Article Text

Abstract
Introduction The burden of type 2 diabetes mellitus (T2DM) and related vascular complications is particularly high in Asians and ethnic minorities living in the West. However, the association of T2DM with socioeconomic status (SES) and ethnicity has not been widely studied in populations living in Asia. Therefore, we investigated these associations among the multiethnic population with uncontrolled hypertension in Singapore.
Research design and methods In a cross-sectional study using baseline data of a 2-year randomized trial in Singapore, we obtained demographic, SES, lifestyle and clinical factors from 915 patients aged ≥40 years with uncontrolled hypertension. T2DM was defined as having either: (i) self-reported ‘physician-diagnosed diabetes confirmed through medical records’ or taking antidiabetes medications, (ii) fasting blood glucose levels ≥7.0 mmol/dL or (iii) hemoglobin A1c ≥6.5%. The SES proxies included education, employment status, housing ownership and housing type, and the ethnicities were Chinese, Malays and Indians. Logistic regression analyses were used to evaluate the association of T2DM with SES and ethnicity.
Results Higher proportion of T2DM was observed in Malays (40.0%) and Indians (56.0%) than Chinese (26.8%) (p<0.001), and in patients with lower SES (ranging from 25.7% to 66.2% using different proxies) than those with higher SES (19.4% to 32.0%). In a multivariate model comprising age, gender, ethnicity and SES, Malay ethnicity (OR 1.59; 95% CI 1.04 to 2.44, p=0.031) or Indian ethnicity (OR 3.65; 95% CI 2.25 to 5.91, p<0.001) versus Chinese and housing type (residing in one to three rooms (OR 2.00; 95% CI 1.16 to 3.43, p=0.012) or four to five rooms public housing (OR 1.86; 95% CI 1.13 to 3.04, p=0.013) vs private housing) were associated with higher T2DM odds. The associations of Indians and one to three rooms public housing with T2DM met the significance after accounting for multiple testing (p≤0.0125).
Conclusion Our study suggests that housing type and ethnic variation are independently associated with higher T2DM risk in patients with uncontrolled hypertension in Singapore. Further studies are needed to validate our results.
Trial registration number NCT02972619.
- epidemiology
- ethnicity
- hypertension
- socioeconomic status
Data availability statement
Data are available on reasonable request from THJ subject to approval by SingHypertension IRB.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Identifying type 2 diabetes mellitus (T2DM) in patients with uncontrolled hypertension is crucial to the prevention of vascular complications.
The association between T2DM and socioeconomic status (SES) has not been consistent.
Higher risk of T2DM has been shown to be associated with lower SES in high-income countries, and with higher SES in low-income and middle-income countries in the general population.
South Asians have been shown to have higher risk of T2DM compared with other ethnicities due to a complex interplay of risk factors.
However, the independent association between SES and ethnicity with T2DM in the Asian population with uncontrolled hypertension is not clear yet.
What are the new findings?
A significant association of T2DM with Indian ethnicity (vs Chinese) and housing type (public housing vs private housing) independent of other sociodemographic factors was observed in patients with uncontrolled hypertension seeking care at the polyclinics in Singapore.
How might these results change the focus of research or clinical practice?
From the perspective of clinical practice, our results implied that identifying and risk stratifying patients with uncontrolled hypertension at T2DM risk using ethnicity and housing type may be beneficial for targeted public health services to reduce inequities in T2DM and developing personalised and ethnicity-centric interventions to prevent and manage T2DM in patients with uncontrolled hypertension in Singapore.
Introduction
The prevalence of type 2 diabetes mellitus (T2DM) is increasing globally. According to the International Diabetes Federation, the total adult population with diabetes in the world is 463 million, out of which approximately 90% have T2DM.1 T2DM is associated with vascular complications such as kidney failure, blindness, lower limb amputation, ischemic heart disease and stroke.2 Additionally, in the USA approximately 74% of patients with diabetes have co-existing uncontrolled hypertension, which further elevates the risk of vascular diseases.3 Furthermore, clinical trials have demonstrated the importance of blood pressure (BP) control to prevent macrovascular and microvascular diseases in patients with diabetes and co-existing hypertension.4 Thus, preventing and treating T2DM early in patients with uncontrolled hypertension is crucial.
