Article Text

Abstract
Objective To identify factors associated with sight-threatening diabetic macular oedema (STDM) in Indigenous Australians attending an Indigenous primary care clinic in remote Australia.
Methods and analysis A cross-sectional study design of retinopathy screening data and routinely-collected clinical data among 236 adult Indigenous participants with type 2 diabetes (35.6% men) set in one Indigenous primary care clinic in remote Australia. The primary outcome variable was STDM assessed from retinal images.
Results Age (median (range)) was 48 (21–86) years, and known diabetes duration (median (range)) was 8.0 (0–24) years. Prevalence of STDM was high (14.8%) and similar in men and women. STDM was associated with longer diabetes duration (11.7 vs 7.9 years, respectively; p<0.001) and markers of renal impairment: abnormal estimated Glomerular Filtration Rate (eGFR) (62.9 vs 38.3%, respectively; p=0.007), severe macroalbuminuria (>300 mg/mmol) (20.6 vs 5.7%, respectively; p=0.014) and chronic kidney disease (25.7 vs 12.2%, respectively; p=0.035). Some clinical factors differed by sex: anaemia was more prevalent in women. A higher proportion of men were smokers, prescribed statins and had increased albuminuria. Men had higher blood pressure, but lower glycated Haemoglobin A1c (HbA1c) levels and body mass index, than women.
Conclusion STDM prevalence was high and similar in men and women. Markers of renal impairment and longer diabetes duration were associated with STDM in this Indigenous primary care population. Embedded teleretinal screening, known diabetes duration-based risk stratification and targeted interventions may lower the prevalence of STDM in remote Indigenous primary care services.
Trial registration number Australia and New Zealand Clinical Trials Register: ACTRN 12616000370404.
- epidemiology
- imaging
- macula
- public health
- retina
- telemedicine
- pathology
- vision
Data availability statement
Data may be obtained from a third party and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Vision loss in diabetes is mainly due to maculopathy. The prevalence of diabetic maculopathy is higher and diabetic eye screening coverage is lower among Indigenous than non-Indigenous Australians.
What are the new findings?
Primary care associations with sight-threatening diabetic macular oedema (STDM) among people with type 2 diabetes routinely attending a geographically remote clinic were assessed for the first time. The group with STDM had a longer duration of known diabetes, and a higher proportion of those with STDM had markers of renal dysfunction and chronic kidney disease. Importantly, STDM was present in some with newly diagnosed diabetes.
How might these results change the focus of research or clinical practice?
There is a need for earlier and targeted primary care interventions, such as teleretinal diabetes eye screening and risk stratification by diabetes duration and renal dysfunction to reduce progression to STDM. Primary healthcare services require greater resources to better support timely eye screening and risk-stratification strategies among Indigenous Australians living with diabetes in remote Australia.
Introduction
The burden of diabetes continues to rise globally,1 causes a substantial reduction in disability-free life expectancy2 and disproportionately affects Indigenous Australians, who have a fourfold higher prevalence of diabetes3 4 and a threefold higher prevalence of vision loss than non-Indigenous Australians.5 Sight-threatening diabetic macular oedema (STDM) is now a more common cause of vision loss in diabetes than proliferative diabetic retinopathy (PDR),6 and both have been shown to predict cardiovascular disease (CVD),7 renal disease and mortality. If timely, the frontline ocular treatments of intravitreal injections and/or laser for STDM are highly effective8 and vision outcomes are similar in Indigenous and non-Indigenous Australians.9 However, recent national data confirm the prevalence of STDM remains higher among Indigenous than non-Indigenous Australians (6.0 vs 3.8%),10 higher than has been reported in a review of previous Indigenous Australian diabetes studies11 and much higher than in some Indigenous populations, such as American Indians and Alaskan Natives in whom reported STDM prevalence was 0.9%.12
In predominantly non-Indigenous adults with type 2 diabetes (T2D), once-daily oral fenofibrate has been shown by the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) and Action to Control Cardiovascular Risk in Diabetes (ACCORD) lipid trials to significantly reduce the risk of both STDM and PDR,13 14 suggesting medical management of diabetic retinopathy (DR) with fenofibrate might be a useful primary care intervention to attenuate the risk of STDM in remote Australia. DR assessment in Australia is largely government funded and undertaken by the ophthalmic workforce in eye-care clinics or ophthalmic outreach services. Increasingly, DR screening of Indigenous Australians in non-urban regions occurs as a telemedicine service provided by non-ophthalmic primary care clinical staff, trained as retinal imagers and offsite certified retinal graders.
