Article Text

Abstract
Objective To evaluate the accuracy of neonatal MRI and general movements assessment (GMA) in predicting neurodevelopmental outcomes in infants with hypoxic-ischaemic encephalopathy (HIE).
Design Secondary analyses of a randomised controlled trial (RCT).
Setting Tertiary neonatal intensive care unit in India.
Methods Fifty infants with HIE were included in an RCT of therapeutic hypothermia (25 cooled and 25 non-cooled). All infants underwent brain MRI at day 5, GMA at 10–15 weeks and outcome assessments including Bayley Scales of Infant and Toddler Development, third edition, at 18 months. Associations between patterns of brain injury, presence/absence of fidgety movements (FMs) and outcomes were assessed.
Results Seventeen of 47 (36%) had adverse outcome (5 (21%) cooled vs 12 (52%) non-cooled, p=0.025). Eight infants died (four before an MRI, another three before GMA). Two developed severe cerebral palsy and seven had Bayley-III motor/cognitive composite score <85. Twelve (26%) had moderately/severely abnormal MRI and nine (23%) had absent FMs. The positive predictive value (95% CI) of an adverse outcome was 89% (53% to 98%) for moderate/severe basal ganglia and thalami (BGT) injury, 83% (56% to 95%) for absent/equivocal signal in the posterior limb of the internal capsule (PLIC) and 67% (38% to 87%) for absent FMs. Negative predictive values (95% CI) were 85% (74% to 92%) for normal/mild BGT injury, 90% (78% to 96%) for normal PLIC and 86% (74% to 93%) for present FMs.
Conclusion(s) Neonatal MRI and GMA predicted outcomes with high accuracy in infants with HIE. The GMA is a feasible low-cost method which can be used alone or complementary to MRI in low-resource settings to prognosticate and direct follow-up.
Trial registration number CTRI/2013/05/003693.
- neonatology
- neurology
- neuropathology
Data availability statement
Data are available on reasonable request. Anonymised data (including data dictionaries) will be made available on request to researchers who provide a methodologically sound proposal for use in achieving the goals of the approved proposal.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
The main burden of hypoxic-ischaemic encephalopathy is in low-income and middle-income countries, and many infants die or survive with disability.
Neonatal MRI and general movements assessment are recommended assessments to predict cerebral palsy in infants at risk of perinatal brain injury.
The literature on outcome and outcome prediction after hypoxic-ischaemic encephalopathy in low-income and middle-income countries is sparse.
What this study adds?
This study from South India showed similar patterns of brain injury in infants with hypoxic-ischaemic encephalopathy as trials from high-income countries.
Both neonatal MRI and general movements assessment predicted neurodevelopmental outcome with high accuracy.
Assessment of fidgety movements is a feasible low-cost method to prognosticate and direct follow-up in low-resource settings.
Introduction
Perinatal asphyxia is ranked among the top 20 causes of death at any age globally.1 The main burden of disease is in low-income and middle-income countries (LMICs), where the incidence of hypoxic-ischaemic encephalopathy (HIE) is 10–20 times higher than in high-income countries (HICs).2 3 Therapeutic hypothermia (TH) has been found to reduce mortality and major disability in survivors by 25% (relative risk) with a number needed to treat of 7.4 The therapeutic hypothermia in India (THIN) study showed a neuroprotective effect of TH on early MRI biomarkers,5 but data on neurodevelopmental outcomes in LMICs are scarce.
