
Microbiological Changes during Orthodontic Aligner Therapy: A Prospective Clinical Trial

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
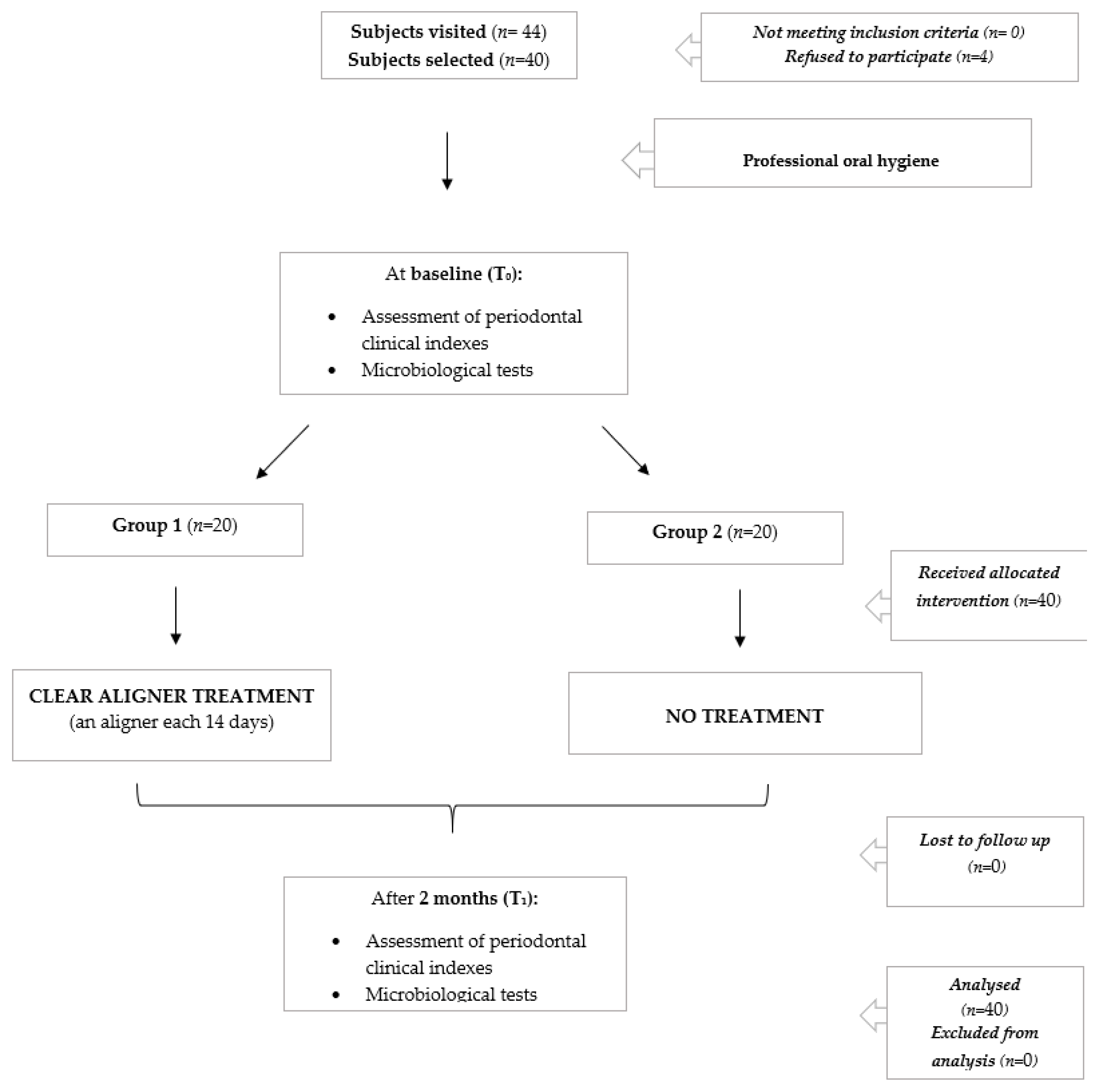
2.1. Trial Design
2.2. Participants
2.3. Interventions and Outcomes
2.4. Sample Size
2.5. Randomisation and Blinding
2.6. Statistical Methods
3. Results
3.1. Periodontal Clinical Indexes
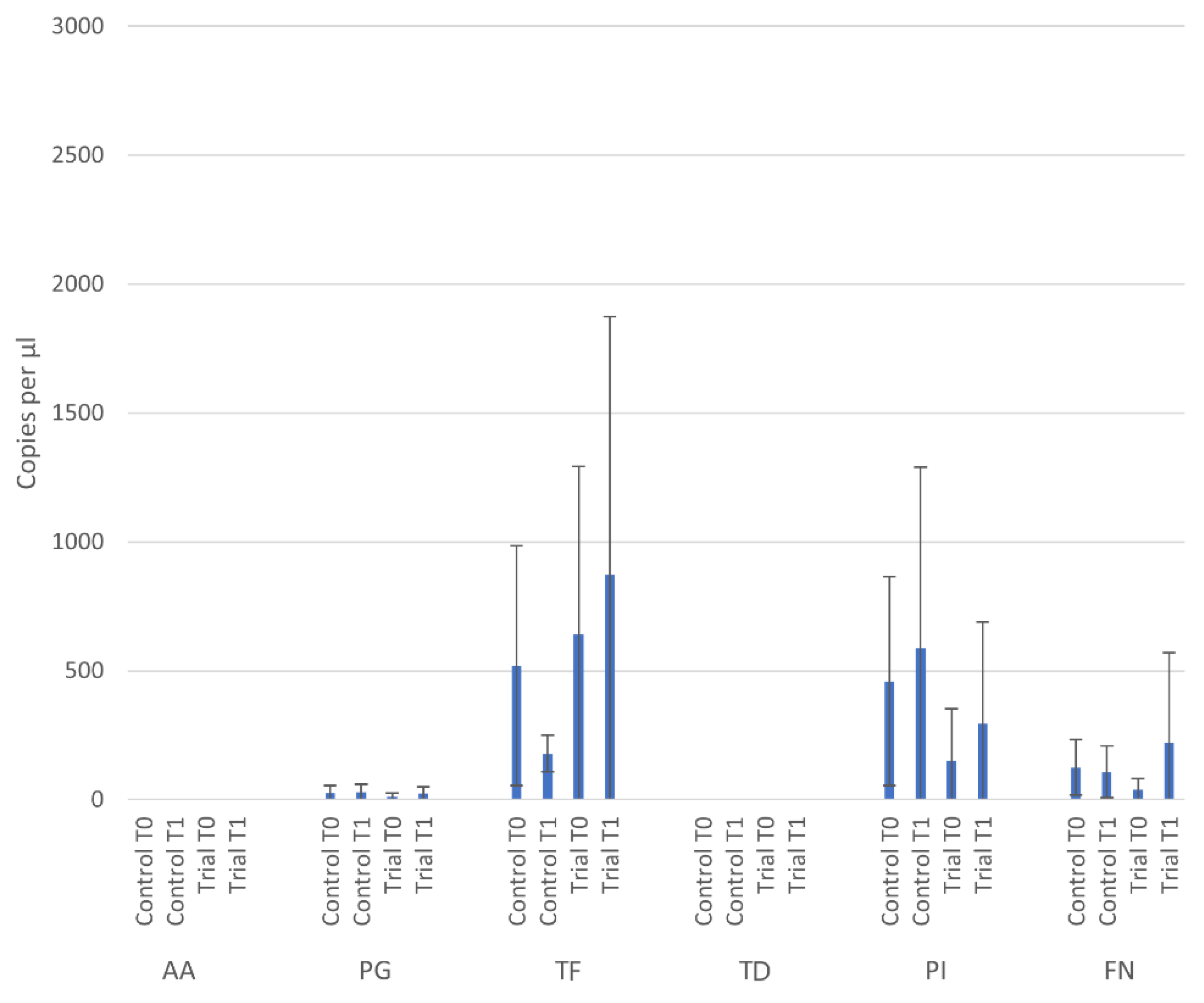
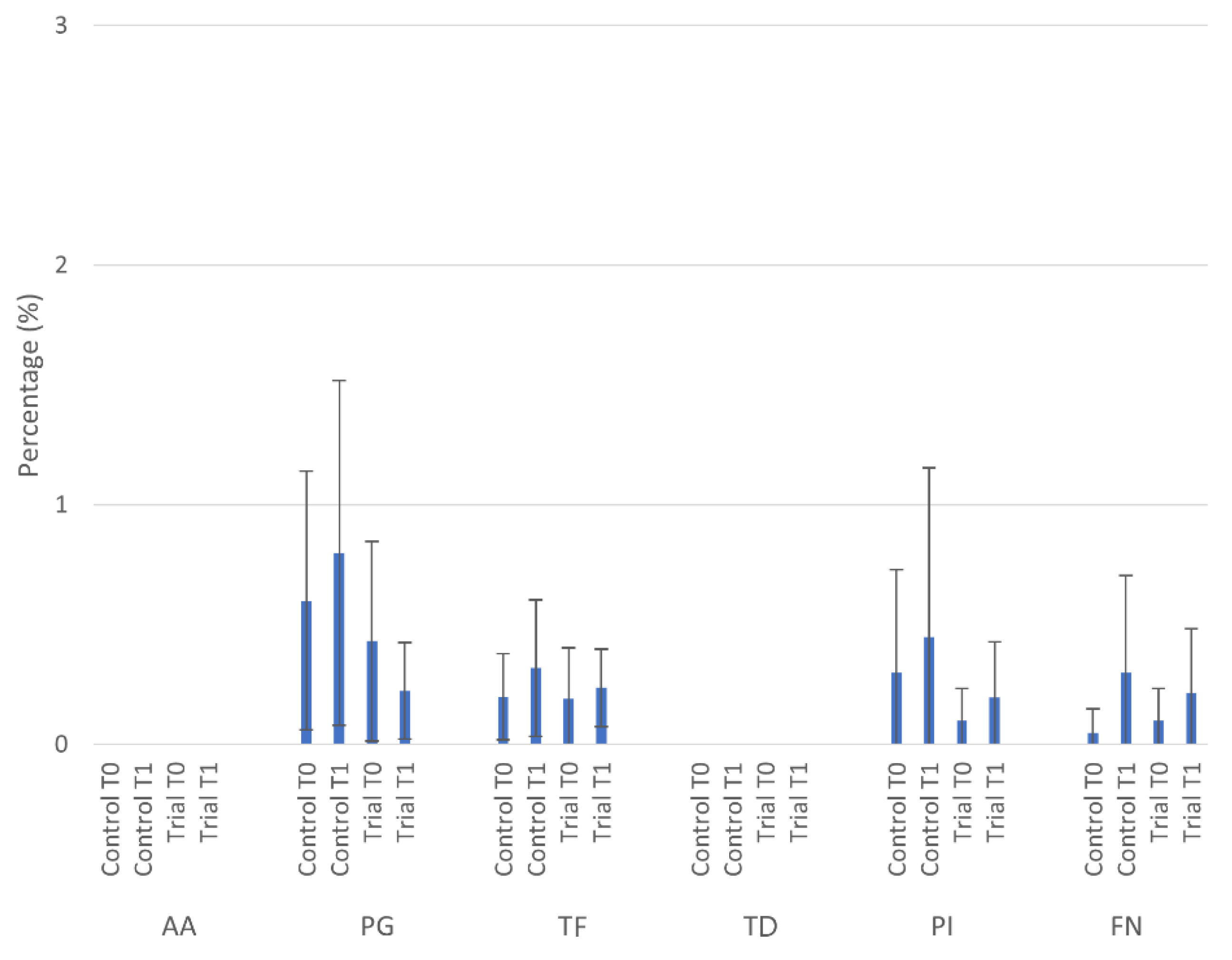
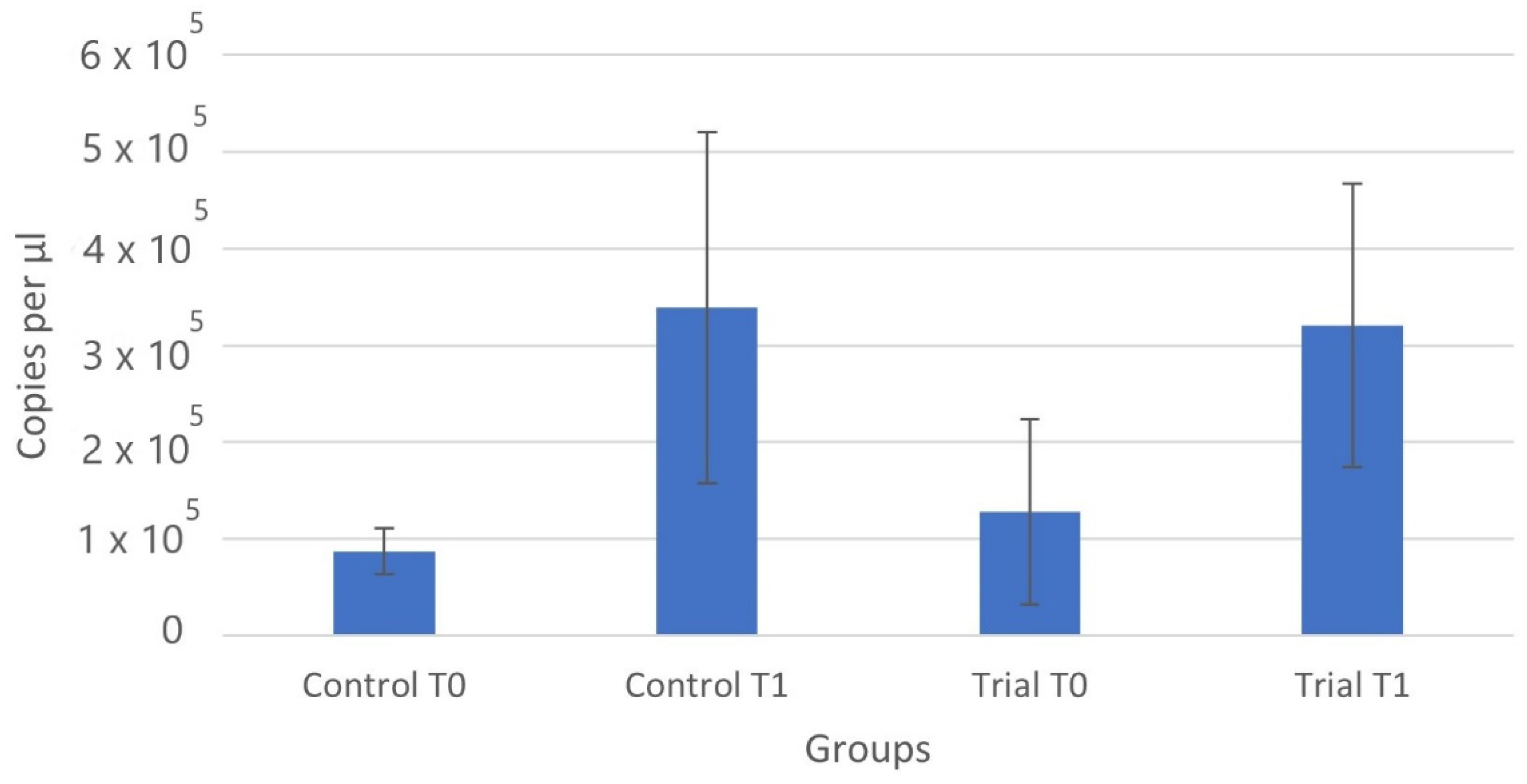
3.2. Microbiological Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xiao, J.; Fiscella, K.A.; Gill, S.R. Oral microbiome: Possible harbinger for children’s health. Int. J. Oral Sci. 2020, 12, 12. [Google Scholar] [CrossRef]
- Lamont, R.J.; Koo, H.; Hajishengallis, G. The oral microbiota: Dynamic communities and host interactions. Nat. Rev. Genet. 2018, 16, 745–759. [Google Scholar] [CrossRef] [PubMed]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45, S1–S8. [Google Scholar] [CrossRef]
- Shirozaki, M.U.; Da Silva, R.A.B.; Romano, F.L.; Da Silva, L.A.B.; De Rossi, A.; Lucisano, M.P.; Messora, M.R.; Feres, M.; Júnior, A.B.N. Clinical, microbiological, and immunological evaluation of patients in corrective orthodontic treatment. Prog. Orthod. 2020, 21, 6. [Google Scholar] [CrossRef] [PubMed]
- Sfondrini, M.F.; Debiaggi, M.; Zara, F.; Brerra, R.; Comelli, M.; Bianchi, M.; Pollone, S.R.; Scribante, A. Influence of lingual bracket position on microbial and periodontal parameters in vivo. J. Appl. Oral Sci. 2012, 20, 357–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, F.; Ahmed, A.; Wang, L.; Dong, M.; Niu, W. Comparison of oral microbiota in orthodontic patients and healthy individuals. Microb. Pathog. 2018, 123, 473–477. [Google Scholar] [CrossRef]