Until recently, the earliest stages of diabetic maculopathy have been difficult to detect with common DR screening technologies, typically non-stereo retinal fundus images obtained using non-mydriatic retinal cameras. Consequently, more comprehensive documentation of the epidemiology of diabetic maculopathy lags that of what is known about DR.15 However, it is established that diabetic maculopathy can develop at any stage of DR, as STDM can be detected in the absence of other extramacular DR, and that the risk of developing STDM increases with the severity of DR. While there is evidence that (extramacular) retinopathy and maculopathy share common risk factors, the epidemiology of maculopathy may differ in type 1 (T1D) and T2D, suggesting risk profiles for maculopathy may be population specific. For example, the risk of maculopathy is greater in (T1D) than in T2D for any duration of diabetes greater than 10 years, while risk of maculopathy is associated with hypertension only in T2D and with hyperlipidaemia only in (T1D).16 Diabetic maculopathy prevalence varies globally between 5.0% in combined Asian and 10.4% in African American populations,17 but whether associations with STDM are ethnicity specific and/or management dependent remains unclear.12
We hypothesised routinely collected clinical risk factor data elements and not achieving clinical targets were associated with STDM among Indigenous Australians with T2D in a remote Indigenous primary healthcare setting. Therefore, our objectives were to identify associations between clinical risk factors (exposures) and STDM (outcome) in a primary care setting.
Materials and methods
Eligible primary care patients (Indigenous adults age ≥18 years; n=301) with diagnosed T2D and at least 6 months of clinical data were recruited from a remote primary care service in Central Australia where the health service board approved researcher access to relevant electronic health record data for patients screened for DR between 2014 and 2016, as previously published.11 The general primary care clinic was the only source of female participants. Male patients sometimes preferred to attend a Men’s Clinic on a separate site nearby. Required exposure data from clinical records (current diabetes duration, HbA1c, blood pressure and lipid levels, anthropometric and renal function measures, insulin use and smoking status) were available for 281 adults in the retinopathy screened group, and 236 of these had both current clinical and gradable diabetic maculopathy data (‘participants’) for the maculopathy substudy (figure 1).

Flow diagram for participation in sight-threatening diabetic macular oedema (STDM) study.
DR screening and treatment coverage, prevalence and vision findings have been reported elsewhere.11 Briefly, the DR screening protocol was as follows: Presenting vision, either unaided or aided, was recorded. Selective pupil dilation was used, that is, mydriatic eye drops (one each of 1% tropicamide and 2.5% phenylephrine) were instilled either by a clinician, certified imager, or by a non-clinical/inexperienced imager under clinical supervision, unless pupil diameter was adequate (≥4 mm), mydriatic drops were contraindicated or clinical supervision was unavailable. Five 45° retinal fundus fields and one anterior eye/external field per eye were imaged. Imaging studies were graded remotely by certified retinal graders in the Centre for Eye Research Australia at the Royal Victorian Eye and Ear Hospital in Melbourne. Type and number of retinal lesions were recorded and a grading algorithm provided a preliminary retinopathy and maculopathy grade that could be modified by the grader who allocated a final ‘worse-eye’ grade. The grading report was uploaded to the electronic health record system of the remote health service. A clinician actioned the report based on the participant’s prior ocular history, for example, urgent referral to an ophthalmologist if no prior ‘referral to’ or ‘report from’ an ophthalmologist was present in the patient’s electronic health record.
