
Deploying a Fotonovela to Combat Methamphetamine Abuse among South Africans with Varying Levels of Health Literacy


Abstract
:1. Introduction
1.1. The Problem of Methamphetamine Use
1.2. Effects of Low Levels of Education and Literacy
1.3. Entertainment-Education to Counter the Effects of Low Health Literacy Levels
1.4. An Earlier Study into the Possible Advantages of a Fotonovela to Combat Methamphetamine Abuse in South Africa
1.5. Knowledge Gaps after the Initial Study
1.6. Research Questions for the New Fotonovela Study about MA Use in South Africa
1.7. Structure of the Rest of the Article
2. Methods
2.1. Method for the Part of the Study Related to RQ1
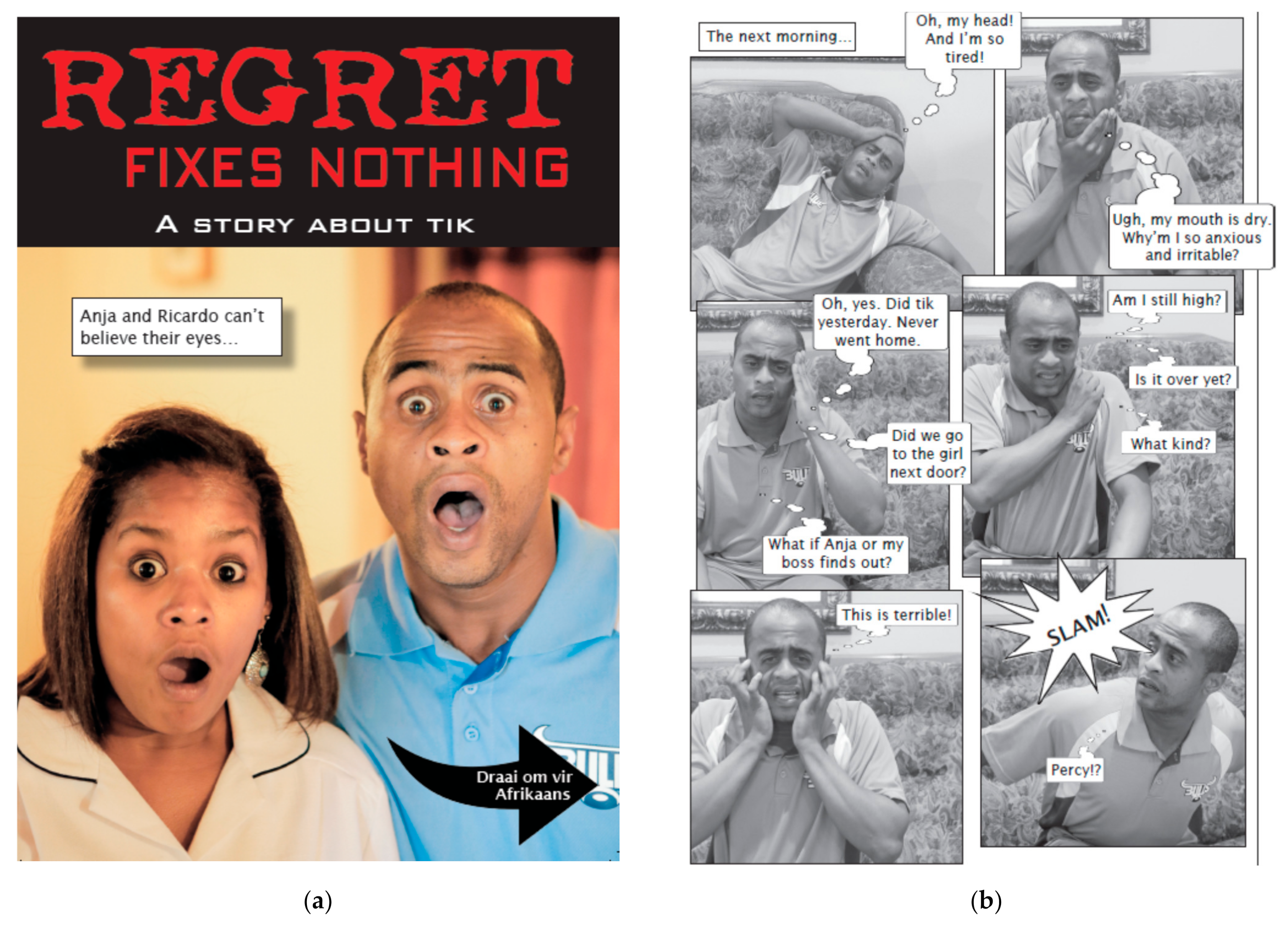
2.1.1. Materials
2.1.2. Participants
2.1.3. Measures
Health Literacy
Knowledge Level
Attitudes and Intentions
- Attitude toward MA Use
- Intention to Use MA
- Attitude toward Starting Conversations about MA
- Intention to Start Conversations about MA
Health Message Preference
2.1.4. Procedure
2.1.5. Statistical Analyses
2.2. Method for the Part of the Study Related to RQ2
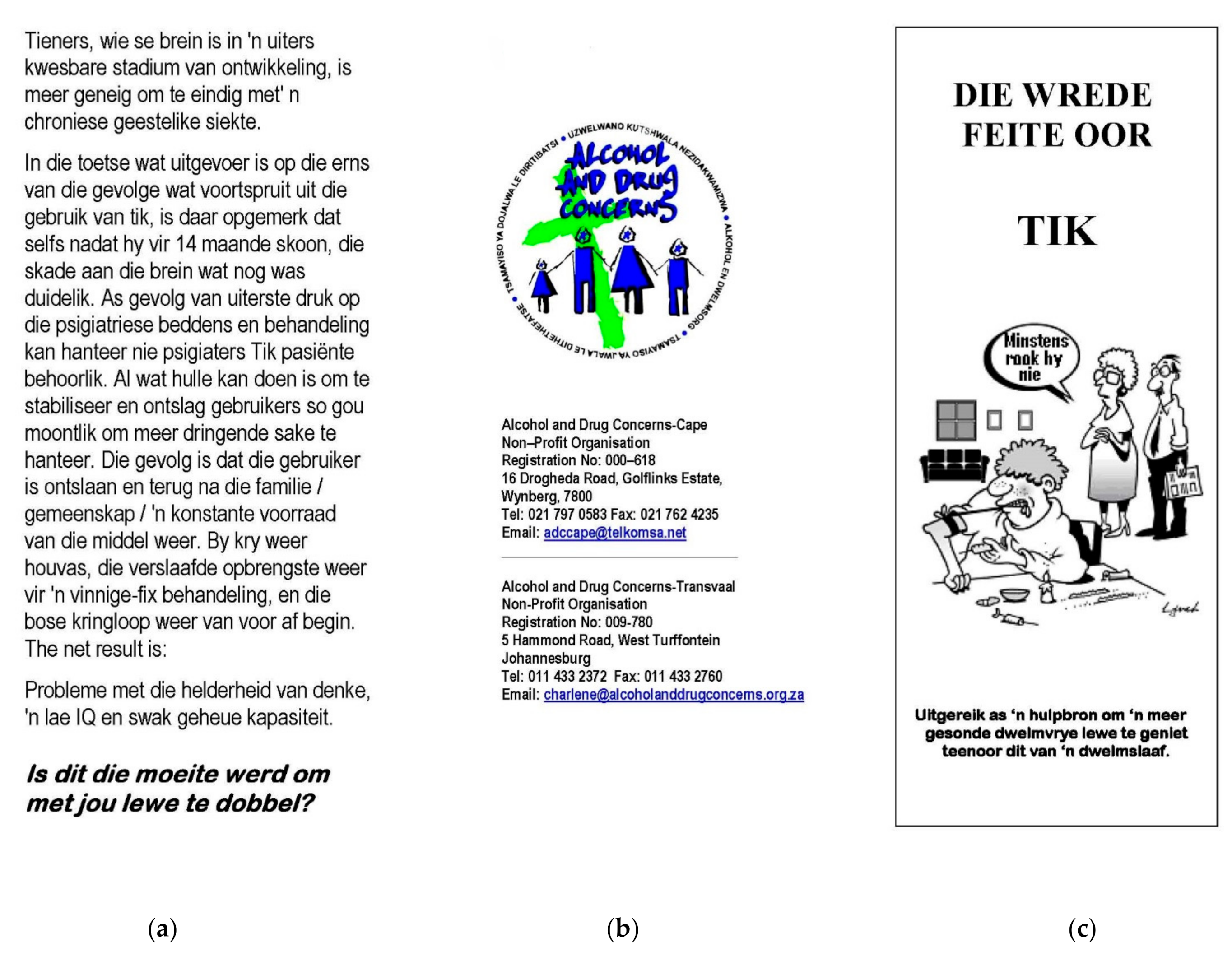
2.2.1. Materials
2.2.2. Participants
2.2.3. Measures
Health Message Preference
Evaluation of Fotonovela Use
2.2.4. Procedure
2.2.5. Statistical Analyses
3. Results
3.1. Results for the Part of the Study Related to RQ1
3.1.1. Knowledge Level
3.1.2. Attitude and Intention toward MA Usage
