Article Text

Abstract
Objective To evaluate whether 1% aqueous chlorhexidine gluconate (CHG) when compared with 2% aqueous chlorhexidine gluconate is non-inferior for neonatal skin antisepsis.
Design Parallel, blinded, non-inferiority randomised trial.
Setting Level III, academic, neonatal intensive care unit.
Patients Infants born at 260/7 to 426/7 weeks of gestation from June 2019 to December 2019.
Interventions Participants were randomised to skin antisepsis by either 1% aqueous CHG or 2% aqueous CHG.
Main outcome measures The primary outcome was the proportion of negative skin swab cultures after skin antisepsis. Secondary outcomes were local skin reactions at 0, 6, 12 and 24 hours and plasma chlorhexidine levels in a subset of the study population.
Results A total of 308 neonates with a median gestation age of 34 (31–37) weeks and mean birth weight of 2029 g were randomised on 685 occasions (1% CHG: n=341; 2% CHG: n=344). 93.0% of the post-antisepsis skin swabs were sterile in 1% CHG group compared with 95.6% of the swabs in the 2% CHG group (risk difference −2.7%, 95% CI −6.2% to +0.8%). The lower bound of 95% CI crossed the pre-specified absolute non-inferiority limit of 5%. Neonates developed mild dermatitis on 16 (2.3%) occasions. There was no significant difference in median plasma CHG levels in the two groups, 19.6 (12.5–36.4) and 12.6 (8.7–26.6) ng/mL, respectively.
Conclusions Application of 1% aqueous CHG was not shown to be non-inferior to 2% chlorhexidine aqueous for skin antisepsis in neonates. There were no severe skin-related adverse events in either of the two groups.
Trial registration number CTRI/2019/06/019822; (http://ctri.nic.in/Clinicaltrials/pmaindet2.php?trialid=33453&EncHid=&userName=CTRI/2019/06/019822)
- neonatology
- microbiology
- pharmacology
Data availability statement
Data are available on reasonable request. Deidentified individual participant data (including data dictionaries) that underlie the results reported in this article will be made available on publication to researchers who provide a methodologically sound proposal for use in achieving the goals of the approved proposal. Proposals should be submitted to ra.aiims@gmail.com.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Aqueous chlorhexidine (0.5%–2% w/v) is widely used for skin antisepsis in neonates despite its lack of evidence for safety and efficacy.
There is a risk of skin dermatitis and systemic toxicity due to percutaneous absorption of chlorhexidine, which is more with alcohol-based preparations.
What this study adds?
1% aqueous chlorhexidine gluconate (CHG) is not non-inferior to 2% aqueous CHG for skin antisepsis in neonates.
Aqueous chlorhexidine does not cause significant adverse skin reactions in neonates, especially in neonates born at gestational age ≥28 weeks.
There is definite percutaneous absorption of chlorhexidine, the extent of which seems to be similar with either of the two strengths of aqueous preparations.
