Article Text

Abstract
Introduction There are conflicting results on the association between type 2 diabetes and chronic low back pain (CLBP). Therefore, the goal was to investigate the relationship between type 2 diabetes and CLBP in individuals followed in general practices in Germany.
Research design and methods Adults diagnosed for the first time with type 2 diabetes in 809 general practices in Germany between 2005 and 2018 (index date) were included. Adults without type 2 diabetes were matched (1:1) to those with type 2 diabetes by sex, age, index year, and the annual number of medical consultations (index date: a randomly selected visit date). The association between type 2 diabetes and the 10-year incidence of CLBP was analyzed in conditional Cox regression models adjusted for a wide range of comorbidities, including hypertension, lipid metabolism disorders, and obesity.
Results There were 139 002 individuals included in this study (women: 58.0%; mean (SD) age 62.5 (13.4) years). There was a positive association between type 2 diabetes and the incidence of CLBP in the overall sample (HR=1.23, 95% CI: 1.13 to 1.35). Sex-stratified analyses showed a higher risk of CLBP in women (HR=1.68, 95% CI: 1.43 to 1.90) and a lower risk in men with than in their counterparts without type 2 diabetes (HR=0.83, 95% CI: 0.71 to 0.97).
Conclusions Newly diagnosed type 2 diabetes was associated with an increased risk of CLBP. There were important sex differences in the type 2 diabetes-CLBP relationship, and more research is warranted to investigate the underlying factors explaining these differences.
- type 2 diabetes
- epidemiology
- cohort studies
- low back pain
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Several studies have investigated the association between type 2 diabetes and chronic low back pain (CLBP), and these studies have yielded inconsistent results.
What are the new findings?
Type 2 diabetes was positively associated with the incidence of CLBP in the overall sample.
Similar findings were obtained in women, and the odds of CLBP was significantly higher in women with than in those without CLBP.
On contrast, men with type 2 diabetes were less likely to be diagnosed with CLBP than their counterparts without type 2 diabetes.
How might these results change the focus of research or clinical practice?
Based on these findings, interventions preventing the occurrence of CLBP in people with type 2 diabetes should be promoted.
Introduction
Chronic low back pain (CLBP) is defined as chronic pain affecting the lower back (lumbar spine) for more than 3 months.1 The prevalence of CLBP is high in the general population and chronic back pain affects almost 60% of older adults.2 CLBP is a risk factor for several unhealthy behaviors (eg, consumption of illicit drugs3 and reduced physical activity4), psychiatric conditions (eg, major depression5 and anxiety6), higher disability,7 and increased mortality.8 In addition, CLBP-related medical and non-medical direct costs are substantial,9 and the condition is also a leading cause of workplace absenteeism.10 Thus, public health interventions focusing on the prevention of CLBP should be prioritized in the coming years, and the implementation of these interventions relies on a better understanding of protective factors against and risk factors for CLBP.
CLBP is a complex disorder that is associated with a wide range of sociodemographic and psychological factors such as low educational attainment,11 workload,12 and psychological comorbidities.13 In terms of chronic physical conditions, an increasing body of research has investigated the relationship between diabetes and back pain, but there are some discrepancies in the results of these studies.14–21 For example, a Spanish case–control study including 4190 individuals with and without diabetes revealed that CLBP and chronic neck pain were more common in people with diabetes.20 By contrast, another cross-sectional study, using data pertaining to 1605 twins in the same country, found that a history of diabetes was negatively associated with the odds of seeking medical care for low back pain.21 Theoretically, diabetes could lead to an increase in the risk of CLBP due to lower muscle mass22 23 and poor mental health (eg, depression13 24), while diabetes and CLBP share common risk factors such as obesity25 26 and low-grade systemic inflammation.27 28 Although previous studies have advanced the field, the majority of these studies were surveys, and the use of self-reported measures may have impacted the validity of their findings. In view of this, further research based on clinical data is warranted to clarify the relationship between diabetes and CLBP.