Screening and action recommendations were based on the 2008 National Health and Medical Research Council of Australia Guidelines for the Management of Diabetic Retinopathy,18 in which the Early Treatment Diabetic Retinopathy Study classification ‘clinically-significant diabetic macular oedema’ (defined as any of the following characteristics: thickening of the retina at or within 500 µm of the centre of the macula; hard exudates at or within 500 µm of the centre of the macula, if associated with thickening of the adjacent retina (not residual hard exudates remaining after disappearance of retinal thickening); a zone or zones of retinal thickening one disc area or larger, any part of which is within one disc diameter of the centre of the macula is considered to be sight-threatening maculopathy, that is, STDM. The United Kingdom’s National Health Scheme Diabetic Eye Screening Programme grading equivalent would be Maculopathy level 1 (MI) plus some level of retinopathy (R1-3), for example, M1R2.19
Statistical analysis
Descriptive statistics and complete-case analysis were used to examine subgroups: demographic and clinical characteristics of participants were compared using one-way analysis of variance for categorical independent variables and normally distributed dependent variables or non-parametric tests for non-normally distributed continuous dependent variables and χ2 tests for categorical variables. Participant clinical characteristics were summarised by sex (due to potential sex differences in the clinical setting (men could attend the General or a Men’s Clinic (on a separate site) while all women attended the General Clinic), management and reported differences in clinical risk factors between Indigenous men and women nationally: for example, Indigenous women have a higher prevalence of diabetes and obesity, while smoking is more prevalent among Indigenous men) and by STDM status as mean (95% CI) or median (IQR) for continuous variables or percentages (counts) for categorical data. A probability of p<0.05 was taken as statistically significant. Statistical analyses were conducted with IBM SPSS Statistics (V.25.0).
Patient and community involvement
This study was supported throughout by Indigenous community members and patients who were members on the board of the participating Indigenous health service. Other supporters were the study’s Indigenous liaison officer and Aboriginal Health Worker staff who assisted in modifying study protocols to minimise participation time, facilitate recruitment, ensure development of culturally safe protocols and facilitate dissemination of the health information and study results as appropriate to family, friends and their community.
Results
Of 281 individuals who had undergone retinal fundus imaging and had clinical risk factor data, 236 (78.4%) had images gradable for maculopathy (35.6% male). STDM study participant (n=236) and non-participant (n=45) characteristics were similar but for the older age of non-participants (57 (51–68) years), who had ungradable images primarily due to cataract, as reported previously.11 Participant characteristics were: median (IQR) age 48 (40–56) years, known diabetes duration 8.0 (3.0–12.0) years, HbA1c 8.5 (6.8–10.4) %, (HbA1c 69 (51–90) mmol/mol), systolic/diastolic blood pressure 126/76 (115/70–140/82) mm Hg, low-density lipoprotein (LDL) cholesterol/high-density lipoprotein (HDL) cholesterol 2.3/1.0 (1.8/0.8–2.8/1.1) mmol/L, body mass index (BMI) 30.6 (26.3–35.3) kg/m2 and urinary albumin to creatinine ratio 5.1 (1.0–36.3) mg/mmol. Prevalence of STDM was 14.8% (n=35).
Participant characteristics by sex are reported in table 1. The proportion of men and women who had STDM, insulin prescribed, achieved lipid targets and normal eGFR was similar. On average, women had a higher HbA1c, but lower systolic and diastolic blood pressure than men. A higher proportion of men than women were former or current smokers, hypertensive or albuminuric (elevated urinary albumin to creatinine ratio). Women were more likely to be anaemic, while men were more likely to have been prescribed statins.