- Awartani, F.; Atassi, F. Oral Hygiene Status among Orthodontic Patients. J. Contemp. Dent. Pract. 2010, 11, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Buschang, P.H.; Chastain, D.; Keylor, C.L.; Crosby, D.; Julien, K.C. Incidence of white spot lesions among patients treated with clear aligners and traditional braces. Angle Orthod. 2018, 89, 359–364. [Google Scholar] [CrossRef] [Green Version]
- D’Apuzzo, F.; Perillo, L.; Carrico, C.K.; Castroflorio, T.; Grassia, V.; Lindauer, S.J.; Shroff, B. Clear aligner treatment: Different perspectives between orthodontists and general dentists. Prog. Orthod. 2019, 20, 10. [Google Scholar] [CrossRef] [Green Version]
- Levrini, L.; Mangano, A.; Montanari, P.; Margherini, S.; Caprioglio, A.; Abbate, G.M. Periodontal health status in patients treated with the Invisalign® system and fixed orthodontic appliances: A 3 months clinical and microbiological evaluation. Eur. J. Dent. 2015, 9, 404–410. [Google Scholar] [CrossRef]
- Karkhanechi, M.; Chow, D.; Sipkin, J.; Sherman, D.; Boylan, R.J.; Norman, R.G.; Craig, R.G.; Cisneros, G.J. Periodontal status of adult patients treated with fixed buccal appliances and removable aligners over one year of active orthodontic therapy. Angle Orthod. 2013, 83, 146–151. [Google Scholar] [CrossRef]
- Abbate, D.G.; Caria, M.; Montanari, P.; Mannu, C.; Orrù, G.; Caprioglio, A.; Levrini, L. Periodontal health in teenagers treated with removable aligners and fixed orthodontic appliances. J. Orofac. Orthop. 2015, 76, 240–250. [Google Scholar] [CrossRef]
- Alqerban, A. Levels of proinflammatory chemokines and advanced glycation end products in patients with type-2 diabetes mellitus undergoing fixed orthodontic treatment. Angle Orthod. 2021, 91, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Corbett, A.I.; Leggitt, V.L.; Angelov, N.; Olson, G.; Caruso, J.M. Periodontal health of anterior teeth with two types of fixed retainers. Angle Orthod. 2014, 85, 699–705. [Google Scholar] [CrossRef] [Green Version]