Therefore, the goal of this retrospective cohort study was to investigate the association between type 2 diabetes and the incidence of CLBP in adults followed up for up to 10 years in general practices in Germany. Given that there are sex-related differences in the epidemiology of diabetes,29 diabetes-related complications,30 and CLBP,31 it was hypothesized that the relationship between type 2 diabetes and the incidence of CLBP would differ between men and women.
Methods
Database
Data from the Disease Analyzer database (IQVIA) were used for this study. The Disease Analyzer database contains sociodemographic, clinical, and pharmaceutical data obtained directly in an anonymous format from general and specialized practices.32 Clinical data were coded using the German version of the International Classification of Diseases, 10th revision (ICD-10), while pharmaceutical data were obtained using the European Pharmaceutical Marketing Research Association (EphMRA) Anatomical Therapeutic Chemical (ATC) system. The quality of the data is assessed regularly on the basis of a wide range of criteria such as completeness of documentation and linkage between clinical and pharmaceutical data. Around 3% of all outpatient practices in Germany are included in the database. Summary statistics from the entire population of German outpatient practices (ie, age of physician, specialty, community size category, and German federal state) are used to select the practices included in the Disease Analyzer database. Finally, this database has been found to be a representative sample of all outpatient practices in Germany.32
Study population
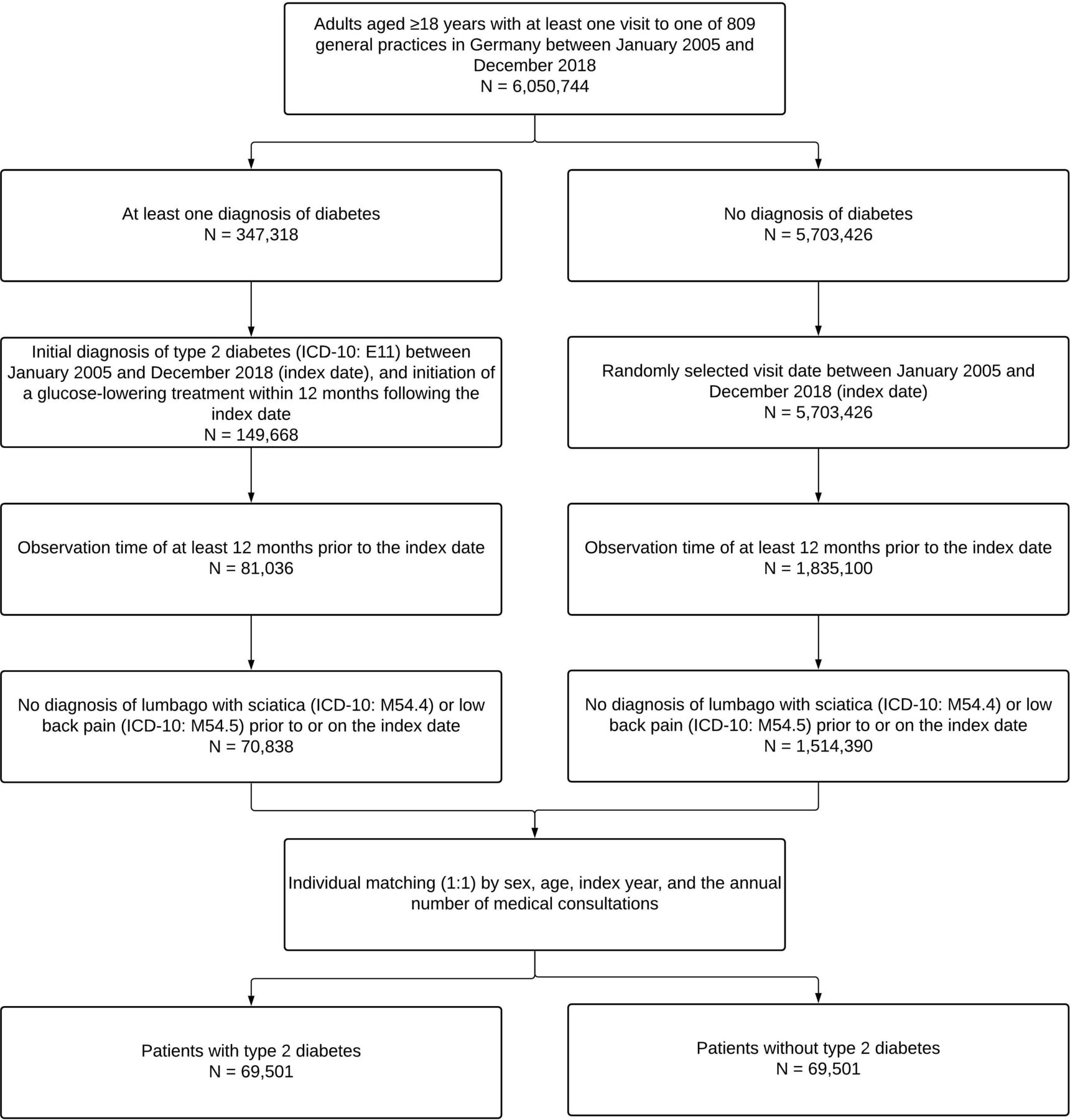
The present study included adults aged ≥18 years first diagnosed with type 2 diabetes (ICD-10: E11) in 1 of 809 general practices in Germany between January 2005 and December 2018 (index date). In order to be included in this study, people with type 2 diabetes had to receive a glucose-lowering treatment within 12 months following the index date, be observed for at least 12 months prior to the index date, and have no diagnosis of lumbago with sciatica (ICD-10: M54.4) or low back pain (ICD-10: M54.5) prior to or on the index date. People without type 2 diabetes were matched (1:1) to their counterparts with type 2 diabetes by sex, age, index year, and the annual number of medical consultations (ie, the number of medical consultations during the follow-up period divided by the number of years of follow-up). In individuals without type 2 diabetes, the index date corresponded to a randomly selected visit date. The flow chart of the study participants is displayed in figure 1.

Selection of study patient.
Study outcome and variables