The influence of socioeconomic status (SES) on the health of individuals has been widely researched in recent times. SES is a complex concept that describes the position an individual occupies in the society.5 An individual’s SES can be described by various factors such as income, education, occupational class and residential locations or housing type.6 As these social and economic factors determine the availability of healthcare resources, occupational opportunity and affordability for healthier lifestyle choices, the differences in SES may subsequently impact health outcomes including T2DM.6 Some studies have shown that SES is associated with T2DM.7–14 Interestingly, studies conducted in high-income countries such as the UK, Canada, Korea and Australia found that lower SES was associated with higher T2DM risk,7–10 13 while studies in low- and middle-income countries such as Bangladesh, India and Nigeria showed the opposite.11 12 14
Another factor that may influence disease risk profiles including T2DM is ethnicity. The differences in environmental, socioeconomic, physiological, genetic and behavioural factors amid ethnic groups may have resulted in differential relationships between risk factors and disease outcomes.15 Evidence suggested that South Asians have higher T2DM risk compared with other ethnicities, often with earlier onset and poorer outcomes.16 The racial and ethnic predisposition for T2DM arises from a complex interplay between risk factors such as genetics, environmental, lifestyle and dietary-related factors over the life course of Asians.16 Thus, SES could be a potential confounding factor between the ethnicity-T2DM association.17 So far, very few studies have investigated the independent association between SES and ethnicity with T2DM. However, the associations of T2DM with SES and ethnicity have not been investigated in an Asian population with uncontrolled hypertension.
Singapore is a high-income Asian country with heavy burden of T2DM and hypertension. The overall prevalence of T2DM in Singapore has increased from 8% in 2004 to 14.2% in 2019.1 18 According to the 2010 National Health Survey Singapore, 23.5% of adults aged 30 years or older suffered from hypertension.19 Out of these, about 32% have uncontrolled hypertension.19 In addition, Singapore has three major ethnic groups of Chinese (74.3%), Malays (13.4%) and Indians (9.0%).20 In the general population, Indians (17.2%) and Malays (16.6%) have higher T2DM prevalence than Chinese (9.7%).19 However, it remains unclear if ethnicity is associated with T2DM among people with hypertension in Singapore, and whether the ethnic differences could be explained by SES. Since patients with uncontrolled hypertension have elevated risk of T2DM and its complications,4 21 understanding the association of SES and ethnic variation with T2DM is key to identify high-risk patients and develop targeted public health strategies to prevent diabetes among patients with uncontrolled hypertension.
Therefore, we conducted this study to investigate the independent association of SES and ethnic variation with T2DM among patients with uncontrolled hypertension visiting the primary care clinics in Singapore. We hypothesize that higher T2DM odds is independently associated with lower SES (education levels, employment status, housing ownership and housing types) in the study population.
Research design and methods
Patient recruitment
The SingHypertension study is a 2-year cluster randomised controlled trial in Singapore which evaluated the effect of a multicomponent intervention in lowering BP compared with usual care.22 Singapore citizens or permanent residents aged 40 years or older have visited the recruiting polyclinic at least twice in 2017–2018, and have uncontrolled BP (systolic BP ≥140 mm Hg or diastolic BP ≥90 mm Hg) were included in the study. Individuals with active systemic illness including fever, recent hospitalisation, clinically unstable heart failure or advanced kidney disease (estimated Chronic Kidney Disease-Epidemiology Collaboration glomerular filtration rate <40 mL/min/1.73m2 or nephrotic range proteinuria (ie, ≥3 g/day)), with known liver disease, who are pregnant or breast feeding or with any other major debilitating disease or mental illness that precludes validity of informed consent were excluded.
Individuals diagnosed with hypertension or on antihypertensive medications visiting the polyclinics involved in the SingHypertension study were approached by the trained clinical research coordinator (CRC) at the health monitoring station or the laboratory when they presented for their annual panel tests (fasting blood and urine tests) and invited to be screened for eligibility to participate in the study. All the patients underwent a computerized cardiovascular disease (CVD) risk scoring at triage and had their BP measured thrice, in the sitting position with arm rested, using a digital device (OMRON HEM-7130) by the CRC as part of prescreening. The average of the last two of three BP readings, obtained 3 min apart, was used to confirm eligibility. Those with systolic BP ≥140 mm Hg or diastolic BP ≥90 mm Hg were considered to have uncontrolled hypertension, in accordance to the Eight Joint National Committee Criteria 2014.23 The CRC obtained written informed consent from eligible individuals. Following that, the CRC administered questionnaires via a face-to-face interview to obtain information on the individuals’ sociodemographics, comorbidities, diet, lifestyle, tobacco use and quality of life.