Outcomes after HIE range from full recovery to death or survival with different degrees of disability.6 7 The prevalence and distribution of outcomes may differ between settings, and factors like maternal morbidities, nutritional status and infections may influence both the pattern of brain injury and the effect of cooling in infants with HIE.8–12 A study from South India reported more white matter (WM) injury in HIE infants as compared with studies from HICs.13
Prediction of outcomes in infants with HIE is essential for affected families, and important for clinicians to direct resources for follow-up. Neonatal MRI and the observation of spontaneous movements using the general movements assessment (GMA) are recommended tools to predict cerebral palsy (CP) in high-risk infants.14 Abnormal signal intensity in the basal ganglia and thalami (BGT) on MRI, which is the typical injury pattern after an acute hypoxic-ischaemic insult, is strongly associated with later motor impairment.15 On the other hand, predominant WM injury, carries a lower risk of motor impairment, but is more related to cognitive and behavioural impairments.16 Absence of fidgety movements (FMs) on GMA between 9 and 20 weeks post-term age is a strong marker for later CP.17 18 In LMICs where resources are limited and MRI not easily available, GMA could be an ideal cost-effective predictive tool. However, most studies on GMA have been done in HICs and mainly in preterm populations.
The aim of this substudy is to evaluate the ability of early MR biomarkers and presence or absence of FMs to predict neurodevelopmental outcomes in infants with HIE included in a randomised controlled trial (RCT) on TH in India.
Methods
Study population
This is a substudy of the THIN-study, a single-centre RCT of infants admitted with HIE to the neonatal intensive care unit (NICU) at the Christian Medical College Vellore, a tertiary care teaching hospital in rural south India. Approximately 15 000 babies are born at the hospital annually. The NICU has 75 beds and is a referral unit for a population of approximately 6 million. The unit offers level 3 neonatal intensive care including high-frequency oscillatory ventilation, inhaled nitric oxide and surgery. Fifty infants at or near term admitted before 5 hours after birth with signs of moderate/severe HIE were recruited between September 2013 and October 2015. The infants were randomly assigned to hypothermia with target core temperature 33.5°C±0.5°C for 72 hours induced by a phase changing material-based cooling device (MiraCradle Neonate Cooler, Pluss Advanced Technologies, India) or standard care with normothermia. Full description of the trial is published.5 Written parental consent was obtained after giving the parents an information leaflet and oral explanation.
Early assessments
All infants underwent cerebral MRI at 5±1 days of age with a 3.0 T Philips Achieva scanner (Philips Healthcare, Best, The Netherlands; software V.3.2.3.1) using a standard protocol.5 The clinical images were reviewed by one neonatologist (MM-B) with experience in neonatal neuroimaging and scored in accordance with Rutherford et al.19 Images were classified as normal/mildly abnormal (BGT score normal or mild and/or WM score normal, mild or moderate) or moderately/severely abnormal (moderate/severe BGT score and/or absent posterior limb of the internal capsule (PLIC), and/or severe WM score).19 Images were also categorised in seven patterns of brain injury: normal (no signs of abnormalities), only mildly/moderately abnormal WM, only severely abnormal WM, mildly abnormal BGT with normal or mildly/moderately abnormal WM, mildly abnormal BGT with severely abnormal WM, moderately abnormal BGT with any WM score and global brain injury (severely abnormal BGT, WM and cortex with absent PLIC and brainstem abnormalities).
At 10 to 15 weeks post-term age, a video for GMA was recorded using a standardised set-up with a digital camera (Sanyo VPC-HD2000, SANYO Electric, Osaka, Japan). The infants were filmed once in active wakefulness laying on a mattress in supine position. The video was analysed independently by two certified GMA observers in accordance with Prechtl's method.18 FMs were classified in accordance with their temporal organisation as continuous, intermittent or sporadic based on their presence and interspersed pauses.20 The category exaggerated was used if the FMs were exaggerated in speed and amplitude. FMs were defined as ‘absent’ if they were not observed, and ‘present’ if present in a continuous, intermittent, sporadic or exaggerated pattern. If disagreement occurred, the observers reassessed the video and reached consensus.