Characteristics of participants, according to sex
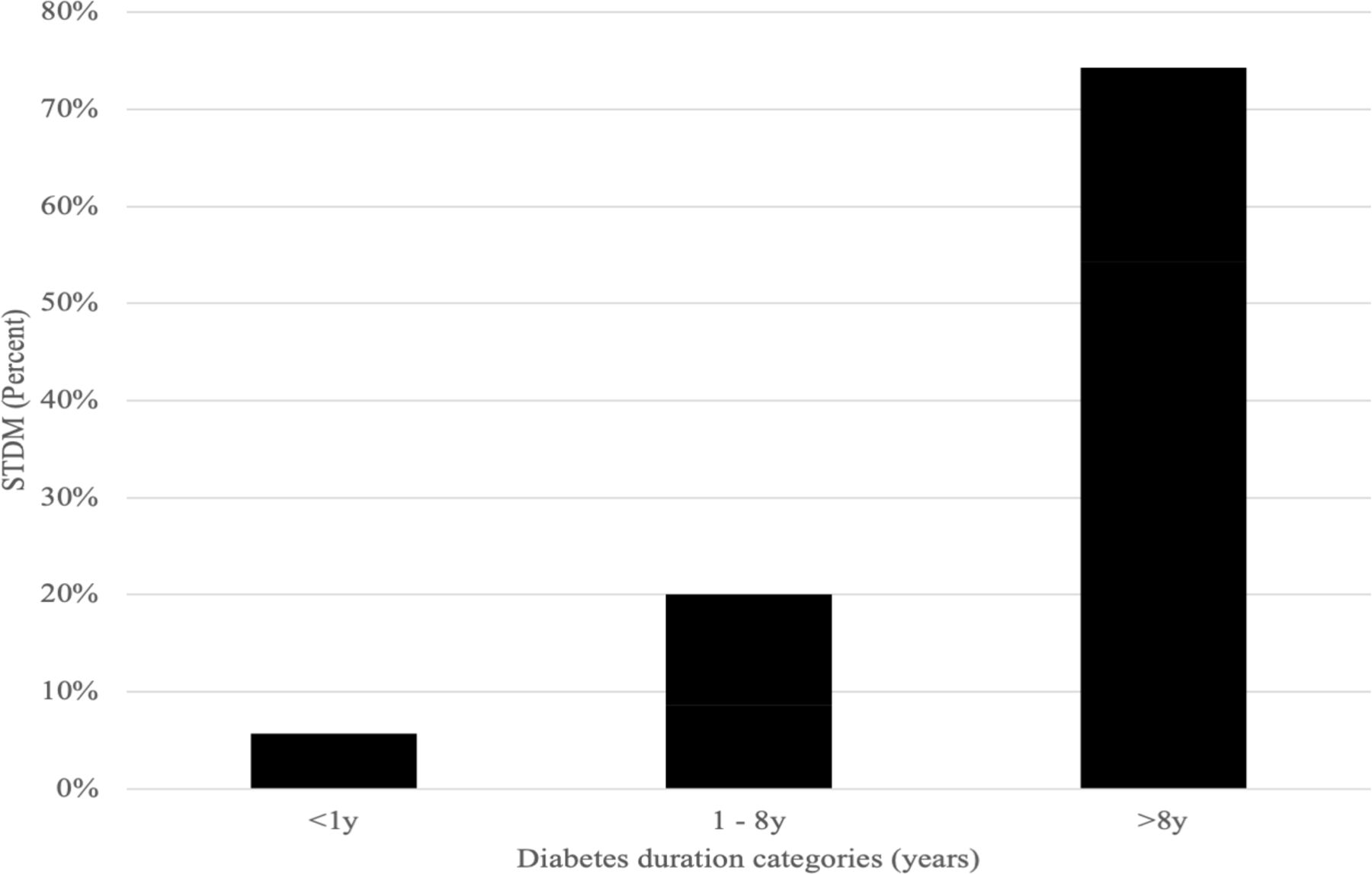
The clinical profile of STDM (table 2) shows STDM was associated with longer known diabetes duration (figure 2), HbA1c above 9% (75 mmol/mol), lower BMI, severe macroalbuminuria, abnormal eGFR and chronic kidney disease. The STDM subset participants were less likely to be overweight or obese, and there was also a (non-significant) trend in the STDM group towards higher rates of anaemia and prescribed insulin (31.0% vs 17.8%, p=0.094% and 31.4% vs 17.9%, p=0.065, respectively).

{kind=link}
{kind=link}
Sight-threatening diabetic macular oedema (STDM) (%) by duration of diabetes categories.