Introduction
Skin disinfection by an appropriate antiseptic agent is essential to prevent healthcare-associated infection.1 Common pathogens responsible for sepsis have been detected in skin microbiota of hospitalised neonates.2 Such skin inhabitants can cause sepsis3 4 and also lead to blood culture contamination5–7 resulting in unnecessary antibiotic use.8 Strict asepsis bundles have been shown to reduce catheter-related blood stream infection (CRBSI)9 and contamination rates.8 The choice of appropriate skin disinfectant is, however, based on low-quality evidence, even in adults.10
Studies comparing efficacy of skin disinfectants in neonates are heterogenous with respect to their methodology, comparator arms and outcomes assessed (bacterial clearance variably measured by post-antisepsis skin swab cultures,11–13 blood culture contamination,14 incidence of catheter tip colonisation15 16 or CRBSI17 18). Concerns of skin-related adverse reactions and potential thyroid dysfunction have led to the replacement of povidone-iodine with chlorhexidine gluconate (CHG) aqueous and alcoholic forms (0.05% to 2% w/v).11 14 17 However, local skin-related adverse reactions have been reported with the latter in preterm infants.19–21 In addition, there are concerns of systemic absorption and potential neurotoxicity.22 The Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC) do not provide any specific recommendations for use of chlorhexidine in neonates due to lack of evidence demonstrating safety.3 23 Notwithstanding the lack of robust evidence for efficacy of aqueous CHG, especially in a concentration of less than 2% w/v, in neonates, many units have incorporated it as a routine skin antiseptic in the neonatal intensive care unit (NICU).24–27
There may be a higher risk of dermatitis and systemic absorption of chlorhexidine with an alcoholic preparation as compared with aqueous preparation.28–30 Therefore, we compared the efficacy of aqueous chlorhexidine in 1% and 2% concentration in terms of the rates of negative post-antisepsis skin swab cultures in neonates of 26–42 weeks of gestation in a randomised non-inferiority (NI) trial. We chose NI design to balance the anticipated decrease in efficacy11 31 with the plausible reduced adverse skin effects and systemic absorption of chlorhexidine by using a lower strength formulation.
Methods
Study design and setting
This was a parallel-group, blinded, non-inferiority, randomised trial conducted in a level-3 unit in India between June 2019 and December 2019. The institute ethics committee approved the study protocol. Written parental consent was obtained before randomisation.
Participants
We enrolled neonates born at 260/7 to 426/7 weeks of gestation who required admission to NICU for at least 48 hours. Outborn neonates were eligible for enrolment from the first day of admission. Neonates with hydrops, generalised skin disorder, skin infection and requiring high ventilator support as adjudged by the clinical team were excluded. Neonates were eligible for enrolment until 28 days of life.
Randomisation and allocation concealment
Participants were stratified by gestation (260/7–276/7, 280/7–346/7 and 350/7–426/7 weeks) and assigned in a 1:1 ratio to skin disinfection by 1% aqueous CHG or 2% aqueous CHG using separate randomisation schedule for each stratum. An independent investigator prepared the computer-generated randomisation sequence with variable block sizes of 2, 4 and 6 (Sealed Envelope Ltd. 2019). Neonates were eligible for repeat enrolment after 4 days from the last enrolment and were randomised again independent of the prior randomisation group. We chose 96 hours of interval for re-enrolment based on previous data, showing peak plasma levels of CHG at 24 to 48 hours post-exposure.32 Random treatment assignment was written on a small paper and placed in serially numbered opaque sealed envelopes kept in the NICU. The staff nurse opened the envelopes at the time of randomisation.
Intervention
The intervention comprised the application of 1% aqueous CHG for skin antisepsis versus application of 2% aqueous CHG (control arm). Antiseptic application was done independent of any routine clinical procedures. No routine bathing/cleansing of body of neonates with any antiseptic solution was practised in the unit during the study period. The two chlorhexidine solutions were prepared in a sterile facility in the pharmacy of Dr Rajendra Prasad Centre of Ophthalmic Sciences, AIIMS, New Delhi. Both stock solutions were transferred to 500 mL of sterile container air packed with a butyl rubber stopper, covered with aluminium foil to prevent degradation, and stored at 4°C in a refrigerator. This solution remains stable for 1 year under optimal conditions. Samples from both stock solutions were sent monthly for bacterial and fungal culture to check for contamination. The pharmacist estimated the final concentration of prepared chlorhexidine solution for its accuracy.
The primary investigator (PI) identified a 4 cm2 skin area to obtain the pre-antisepsis skin swab from one of the following sites: cubital fossa, dorsum hand or dorsum foot. An alternate site was selected at the time of repeat enrolment. The PI soaked the sterile swab in distilled water and rubbed it five times each in horizontal, vertical and diagonal strokes on the designated area and placed it in 5 mL of brain heart infusion (BHI) broth. The staff nurse opened the randomisation envelopes and dipped the swab stick in the antiseptic solution for 5–10 s in the absence of the PI to ensure blinding. It was then applied to the skin by the PI. After 60 s, the PI took the post-antisepsis skin swab in the same way as before. The labelled pre-antisepsis and post-antisepsis BHI media were sent to the laboratory immediately (online supplemental panel 1). The staff nurse who opened the randomisation envelopes and prepared the swabs for antiseptic application was not involved in the assessment of skin-related adverse events of enrolled neonates.