Neurodevelopmental outcome
At 18 months, an experienced developmental paediatrician and a clinical psychologist performed a complete neurological examination, the Bayley Scales of Infant and Toddler Development, third edition (Bayley-III),21 and clinical assessment of vision and hearing. CP and CP subtype were diagnosed in accordance with Surveillance of Cerebral Palsy in Europe22 and gross motor function was classified using the Gross Motor Function Classification System (GMFCS).23 Adverse outcome was defined as a Bayley-III cognitive and/or motor composite score (CS) <85 (−1 SD),24 25 a diagnosis of CP GMFCS level 3–5, impaired sensory/communication outcomes (blindness or deafness), ongoing seizure disorder or death related to associated causes. The Bayley-III language CS was not used in the analysis due to the infants’ young age and the subjectivity of their non-English application. One infant had a normal Griffith Mental Development Scales (GMDS) assessment at 48 months and was assigned a Bayley motor and cognitive CS of 105 and 107, respectively, due to higher scores found in testing of typically developing children.26 27 Another infant’s outcome was based on phone assessment and classified as normal in the binary analysis of outcome. All assessors of MRI, GMA and outcomes were blinded to the intervention and the results of former examinations.
Statistics
Data were analysed using SPSS V.25 (IBM, Chicago, Illinois, USA). Clinical characteristics and outcomes were summarised with absolute numbers (percentages) for categorical variables and means (SD) or medians (IQR) for continuous variables. Group differences in outcomes were analysed by χ2 tests, Fisher’s exact tests, linear-by-linear associations, Student’s t-tests or Mann-Whitney U tests, as appropriate. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and the predictive accuracy for adverse outcome were calculated for moderately/severely abnormal MRI, moderate/severe BGT injury, absent PLIC, combined absent and equivocal PLIC, absent FMs and combined absent and sporadic FMs. The CIs for the predictive values were calculated using a free online statistical calculator from MedCalc (MedCalc Software, Ostend, Belgium).28 There were no corrections made for multiple comparisons. Differences with p values <0.05 were considered statistically significant.
