
Abstract
Purpose
The ClinGen Variant Curation Expert Panels (VCEPs) provide disease-specific rules for accurate variant interpretation. Using the hearing loss-specific American College of Medical Genetics and Genomics/Association for Molecular Pathology (ACMG/AMP) guidelines, the Hearing Loss VCEP (HL VCEP) illustrates the utility of expert specifications in variant interpretation.
Methods
A total of 157 variants across nine HL genes, previously submitted to ClinVar, were curated by the HL VCEP. The curation process involved collecting published and unpublished data for each variant by biocurators, followed by bimonthly meetings of an expert curation subgroup that reviewed all evidence and applied the HL-specific ACMG/AMP guidelines to reach a final classification.
Results
Before expert curation, 75% (117/157) of variants had single or multiple variants of uncertain significance (VUS) submissions (17/157) or had conflicting interpretations in ClinVar (100/157). After applying the HL-specific ACMG/AMP guidelines, 24% (4/17) of VUS and 69% (69/100) of discordant variants were resolved into benign (B), likely benign (LB), likely pathogenic (LP), or pathogenic (P). Overall, 70% (109/157) variants had unambiguous classifications (B, LB, LP, P). We quantify the contribution of the HL-specified ACMG/AMP codes to variant classification.
Conclusion
Expert specification and application of the HL-specific ACMG/AMP guidelines effectively resolved discordant interpretations in ClinVar. This study highlights the utility of ClinGen VCEPs in supporting more consistent clinical variant interpretation.
Similar content being viewed by others


INTRODUCTION
Hearing loss (HL) is the most common congenital sensory condition, with approximately 50% of affected individuals having an identifiable genetic etiology [1]. HL is a heterogeneous condition with more than 100 genes underlying nonsyndromic HL, and over 400 genes implicated in syndromic forms of deafness [2, 3]. A clinical genetics evaluation is recommended as part of a standard of care diagnostic work-up, and results from genetic testing can often inform clinical management, especially if a genetic syndrome is identified before the onset of additional clinical manifestations [1, 4]. As an expert panel of the Clinical Genome Resource (ClinGen), a National Institute of Health (NIH)–funded resource focused on defining the clinical validity of gene and variant contributions to disease, the Hearing Loss Clinical Domain Working Group (HL-CDWG) (https://www.clinicalgenome.org/working-groups/clinical-domain/hearing-loss/), has worked to evaluate gene–disease relationships and standardize variant interpretation in hereditary HL [5,6,7].
Interpretation of variants’ clinical significance is a rigorous process that involves collating and analyzing available literature and evidence, followed by a formal classification based on this evidence. The ClinVar database (https://www.ncbi.nlm.nih.gov/clinvar/) archives and aggregates variant interpretations from various submitters and indicates whether the submitted interpretations are concordant or discordant. Data sharing through ClinVar provides an invaluable opportunity to identify classification differences and to collaborate with submitters to resolve these discrepancies. A pilot study conducted by four clinical laboratories showed that 87.2% (211/242) of discordant variants were resolved when the variant was reassessed with current criteria and/or through internal data sharing [8]. The resolution of conflicting interpretations helps provide crucial diagnostic information to clinicians and patients.
Here we demonstrate the successful implementation of the HL-specific ACMG/AMP guidelines [5] by the ClinGen HL Variant Curation Expert Panel (HL VCEP) to resolve discrepancies in variant interpretations.
MATERIALS AND METHODS
HL-CDWG organizational structure
The HL-CDWG has worked to create a standardized, thorough set of genes and variants that are associated with syndromic and nonsyndromic HL [5, 9]. The members include otolaryngologists, clinical geneticists, molecular geneticists, ClinGen biocurators, clinical researchers, and genetic counselors from 11 different countries including China, France, Israel, Japan, Netherlands, Singapore, South Korea, Spain, Tunisia, the United Arab Emirates, and the United States, representing 26 institutions. In order to accomplish this goal, the HL-CDWG formed two other groups defined by ClinGen as a Gene Curation Expert Panel (GCEP) and a Variant Curation Expert Panel (VCEP).