Supplemental material
Outcomes
The primary outcome was the proportion of negative post-antisepsis skin swab cultures, defined as number of colony-forming units ≤15/mL.12 The secondary outcomes were local skin-related adverse reactions—at 0, 6, 12 and 24 hours post-application by using contact dermatitis severity scoring15, and plasma chlorhexidine concentration. The chlorhexidine levels were estimated in a subset of neonates, sampled only once, either at 6, 12 and 24 hours after application. We intended to obtain 20 samples from each stratum at 24 hours and five samples from each stratum at 6 and 12 hours to help explore the pharmacokinetics of CHG in neonates. We estimated the effect of gestational age and multiplicity of exposures on plasma chlorhexidine levels as a post hoc exploratory analysis.
Outcome assessment
Inoculums (50 µL) from BHI were placed onto the sheep blood agar and McConkey agar media by using a calibrated loop and incubated at 37°C for 18 to 24 hours. Colony count was estimated by semi-quantitative analysis. Identification of the colonising microorganism was made by matrix-assisted laser desorption/ionisation–time of flight mass spectrometry. A microbiologist blinded to the group assignment counterchecked the colony counts.
The on-duty nurse assigned the skin dermatitis severity scoring serially at the defined time points (form used for recording in online supplemental figure 1).15 We collected 0.5–1 mL of blood in EDTA vial and centrifuged at 6000 rpm for 15 min for estimation of plasma CHG. The separated plasma was stored at −80°C until analysis. Previous studies have reported residual skin action until 24 hours and maximum plasma chlorhexidine levels between 24 hours and 7 days after initial exposure to the antiseptic solution. We chose three time points as 6, 12 and 24 hours to explore these serial trends.15 32
High-performance liquid chromatography–mass spectrometry (HPLC-MS/MS) experiments were performed using 4000 Q-TRAP triple quadrupole, tandem mass spectrometer (AB Sciex, Foster City, CA, USA) coupled with ultra-high performance liquid chromatography (UHPLC; Accela Thermo Fisher, Waltham, MA, USA) with autosampler and online vacuum degasser. We used hydrophilic interaction (HILIC)–based separation technique instead of ultraviolet detection to achieve a higher analytical sensitivity. All the parameters of tandem mass spectrometer and UHPLC were controlled by Analyst software, V.1.4.2 (AB Sciex) and Chrom Quest software, V.4.5 (Thermo Fisher, USA), respectively. The process was validated as per US FDA guidelines to ensure within permissible levels of matrix effect.33
Statistical methods
In a prior study from our unit (Kulkarni 2018, unpublished), the incidence of negative post-antisepsis skin swab after skin disinfection by 2% aqueous chlorhexidine was 94%. Assuming that 1% aqueous CHG would have a similar proportion of negative skin swabs, an absolute non-inferiority limit of 5% with a power of 80% and a one-sided type I error size of 0.025, the number of total post-antisepsis skin swabs required in each group was 355.34 We considered an absolute non-inferiority limit of 5% to be clinically meaningful as a previous study observed an efficacy of 90% (95% CI 85% to 97%) after application of 2% chlorhexidine in neonates.12
Statistical analysis was performed with STATA V.14.2 (StataCorp, TX). Normality of the distribution for chlorhexidine concentration was checked by Shapiro-Wilk test and Wilcoxon rank-sum test was employed to analyse skewed data. Categorical variables were compared using the χ2/Fisher’s exact test. All analyses were carried out at 5% level of significance. Test for interaction (Mantel-Haenszel) between the gestation age strata and treatment group for the primary outcome was performed for the subgroup analysis.