Results
Fifty neonates were recruited, 25 in the cooled and 25 in the non-cooled group (figure 1). Demographics, neonatal characteristics and outcomes according to treatment group are shown in online supplemental eTable 1 and 2. Forty-six infants who survived until day 4 underwent MRI at a median age of 5 days (range 4–7), and 12 (26%) of these had moderately/severely abnormal MRI (table 1). The most frequent pattern of brain injury was mildly abnormal BGT with normal or mildly/moderately abnormal WM (online supplemental eTable 1). A video recording for GMA was obtained in 39 infants at a median post-term age of 12 weeks (range 8–16), and 9 (23%) infants had absent FMs. Two came for GMA before 10 weeks, and both had intermittent FMs. Assessment of outcome using Bayley-III was available in 37 infants at a median age of 18 months (range 16–21), and another infant had Bayley-III score estimated based on a normal assessment with GMDS. Three infants were lost to follow-up (one with completely normal MRI, one with moderate WM injury and present FMs and one with moderate BGT and severe WM injury).
Supplemental material
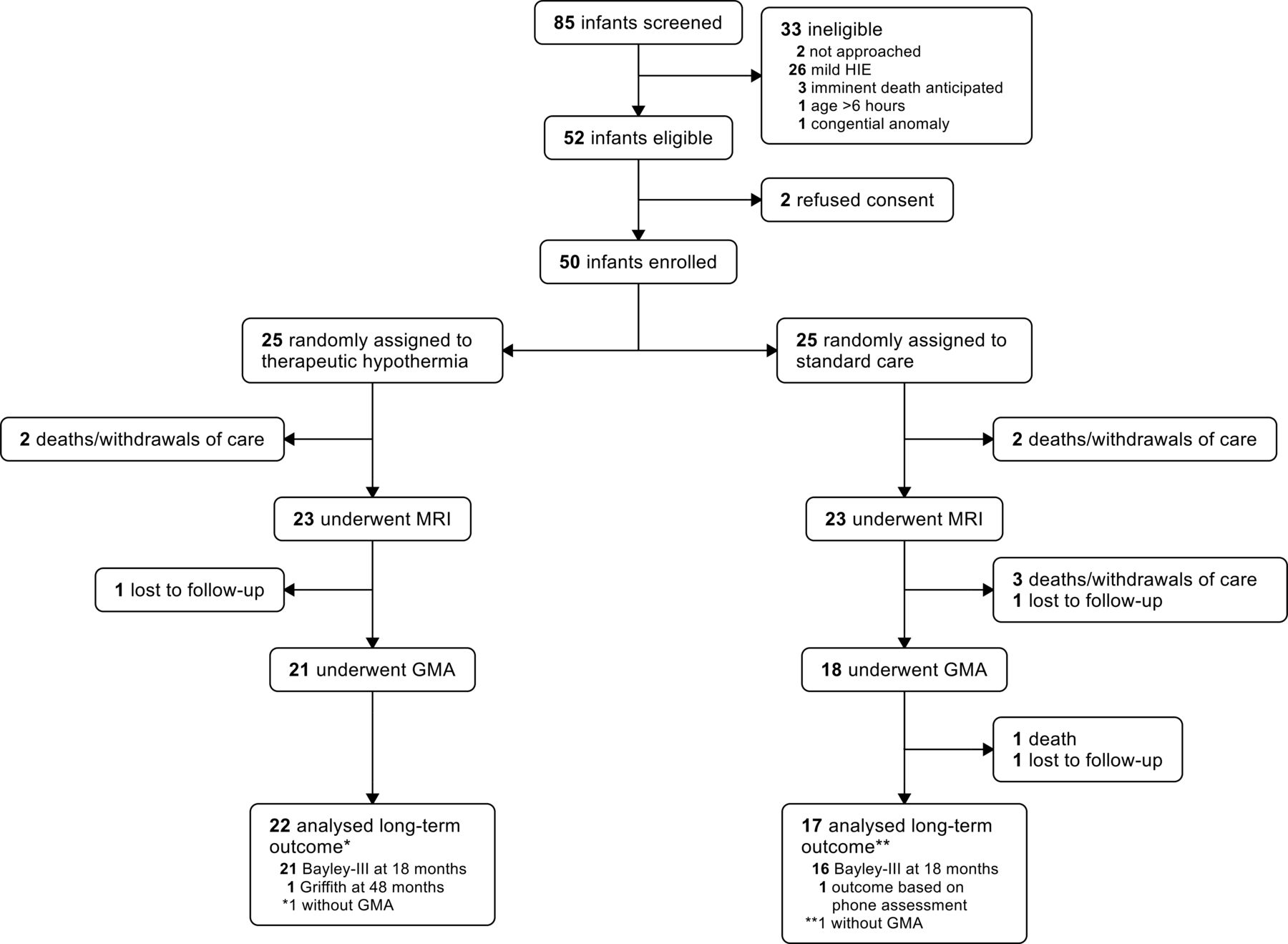
Trial profile. Bayley-III, Bayley Scales of Infant and Toddler Development (third edition); GMA, general movements assessment; Griffith, Griffith Mental Development Scales; HIE, hypoxic-ischaemic encephalopathy.
Outcomes according to neonatal MRI*
Seventeen of 47 (36%) infants with available follow-up data had adverse outcome, 5 cooled and 12 non-cooled (21% vs 52%, p=0.025). Eight infants died of reasons related to HIE, seven in the neonatal period and one at 12 months. The nine survivors with adverse outcomes included two with CP GMFCS level 5 (both had Bayley-III scores <70), and seven who had a Bayley-III motor and/or cognitive CS <85 (one with bilateral hearing loss, and one with CP GMFCS level 1 and Bayley-III scores <70).