HL VCEP rule specification and curation process
A smaller task team of the HL VCEP worked to provide expert guidance for standardized variant interpretation and adapted the ACMG/AMP guidelines for the interpretation of sequence variants in nine HL genes, specifically USH2A, SLC26A4, GJB2, MYO7A, CDH23, TECTA, COCH, KCNQ4, and MYO6 [5]. Those genes represent the major causes of hereditary hearing loss encompassing dominant and recessive inheritance models, different disease mechanisms, penetrance, and expressivities.
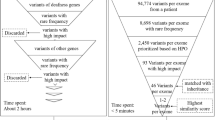
The HL VCEP group then continued to curate variants in these nine genes according to the new HL-specific standards with an emphasis on those that have conflicting interpretations in ClinVar (Fig. 1). The HL VCEP utilizes monthly meetings in addition to email correspondence to present, review, and reach consensus on the classification of these variants. Each variant was assigned to a single trained ClinGen biocurator who utilized various literature search engines and databases including PubMed, the Deafness Variation Database (DVD) [10], Human Gene Mutation Database (HGMD) [11], Google Scholar, Leiden Open Variation Database (LOVD) [12], and LitVar [13] to find publications associated with these variants. HL VCEP members also contributed case observations and phenotypic information from their laboratories or clinics. Additionally, ClinVar submitters were contacted via email to provide internal genotype and phenotype data for their submissions so that biocurators could aggregate all the relevant data. Curators utilized ClinGen’s Variant Curation Interface (https://curation.clinicalgenome.org/) to assess and document the applicable rules for each variant. Provisional classifications made by the curators were comprehensively presented to the chairs and members of the HL VCEP during the monthly meetings. Members provided verbal feedback during these calls to help modify and approve the various ACMG/AMP codes as necessary. Monthly calls between the biocurators and the chairs of the group were utilized to finalize the classification of variants and to discuss the language of the classification summary text. The average curation time for an individual variant was 40 minutes, with a range from 10 minutes to 2 hours. The expert classifications of these variants were submitted to ClinVar on a quarterly basis (Fig. 1).

Refer to “Materials and Methods” for a detailed description of the curation process. ACMG/AMP American College of Medical Genetics and Genomics/Association for Molecular Pathology, HL hearing loss, VCEP Variant Curation Expert Panel.
RESULTS
Curated variants
Since the specification and promulgation of the ACMG/AMP variant rules by the HL VCEP [5, 9], 157 variants—including the 51 variants used to pilot the newly specified rules—across nine HL genes (Supplementary Figure 1, Supplementary Table 1) underwent an expert review and classification process as shown in Fig. 1. The majority of variants were missense (n = 124), while the remaining were in essential (+/−1,2) splice sites (n = 4), frameshift (n = 7), synonymous (n = 5), nonessential splice regions (n = 10), nonsense (n = 3), inframe deletion (n = 1), exon deletion (n = 1), start loss (n = 1), or in untranslated region (UTR) (n = 1) variants (Supplementary Table 1). As of 8 January 2021, 937 classifications have been submitted from 70 submitters for these 157 variants. Submitters were mainly affiliated with academic or commercial diagnostic laboratories, while a few were from academic research institutions.
Prior to expert curation, 100 variants had conflicting interpretations, 17 variants had VUS classifications, and 40 variants had no conflicts in ClinVar. Of the 100 variants with conflicting interpretations, 76 variants had medically significant conflicting classifications (P/LP vs. VUS/LB/B as defined by Harrison et al. [8]), and 24 variants had VUS versus LB/B conflicts. Only three variants had conflicting classifications of P/LP versus LB/B. For the 40 variants with no conflicting classifications, 33 variants were supported by multiple submissions, 5 variants had only one submission, and 2 variants had no previous submissions. Of these 40 variants, some were chosen to pilot the initial specifications of the rules while others were considered clinically significant variants or common pathogenic variants in a specific subpopulation [5] (Supplementary Figure 1).