Results
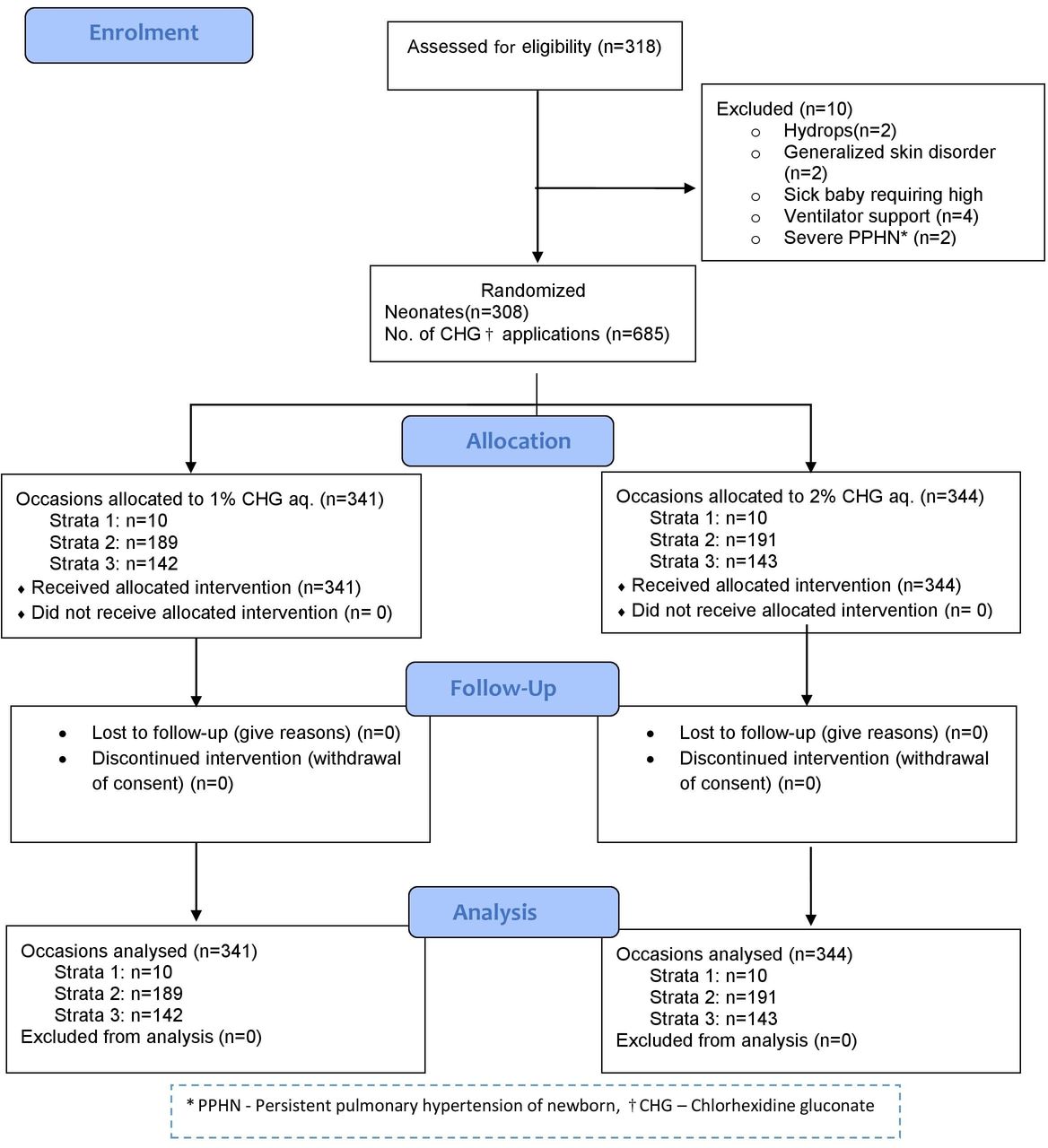
A total of 318 neonates were assessed for eligibility during the study period, of whom 308 were randomised on 685 occasions to skin disinfection by 1% CHG aqueous (n=341) or 2% aqueous CHG (n=344). Neonates on all occasions received the intended intervention (figure 1). The median gestation and the mean birth weight of the neonates at the time of first enrolment in the 1% CHG (n=158) and 2% CHG (n=150) groups were 34 and 35 weeks, and 2018 g and 2029 g, respectively. There were no differences in the perinatal characteristics between groups (table 1). The postnatal characteristics prior to enrolment on all occasions were similar between groups (table 2).