Prediction of outcome
MRI and outcome
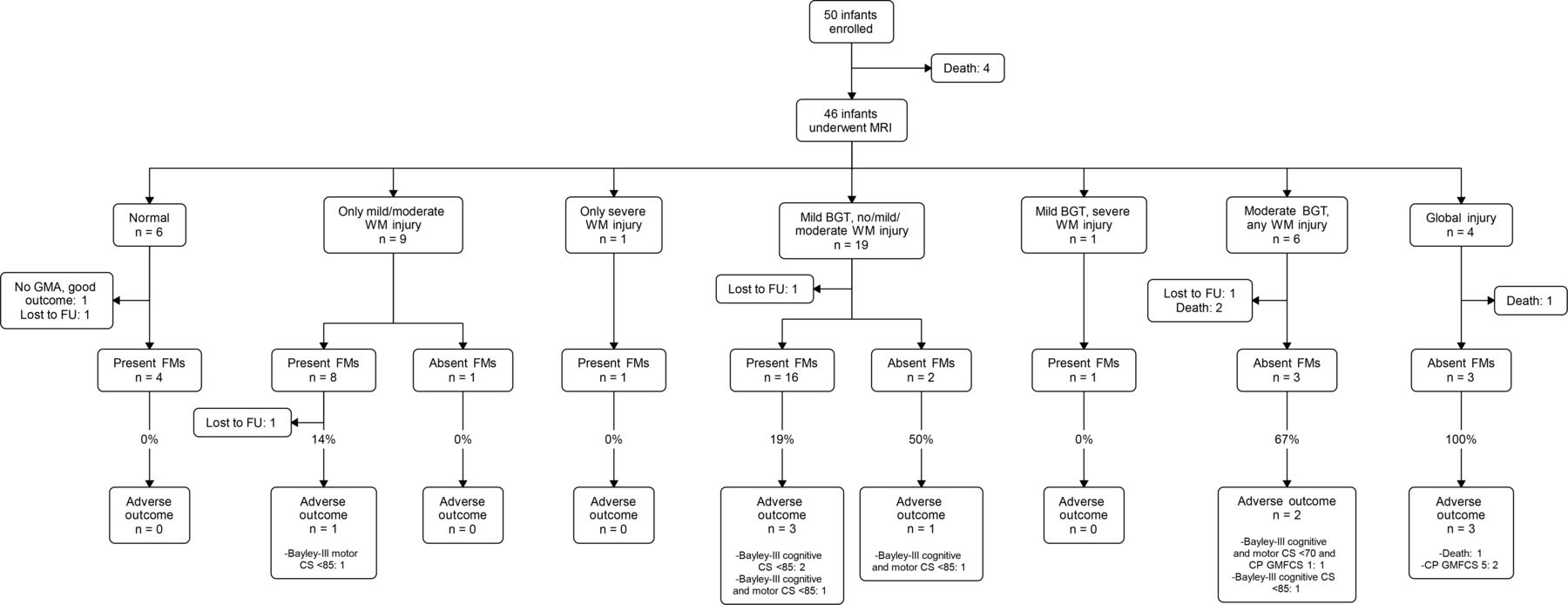
Adverse outcome was significantly more common among infants with moderately/severely abnormal than normal/mildly abnormal MRI (8 of 11 and 5 of 32, respectively; p<0.001, table 1). The eight infants with moderately/severely abnormal MRI and adverse outcome had either a global brain injury pattern or moderate BGT injury with absent or equivocal PLIC (figure 2). All five infants with normal/mildly abnormal MRI and adverse outcome had either mild BGT injury with normal or equivocal PLIC and/or moderate WM injury (online supplemental eTable 3).