- Ross, M.C.; Campbell, P.M.; Tadlock, L.P.; Taylor, R.W.; Buschang, P.H. Effect of automated messaging on oral hygiene in adolescent orthodontic patients: A randomized controlled trial. Angle Orthod. 2019, 89, 262–267. [Google Scholar] [CrossRef] [Green Version]
- Sifakakis, I.; Papaioannou, W.; Papadimitriou, A.; Kloukos, D.; Papageorgiou, S.N.; Eliades, T. Salivary levels of cariogenic bacterial species during orthodontic treatment with thermoplastic aligners or fixed appliances: A prospective cohort study. Prog. Orthod. 2018, 19, 25. [Google Scholar] [CrossRef] [Green Version]
- Gomes, S.C.; Varela, C.C.; Da Veiga, S.L.; Rosing, C.; Oppermann, R.V. Periodontal conditions in subjects following orthodontic therapy. A preliminary study. Eur. J. Orthod. 2007, 29, 477–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calniceanu, H.; Stratul, S.-I.; Rusu, D.; Jianu, A.; Boariu, M.; Nica, L.; Ogodescu, A.; Sima, L.; Bolintineanu, S.; Anghel, A.; et al. Changes in clinical and microbiological parameters of the periodontium during initial stages of orthodontic movement in patients with treated severe periodontitis: A longitudinal site-level analysis. Exp. Ther. Med. 2020, 20, 199. [Google Scholar] [CrossRef] [PubMed]
- Diedrich, P.; Rudzki-Janson, I.; Wehrbein, H.; Fritz, U. Effects of orthodontic bands on marginal periodontal tissues. A histologic study on two human specimens. J. Orofac. Orthop. 2001, 62, 146–156. [Google Scholar] [CrossRef]
- Ghijselings, E.; Coucke, W.; Verdonck, A.; Teughels, W.; Quirynen, M.; Pauwels, M.; Carels, C.; Van Gastel, J. Long-term changes in microbiology and clinical periodontal variables after completion of fixed orthodontic appliances. Orthod. Craniofacial Res. 2013, 17, 49–59. [Google Scholar] [CrossRef]