Primary care clinical associations with sight-threatening diabetic macular oedema (STDM)
Discussion
To the best of our knowledge, this is the first study to describe the factors associated with STDM among Indigenous Australians in a remote primary-care setting. STDM prevalence was higher in both Indigenous men (13.1%) and women (15.8%) than reported in a recent national eye survey (6.0% Indigenous; 3.8% non-Indigenous),10 earlier Indigenous studies,11 and global data (7.4%).17 By contrast, the remarkably low STDM rate of 0.9% (n=394) among 46 853 Indigenous Americans screened by the Indian Health Service12 is noteworthy: In that cohort, STDM was associated with longer diabetes duration (as in this study), insulin use (a similar trend in this study), and a high HbA1c, that is, greater than 10% (86 mmol/mol) (greater than 9% (75 mmol/mol) in this study). While diabetic eye disease screening protocols differed between some of these studies, all protocols had adequate sensitivity for the detection of treatable diabetic maculopathy, that is, clinically-significant diabetic macular oedema (STDM), and it is unlikely the reported prevalence differences can be attributed to heterogeneous screening protocols.
Implications of diabetes duration in primary care practice
Our findings suggest that among Indigenous Australians, diabetes duration may be a useful risk marker for STDM, the most common cause of impaired vision and blindness in diabetic populations and an important predictor of other complications and all-cause mortality.20 Diabetes duration also predicts non-referable DR, which can now be treated medically with fenofibrate in Australians with T2D and existent retinopathy, independent of lipid levels, by primary care doctors or nurse practitioners with prescribing rights. Fenofibrate has also been approved for use to retard DR progression in T2D in 18 other countries (personal communication Abbott).
Until a validated Indigenous risk calculator for DR becomes available, an interim, simple and effective primary care risk management strategy worth consideration might be to triage those individuals with a known diabetes duration of over 10 years to more frequent comprehensive eye exams or camera-based DR screening where barriers to regular comprehensive eye exams exist. This strategy is supported by the findings in the 2016 National Eye Health Survey21 that reported only 53% of Indigenous Australians with diabetes are screened according to current evidence-based recommendations in Australia’s Clinical Guidelines for the Management of Diabetic Retinopathy.18 By contrast, screening coverage of non-Indigenous Australians in the 2016 survey was 78%, and this difference in screening coverage may in part explain the lower blindness rate among non-Indigenous than Indigenous Australians. Importantly, treatment coverage in our study group was similar to national treatment coverage data for both Indigenous and non-Indigenous Australians, as reported previously.11 It is noteworthy that national screening recommendations have been unchanged for more than 20 years, that is, since 1997 when diabetic eye disease was declared a major public health problem by the Australian government.
Implications for primary care practice of age at diabetes diagnosis and established risk factors
The relatively younger age at diagnosis of diabetes among Indigenous than non-Indigenous Australians and the increasing life expectancy of Indigenous Australians may in part explain the higher prevalence of STDM observed among Indigenous Australians with diabetes in recent studies.10 11 Since most participants with STDM (78%) had already been treated for STDM, intensified primary care risk factor management post-STDM treatment may in part explain the lack of an association between STDM and some known modifiable retinopathy risk factors, such as HbA1c, blood pressure and lipids.
Elevated blood pressure is a risk factor for DR and maculopathy globally,15 22 23 but in this clinical population was not associated with STDM. As in most clinical populations with diabetes, HbA1c levels were suboptimal in this clinical population. However, the anticipated difference in HbA1c level between those with and without STDM was not observed, most likely due to the high STDM treatment coverage and post-treatment intensified glycaemic control in this setting, that is, the proportion with untreated STDM was 22%.
Given the prevalence of diabetes is almost sevenfold higher in Indigenous than non-Indigenous Australians in the 24–35 year age group and fourfold higher overall,3 these data suggest a need for intensified management of blood pressure and blood glucose levels in younger Indigenous Australians with diabetes.
We observed a non-statistical trend towards greater prescribed insulin in those with versus without STDM. Insulin use in T2D usually reflects longer diabetes duration, more advanced progression of the natural history of T2D with beta-cell failure, and of prior poor glycaemic control. Adherence to prescribed medications was not recorded routinely in clinical records, nor is linkage with pharmacy prescription dispensing data available in Australia. Therefore, it is possible that some medication usage misclassification may have occurred and reduced our ability to detect an association of for example, prescribed insulin with STDM.
The association between DR and nephropathy is well-known, and both are frequently asymptomatic. Therefore, detection in primary care of either renal or retinal disease in a person with diabetes flags the need to urgently screen for the other, and the urinary albumin to creatinine ratio, an important biomarker for microalbuminuria, and also plasma creatinine can now be performed as point-of-care pathology tests, ideal for remote healthcare services.24 25 Our findings also present a rationale for considering future diabetes eye screening studies of Indigenous Australians in renal clinics and dialysis centres, in addition to primary care settings, as such studies should facilitate DR detection and provide important insights into the observed STDM-renal association.