3.1.3. Attitude toward Starting MA Conversations
3.1.4. Intention to Start Conversations about MA
3.1.5. Health Message Preference
3.2. Results for the Part of the Study Related to RQ2
3.2.1. Health Message Preference
3.2.2. Evaluation of Fotonovela Use
4. General Discussion
4.1. Strengths and Limitations
4.2. Implications for Practice
4.3. Implications for Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Okafor, C.N.; Stein, D.J.; Dannatt, L.; Ipser, J.; van Nunen, L.J.; Lake, M.T.; Krishnamurti, T.; London, E.D.; Shoptaw, S. Contingency management treatment for methamphetamine use disorder in South Africa. Drug Alcohol Rev. 2020, 39, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Watt, M.H.; Meade, C.S.; Kimani, S.; MacFarlane, J.C.; Choi, K.W.; Skinner, D.; Pieterse, D.; Kalichman, S.C.; Sikkema, K.J. The impact of methamphetamine (“tik”) on a peri-urban community in Cape Town, South Africa. Int. J. Drug Policy 2014, 25, 219–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Social Development, South Africa. The National Drug Master Plan (NDMP) 2018–2024; Department of Social Development, South Africa: Pretoria, South Africa. Available online: https://www.gov.za/sites/default/files/gcis_document/202006/drug-master-plan.pdf (accessed on 15 May 2021).