The outcome of this retrospective cohort study was the 10-year cumulative incidence of CLBP in individuals with and without type 2 diabetes. CLBP was defined as the presence of low back pain (ie, lumbago with sciatica (ICD-10: M54.4) or low back pain (ICD-10: M54.5)) during at least two different medical consultations no less than 3 months apart. Other study variables included type 2 diabetes (ICD-10: E11), sex, age, index year, the annual number of medical consultations, comorbidities (ie, hypertension (ICD-10: I10), osteoarthritis (ICD-10: M15–M19), lipid metabolism disorders (ICD-10: E78), obesity (ICD-10: E66), spondylopathies (ICD-10: M45–M49), chronic coronary heart disease (ICD-10: I25 excluding I25.2), osteoporosis (ICD-10: M80, M81), peripheral vascular disease (ICD-10: I70.3, I73.9, and E11.5), history of myocardial infarction (ICD-10: I21-I23, and I25.2), and history of stroke or transient ischemic attack (ICD-10: I63, I64, and G45)), and glucose-lowering drugs (ie, metformin (EphMRA ATC: A10J, A10N3, A10K2, and A10P2), sulfonylurea (EphMRA ATC: A10H), dipeptidyl peptidase (DPP)-4 inhibitors (EphMRA ATC: A10N), sodium glucose cotransporter 2 (SGLT2) inhibitors (EphMRA ATC: A10P), glucagon-like peptide 1 receptor agonists (GLP-1RAs) (EphMRA ATC: A10S), other oral drugs (EphMRA ATC: A10K, A10L, and A10M), and insulin (EphMRA ATC: A10C)).
Statistical analyses
Baseline characteristics were compared for subjects with and those without type 2 diabetes using McNemar tests for categorical variables and Wilcoxon signed-rank tests for continuous variables. In addition, differences in the prescription of glucose-lowering drugs between women and men with type 2 diabetes were assessed using χ2 tests. Kaplan-Meier curves and log-rank p values were used to analyze the 10-year cumulative incidence of CLBP in the overall sample, women and men by type 2 diabetes status. Finally, the associations between type 2 diabetes and the incidence of CLBP in the overall sample, women and men were investigated using conditional Cox regression models. These Cox regression models were adjusted for hypertension, osteoarthritis, lipid metabolism disorders, obesity, spondylopathies, chronic coronary heart disease, osteoporosis, peripheral vascular disease, history of myocardial infarction, and history of stroke or transient ischemic attack. As subjects without type 2 diabetes were matched to those with type 2 diabetes by sex, age, index year, and the annual number of medical consultations, these variables were not included in the Cox regression models. The results of the Cox regression analyses are presented as HRs with 95% CIs. P values lower than 0.05 were considered statistically significant. All analyses were performed using SAS V.9.4.