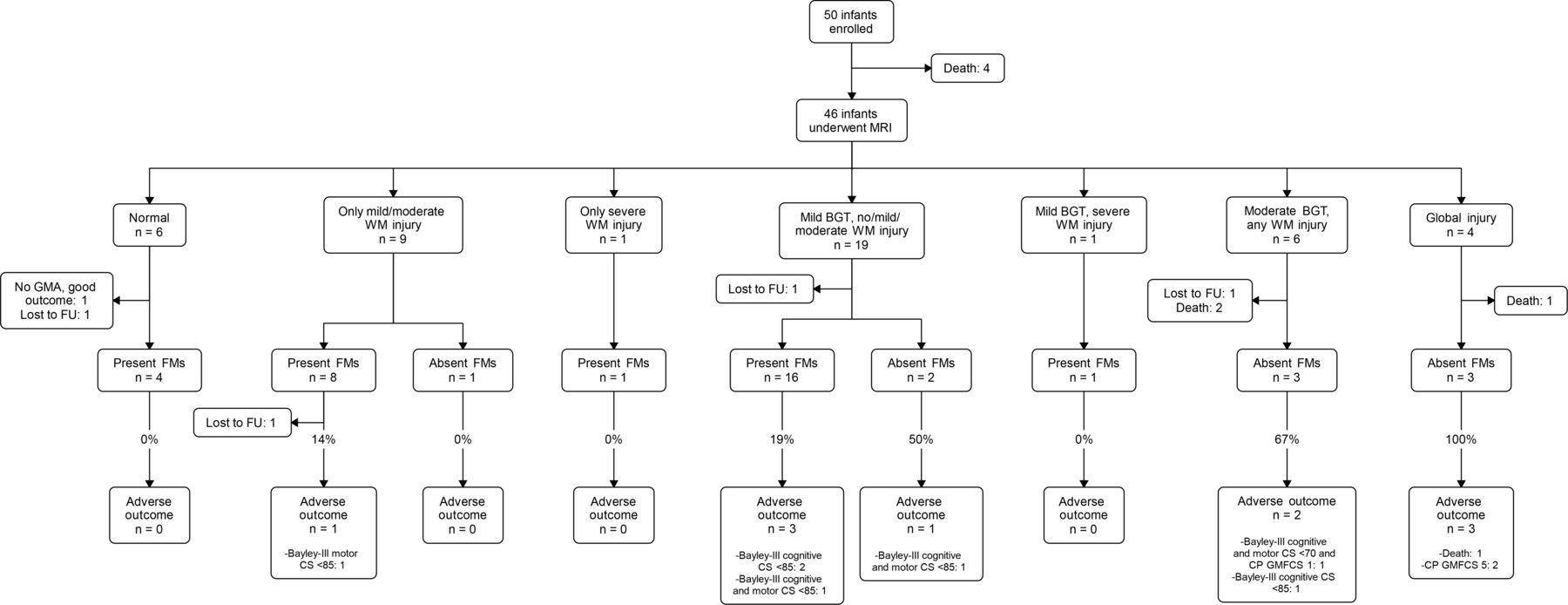
Flow chart showing patterns of brain injury, present or absent fidgety movements (FMs) and outcomes. BGT, basal ganglia and thalami; CP, cerebral palsy; CS, composite score; FU, follow-up; GMA, general movements assessment; GMFCS, Gross Motor Function Classification System; WM, white matter.
Bayley-III cognitive CS was significantly lower in infants with moderately/severely abnormal MRI compared with those with normal/mildly abnormal MRI (median (IQR) 80 (55–100) vs 95 (90–105), respectively, p=0.030). Infants with moderately/severely abnormal MRI also had lower Bayley-III motor CS than infants with normal/mildly abnormal MRI, but this difference was not significant (median (IQR) 100 (46–115) vs 107 (91–112), p=0.335). The Bayley-III cognitive and motor CS according to injury patterns on MRI are shown in figure 3.

Bayley-III cognitive (A) and motor (B) composite score (median, first and third quartile and range) according to injury pattern on neonatal MRI. Bayley-III, Bayley Scales of Infant and Toddler Development, third edition; WM, white matter; BGT, basal ganglia and thalami.
GMA and outcome
Six of nine (67%) infants with absent FMs had adverse outcome: one died, two developed severe CP and three had Bayley-III motor and/or cognitive CS <85. The remaining three infants with absent FMs had normal outcome. Most infants with present FMs (25 of 29) had normal outcome, and the four with adverse outcome all had Bayley-III motor and/cognitive CS 70–85 and none of them developed CP. Ten (26%) infants had sporadic FMs, of whom one had adverse outcome (Bayley-III cognitive CS <85).
Infants with present FMs had significantly higher Bayley-III cognitive CS than those with absent FMs (median (IQR) 100 (91–105) vs 80 (58–94), respectively, p=0.001). The Bayley-III motor CS was also higher, although not significant, in infants with present versus absent FMs (median (IQR) 107 (94–112) vs 85 (51–110), p=0.091). The Bayley-III cognitive and motor CS for the different temporal classifications of FMs are shown in figure 4.