Obesity is a risk factor for the chronic complications of diabetes, including DR,22 yet we identified a novel inverse association between STDM and BMI. This may be due to unmeasured confounding, such as comorbid conditions, progressive beta cell failure with increasing duration of diabetes, or may reflect the need for caution in the standard interpretation of BMI that was developed as a measure of healthy weight in and for
Caucasian populations that have different body proportions to the Indigenous Australian population.26 27 A BMI cut-off of 22 kg/m2 has been suggested to define the upper limit of the healthy weight range for Indigenous Australians. Based on this cut-off, the proportion of participants in the non-overweight/obese range falls from 37.1% to 11.4% and the association between BMI status and STDM becomes statistically non-significant (p=0.157).
To date, risk management of diabetic eye disease in primary care has been based on treatment of established retinopathy risk factors (prevention), regular eye exams or camera-based retinopathy screening (early detection of disease), intensified treatment of risk factors (management of prevalent non-sight threatening disease) and referral of sight-threatening disease for tertiary treatment. More recently, DR risk calculators have been developed,28 29 but none are based on Indigenous eye data or specifically address risk of STDM, the most common cause of vision loss in diabetes. This is an important knowledge gap in Indigenous and eye health research. Until such a tool is developed, our findings together with current risk management approaches suggest strategies that may help address STDM risk in this setting, including risk stratification by diabetes duration; intensified management of risk factors associated with STDM, particularly in the younger diabetes-onset group, and primarily systolic hypertension and renal dysfunction. Furthermore, our findings strongly support an integrated telemedicine retinal screening programme in primary care services and/or community settings to augment existing ophthalmic services and address low screening coverage of Indigenous Australians with diabetes. Improved screening rates would not only identify people with or at high risk of STDM and related diabetes complications, but may alert clinicians when intensified management is needed to prevent STDM and related adverse outcomes. For example, formation of two or more microaneurysms between successive annual retinal screenings is a predictive marker for progression to STDM within 5 years.30 The importance of STDM extends well beyond the increased risk of vision loss and blindness, which is in itself a great individual, societal and public health burden. People with diabetic maculopathy are also at increased risk of incident CVD7 and premature mortality and so should be followed more closely and their risk factors aggressively treated.
We acknowledge both study strengths and limitations: importantly, this is the first study to examine STDM, the main cause of vision loss in diabetes globally, among Indigenous Australians. Furthermore, we shed light on modifiable clinical factors associated with the disproportionately high and increasing prevalence of STDM among Indigenous Australians with diabetes. We expect these findings to influence care provision of any person with diabetes who has any markers of renal dysfunction or duration of diabetes of at least 10 years by raising the treating doctor’s index of suspicion for STDM and awareness of the need for more frequent retinal screening. Importantly, the infrastructure and training for image-based diabetic eye screening in Indigenous primary care clinics has been largely funded by the Australian Government, and the screening is a reimbursable service under the national Medicare Health Benefits Scheme. Consequently, the clinical and cost effectiveness of the retinal screening model has already been established, and the granularity our findings provide will improve risk management of sight-threatening diabetic eye disease and lead to earlier detection and timelier treatment, thereby further improving clinical and cost effectiveness of this screening model.