Current study population
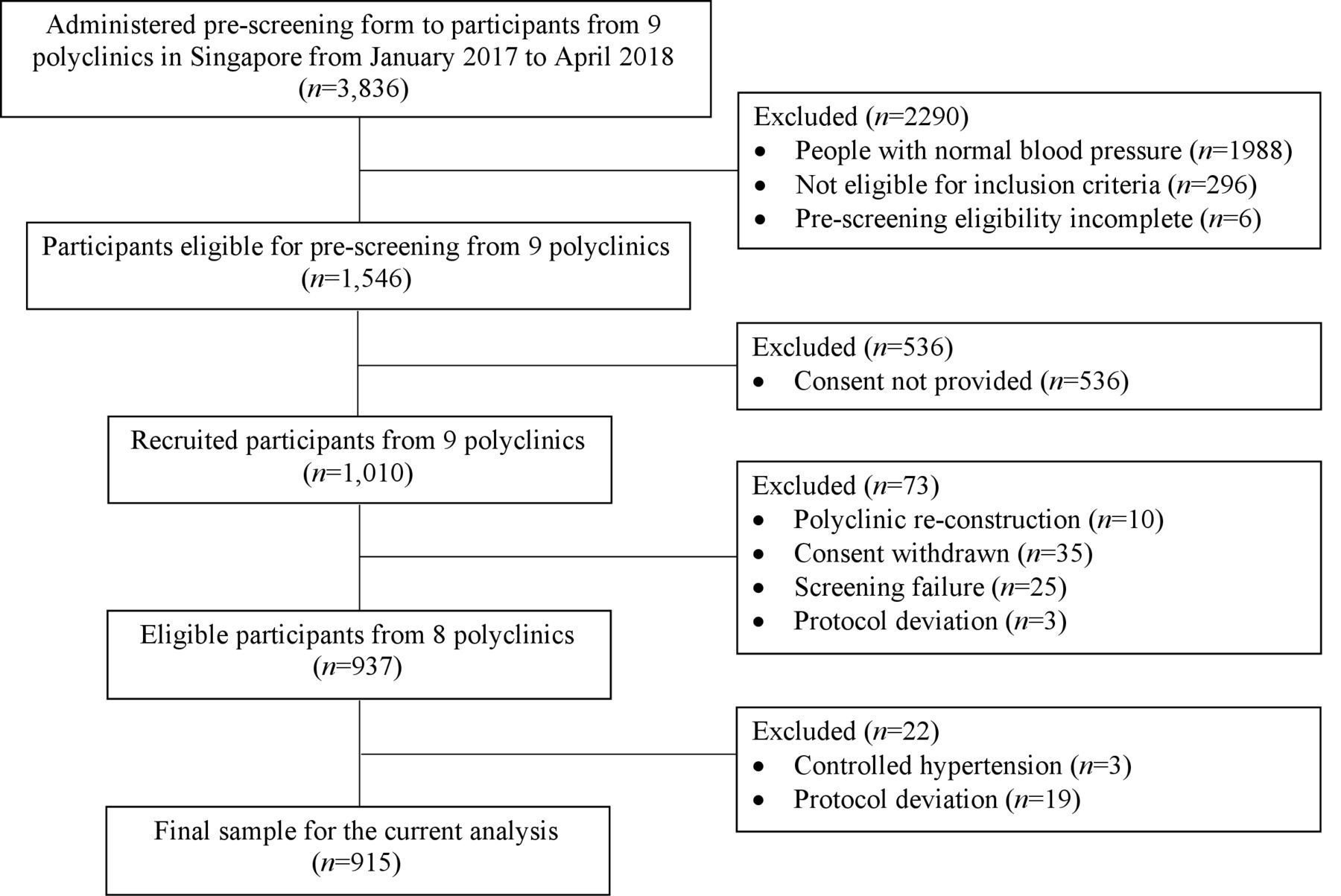
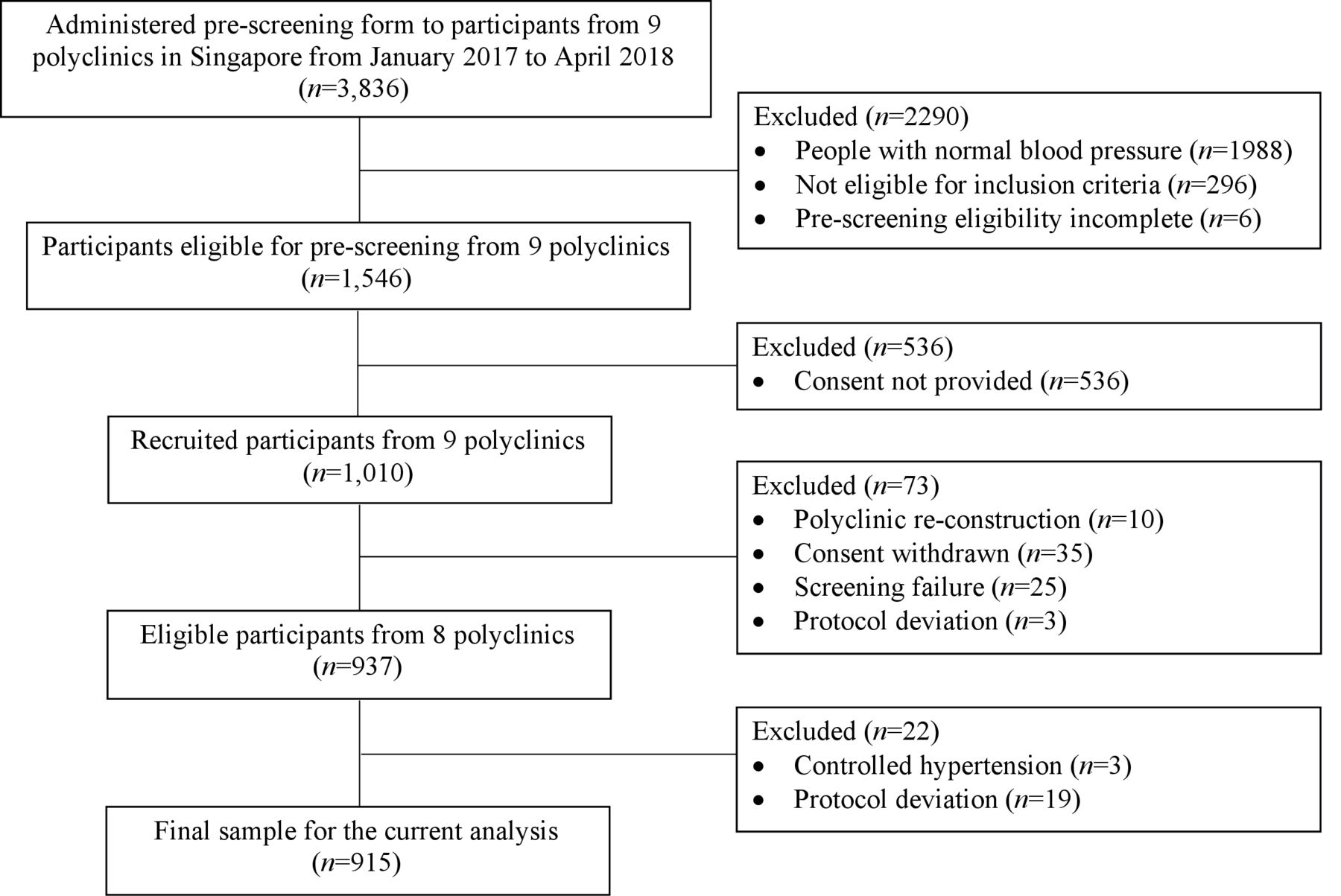
The current study used the baseline data of the SingHypertension study. A total of 1010 patients were recruited between January 2017 and April 2018.22 Among them, 73 participants were excluded (screening failure (n=25), consent withdrawn (n=35), polyclinic reconstruction (n=10) and protocol deviation (n=3)), leaving 937 participants enrolled in the current study. A total of 22 participants who had controlled hypertension (n=3) and protocol deviation (n=19) were further excluded and the final sample size for the current analysis was 915. The flow chart of the current study design is shown in figure 1.
{kind=link}
Flow chart of SingHypertension and current study design.
Assessment of primary outcome
T2DM was defined as meeting one of the three criteria: (i) self-reported ‘physician-diagnosed diabetes confirmed through medical records’ or taking antidiabetes medications, (ii) fasting blood glucose levels ≥7.0 mmol/dL or (iii) hemoglobin A1c (HbA1c) ≥6.5%. The thresholds of blood tests were based on 2019 American Diabetes Association recommendations on the diagnosis of diabetes.24 Each participant received a panel test of blood biomarkers at a subsidised cost including glucose indices (fasting blood glucose and HbA1c). Glucose measurements were assayed on the Roche Cobas c702 automated chemistry using Roche Diagnostics Glucose reagent.
Assessment and definition of variables
A face-to-face interview was conducted by the CRC with each participant using structured questionnaires as described below. Information on the demographics, SES, lifestyle and some clinical factors were collected as described below.