Expert curation outcomes
After applying the HL-specific ACMG/AMP variant rules, 73 of the 117 variants (63%) with either conflicting or VUS classifications were classified as B, LB, LP, or P, while 44 variants (37%) were classified as VUS (Fig. 2). A significant proportion of the resolved classifications belonged to the VUS vs LB/B conflicting category where 20 of those 24 variants (83%) were classified as B or LB and the remaining as VUS. On the other hand, 38 of the 63 variants (60.3%) with VUS versus LP/P conflicting interpretations were classified as P or LP, one was classified as LB, and the remaining as VUS. Four of 17 variants (24%) with single or multiple VUS submissions in ClinVar were classified as B (n = 1) or LB (n = 2), or LP (n = 1) (Fig. 2a). Of the 40 non-VUS variants without conflicts, 13 (32.5%) were classified as B or LB, while 23 (57.5%) were classified as P or LP (Fig. 2a). Overall, 109 of the 157 variants (69%) were assigned non-VUS classifications (B, LB, LP, P) after applying the HL-specific ACMG/AMP modified variant interpretation guidelines by the expert group (Fig. 2b).

(a) Resolution of variants with different conflict types into pathogenic (P), likely pathogenic (LP), variant of uncertain significance (VUS), likely benign (LB), or benign (B) by the ClinGen HL-EP. y-axis represents the number of variants; x-axis represents the conflict type in ClinVar. “Single” and “multi” refer to single and multiple submitters in ClinVar, respectively. (b) Final classifications of all variants curated by the Hearing Loss VCEP (N = 157).
Criteria contribution to the final classification
In classifying the 157 variants, the most commonly applied criteria codes were PM2 (absence or rare occurrence in population databases) at two different strength levels (PM2_Supporting and PM2) and PM3 (allelic observations in recessive cases) at four different strength levels (PM3_Supporting, PM3, PM3_Strong, PM3_Very Strong), as specified by the HL VCEP [5]. Both the PM2 and PM3 codes were used 80 times and were applied to 77% (49/64) and 88% (56/64) of the variants classified as P/LP, respectively (Supplementary Figure 2). The in silico prediction code PP3, specified using REVEL [5, 14], was applied 64 times as the second most commonly used code, and was applied to 59% (38/64) of P/LP variants. The BA1, BS1, and BS1_Supporting allele frequency codes, as specified by the expert panel, were applied 59 times and to 91% (41/45) of the B/LB classifications. The phenotype code PP4 was used 47 times and was applied to 58% (37/64) of P/LP variants. The specified segregation code PP1 at three different strength levels (PP1, PP1_Moderate, PP1_Strong) was used 31 times and was applied to 41% (26/64) of P/LP variants. Finally, the specified functional codes (BS3_P, PS3_P, PS3_M, and PS3) [5] were used 31 times, 48% (15/31) of which were toward P/LP classifications. Several other codes were utilized as specified by the HL VCEP and as shown in Supplementary Figure 2.
DISCUSSION
Of the 28 ACMG/AMP criteria, 25 were specifically tailored to hereditary HL [5, 9]. The HL VCEP included an international group of scientists, clinicians, geneticists, genetic counselors, and laboratory directors. This panel leveraged the collective members’ expertise and knowledge, along with internal unpublished data sets accessible to the group, to characterize several HL attributes such as prevalence, penetrance, genetic and allelic heterogeneity, and phenotypic presentations (onset, severity, frequencies affected, symmetry and audiometric profile) specific to several HL-associated genes. This information was then used to define the criteria for variant classification in hearing loss [5].
Our panel implemented these HL-specific guidelines to classify 157 variants. One hundred and nine variants (69%) were classified into non-VUS categories. Interestingly, the commonly used classification criteria codes were specified either for HL (e.g., PM2, BA1, BS1, BS1_Supporting, PP3, PP4) or, in collaboration with the ClinGen Sequence Variant Interpretation (SVI) workgroup, more broadly for recessive disorders (e.g., PM3) or any disorder (e.g., PP1). Application of criteria without disease-specific guidance is a significant contributor to conflicting classifications, emphasizing the importance of expert guidance and specification in usage of the ACMG/AMP rules. Several variants classified as P and LP also had BA1 and BS1 codes that were applied to them. Given that many of these variants were founder variants in specific subpopulations or had other evidence such as case–control data and case counts, the expert group decided to exclude the conflicting benign population frequency codes from the overall clinical interpretation of the variant.