- Cosola, S.; Giammarinaro, E.; Genovesi, A.M.; Pisante, R.; Poli, G.; Covani, U.; Marconcini, S. A short-term study of the effects of ozone irrigation in an orthodontic population with fixed appliances. Eur. J. Paediatr. Dent. 2019, 20, 15–18. [Google Scholar] [PubMed]
- Miethke, R.-R.; Brauner, K. A Comparison of the Periodontal Health of Patients during Treatment with the Invisalign® System and with Fixed Lingual Appliances. J. Orofac. Orthop. 2007, 68, 223–231. [Google Scholar] [CrossRef]
- Azaripour, A.; Weusmann, J.; Mahmoodi, B.K.; Peppas, D.; Gerhold-Ay, A.; Van Noorden, C.J.F.; Willershausen, B. Braces versus Invisalign®: Gingival parameters and patients’ satisfaction during treatment: A cross-sectional study. BMC Oral Health 2015, 15, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, H.; Tang, H.; Zhou, T.; Kang, N. Assessment of the periodontal health status in patients undergoing orthodontic treatment with fixed appliances and Invisalign system: A meta-analysis. Medicine 2018, 97, e0248. [Google Scholar] [CrossRef]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Periodontal health during clear aligners treatment: A systematic review. Eur. J. Orthod. 2015, 37, 539–543. [Google Scholar] [CrossRef]
- Guo, R.; Zheng, Y.; Liu, H.; Li, X.; Jia, L.; Li, W. Profiling of subgingival plaque biofilm microbiota in female adult patients with clear aligners: A three-month prospective study. PeerJ 2018, 6, e4207. [Google Scholar] [CrossRef] [Green Version]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2021, 9, 69. [Google Scholar] [CrossRef]