Demographic variables
Age was categorized as ‘40–65 years old’ and ‘>65 years old’. Ethnicity was categorized as ‘Chinese’, ‘Malays’, ‘Indians’ and ‘others’. In the general population in Singapore, 74.3% were Chinese, 13.4% were Malays and 9.0% were Indians.20
SES variables
Four variables were used as proxies for SES: (i) education levels, (ii) current employment status, (iii) living in rental housing and (iv) housing types. Education levels were categorised into ‘primary school and below’ and ‘secondary school and above’. Current employment status was classified as ‘employed’ and ‘unemployed’ while ‘living in rental housing’ was classified as ‘yes’ and ‘no’. Housing types were categorised into ‘private housing’ (condominium, other apartments and landed properties) and ‘public housing’. Public housing was further classified into ‘one to three rooms’ and ‘four to five rooms’. Housing type in Singapore is positively correlated with household income and often used as a surrogate of income status.25 Of note, housing type has been shown to be a proxy for SES in other studies in Singapore.26 Data on self-reported monthly income (including money from family members) were collected; however, it was excluded from the current analysis because of the large proportion of missing values from participants who preferred not to report it (>40%). The proportions of missing value for other SES variables were small (<2%); therefore, we deleted the participants with missing values when analysing the association between respective SES indicator and T2DM risk.