Study flow.
Perinatal characteristics prior to first enrolment
Postnatal characteristics prior to enrolment (all occasions)*
The proportion of negative skin swabs after application of 1% CHG and 2% CHG was 93.0% and 95.6%, respectively (risk difference −2.7%, 95% CI −6.2% to +0.8%). The proportion of negative swabs was significantly lower in the 1% CHG group in the subgroup of neonates born at 280/7–346/7 weeks, but the test for interaction did not reveal a significant interaction (table 3).
Primary outcome, adverse skin reactions and subgroup analysis
The worst skin reaction was slight pink discolouration without oedema just after application of any CHG (a score of 1 out of 4), which did not persist after 6, 12 and 24 hours. The risk was similar in the two groups, 2.3% in each (risk difference +0.02%, 95% CI −2.2% to +2.2%) (table 3).
The plasma chlorhexidine levels were estimated in randomly selected 59 neonates at 6 hours (n=9), 12 hours (n=9) and 24 hours (n=41) (online supplemental table S1). Twenty-four hours after the intervention, the median plasma concentration in 1% CHG group (n=24; 19.6 ng/mL) was similar to 2% CHG (n=17; 12.6 ng/mL) (table 3).
The number of cumulative exposures to chlorhexidine at the time of plasma CHG estimation varied in neonates from one to six (online supplemental table S2). Only one neonate had a plasma sample taken after six exposures (289.3 ng/mL). Among neonates exposed only once to any chlorhexidine before the blood draw, the median levels in neonates at gestation age 280/7–346/7 weeks (n=13) were similar to those born at 350/7–426/7 weeks (n=13) (12.6 (10.7–28.9) vs 17.6 (9.3–33.5)) (online supplemental table S3).
Discussion
In this non-inferiority trial of skin disinfection by 1% aqueous chlorhexidine versus 2% aqueous chlorhexidine, the non-inferiority of 1% CHG could not be established as the lower bound of CI crossed the pre-specified non-inferiority margin of 5% (figure 2). In other words, we were unable to show that 1% CHG was not unacceptably worse than 2% CHG. The skin-related adverse events and the plasma chlorhexidine levels were similar in both groups.

{kind=link}
{kind=link}
Non-inferiority diagram with absolute risk difference of obtaining negative post-antisepsis skin swabs between 1% chlorhexidine aqueous and 2% chlorhexidine aqueous groups. (i) Lower bound of the 95% CI crossed −5%, the pre-specified non-inferiority margin representing 5% lower efficacy for 1% chlorhexidine gluconate (CHG) compared with the control 2% CHG solution, indicating that non-inferiority was not demonstrated. (ii) Because 5% is included within this 95% CI, there still remains a possibility that 1% CHG is non-inferior to 2% CHG (ie, this was an indeterminate trial result). (iii) Because the upper bound of the 95% CI is greater than 0, it is impossible to say from these results whether 1% CHG is inferior to 2% CHG.