- Preda, C.; Butera, A.; Pelle, S.; Pautasso, E.; Chiesa, A.; Esposito, F.; Oldoini, G.; Scribante, A.; Genovesi, A.; Cosola, S. The Efficacy of Powered Oscillating Heads vs. Powered Sonic Action Heads Toothbrushes to Maintain Periodontal and Peri-Implant Health: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 1468. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Probing Pocket Depth (mm) | Measurement from the Free Gingival Margin to the Bottom of the Periodontal Pocket by Means of a Millimetre Probe |
|---|---|
| Bleeding on Probing (%) | 0—no bleeding upon 20 s after probing 1—bleeding upon 20 s after probing BOP is calculated as the ratio between the number of bleeding sites and the total sites evaluated (expressed as percentage) |
| Plaque Index (Score 0–3) | 0—No plaque 1—Thin plaque layer at the margin, only detectable by scraping with a probe 2—Moderate layer of plaque along gingival margin; interdental spaces free, but plaque is visible to the naked eye 3—Abundant plaque along to the gingival margin; interdental spaces filled with plaque |
| Group | Procedures |
|---|---|
| GROUP 1 (Trial Group) | Signature of the informed consent for the study Professional oral hygiene and motivation to the domiciliary oral hygiene After 14 days from the professional oral hygiene, assessment of periodontal clinical indexes and execution of microbiological tests (T0) Delivery of the first clear alignment and change each 14 days After 2 months from T0, re-assessment of periodontal clinical indexes and re-execution of microbiological tests (T1) |
| GROUP 2 (Control Group) | Signature of the informed consent for the study Professional oral hygiene and motivation to the domiciliary oral hygiene After 14 days from the professional oral hygiene, assessment of periodontal clinical indexes and execution of microbiological tests (T0) After 2 months from T0, re-assessment of periodontal clinical indexes and re-execution of microbiological tests (T1) |
| Variable | Group | Mean | SD | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| PPD (mm) | Control T0 | 2.26 | 0.40 | 1.53 | 2.42 | 2.61 | p > 0.05 |