- Plüddemann, A.; Myers, B.J.; Parry, C.D. Surge in treatment admissions related to methamphetamine use in Cape Town, South Africa: Implications for public health. Drug Alcohol Rev. 2008, 27, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Weybright, E.H.; Caldwell, L.L.; Wegner, L.; Smith, E.A.; Jacobs, J.J. The state of methamphetamine (‘tik’) use among youth in the Western Cape, South Africa. SAMJ 2016, 106, 1125–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasche, S.; Myers, B. Substance misuse trends in South Africa. Hum. Psychopharmacol. 2012, 27, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Peltzer, K.; Ramlagan, S.; Johnson, B.D.; Phaswana-Mafuya, N. Illicit drug use and treatment in South Africa: A review. Subst. Use Misuse 2010, 45, 2221–2243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puljević, C.; Learmonth, D. Substance abuse prevention in Cape Town’s peri-urban settlements: Local health trainers’ perspectives. Health Psychol. Behav. Med. 2014, 2, 183–197. [Google Scholar] [CrossRef]
- Asante, K.O.; Lentoor, A.G. Use of crystal methamphetamine among male adolescents in Cape Town, South Africa: Caregivers’ experiences. Subst. Abuse Treat. Prev. Policy 2017, 12, 18. [Google Scholar] [CrossRef] [Green Version]
- The Citizen. City of Cape Town’s Drug Strategy ‘Puts Prevention First [Press Release]. Available online: https://citizen.co.za/news/south-africa/1551445/city-cape-towns-drug-strategy-puts-prevention-first/ (accessed on 15 May 2021).