Results
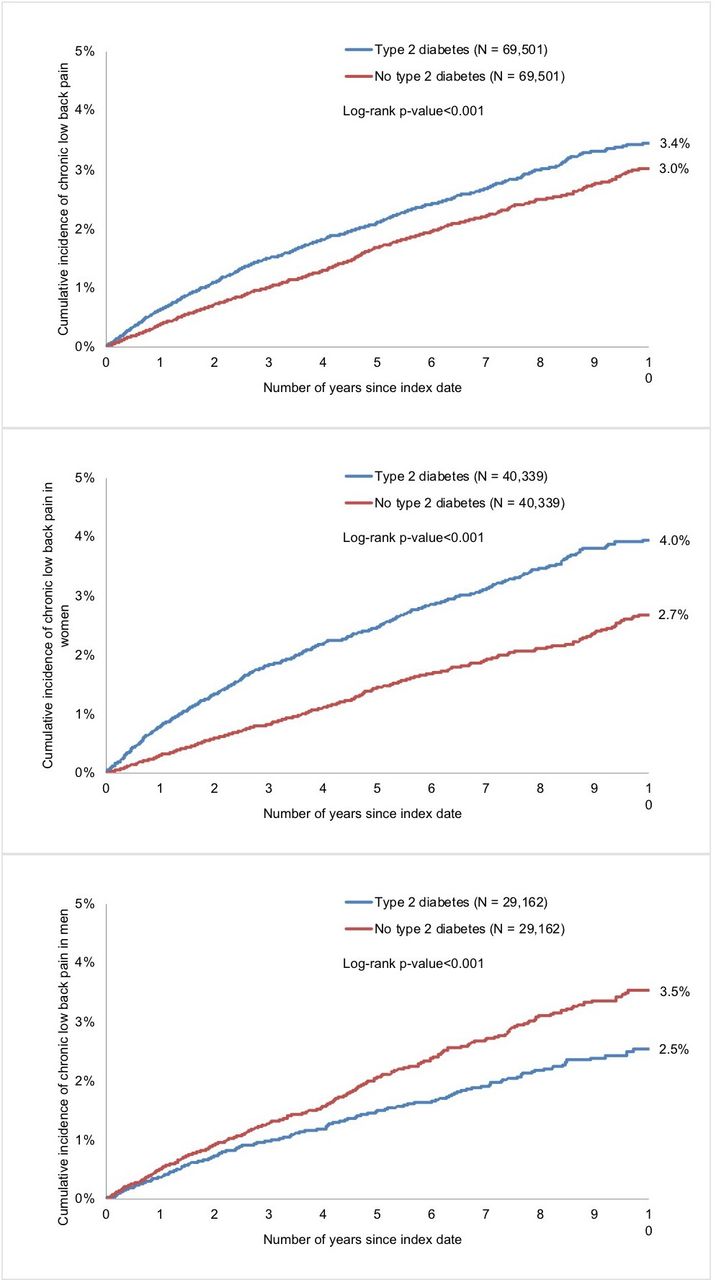
Overall, 69 501 people with type 2 diabetes and 69 501 people without type 2 diabetes were included in this study. The baseline characteristics of the study sample are displayed in table 1. In total, 58.0% of the subjects included were women, and the mean (SD) age was 62.5 (13.4) years. The mean follow-up period was 4.4 (3.5) years in participants with type 2 diabetes and 5.0 (3.5) years in those without type 2 diabetes. The mean (SD) HbA1c was 7.3% (1.6%) in the type 2 diabetes group. All glucose-lowering drugs except GLP-1RAs were prescribed less frequently in women than in men with type 2 diabetes, and the three most commonly prescribed families of molecules were metformin (63.6% in women vs 66.2% in men), insulin (46.9% vs 47.1%), and DPP-4 inhibitors (26.9% vs 29.9%; table 2). Within 10 years of the index date, 3.4% of subjects with and 3.0% of those without type 2 diabetes had received a diagnosis of CLBP (log-rank p value <0.001; figure 2, upper panel). Similar findings were obtained in women (4.0% vs 2.7%, log-rank p value <0.001; figure 2, middle panel). However, the 10-year cumulative incidence of CLBP was significantly lower in men with type 2 diabetes than in their counterparts without type 2 diabetes (2.5% vs 3.5%, log-rank p value <0.001; figure 2, lower panel). Finally, the results of the Cox regression analyses are displayed in table 3. Type 2 diabetes was associated with an increased risk of CLBP in the overall population (HR=1.23, 95% CI: 1.13 to 1.35). We also found that women with type 2 diabetes had a higher risk of CLBP than their counterparts without type 2 diabetes (HR=1.68, 95% CI: 1.43 to 1.90), whereas a lower risk was observed in men generally (HR=0.83, 95% CI: 0.71 to 0.97).