| Control T1 | 2.12 | 0.35 | 1.78 | 2.06 | 2.78 | ||
| Trial T0 | 1.89 | 0.46 | 1.17 | 1.81 | 3.00 | ||
| Trial T1 | 1.99 | 0.51 | 0.64 | 2.17 | 2.47 | ||
| BOP (%) | Control T0 | 5.98 | 10.53 | 0.00 | 1.00 | 38.91 | p > 0.05 |
| Control T1 | 7.57 | 10.50 | 0.00 | 4.92 | 36.10 | ||
| Trial T0 | 4.55 | 5.05 | 0.00 | 2.52 | 15.00 | ||
| Trial T1 | 4.08 | 5.50 | 0.00 | 1.80 | 15.00 | ||
| PI (0–4) | Control T0 | 0.50 | 0.46 | 0.00 | 0.38 | 1.58 | p > 0.05 |
| Control T1 | 0.57 | 0.54 | 0.00 | 0.46 | 1.78 | ||
| Trial T0 | 0.39 | 0.22 | 0.00 | 0.36 | 0.78 | ||
| Trial T1 | 0.30 | 0.23 | 0.00 | 0.25 | 0.65 |
| Bacteria Type | Group | Mean | SD | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| Aggregatibacter actinomycetemcomitans | Control T0 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | p > 0.05 |
| Control T1 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Trial T0 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Trial T1 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Porphyromonas gingivalis | Control T0 | 26.63 | 61.50 | 0.00 | 0.00 | 223.00 | p > 0.05 |
| Control T1 | 29.47 | 65.88 | 0.00 | 0.00 | 223.00 | ||
| Trial T0 | 12.15 | 31.76 | 0.00 | 0.00 | 102.00 | ||
| Trial T1 | 23.15 | 61.75 | 0.00 | 0.00 | 199.00 | ||
| Tannerella forsythia | Control T0 | 520.00 | 1034.57 | 0.00 | 0.00 | 2470.00 | p > 0.05 |
| Control T1 | 178.74 | 157.84 | 0.00 | 158.00 | 351.00 | ||
| Trial T0 | 641.00 | 1487.69 | 0.00 | 0.00 | 4720.00 | ||
| Trial T1 | 874.60 | 2280.12 | 0.00 | 0.00 | 7480.00 | ||
| Treponema denticola | Control T0 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | p > 0.05 |
