https://doi.org/10.3390/ani11082255