Baseline characteristics of the study sample after 1:1 matching by sex, age, index year, and the annual number of medical consultations
{kind=link}
{kind=link}
10-year cumulative incidence of chronic low back pain by type 2 diabetes status in the overall population (upper panel), women (middle panel) and men (lower panel; Kaplan-Meier curves).
Prescription of glucose-lowering drugs in women and men with type 2 diabetes
Association between type 2 diabetes and the 10-year cumulative incidence of chronic low back pain in the overall sample, women and men (Cox regression models)
Discussion
Main findings
This retrospective cohort study including more than 139 000 patients from general practices in Germany found that overall, the 10-year cumulative incidence of CLBP was higher in individuals with than in those without type 2 diabetes. These findings were corroborated in the Cox regression analyses adjusted for a large number of chronic conditions, as type 2 diabetes was associated with a 1.23-fold increase in the incidence of CLBP. Interestingly, stratified analyses also revealed that the relationship between type 2 diabetes and CLBP was positive in women but negative in men. To the best of our knowledge, this is one of the largest studies to date to have investigated the association between type 2 diabetes and CLBP, and it is also one of the few studies based on clinical and not self-reported data.
Interpretation of findings
In recent years, a significant body of literature has focused on the relationship between diabetes and CLBP, and these studies have reported conflicting results.14–21 For example, a Spanish study including 2096 twins revealed that type 2 diabetes was cross-sectionally associated with a wide range of back conditions such as severe CLBP and severe chronic spinal pain.14 A systematic review and meta-analysis of eight studies also showed a positive association between diabetes and both low back and neck pain.18 By contrast, a longitudinal study using data pertaining to 3045 men living in the USA found no significant association between diabetes and incident chronic back pain.16 The discrepancies in these findings may be due to the fact that back pain was usually self-reported and that the definition of back pain varied between studies. Taking these limitations into consideration, the present retrospective study conducted in Germany adds to the literature by showing that a diagnosis of type 2 diabetes is positively associated with a diagnosis of CLBP later in life.