- Davis, B.; Jansen, C. Using a fotonovela to battle chrystal meth in South Africa. J. Ethn. Subst. Abuse 2020, 19, 151–169. [Google Scholar] [CrossRef]
- Monitoring Alcohol, Tobacco, and Other Drug Use Trends (South Africa): January–June 2020 (Update). Available online: https://www.careljansen.nl/SACENDU_Update_PHASE_48_Final.pdf (accessed on 15 May 2021).
- Hobkirk, A.L.; Watt, M.A.; Myers, B.; Skinner, D.; Meade, C.S. A qualitative study of methamphetamine initiation in Cape Town, South Africa. Int. J. Drug Policy 2016, 30, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Statistics South Africa. General Household Survey 2017 [Report No. PO318, 2018]. Available online: https://www.statssa.gov.za/publications/P0318/P03182017.pdf (accessed on 15 May 2021).
- Vágvölgyi, R.; Bergström, K.; Bulajić, A.; Klatte, M.; Fernandes, T.; Grosche, M.; Huettig, F.; Rüsseler, J.; Lachmann, T. Functional illiteracy and developmental dyslexia: Looking for common roots. A systematic review. J. Cult. Cogn. Sci. 2021, 1–21. [Google Scholar] [CrossRef]
- Parker, R.M.; Baker, D.W.; Williams, M.V.; Nurss, J.R. The test of functional health literacy in adults: A new instrument for measuring patents’ literacy skills. J. Gen. Intern. Med. 1995, 10, 537–541. [Google Scholar] [CrossRef]
- Williams, M.V.; Parker, R.M.; Baker, D.W.; Parikh, N.S.; Pitkin, K.; Coates, W.C.; Nurss, J.R. Inadequate functional health literacy among patients at two public hospitals. JAMA 1995, 274, 1677–1682. [Google Scholar] [CrossRef]
- Kutner, M.; Greenberg, E.; Jin, Y.; Paulsen, C. The Health Literacy of America’s Adults: Results from the 2003 National Assessment of Adult Literacy (NCES 2006-483); National Center for Education Statistics, US Department of Education: Washington, DC, USA, 2006.
- Dewalt, D.A.; Berkman, N.D.; Sheridan, S.; Lohr, K.N.; Pignone, M.P. Literacy and health outcomes. J. Gen. Intern. Med. 2004, 19, 1228–1239. [Google Scholar] [CrossRef]
- Geboers, B.; Reijneveld, S.A.; Jansen, C.J.M.; de Winter, A.F. Health literacy is associated with health behaviors and social factors among older adults: Results from the life lines cohort study. J. Health Commun. 2016, 21, 45–53. [Google Scholar] [CrossRef]
- Van’t Jagt, R.K.; Hoeks, J.C.J.; Duizer, E.; Baron, M.; Molina, G.B.; Unger, J.B.; Jansen, C.J.M. Sweet temptations: How does reading a fotonovela about diabetes affect Dutch adults with different levels of literacy? Health Commun. 2018, 33, 284–290. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, M.Y.; Organista, K.C. Entertainment-education? A fotonovela? A new strategy to improve depression literacy and help-seeking behaviors in at-risk immigrant Latinas. Am. J. Community Psychol. 2013, 52, 224–235. [Google Scholar] [CrossRef]
- Singhal, A.; Rogers, E.M. Entertainment Education: A Communication Strategy for Social Change; Lawrence Erlbaum Associates Inc.: Mahwah, NJ, USA, 1999. [Google Scholar]
- Unger, J.B.; Molina, G.B.; Baron, M. Evaluation of sweet temptations, a fotonovela for diabetes education. Hisp. Health Care Int. 2009, 7, 145–152. [Google Scholar] [CrossRef]
