
Abstract
Background
The surgical approach to treat Bismuth type I and II hilar cholangiocarcinoma (HCCA) has been a topic of debate. We sought to characterize whether bile duct resection (BDR) with or without concomitant hepatic resection (HR) was associated with R0 margin status, as well as define the impact of HR+BDR versus BDR alone on long-term survival.
Methods
Patients who underwent curative-intent HR+BDR for HCCA between 2000 and 2014 were identified from a multi-institutional database. Perioperative and long-term outcomes were compared among patients who underwent BDR only, BDR+left hepatic resection (LHR), and BDR+right hepatic resection (RHR) for Bismuth type I and II HCCA.
Results
Among 257 patients with HCCA, 61 (23.7%) patients had a Bismuth type I (n=25, 41.0%) or II (n=36, 59.0%) lesion. The incidence of R0 resection after BDR only was the same as among patients after LHR and RHR (BDR 70.0% vs. BDR+LHR 71.4% vs. BDR+RHR 76.5%, p=0.891). In contrast, severe complications were more likely after LHR and RHR than BDR only (BDR 21.4% vs. BDR+LHR 60.0% and BDR+RHR 50.0%, p=0.041). Overall (median: BDR 20.9 vs. BDR+LHR 23.2 and BDR+RHR 25.0 months, p=0.213) and recurrence-free (median: BDR 13.4 vs. BDR+LHR 15.3 and BDR+RHR 25.0, p= 0.109) survival were comparable. On multivariable analysis, while CA19-9>37.0U/ml (Ref. CA19-9≤37.0U/ml, HR 3.2, 95% CI 1.1–9.4, p=0.035) and AJCC T3-T4 disease (Ref. T1-T2, HR 4.6, 95% CI 1.5–13.7, p=0.007) were associated with long-term survival, surgical approach was not (BDR+LHR: HR 1.0, 95% CI 0.5–2.2, p=0.937; BDR+RHR: HR 0.6, 95% CI 0.3–1.3, p=0.197).
Conclusion
R0 resection, overall survival, and recurrence-free survival were comparable among well-selected patients who had BDR versus BDR+HR for Bismuth type I and II HCCA.