Lifestyle factors
Cigarette smoking was determined using questions adapted from the WHO Tobacco Questions for Surveys.27 Physical activity was evaluated using the International Physical Activity Questionnaire 9-item short form. High levels of physical activity was defined as >150 min of moderate exercise weekly or >75 min of vigorous activity weekly based on the American Heart Association guidelines.28 We used the frequency eating at hawker center as a variable to measure eating-out habit since hawkers centers are main venues for eating-out in Singapore. Poor dietary quality was defined as eating uncooked vegetables <4 times a month and eating fruits <4 times a week29 (online supplemental figure 1).
Supplemental material
Clinical factors
The participants’ BP was measured using an automated device (OMRON HEM-7130) after they rested for ≥5 min in a sitting position. The right cuff size was selected based on the participant’s mid-arm circumference (small (arm circumference <23 cm), standard (23 to <33 cm) and large (≥33 cm)). Weight, height and waist circumference (WC) were also measured for each participant following the WHO protocol. WC was defined as ‘desirable’ (men <90 cm; women <80 cm), ‘high’ (men 90 to <102 cm; women 80 to <88 cm) and ‘very high’ (men ≥102 cm; women ≥88 cm) according to the WHO definition.30 Central obesity was defined as WC ≥102 cm in men and WC ≥88 cm in women.31 Body mass index (BMI) was calculated as  , and categorized using Asian-specific thresholds of ‘underweight and normal’ (BMI<23 kg/m2), ‘overweight’ (23–<27.5 kg/m2) and ‘obese’ (≥27.5 kg/m2) according to the WHO definition.32 Waist-to-height ratio (WHtR) was calculated as
, and categorized using Asian-specific thresholds of ‘underweight and normal’ (BMI<23 kg/m2), ‘overweight’ (23–<27.5 kg/m2) and ‘obese’ (≥27.5 kg/m2) according to the WHO definition.32 Waist-to-height ratio (WHtR) was calculated as  . The history of CVD and stroke were obtained from the baseline interview. Lastly, the lipid profile consisting of serum total cholesterol (TC), high-density lipoprotein cholesterol (HDL-c), low-density lipoprotein cholesterol (LDL-c) and triglycerides was measured for each participant.
. The history of CVD and stroke were obtained from the baseline interview. Lastly, the lipid profile consisting of serum total cholesterol (TC), high-density lipoprotein cholesterol (HDL-c), low-density lipoprotein cholesterol (LDL-c) and triglycerides was measured for each participant.
Statistical analysis
The proportion of T2DM among participants was presented as count (percentage) in the overall population. Demographic, SES, lifestyle and clinical characteristics between the participants with and without T2DM were summarised using count and percentages for categorical variables and mean and SD for continuous variables. These characteristics were compared using Fisher’s exact test and Student’s t-test for categorical and continuous variables, respectively.
Univariate and multivariable logistic regression analyses were performed to examine the independent association between T2DM and SES. The OR, 95% CI and p value were calculated. Additionally, the type 3 p value was computed for variables with more than two categories (ethnicity, housing type, BMI and WC) to determine if all the categories had the same effect on T2DM risk as the reference category. Several models were developed to adjust for potential confounding factors, which were chosen based on clinical and statistical significance. Model 1 included age, gender, ethnicity and SES variables. In addition to model 1, model 2 and 3 adjusted for lifestyle factors, which included smoking, dietary habits, dietary quality and physical activities, and central obesity (WC), respectively. We excluded BMI and WHtR in model 3 due to the collinearity with WC and included WC as previous studies reported it to be the best predictor of metabolic syndrome.33 Model 4 was the full model adjusting for other clinical factors (history of CVD, history of stroke, HDL-c, LDL-c and triglycerides) in addition to model 3. We excluded TC level due to the collinearity with HDL-c, LDL-c and triglycerides.
Moreover, an unweighted composite SES score was constructed as an exploratory analysis. Each SES proxy was converted into an ordinal variable to create the composite SES score following the method of previous studies.34 The ordinal variables of each SES proxy (coded as 0 and 1 for low and high SES variables, respectively) were summed to create a 5-level score with higher values corresponding to higher SES. The 5-level SES composite score was further categorized into low SES (0–1), medium SES (2) and high SES (3–4).34–36 The association between the composite SES score and T2DM was examined in the above-mentioned univariate and multivariable logistic regression models. All statistical analyses were done using IBM SPSS V.25 (Chicago, Illinois, USA), where two-sided p value ≤0.0125 was considered to be statistically significant.