Bayley-III cognitive (A) and motor (B) composite score (median, first and third quartile and range) according to temporal organisation of fidgety movements (FMs) on general movements assessment. One infant with exaggerated FMs is not included in the box plot but had Bayley-III cognitive and motor composite score of 95 and 85, respectively. Bayley-III, Bayley Scales of Infant and Toddler Development, third edition.
MRI, GMA and outcome
Different patterns of brain injury in relation to GMA and outcome are shown in figure 2. All infants with a completely normal MRI and available follow-up assessments had present FMs and favourable outcome. One infant with mild BGT and WM injury had exaggerated FMs and was diagnosed with CP GMFCS level 1 (normal Bayley-III scores). All six infants with moderate BGT injury or global brain injury who came for GMA had absent FMs, and five of them had an adverse outcome (figure 2). All six infants with absent PLIC either died or survived with severe CP (figure 5). Sensitivity, specificity, PPV, NPV and accuracy of MRI and GMA for adverse outcomes are shown in table 2.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Flow chart showing involvement of posterior limb of internal capsule (PLIC), present or absent fidgety movements (FMs) and outcomes. CS, composite score; CP, cerebral palsy; FU, follow-up; GMA, general movements assessment; GMFCS, Gross Motor Function Classification System.
Predictive ability of MRI abnormalities and general movements assessment for adverse outcome*
Four infants had either moderately/severely abnormal MRI or absent FMs, and a normal outcome (online supplemental etable4). Two had severe WM injury as predominant injury pattern, and the other two had absent FMs but a normal/mildly abnormal MRI. In addition, one cooled infant with both moderate BGT injury, equivocal PLIC and absent FMs had a normal outcome.
Discussion
This substudy of an RCT on TH for HIE in a low-resource setting found that both neonatal MRI and GMA are closely associated with the combined outcome of death and adverse neurodevelopment at 18 months. The patterns of brain injury, with the majority of infants having BGT injury with or without WM injury, is similar to studies from high-income settings.19 29 30 Normal/Mildly abnormal BGT, normal PLIC and present FMs were all highly predictive of a normal outcome in this study. The GMA at 10–15 weeks post-term age may be an alternative predictive tool in settings where MRI is not available.
The BGT injuries in our study were mainly mild. Severe BGT injury was less common compared with the National Institute of Child Health and Human Development (NICHD) trial and the Total Body Hypothermia (TOBY) trial,19 30 and this is most likely due to the low proportion of infants with severe HIE in our study. We found a similar distribution of WM injury to the TOBY trial.19 Another Indian HIE trial reported predominantly WM injury and more than half of infants with moderate/severe HIE had normal BGT.13 WM injury is generally thought to be caused by more prolonged asphyxia or other causes of neonatal encephalopathy.16 Patterns of brain injury in HIE infants in different low-resource settings should be further explored.
Our results confirmed a close association between early spontaneous movements and neurodevelopmental outcome. Normal FMs at 2–3 months post-term age is a well-known predictor of a normal motor outcome.17 31 The association between FMs and cognitive outcome found in this study has also been reported by others.32 33 A normal outcome in 9 of 10 infants with sporadic FMs is in accordance with a large multicentre study where only 8% of infants with sporadic FMs developed CP.34
Moderate/Severe BGT abnormalities, equivocal/absent PLIC and absent FMs had the highest predictive accuracy for adverse outcome in this study. Ferrari et al found that the site and severity of brain injury on neonatal MRI and the results of GMA are closely correlated and has comparable accuracy in predicting motor outcome in non-cooled HIE infants.35 Similar predictive accuracy of MRI has been found in substudies of both the TOBY trial and the Infant Cooling Evaluation (ICE) trial.19 36 Lally et al,13 however, reported low sensitivity, but high specificity of MRI abnormalities in their study from South India, but only a small proportion of infants in that study had BGT injury.