- Cabassa, L.J.; Contreras, S.; Aragón, R.; Molina, G.B.; Baron, M. Focus group evaluation of “Secret Feelings”: A depression fotonovela for Latinos with limited English proficiency. Health Promot. Pract. 2012, 12, 840–847. [Google Scholar] [CrossRef] [Green Version]
- Cabassa, L.J.; Molina, G.B.; Baron, M. Depression fotonovela: Development of a depression literacy tool for Latinos with limited English proficiency. Health Promot. Pract. 2012, 13, 747–754. [Google Scholar] [CrossRef]
- Unger, J.B.; Cabassa, L.J.; Molina, G.B.; Contreras, S.; Baron, M. Evaluation of a fotonovela to increase depression knowledge and reduce stigma among Hispanic adults. J. Immigr. Minor. Health 2013, 15, 398–406. [Google Scholar] [CrossRef] [Green Version]
- James, S.; Reddy, P.S.; Ruiter, R.A.C.; Taylor, M.; Jinabhai, C.C.; van Empelen, P.; van den Borne, B. The effects of a systematically developed photo-novella on knowledge, attitudes, communication and behavioural intentions with respect to sexually transmitted infections among secondary school learners in South Africa. Health Promot. Int. 2005, 20, 157–165. [Google Scholar] [CrossRef] [Green Version]
- Valle, R.; Yamada, A.M.; Matiella, A.C. Fotonovelas: A health literacy tool for educating Latino older adults about dementia. Clin. Gerontol. 2006, 30, 71–88. [Google Scholar] [CrossRef]
- Boyte, R.M.; Pilisuk, T.; Matiella, A.C.; Macario, E. Developing a bilingual fotonovela to encourage human papillomavirus preteen immunization in California: A case study. Calif. J. Health Promot. 2014, 12, 1–13. [Google Scholar] [CrossRef]
- Chan, A.; Brown, B.; Sepulveda, E.; Teran-Clayton, L. Evaluation of fotonovela to increase human papillomavirus vaccine knowledge, attitudes, and intentions in a low-income Hispanic community. BMC Res. Notes 2015, 8, 615. [Google Scholar] [CrossRef] [Green Version]
- Davis, H.D. Spyt Kom te Laat: The Development and Evaluation of a Health-Related Fotonovela about Methamphetamine (‘Tik’) Use in the Western Cape and Northern Cape Provinces of South Africa. Ph.D. Thesis, Stellenbosch University, Stellenbosch, South Africa, 2017. [Google Scholar]
- Isaacs, F.; Department of Social Development, Western Cape Government Health, Western Cape Province, South Africa. Personal communication, 2021.
- Zamora, H.; Clingerman, E.M. Health literacy among older adults: A systematic literature review. J. Gerontol. Nurs. 2011, 37, 41–51. [Google Scholar] [CrossRef]
- Van’t Jagt, R.K.; Tan, S.L.; Hoeks, J.C.J.; Spoorenberg, S.; Reijneveld, S.A.; de Winter, A.F.; Lippke, S.; Jansen, C.J.M. Using photo stories to support doctor-patient communication: Evaluating a communicative health literacy intervention for older adults. Int. J. Environ. Res. Public Health 2019, 16, 3726. [Google Scholar] [CrossRef] [Green Version]
- Moyer-Gusé, E.; Jain, P.; Chung, A.H. Reinforcement or reactance? Examining the effect of an explicit persuasive appeal following an entertainment-education narrative. J. Commun. 2012, 62, 1010–1027. [Google Scholar] [CrossRef]