Sharing of internal clinical laboratory case data among members of the HL VCEP has also served as an invaluable resource for resolving variants with conflicting interpretations. For example, the c.1708G>A (p.Val570Ile) variant in SLC26A4 previously had a conflicting classification and a medically significant classification difference of VUS vs LP. The HL VCEP resolved this conflict by counting 2 compound heterozygous internal cases from the Laboratory of Molecular Medicine, which led to the application of PM3_Strong, and PP4, leading to a LP classification. Without these internal cases, the variant would have been classified as VUS due to a lack of published case-level evidence.
Our curation process included bimonthly calls where biocurators first present all evidence used for each variant classification to the experts. Based on the feedback, biocurators often reached out to ClinVar submitters, authors of certain publications, and/or any of the experts to gather additional unpublished data required for final variant interpretation. The group also relied on feedback from expert clinicians regarding any genotype–phenotype correlations. The final evidence was then discussed on intervening monthly calls with the HL VCEP chairs, and if needed on subsequent calls with the larger group, to reach a final classification, including a text-based variant evidence summary documenting all applied evidence to be submitted to ClinVar and publicly accessible through ClinGen’s Evidence Repository (https://erepo.clinicalgenome.org/evrepo/). This process has been, and continues to be, optimized for more efficient expert interpretations while still leveraging the diverse expertise within the group. It is important to note that this initial effort was mostly focused on variants with conflicting or uncertain significance to highlight the utility of the specified rules. In this process, a significant effort was dedicated to contacting ClinVar submitters and obtaining additional unpublished evidence to resolve interpretation discrepancies. We therefore expect this process to be faster for novel variants or ones without conflicting evidence. Ultimately, this process can be optimized to strike a balance between efficiency and leveraging the expertise of any disease group.
We have focused this pilot project on variants in nine HL-associated genes, USH2A, SLC26A4, GJB2, MYO7A, CDH23, TECTA, COCH, KCNQ4, and MYO6, for which ACMG/AMP specifications were tailored. However, most of those specified rules are equally applicable to other HL-associated genes. As such, the population frequency (BA1, BS1, PM2), allelic (PM3, BP2), de novo (PS2, PM6), segregation (PP1), predicted effects (PVS1, PM4, PP3, BP3, BP4, BP7), case–control (PS4), and their varied strength levels as specified by the expert group, are currently being extended to other genes. The group will also continue to prioritize curation of variants in HL genes with medically significant differences and those of uncertain significance.
In summary, our study shows that expert curation using disease-specific modifications of ACMG/AMP guidelines resolves discrepancies in variant classification, leading to more consistent results for patients in need of accurate diagnoses and management decisions.
Data availability
All variants were submitted to ClinVar by the HL-EP. Refer to Supplementary Table 1 for a list of all variants and their ClinVar IDs.
References
Alford RL, Arnos KS, Fox M, Lin JW, Palmer CG, Pandya A, et al. American College of Medical Genetics and Genomics guideline for the clinical evaluation and etiologic diagnosis of hearing loss. Genet Med. 2014;16:347–55.
Abou Tayoun AN, Al Turki SH, Oza AM, Bowser MJ, Hernandez AL, Funke BH, et al. Improving hearing loss gene testing: a systematic review of gene evidence toward more efficient next-generation sequencing-based diagnostic testing and interpretation. Genet Med. 2016;18:545–53.
DiStefano MT, Hughes MY, Patel MJ, Wilcox EH, Oza AM. Expert interpretation of genes and variants in hereditary hearing loss. Medizinische Genetik. 2020;32:109–15.
Shearer AE, Shen J, Amr S, Morton CC, Smith RJ. A proposal for comprehensive newborn hearing screening to improve identification of deaf and hard-of-hearing children. Genet Med. 2019;21:2614–30.