At least two factors likely play a mediating role with respect to the association between type 2 diabetes and CLBP. First, people with type 2 diabetes are at a particular risk of accelerated decline in muscle mass compared with their counterparts without type 2 diabetes.23 As a matter of fact, insulin resistance favors the inhibition of the mammalian target of rapamycin (mtoR) pathway, which leads to a decrease in protein synthesis and an increase in protein degradation.33 Meanwhile, there is some literature indicating that trunk muscle weakness may favor the occurrence of low back pain.22 Second, type 2 diabetes has deleterious effects on mental health, and previous data have suggested that there is a bidirectional relationship between type 2 diabetes and depression.24 Interestingly, depression and other psychiatric disorders such as anxiety are also key factors in the transition from acute low back pain to CLBP.13 Furthermore, type 2 diabetes and CLBP share common risk factors such as obesity and low-grade systemic inflammation, and regression analyses conducted in this study were therefore adjusted for obesity. In terms of low-grade systemic inflammation, there is a strong body of literature showing that this factor likely plays an important role in the etiology of both type 2 diabetes27 34 and CLBP.28 35 Low-grade systemic inflammation may favor the occurrence of type 2 diabetes via molecular pathways enhancing insulin resistance (eg, activation of Jun kinase and downregulation of peroxisome proliferator-activated receptor (PPAR)-γ expression),27 while proinflammatory molecules may contribute to back pain through the sensitization of peripheral nociceptors and the promotion of hyperalgesia.28
Another interesting finding of this study is the sex-related difference in the association between type 2 diabetes and CLBP. Indeed, the relationship between type 2 diabetes and CLBP was positive in women and negative in men. Before going further, it is important to bear in mind that the negative association observed in male participants may be due to residual confounding factors not included in the regression analyses (eg, physical activity and inflammatory markers). That being said, these differing results may also be the result of differences between men and women in terms of the burden and complications of type 2 diabetes. As a matter of fact, glycemic control is poorer in women than in men with diabetes,36 37 and low-grade systemic inflammation related to type 2 diabetes may therefore be more pronounced in women than in their male counterparts, potentially increasing their risk of developing CLBP. In line with this hypothesis, glucose-lowering drugs were prescribed less frequently in women than in men in this study and as some of these molecules (eg, insulin) have anabolic effects,38 this could at least partially explain these sex-related differences in the relationship between type 2 diabetes and CLBP. Furthermore, given that women with diabetes exhibit more difficulties in activities of daily living and instrumental activities of daily living than men with diabetes,39 they may be more likely to suffer from muscle mass decline and indirectly develop CLBP. Finally, depressive symptoms related to type 2 diabetes are more significant in female than in male adults,40 41 which could also be a contributing factor with regard to the sex-related differences in the results of this study.
Clinical implications and directions for future research
Based on these findings, women with type 2 diabetes may be at a higher risk of developing CLBP than those without type 2 diabetes. Therefore, interventions aiming at the prevention of CLBP in people with type 2 diabetes are urgently needed. Personalized treatment and management are necessary to reduce the burden and the complications of type 2 diabetes. Furthermore, exercise therapy should be favored in people with diabetes to lower their risk of muscle mass loss. Finally, the potential deleterious effects of type 2 diabetes on mental health should be assessed on a regular basis, and patients should be referred to mental health specialists when psychiatric disorders are present. In terms of future research, more clinical data of a longitudinal nature are needed to obtain a better picture of the association between type 2 diabetes and CLBP. In addition, further research should confirm or refute the sex-related differences in the relationship between type 2 diabetes and CLBP observed in the present study.
Strengths and limitations
Major strengths of this study include the large sample size, the duration of follow-up for patients, and the use of clinical data. However, there are also several limitations that should be acknowledged at this point. First, no data was available on the severity of diabetes, although this severity may have impacted the relationship between type 2 diabetes and CLBP. Second, no information was available on physical activity and given that lack of physical activity is associated with both type 2 diabetes42 and CLBP,43 this may have biased the study results. Third, CLBP may have been diagnosed by health professionals other than general practitioners (eg, rheumatologists) and as this study included general practices only, it is therefore possible that the incidence of CLBP has been underestimated.
Conclusion
Overall, there was a positive and significant association between type 2 diabetes and the 10-year incidence of CLBP. Interestingly, there were significant sex-related differences in the association between type 2 diabetes and CLBP, with this relationship being positive in women and negative in men. Further studies of a longitudinal nature are needed to identify mediators involved in this association and to confirm these sex-related differences.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Acknowledgments
Professional English language editing services were provided by Claudia Jones, MA, Radford, Virginia, USA.
References
Footnotes
Contributors LJ contributed to the design of the study, managed the literature searches, wrote the first draft of the manuscript, and corrected the manuscript. WR, AK, and JMH contributed to the design of the study and corrected the manuscript. KK contributed to the design of the study, performed the statistical analyses, and corrected the manuscript. All authors contributed to and have approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.