- Murphy, J.P.; Moolla, A.; Kgowedi, S.; Mongwenyana, C.; Mngadi, S.; Ngcobo, N.; Miot, J.; Evans, D.; Pascoe, S. Community health worker models in South Africa: A qualitative study on policy implementation of the 2018/19 revised framework. Health Policy Plan. 2020, 36, 1–13. [Google Scholar] [CrossRef]
- Morgan, G.B.; Renbarger, R.L. Posttest-only control group design. In The Sage Encyclopedia of Educational Research, Measurement, and Evaluation; Frey, B.B., Ed.; Sage Publications Inc.: Thousand Oaks, CA, USA, 2018; Research Designs; pp. 1–5. [Google Scholar]
- Chew, L.D.; Bradley, K.A.; Boyko, E.J. Brief questions to identify patients with inadequate health literacy. Fam. Med. 2004, 26, 588–594. [Google Scholar]
- Chew, L.D.; Griffin, J.M.; Partin, M.R.; Noorbaloochi, S.; Grill, J.P.; Snyder, A.; Bradley, K.A.; Nugent, S.M.; Baines, A.D.; Vanryn, M. Validation of screening questions for limited health literacy in a large VA outpatient population. J. Gen. Intern. Med. 2008, 23, 561–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubinga, E.; Maes, A.; Jansen, C. How peer conversations about HIV/AIDS media messages affect comprehension and beliefs of young South African women. SAHARA J J. Soc. Asp. HIV/AIDS 2016, 13, 68–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, Y. Social diffusion of campaign effects: Campaign-generated interpersonal communication as a mediator of anti-tobacco campaign effects. Commun. Res. 2012, 39, 120–141. [Google Scholar] [CrossRef]
- Hendriks, H.; van den Putte, B.; de Bruijn, G. Changing the conversation: The influence of emotions of conversation valence and alcohol consumption. Prev. Sci. 2014, 15, 684–693. [Google Scholar] [CrossRef]
- Chatterjee, J.S.; Bhanot, A.; Frank, L.B.; Murphy, S.T.; Power, G. The importance of interpersonal discussion and self-efficacy in knowledge, attitude and practice models. Int. J. Commun. 2009, 3, 607–634. [Google Scholar]
- Van den Putte, B.; Yzer, M.; Southwell, B.G.; de Bruijn, G.; Willemsen, M.C. Interpersonal communication as an indirect pathway for the effect of antismoking media content on smoking cessation. J. Health Commun. 2011, 16, 470–485. [Google Scholar] [CrossRef]
- Jeong, M.; Bae, R.E. The effect of campaign-generated interpersonal communication on campaign-targeted health outcomes: A meta-analysis. Health Commun. 2017, 33, 988–1003. [Google Scholar] [CrossRef]
- Witte, K.; Cameron, K.A.; McKeon, J.K.; Berkowitz, J.M. Predicting risk behaviors: Development and validation of a diagnostic scale. J. Health Commun. 1996, 1, 317–341. [Google Scholar] [CrossRef]
- Witte, K.; Meyer, G.; Martell, D. Effective Health Risk Messages: A Step-by-Step Guide; Sage Publications Inc.: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Ajzen, I. Theory of Planned Behaviour Questionnaire. Measurement Instrument Database for the Social Sciences. Available online: http://www.midss.org/content/theory-planned-behaviour-questionnaire (accessed on 15 May 2021).