However, the following limitations are noteworthy: there may be selection bias as some people with (known or unknown) T2D may not have attended a primary care clinic. Site differences may have contributed to the sex-specific associations with STDM, since male participants may have attended the Men’s Clinic rather than the General Clinic attended by female and male participants. However, unlike non-Indigenous studies where participation rates are similar by sex, Indigenous male participation rates are generally lower than Indigenous female participation rates in retinopathy screening studies. Causal inferences cannot be made given the cross-sectional nature of the data, that is, risk factor levels (eg, BMI, BP, HbA1c, levels, Albumin to Creatinine Ratio (ACR)) are reported at the time of assessment and not over time. T2D may be present for years prior to its formal diagnosis; hence, diabetes duration may be an underestimate. There may be measurement error in some clinical risk factors such as weight and blood pressure obtained by clinic staff. They were not verified by research staff. Due to the number with STDM, multivariate analysis was not undertaken. Similarly, the untreated STDM subset was too small to undertake subanalyses to compare clinical associations between treated and untreated STDM cases. Larger Indigenous STDM studies are needed to better understand the factors associated with STDM and the impact of STDM treatment on risk factor control, given the important association reported recently between diabetic eye disease and 10-year mortality in a remote Indigenous population.31
Finally, remoteness is a risk factor for other adverse health outcomes in Australia, notably diabetes,31 and may have been a contributing factor to the observed associations with STDM. However, our findings have face validity as they are broadly in line with current evidence. Moreover, our sample is representative of the Indigenous Australian population with diabetes on key parameters, such as prevalence of diabetes and risk factors for DR, and so we expect our findings to be generalisable to the Indigenous sector of the Australian population with diabetes.
The factors underpinning both the apparent susceptibility of remote-living Indigenous Australians to STDM and the different clinical profiles in Indigenous men and women, despite similarly high STDM prevalence rates, require further evaluation. Future Indigenous studies of diabetic maculopathy should include earlier (non-sight-threatening) stages of maculopathy as an outcome, now detectable with optical coherence tomography technology, and a broader range of exposures among Indigenous Australians in larger multicentre Australian studies that include urban, regional and very remote primary care settings. Given the high rates of STDM and blindness among Indigenous Australians and the approved use in Australia of fenofibrate for slowing retinopathy and maculopathy progression to sight-threatening stages and tertiary intervention,14 32 a fenofibrate intervention arm in future Indigenous primary care studies of diabetic eye diseases may be warranted. Fenofibrate can also slow the progression of renal dysfunction,14 33 which has recently been associated with 10-year mortality in this remote population.31 For successful implementation and effective outcomes of such studies and interventions, local Indigenous community support, culturally-sensitive protocols and collaboration with ophthalmic clinicians, ideally local, are essential.
Data availability statement
Data may be obtained from a third party and are not publicly available.
Ethics statements
Ethics approval
The University of Melbourne and the Central Australian Human Research Ethics Committees approved study conduct. Every participant provided written informed consent.
Acknowledgments
The authors acknowledge the traditional custodians of the land on which this study was conducted and wholeheartedly thank study participants and the dedicated study and clinic staff without whom this study would not have been possible (Aboriginal Health Practitioners, administrators, drivers, doctors and the chronic care team). The authors also thank the TEAMSnet Study Group, Partners and Collaborators: TEAMSnet Study Group: Chief investigators: Professor Sven-Erik Bursell, Professor Alex Brown, Professor Alicia Jenkins, Professor David O'Neal, Professor Danny Liew, Associate Investigators: Professor Tien Wong, Professor Hugh Taylor, Professor Anthony Keech, Professor Kerin O’Dea, Professor Ecosse Lamoureux, Dr Mark Horton, TEAMSnet Programme Director: Dr Laima Brazionis, TEAMSnet Project Manager: Christopher Ryan. Partners: Central Australian Aboriginal Congress [Alice Springs]; Aboriginal Medical Services Alliance [NT]; CERA [Melbourne]; Estenda Solutions [USA]; the Fred Hollows Foundation [Global]; The University of Melbourne; NHMRC Clinical Trials Centre [University of Sydney]. Collaborators: Telstra [Communicare]; Dr Tim Henderson [Ophthalmology Department Head, Alice Springs Hospital].
References
Footnotes
Contributors LB wrote the report and contributed to the design, implementation and conduct of the study and analyses. AK, CR, AB, DON, JB, S-EB and AJ provided input on study design and conduct and reviewed drafts of the manuscript. S-EB is the guarantor of this work and takes responsibility for the integrity of the data and accuracy of the analyses.
Funding This study was funded by the National Health and Medical Research Council of Australia [NHMRC] Centre for Research Excellence in Diabetic Retinopathy grant, an NHMRC Partnership Project grant and a Fred Hollows Foundation Global Partnership grant. Funding bodies had no input into the design or conduct of the study or the interpretation of results.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.