In low-resource settings, MRI is often unavailable and expensive, while smartphones and internet access are cheap and available even in remote areas.37 A video recording for GMA can easily be performed using a simple video camera or even a smartphone. GMA is both time-efficient and cost-efficient and could be evaluated by remote assessment, which is especially important for LMICs. We suggest that in low-resource settings GMA is a good supplement, or even an alternative, to MRI to direct interventions and further follow-up in babies with HIE.
Although this study was not powered to detect differences in neurodevelopmental outcome between treatment groups, we found a reduction in adverse outcomes in cooled infants. Together with our previous report on reduction in several MRI biomarkers, we therefore state that TH for moderate HIE is feasible and may be neuroprotective in a low-resource setting.5 However, implementation of TH in LMICs should be limited to tertiary NICUs and requires development of guidelines and training programmes.
Limitations of this study include a small sample size and short duration of follow-up. This applies in particular to infants with severe WM injury and normal outcome, who are at risk of later cognitive/behavioural disabilities.38 However, we had good follow-up rate. Another limitation is the low proportion of infants with severe HIE, which is most likely due to selection bias.
Conclusion
In conclusion, we report that both neonatal MRI and GMA are strongly associated with neurodevelopmental outcome at 18 months in infants with HIE admitted to a tertiary care NICU in South India. GMA at 10–15 weeks post-term age has similar predictive accuracy as neonatal MRI and is therefore a feasible low-cost predictive tool in low-resource settings. The patterns of brain injury and incidence of adverse outcomes should be further explored in these settings.
Data availability statement
Data are available on reasonable request. Anonymised data (including data dictionaries) will be made available on request to researchers who provide a methodologically sound proposal for use in achieving the goals of the approved proposal.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Institutional Review Board at the Christian Medical College (number 2013/8223) and the Regional Committee for Medical and Health Research Ethics in central Norway (number 2013/2167).
Acknowledgments
The authors thank all the staff of the Department of Neonatology, the Christian Medical College (CMC), Vellore who took care of the study babies, and the research officers for adequate recruitment and collection of clinical data. The authors thank Live Eikenes (Department of Circulation and Medical Imaging, Norwegian University of Science and Technology (NTNU)) and Asta Håberg (Department of Neuromedicine and Movement Science, NTNU and Department of Radiology and Nuclear Medicine, St. Olavs Hospital, Trondheim University Hospital) for contribution in making the MRI protocol. The authors thank Toril Larsson Fjørtoft (Clinic of Clinical Services, St. Olavs Hospital, Trondheim University Hospital and Institute of Clinical and Molecular Medicine, NTNU) for participation in GMA analysis. The authors thank Associate Professor in Statistics Turid Follestad (Clinical Research Unit Central Norway, NTNU) for statistical counselling. The authors also thank members of the Data Safety Monitoring Board at the CMC for monitoring the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors NT was study PI. KA performed the literature search, conceptualised and designed the study, wrote the manuscript, performed the data analysis and data interpretation and reviewed and revised the manuscript. NT did the literature search, conceptualised and designed the study, enrolled patients, collected clinical data, was involved in data analysis and data interpretation and reviewed and revised the manuscript. LA did the GMA analysis, was involved in data analysis and data interpretation and reviewed and revised the manuscript. MM-B did the MRI analysis, was involved in data analysis and data interpretation and reviewed and revised the manuscript. IN made the MRI protocol, implemented and adapted the protocol on the local scanner and reviewed and revised the manuscript. BK and CSP did the outcome assessments, and reviewed and revised the manuscript. RS did the literature search, conceptualised and designed the study, was involved in data analysis and data interpretation and reviewed and revised the manuscript.
Funding The trial was funded by the Liaison Committee for Education, Research and Innovation in Central Norway, and the Joint Research Committee between St. Olavs Hospital, Trondheim University Hospital, and the Faculty of Medicine, NTNU, Trondheim, Norway.
Disclaimer The funders/sponsors had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript or decision to submit the manuscript for publication.
Competing interests NT has a patent 1796/DEL/2013 Life cradle device for inducing neonatal hypothermia issued.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.