Oza AM, DiStefano MT, Hemphill SE, Cushman BJ, Grant AR, Siegert RK, et al. Expert specification of the ACMG/AMP variant interpretation guidelines for genetic hearing loss. Hum Mutat. 2018;39:1593–613.
Shen J, Oza AM, del Castillo I, Duzkale H, Matsunaga T, Pandya A, et al. Consensus interpretation of the p.Met34Thr and p.Val37Ile variants in GJB2 by the ClinGen Hearing Loss Expert panel. Genet Med. 2019;21:2442–52.
DiStefano MT, Hemphill SE, Oza AM, Siegert RK, Grant AR, Hughes MY, et al. ClinGen expert clinical validity curation of 164 hearing loss gene–disease pairs. Genet Med. 2019;21:2239–47.
Harrison SM, Dolinsky JS, Knight Johnson AE, Pesaran T, Azzariti DR, Bale S, et al. Clinical laboratories collaborate to resolve differences in variant interpretations submitted to ClinVar. Genet Med. 2017;19:1096–104.
Abou Tayoun AN, Pesaran T, DiStefano MT, Oza A, Rehm HL, Biesecker LG, et al. Recommendations for interpreting the loss of function PVS1 ACMG/AMP variant criterion. Hum Mutat. 2018;39:1517–24.
Azaiez H, Booth KT, Ephraim SS, Crone B, Black-Ziegelbein EA, Marini RJ, et al. Genomic landscape and mutational signatures of deafness-associated genes. Am J Hum Genet. 2018;103:484–97.
Stenson PD, Mort M, Ball EV, Shaw K, Phillips A, Cooper DN, et al. The Human Gene Mutation Database: building a comprehensive mutation repository for clinical and molecular genetics, diagnostic testing and personalized genomics medicine. Hum. Genet. 2014;133:1–9.
Fokkema IF, Taschner PE, Schaafsma GC, Celli J, Laros JF, den Dunnen JT, et al. LOVD v2.0: the next generation in gene variant databases. Hum. Mutat. 2011;32:557–63.
Allot A, Peng Y, Wei C-H, Lee K, Phan L, Lu Z, et al. LitVar: a semantic search engine for linking genomic variant data in PubMed and PMC. Nucleic Acids Res. 2018;46:W530–6.
Ioannidis NM, Rothstein JH, Pejaver V, Middha S, McDonnell SK, Baheti S, et al. REVEL: an ensemble method for predicting the pathogenicity of rare missense variants. Am J Hum Genet. 2016;99:877–85.
Acknowledgements
The authors would like to acknowledge Larry Babb for his help in compiling data from ClinVar to conduct some of these analyses. Research reported in this publication was supported by the National Human Genome Research Institute (NHGRI) under award number U41HG006834. The content is solely the responsibility of the author and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Consortia
Contributions
Conceptualization: A.A.T., S.A., H.L.R. Data curation: M.J.P., M.T.D., A.M.O., M.Y.H., E.H.W., S.H.E., B.J.C., R.G., R.K.S., A.C. Formal analysis: A.A.T., M.J.P. Funding acquisition: H.L.R. Writing—original draft: A.A.T., M.J.P. Writing—review & editing: M.T.D., A.M.O., M.Y.H., E.H.W., S.H.E., B.J.C., R.G., R.K.S., A.C., J.S., N.J.B., L.A.S., K.N., M.K., H.A., K.T.B., A.G., K.B.A., H.K., H.L.R., S.A.
Corresponding author
Ethics declarations
Ethics Declaration
All curated variants were obtained from ClinVar, and were therefore, publicly available. As per ClinVar policy, variant submitters are expected to have obtained appropriate consent for data submission and sharing.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Patel, M.J., DiStefano, M.T., Oza, A.M. et al. Disease-specific ACMG/AMP guidelines improve sequence variant interpretation for hearing loss. Genet Med 23, 2208–2212 (2021). https://doi.org/10.1038/s41436-021-01254-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41436-021-01254-2