Furthermore, we determined the sample size required to obtain a power of 80% for our study using PS: Power and Sample Size Calculation V.3.1.6 (Vanderbilt University Medical Center, Tennessee, USA). Prior data37 indicate that the probability of low SES (education level, job status, residential location and household income status) in controls is 0.3. If the true OR for T2DM in those with low SES relative to those with high SES is 1.70, we need at least 269 patients with T2DM and 538 control patients to be able to reject the null hypothesis that OR=1 with power 0.8. In the current study, we had 284 patients with T2DM and 631 patients without T2DM, thus ensuring sufficient sample size and power for the statistical analysis. We applied the Bonferroni correction and used p value ≤0.0125 as the selection criteria to account for the four SES indicators we used to test the primary hypothesis.
Results
Baseline characteristics
The demographic, socioeconomic, lifestyle and clinical characteristics of the study population are summarized in table 1. Among 915 patients with uncontrolled hypertension, about half were above 65 years (n=448; 49.0%) and half were women (n=448; 49.0%). A total of 74.2% were Chinese, 13.1% were Malays and 9.2% were Indians. This ethnic distribution was similar to that of the general population in Singapore (74.3% Chinese, 13.4% Malays and 9.0% Indians20). Moreover, 27.5% were of lower education (primary school and below), 51.3% were unemployed, 15.3% resided in rental housing and 85.3% resided in public housing (table 1).
Demographic, socioeconomic status (SES) of participants with hypertension visiting polyclinics in Singapore with and without type 2 diabetes mellitus (T2DM)
Proportion of T2DM
A total of 284 patients (31.0%) had T2DM (table 1). The proportion of T2DM (%) was highest in Indians (56.0%; 95% CI 45.3% to 66.1%) followed by Malays (40.0%; 95% CI 31.7% to 48.9%) and Chinese (26.8%; 95% CI 23.6% to 30.3%). In terms of SES, the proportion of T2DM (%) was higher in patients with lower education (primary school and below: 35.9%; 95% CI 30.2% to 42.0%), currently unemployed (31.1%; 95% CI 27.1% to 35.5%) and living in public housing (33.2%; 95% CI 27.7% to 39.2% (one to three rooms) or 33.0%; 95% CI 29.1% to 37.2% (four to five rooms)) compared with those with higher education (secondary and above: 29.2%; 95% CI 25.8% to 32.8%), currently employed (30.9%; 95% CI 26.8% to 35.4%) and living in private housing (19.4%; 95% CI 13.6% to 26.9%). The proportion of T2DM by lifestyle and clinical factors is shown in online supplemental table 1.
Supplemental material
Factors associated with T2DM: SES and ethnicity
Factors associated with T2DM (p≤0.05) are shown in online supplemental table 2. Factors associated with T2DM after accounting for multiple testing (p≤0.0125) are shown in table 2. In the univariate analysis, ethnic variation was significantly associated with T2DM (type 3 p<0.001). Malays (OR 1.82; 95% CI 1.21 to 2.72, p=0.004) and Indians (OR 3.46; 95% CI 2.18 to 5.51, p<0.001), had significantly higher T2DM odds compared with the Chinese. Among the SES variables, housing type had an association with T2DM (type 3 p=0.008) while other less direct SES proxies such as education levels, current employment status and living in rental housing did not. Higher T2DM odds was observed among those living in one to three rooms (OR 2.06; 95% CI 1.25 to 3.40, p=0.005) and four to five rooms public housing (OR 2.04; 95% CI 1.28 to 3.26, p=0.003) compared with those living in private housing.
Associations between participants’ characteristics and risk of having type 2 diabetes mellitus (T2DM) among patients with uncontrolled hypertension
In multivariate model 1 including demographic and SES factors, T2DM was independently associated with ethnicity (type 3 p<0.001) and housing type (type 3 p=0.030). For ethnic variation, both Indians (OR 3.65; 95% CI 2.25 to 5.91, p<0.001) and Malays (OR 1.59; 95% CI 1.04 to 2.44, p=0.031) had higher T2DM odds compared with Chinese. For housing type, higher T2DM odds was associated with residing in one to three rooms (OR 2.00; 95% CI 1.16 to 3.43, p=0.012) and four to five rooms public housing (OR 1.86; 95% CI 1.13 to 3.04, p=0.013) versus private housing. However, the association of higher T2DM odds with residing in four to five rooms public housing (p=0.013) and Malays (p=0.031) did not meet the level of significance criteria for multiple testing (table 2 and online supplemental table 2).
Adjustment of lifestyle factors in multivariate model 2 (table 2 and online supplemental table 2) did not attenuate the association of T2DM with housing type (type 3 p=0.044) and ethnicity (type 3 p<0.001). However, only the association between Indians (OR 3.50; 95% CI 2.14 to 5.74, p<0.001) and higher T2DM odds met the level of significance for multiple testing.