| Control T1 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Trial T0 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Trial T1 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Prevotella intermedia | Control T0 | 459.16 | 901.71 | 0.00 | 0.00 | 2650.00 | p > 0.05 |
| Control T1 | 586.84 | 1562.15 | 0.00 | 0.00 | 6600.00 | ||
| Trial T0 | 150.00 | 461.69 | 0.00 | 0.00 | 1500.00 | ||
| Trial T1 | 294.40 | 901.37 | 0.00 | 0.00 | 2930.00 | ||
| Fusobacterium nucleatum | Control T0 | 125.21 | 238.97 | 0.00 | 0.00 | 712.00 | p > 0.05 |
| Control T1 | 107.58 | 223.23 | 0.00 | 0.00 | 766.00 | ||
| Trial T0 | 38.45 | 97.81 | 0.00 | 0.00 | 305.00 | ||
| Trial T1 | 220.85 | 797.48 | 0.00 | 0.00 | 3590.00 |
| Bacteria Type | AA | Mean | SD | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| Aggregatibacter actinomycetemcomitans | Control T0 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | p > 0.05 |
| Control T1 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Trial T0 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Trial T1 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Porphyromonas gingivalis | Control T0 | 0.60 | 1.23 | 0.00 | 0.00 | 3.00 | p > 0.05 |
| Control T1 | 0.80 | 1.64 | 0.00 | 0.00 | 4.00 | ||
| Trial T0 | 0.43 | 0.95 | 0.00 | 0.00 | 3.00 | ||
| Trial T1 | 0.22 | 0.46 | 0.00 | 0.00 | 2.00 | ||
| Tannerella forsythia | Control T0 | 0.20 | 0.41 | 0.00 | 0.00 | 1.00 | p > 0.05 |
| Control T1 | 0.32 | 0.65 | 0.00 | 0.00 | 1.59 | ||
| Trial T0 | 0.19 | 0.49 | 0.00 | 0.00 | 1.59 | ||
| Trial T1 | 0.24 | 0.37 | 0.00 | 0.00 | 0.87 | ||
| Treponema denticola | Control T0 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | p > 0.05 |
| Control T1 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Trial T0 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Trial T1 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Prevotella intermedia | Control T0 | 0.30 | 0.98 | 0.00 | 0.00 | 4.00 | p > 0.05 |