Similar content being viewed by others


References
Nakeeb A, Pitt HA, Sohn TA, et al. Cholangiocarcinoma. A spectrum of intrahepatic, perihilar, and distal tumors. Ann Surg. 1996;224:463-473; discussion 473-465.
Mansour JC, Aloia TA, Crane CH, Heimbach JK, Nagino M, Vauthey JN. Hilar cholangiocarcinoma: expert consensus statement. HPB (Oxford). 2015;17:691-699.
Ma WJ, Li FY, Cheng NS. When Should Hepatectomy be Performed for the Treatment of Bismuth Type I and II Hilar Cholangiocarcinoma? Ann Surg Oncol. 2020;27:926-927.
Jarnagin WR, Fong Y, DeMatteo RP, et al. Staging, resectability, and outcome in 225 patients with hilar cholangiocarcinoma. Ann Surg. 2001;234:507-517; discussion 517-509.
Kobayashi A, Miwa S, Nakata T, Miyagawa S. Disease recurrence patterns after R0 resection of hilar cholangiocarcinoma. Br J Surg. 2010;97:56-64.
Rea DJ, Munoz-Juarez M, Farnell MB, et al. Major hepatic resection for hilar cholangiocarcinoma: analysis of 46 patients. Arch Surg. 2004;139:514-523; discussion 523-515.
Lee SG, Song GW, Hwang S, et al. Surgical treatment of hilar cholangiocarcinoma in the new era: the Asan experience. J Hepatobiliary Pancreat Sci. 2010;17:476-489.
Tsao JI, Nimura Y, Kamiya J, et al. Management of hilar cholangiocarcinoma: comparison of an American and a Japanese experience. Ann Surg. 2000;232:166-174.
Nagorney DM, Kendrick ML. Hepatic resection in the treatment of hilar cholangiocarcinoma. Adv Surg. 2006;40:159-171.
Weiss MJ, Cosgrove D, Herman JM, Rastegar N, Kamel I, Pawlik TM. Multimodal treatment strategies for advanced hilar cholangiocarcinoma. Langenbecks Arch Surg. 2014;399:679-692.
Cho MS, Kim SH, Park SW, et al. Surgical outcomes and predicting factors of curative resection in patients with hilar cholangiocarcinoma: 10-year single-institution experience. J Gastrointest Surg. 2012;16:1672-1679.
Nuzzo G, Giuliante F, Ardito F, et al. Improvement in perioperative and long-term outcome after surgical treatment of hilar cholangiocarcinoma: results of an Italian multicenter analysis of 440 patients. Arch Surg. 2012;147:26-34.
Zheng-Rong L, Hai-Bo Y, Xin C, et al. Resection and drainage of hilar cholangiocarcinoma: an 11-year experience of a single center in mainland China. Am Surg. 2011;77:627-633.
de Jong MC, Marques H, Clary BM, et al. The impact of portal vein resection on outcomes for hilar cholangiocarcinoma: a multi-institutional analysis of 305 cases. Cancer. 2012;118:4737-4747.
Xiang S, Lau WY, Chen XP. Hilar cholangiocarcinoma: controversies on the extent of surgical resection aiming at cure. Int J Colorectal Dis. 2015;30:159-171.
Ikeyama T, Nagino M, Oda K, Ebata T, Nishio H, Nimura Y. Surgical approach to bismuth Type I and II hilar cholangiocarcinomas: audit of 54 consecutive cases. Ann Surg. 2007;246:1052-1057.
Launois B, Terblanche J, Lakehal M, et al. Proximal bile duct cancer: high resectability rate and 5-year survival. Ann Surg. 1999;230:266-275.
Otani K, Chijiiwa K, Kai M, Ohuchida J, Nagano M, Kondo K. Role of hilar resection in the treatment of hilar cholangiocarcinoma. Hepatogastroenterology. 2012;59:696-700.
Chen RX, Li CX, Luo CH, et al. Surgical Strategies for the Treatment of Bismuth Type I and II Hilar Cholangiocarcinoma: Bile Duct Resection with or Without Hepatectomy? Ann Surg Oncol. 2020;27:3374-3382.
Kondo S, Hirano S, Ambo Y, et al. Forty consecutive resections of hilar cholangiocarcinoma with no postoperative mortality and no positive ductal margins: results of a prospective study. Ann Surg. 2004;240:95-101.
Lim JH, Choi GH, Choi SH, Kim KS, Choi JS, Lee WJ. Liver resection for Bismuth type I and Type II hilar cholangiocarcinoma. World J Surg. 2013;37:829-837.
Capussotti L, Muratore A, Polastri R, Ferrero A, Massucco P. Liver resection for hilar cholangiocarcinoma: in-hospital mortality and longterm survival. J Am Coll Surg. 2002;195:641-647.
Xiong J, Nunes QM, Huang W, et al. Major hepatectomy in Bismuth types I and II hilar cholangiocarcinoma. J Surg Res. 2015;194:194-201.
Zhang XF, Squires MH, 3rd, Bagante F, et al. The Impact of Intraoperative Re-Resection of a Positive Bile Duct Margin on Clinical Outcomes for Hilar Cholangiocarcinoma. Ann Surg Oncol. 2018;25:1140-1149.
Rizvi S, Gores GJ. Pathogenesis, diagnosis, and management of cholangiocarcinoma. Gastroenterology. 2013;145:1215-1229.
Klatskin G. Adenocarcinoma of the Hepatic Duct at Its Bifurcation within the Porta Hepatis. An Unusual Tumor with Distinctive Clinical and Pathological Features. Am J Med. 1965;38:241-256.
Ma WJ, Wu ZR, Shrestha A, et al. Effectiveness of additional resection of the invasive cancer-positive proximal bile duct margin in cases of hilar cholangiocarcinoma. Hepatobiliary Surg Nutr. 2018;7:251-269.
Li H, Qin Y, Cui Y, Chen H, Hao X, Li Q. Analysis of the surgical outcome and prognostic factors for hilar cholangiocarcinoma: a Chinese experience. Dig Surg. 2011;28:226-231.
Ribero D, Amisano M, Lo Tesoriere R, Rosso S, Ferrero A, Capussotti L. Additional resection of an intraoperative margin-positive proximal bile duct improves survival in patients with hilar cholangiocarcinoma. Ann Surg. 2011;254:776-781; discussion 781-773.
Anderson B, Doyle MBM. Surgical Considerations of Hilar Cholangiocarcinoma. Surg Oncol Clin N Am. 2019;28:601-617.
Hemming AW, Reed AI, Fujita S, Foley DP, Howard RJ. Surgical management of hilar cholangiocarcinoma. Ann Surg. 2005;241:693-699; discussion 699-702.
Otsuka S, Ebata T, Yokoyama Y, et al. Clinical value of additional resection of a margin-positive distal bile duct in perihilar cholangiocarcinoma. Br J Surg. 2019;106:774-782.
Seyama Y, Kubota K, Sano K, et al. Long-term outcome of extended hemihepatectomy for hilar bile duct cancer with no mortality and high survival rate. Ann Surg. 2003;238:73-83.
Sugiura T, Okamura Y, Ito T, et al. Left Hepatectomy with Combined Resection and Reconstruction of Right Hepatic Artery for Bismuth Type I and II Perihilar Cholangiocarcinoma. World J Surg. 2019;43:894-901.
Cheng QB, Yi B, Wang JH, et al. Resection with total caudate lobectomy confers survival benefit in hilar cholangiocarcinoma of Bismuth type III and IV. Eur J Surg Oncol. 2012;38:1197-1203.
Bhutiani N, Scoggins CR, McMasters KM, et al. The impact of caudate lobe resection on margin status and outcomes in patients with hilar cholangiocarcinoma: a multi-institutional analysis from the US Extrahepatic Biliary Malignancy Consortium. Surgery. 2018;163:726-731.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 17 kb)
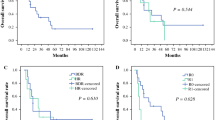
Supplementary Figure 1
Overall survival of patients who underwent bile duct resection only versus bile duct resection and left or right hepatic resection for Bismuth type I (a) or type II (b) hilar cholangiocarcinoma. (PNG 7767 kb)
Rights and permissions
About this article

Cite this article
Zhang, XF., Zhang, N., Tsilimigras, D.I. et al. Surgical Strategies for Bismuth Type I and II Hilar Cholangiocarcinoma: Impact on Long-Term Outcomes. J Gastrointest Surg 25, 3084–3091 (2021). https://doi.org/10.1007/s11605-021-05049-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-021-05049-3