In the fully adjusted model (model 4) comprising sociodemographic factors, lifestyle factors, central obesity and other clinical factors, the association between Indians (OR 2.53; 95% CI 1.47 to 4.36, p=0.001) and higher T2DM odds was observed (table 2). Furthermore, housing type was not associated with T2DM.
Exploratory analysis using composite SES score
The association between SES and T2DM using the composite SES score is shown in online supplemental table 3. In multivariate model 1 comprising sociodemographic factors, the association between composite SES score and T2DM was marginally significant (type 3 p=0.061). This association was attenuated after further adjustment of lifestyle factors, central obesity and other clinical factors.
Discussion
Statement of principal findings
Among 915 patients with uncontrolled hypertension seeking care at the polyclinics in Singapore, we found a significant association of T2DM with ethnic variation (Indians vs Chinese) and housing type (public housing vs private housing) independent of other sociodemographic factors. Of note, the association of T2DM with Indians versus Chinese remained significant in the fully adjusted model that accounted for clinical comorbidities. Our results are of high relevance from a public health perspective in terms of identification and risk stratification of patients at high risk of T2DM. Our findings underscore the importance of designing personalised and ethnicity-centric interventions to prevent and manage T2DM in patients with uncontrolled hypertension belonging to Indian ethnicity and residence in public housing in Singapore.
In relation to other studies
The significant association between higher T2DM odds and ethnic variation (Indians vs Chinese) in Singapore, independent of demographic and lifestyle factors, corroborated with studies from the UK and the USA.13 38 39 The observed association may be explained by a complex interplay of biological, clinical, behavioral and healthcare system factors.13 Evidence suggests that Indians may be more predisposed to T2DM than Chinese.39 For example, majority of Indians were shown to have lower insulin sensitivity40 41 and higher insulin resistance38 compared with Chinese, while a minority of Indians (approximately 20%) were shown to have lower insulin secretory capacity.42 These ethnic differences may be further exaggerated by clinical and lifestyle factors, such as obesity, dietary imbalances and lower physical activity.43 According to the National Nutrition Survey 2010 conducted in Singapore, Indians consumed more carbohydrates, more saturated fats and lesser proteins than Chinese,44 which may increase T2DM risk by adversely affecting glucose metabolism and insulin resistance.43 Hence, differences in diet may partially explain the association between ethnic variation and higher T2DM odds in Singapore. Moreover, ethnic inequalities in healthcare provision due to differences in SES, health literacy, linguistics and culture13 may also contribute to higher T2DM risk among the Indian ethnicity. Therefore, our results highlight the importance of developing personalized and ethnicity-centric interventions targeting dietary and lifestyle habits of the Indian ethnicity for the prevention and management of T2DM such as tailoring the health education messages according to the health literacy, dietary patterns and cultural acceptability of targeted populations in Singapore.
The positive association between public housing and higher T2DM risk observed after adjusting for sociodemographic factors is consistent with most studies conducted in high-income countries. The latter studies used various SES surrogates including lower education,9 34 lower income7 9 45 and deprivation45 that demonstrated an association between lower SES and higher T2DM risk. Given our findings, residing in smaller public housing is likely to be a useful surrogate for lower SES in Singapore. Collectively, our findings implied that while the underlying social determinants of T2DM in patients with hypertension need to be addressed, more healthcare resources for better access to healthcare could be provided in the areas with more public housing compared with private housing. For example, health education, screening and counselling could be conducted at community levels to increase health awareness among these areas. In addition, since moderate exercise has shown to reduce the risk of T2DM,46 modifications to environment and infrastructure around the areas with more public housing (eg, having bicycle paths, running tracks and sports complexes47) to promote physical activity may also facilitate the prevention of T2DM.
Furthermore, we found that the independent association between public housing and T2DM was attenuated by adjusting for clinical factors and comorbidities (eg, history of CVD, history of stroke and lipid profile). This was in contrast with previous cross-sectional studies that found an independent association between SES and T2DM after adjusting for clinical factors like BMI,7 8 11 48 WC,8 WHtR8 and history of CVD.48 However, unlike our study, the self-reported clinical parameters were not verified in the above-mentioned studies. Thus, the heterogeneity may be partly due to the better caption on clinical risk factors in our study. Furthermore, those with lower SES are more likely to have poorer health-related behaviours and access to healthcare services which may result in poorer clinical factors such as diabetes-related comorbidities and metabolic risk factors compared with those with higher SES.49 These may have increased the risk of CVD among those with low SES. These results highlighted the need for further studies to investigate the independent association between T2DM and SES by accounting for the presence of diabetes-related comorbidities and metabolic risk factors.