| Control T1 | 0.45 | 1.61 | 0.00 | 0.00 | 7.00 | ||
| Trial T0 | 0.10 | 0.31 | 0.00 | 0.00 | 1.00 | ||
| Trial T1 | 0.20 | 0.53 | 0.00 | 0.00 | 1.73 | ||
| Fusobacterium nucleatum | Control T0 | 0.05 | 0.22 | 0.00 | 0.00 | 1.00 | p > 0.05 |
| Control T1 | 0.30 | 0.92 | 0.00 | 0.00 | 4.00 | ||
| Trial T0 | 0.10 | 0.31 | 0.00 | 0.00 | 1.00 | ||
| Trial T1 | 0.22 | 0.61 | 0.00 | 0.00 | 2.00 |
| Group | Mean | SD | Min | Median | Max | Intergroup Differences * | Intragroup Differences * |
|---|---|---|---|---|---|---|---|
| Control T0 | 86,800 | 54,597 | 19,000 | 100,000 | 166,000 | p < 0.05 | T0–T0: p > 0.05 T1–T1: p > 0.05 |
| Control T1 | 338,960 | 414,281 | 67,800 | 100,000 | 1,130,000 | ||
| Trial T0 | 128,010 | 219,412 | 1480 | 4270 | 546,000 | p < 0.05 | |
| Trial T1 | 320,960 | 334,473 | 78,400 | 260,000 | 1,260,000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sfondrini, M.F.; Butera, A.; Di Michele, P.; Luccisano, C.; Ottini, B.; Sangalli, E.; Gallo, S.; Pascadopoli, M.; Gandini, P.; Scribante, A. Microbiological Changes during Orthodontic Aligner Therapy: A Prospective Clinical Trial. Appl. Sci. 2021, 11, 6758. https://doi.org/10.3390/app11156758
Sfondrini MF, Butera A, Di Michele P, Luccisano C, Ottini B, Sangalli E, Gallo S, Pascadopoli M, Gandini P, Scribante A. Microbiological Changes during Orthodontic Aligner Therapy: A Prospective Clinical Trial. Applied Sciences. 2021; 11(15):6758. https://doi.org/10.3390/app11156758
Chicago/Turabian StyleSfondrini, Maria Francesca, Andrea Butera, Pietro Di Michele, Claudia Luccisano, Beatrice Ottini, Enrico Sangalli, Simone Gallo, Maurizio Pascadopoli, Paola Gandini, and Andrea Scribante. 2021. "Microbiological Changes during Orthodontic Aligner Therapy: A Prospective Clinical Trial" Applied Sciences 11, no. 15: 6758. https://doi.org/10.3390/app11156758