- McMillan, B.; Conner, M. Applying an extended version of the theory of planned behavior to illicit drug use among students. J. Appl. Soc. Psychol. 2003, 33, 1662–1683. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using SPSS, 3rd ed.; Sage Publications Ltd.: London, UK, 2009. [Google Scholar]
- McGuire, W.J. McGuire’s classic input-output framework for constructing persuasive messages. In Public Communication Campaigns, 4th ed.; Rice, R.E., Atkin, C.K., Eds.; Sage Publications Inc.: Thousand Oaks, CA, USA, 2012; pp. 136–146. [Google Scholar]
- Moyer-Gusé, E. Toward a theory of entertainment persuasion: Explaining the persuasive effects of entertainment-education messages. Commun. Theory 2008, 18, 407–425. [Google Scholar] [CrossRef]
- Moyer-Gusé, E.; Dale, K. Narrative persuasion theories. In The International Encyclopedia of Media Effects; Rössler, P., Hoffner, C.A., van Zoonen, L., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2017; pp. 1345–1355. [Google Scholar]
- Ooms, J.; Hoeks, J.; Jansen, C. Hey, that could be me: The role of similarity in narrative persuasion. PLoS ONE 2019, 14, e0215359. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Fotonovela with Q&A Section | Fotonovela without Q&A Section | Existing Brochure | Control Condition | Total | |
|---|---|---|---|---|---|
| (n = 99) | (n = 82) | (n = 94) | (n = 97) | (n = 372) | |
| Gender | |||||
| Male | n = 31 | n = 38 | n = 30 | n = 42 | n = 141 |
| Female | n = 66 | n = 40 | n = 60 | n = 49 | n = 215 |
| Missing values | (n = 2) | (n = 4) | (n = 4) | (n = 6) | (n = 16) |
| Place of residence | |||||
| Ceres | n = 7 | n = 0 | n = 2 | n = 0 | n = 9 |
| Swellendam | n = 16 | n = 9 | n = 13 | n = 22 | n = 60 |
| Malmesbury | n = 8 | n = 11 | n = 13 | n = 8 | n = 40 |
| Calvinia | n = 68 | n = 62 | n = 56 | n = 67 | n = 263 |
| Level of education | |||||
| Low (still at school; left school before Grade 10, 11, or 12) | n = 78 | n = 59 | n = 60 | n = 70 | n = 267 |
| High (high school diploma or degree after high school) | n = 10 | n = 13 | n = 24 | n = 17 | n = 64 |
| Missing values | (n = 11) | (n = 10) | (n = 10) | (n = 10) | (n = 41) |
| Age Group | |||||
| 19 or younger | n = 51 | n = 53 | n = 50 | n = 58 | n = 212 |
| 20–34 years | n = 29 | n = 19 | n = 22 | n = 26 | n = 96 |
| 35 years or older | n = 17 | n = 6 | n = 17 | n = 9 | n = 49 |
| Missing values | (n = 2) | (n = 4) | (n = 5) | (n = 4) | (n = 15) |
| Fotonovela with Q&A Section | Fotonovela without Q&A Section | Existing Brochure | Control Condition | Total | |
|---|---|---|---|---|---|
| (n = 99) | (n = 82) | (n = 94) | (n = 97) | (n = 372) | |
| Level of health literacy | |||||
| Low | n = 40 | n = 38 | n = 33 | n = 48 | n = 159 |
| High | n = 58 | n = 43 | n = 58 | n = 49 | n = 208 |
| Missing values | (n = 1) | (n = 1) | (n = 3) | (n = 0) | (n = 5) |
| Total | |
|---|---|
| (n = 75) | |
| Gender | |
| Male | n = 3 |
| Female | n = 71 |
| Missing values | (n = 1) |
| Place of residence | |
| Ceres | n = 49 |
| Prince Alfred Hamlet | n = 26 |
| Level of education | |
| Low (still at school; left school before Grade 10, 11, or 12) | n = 27 |
| High (high school diploma or degree after high school) | n = 45 |
| Missing values | (n = 3) |
| Age Groups | |
| 19 or younger | n = 0 |
| 20–34 years | n = 25 |
| 35 years and older | n = 49 |
| Missing values | (n = 1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davis, B.; Jansen, C.J.M. Deploying a Fotonovela to Combat Methamphetamine Abuse among South Africans with Varying Levels of Health Literacy. Int. J. Environ. Res. Public Health 2021, 18, 6334. https://doi.org/10.3390/ijerph18126334
Davis B, Jansen CJM. Deploying a Fotonovela to Combat Methamphetamine Abuse among South Africans with Varying Levels of Health Literacy. International Journal of Environmental Research and Public Health. 2021; 18(12):6334. https://doi.org/10.3390/ijerph18126334
Chicago/Turabian StyleDavis, Burt, and Carel J. M. Jansen. 2021. "Deploying a Fotonovela to Combat Methamphetamine Abuse among South Africans with Varying Levels of Health Literacy" International Journal of Environmental Research and Public Health 18, no. 12: 6334. https://doi.org/10.3390/ijerph18126334