Implications of the study
This study has important implications on clinical practice and public health. Firstly, the suggested association of higher T2DM odds with Indian ethnicity and residing in public housing in Singapore implies that identifying and risk stratifying patients with uncontrolled hypertension at T2DM risk using ethnicity and housing type may be beneficial for targeted public health services to reduce inequities in T2DM in Singapore. As observed in other high-income countries, the presence and persistence of ethnic differences in cardiometabolic risk factors and comorbidities can lead to disparities in cardiovascular mortality rates.50 Secondly, the results suggested that personalised and ethnicity-centric interventions to prevent and manage T2DM in patients of Indian ethnicities and those residing in public housing with uncontrolled hypertension may be beneficial in Singapore.
Strengths and limitations of the study
To the best of our knowledge, this is the first study examining the association between SES, ethnicity and T2DM adjusting for lifestyle and clinical factors among patients with uncontrolled hypertension in Singapore. As the patients were recruited from eight different polyclinics throughout Singapore and majority of individuals (60%) with hypertension or diabetes are reported to seek care at the government polyclinics in Singapore,19 22 this study has high external validity. A major strength of this study is that the self-reported T2DM status, uncontrolled hypertension and other clinical parameters were verified objectively using standardised laboratory tests and medical records. In addition, since the age-specific for hypertension rises markedly from age 40 years onwards in Singapore, we included patients aged 40 years or older in our study as prevention and control of hypertension is of critical importance among them. Moreover, the Ministry of Health Clinical Practice Guideline suggests starting screening of T2DM at 40 years of age in Singapore.51 Therefore, the inclusion of patients 40 years or older in the current study could also enable the capture of majority of T2DM cases in this multiethnic population.
However, there are several limitations to be considered. This study was a cross-sectional design so the temporal relationship and causality between the variables cannot be established. Hence, the internal validity of this study is not high. However, our results offered valuable information for identifying and risk stratifying those with high T2DM risk and designing personalised and ethnicity-centric interventions, and the temporal relationships will be further validated after completing the 2-year follow-up interviews. In addition, although we adjusted for major T2DM risk factors including socioeconomic, environmental, behavioural and clinical factors, residual confounding may exist, and we did not collect physiological and genetic factors. Moreover, we did not collect information on the type of diabetes and could include patients with type 1 diabetes. However, the onset of type 1 diabetes in adults aged 40 years and above is rare (<2%);52 therefore, we assumed that diabetes cases included in the present study could represent T2DM. Lastly, as the association of T2DM with Malays and public housing did not meet the statistical significance criteria for multiple comparisons using the highly conservative Bonferroni correction method, the results are only suggestive but not conclusive. Thus, future studies using other less conservative methods (eg, false discovery rate) or larger sample sizes need to be conducted to determine if these associations are conclusive.
Conclusion
In conclusion, our study suggested that higher T2DM odds are associated with residing in public housing versus private housing and Indian patients with uncontrolled hypertension in Singapore. Our findings highlight the importance of developing personalised, ethnicity-centric interventions to prevent and manage T2DM in high-risk patients, especially of public housing residence and ethnic variation. Further studies are necessary to determine if the association of T2DM with Malays and SES observed in our study are conclusive.
Data availability statement
Data are available on reasonable request from THJ subject to approval by SingHypertension IRB.
Ethics statements
Ethics approval
The study protocol was approved by SingHealth Centralised Institutional Review Board (CIRB Ref: 2015/3115).
Acknowledgments
The authors would like to thank Ms Rehana Sultana, Associate Professor Deidre Anne De Silva and Assistant Professor Sung Sharon Cohan from Duke-NUS Medical School for providing valuable feedbacks. The authors would also like to thank Ms Patricia T. Kin and Ms Caris Yang Thong Tan from the Department of Research in SingHealth Polyclinics, Dr Rupesh M. Shirore and Dr Chandrika Ramakrishnan from Duke-NUS Medical School for the study coordination and data management. In addition, the authors would like to thank all site principal investigators (Dr Paul Goh, Dr Peter Moey, Dr Joanne Hui Min Quah, Dr Siew Wai Hwang, Dr Juliana Bahadin, Dr Anandan Gerard Thiagarajah, Dr Jason Chan, Dr Gary Kang and Dr Agnes Koong), participants and all administrative and support staff involved with the study at recruiting polyclinics.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors THJ conceived the study idea, designed the study and directed the overall conduct of the study; NCT contributed to protocol implementation and data acquisition; VD/OP and YW conducted the analysis. VD/OP wrote the first and final drafts. All authors provided critical comments, and approved the final version.
Funding SingHypertension was supported by research funds from Clinician Scientist Award to THJ from National Medical Research Council (NMRC/CSA-SI/0005/2015).
Disclaimer The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.