The overall efficacy of 2% CHG was 95.6% which is similar to previously reported results, ensuring that constancy assumption for the active control was met in this NI trial.12 35 The efficacy of 1% CHG (93.0%) was slightly lower than that of the 2% CHG, the active control in this study, yet was nevertheless comparable with reported efficacy data for 2% CHG aqueous in literature.12
There are reports of differing rates of efficacy for CHG in neonates, based on blood culture contamination rates,14 CRBSI17 18 or post-antisepsis skin11–13 or catheter colonisation.15 16 This phenomenon may be due to different methods of antiseptic application like spraying, swab stick or by soaking sterile cotton/gauze piece, and due to the varying duration of skin exposure to the disinfectant. There is, however, no consensus on the ideal method of application. A low proportion of negative post-antisepsis skin swabs in the present study after application of 1% CHG indicates a potentially higher risk of microbial translocation from the skin into the bloodstream.
Higher risk of dermatitis in preterm neonates is due to a thin stratum corneum, sparse dermal elastic fibres and a weak dermal–epidermal junction. There were no cases of burns/severe dermatitis in both groups. Garland et al in their pilot study on skin antisepsis reported no adverse skin reactions, but these neonates were more than 7 days old and >1500 g.15 Studies enrolling smaller neonates have noted a higher incidence of dermatitis.36 A recent survey in 124 Canadian neonatal units showed that nearly 68% of the users had experienced severe skin-related adverse events after using chlorhexidine.27 The present study provides reassuring safety data from a large cohort regarding routine use of 1% and 2% aqueous CHG solutions in neonates born after 26 weeks’ gestation.
Chlorhexidine was detectable in plasma of all 59 randomly selected neonates. Since a neonate was eligible for repeat enrolment after every 96 hours, there could be a potentiating effect of multiple exposures to CHG, simulating the real-life scenario wherein a neonate experiences multiple exposure during hospital stay. There were no differences in plasma levels done at 24 hours postexposure between the intervention and the control group. In the post hoc analysis, the median plasma chlorhexidine levels at 24 hours did not differ between the gestational age strata, 280/7–346/7(n=13) and 350/7–426/7(n=13) weeks. The trial, however, was underpowered to detect true difference in plasma chlorhexidine levels. Chapman et al found detectable chlorhexidine level (1.6–206 ng/mL) in 50% of preterm neonates (n=10/20).32 The difference in the extent of absorption after exposure to the same strength of antiseptic in different studies could be due to the effect of mass balance, that is, application mode and amount of CHG transferred from the applicator to the skin. There are currently no studies comparing the mass balance and bioavailability of CHG for different methods of application. In vitro studies have demonstrated damaging effects on odontoblasts, fibroblasts, human epithelial cells as well as neuronal cells.37 38 Only one neonate in the study showed plasma concentration more than 125 ng/mL (suggested in vitro threshold for neurite outgrowth inhibition).22 Further studies are essential to establish a definitive safe threshold of plasma chlorhexidine.
The current study tried to address the issue of appropriate chlorhexidine preparation for pre-procedural skin antisepsis in neonates admitted in the NICU. Adequate sterility is required before intravenous cannulation, insertion of umbilical line, peripherally inserted central catheter and central venous catheters, before lumbar puncture and for obtaining samples for blood culture. Chlorhexidine is also used for umbilical cord care—at a much higher concentration (4%)—in neonates born at home in settings with high neonatal mortality.39 It has also been used for whole body bathing to reduce the skin bacterial burden, particularly Staphylococcus aureus 40 in some NICUs. The choice of a safe and efficacious strength of chlorhexidine preparation would probably be different for these indications as the skin exposure area and chances of percutaneous absorption are likely to be higher.
As the incidence of skin-related adverse effects and the extent of percutaneous absorption were similar with both preparations in the study and the non-inferiority was not proven for the primary outcome, we do not find any reason to prefer 1% CHG over 2% CHG. Hence, from a clinician’s perspective, 2% CHG may be continued to be used for skin antisepsis until further evidence is generated regarding the non-inferiority of 1% CHG in neonates.
The study had a rigorous methodology. The primary investigator who collected the skin swab, the microbiologist and the data analyst were blinded to the group allocation. Quality assurance measures were in place throughout the study period. Our study had some limitations too. We could not enrol the intended number of samples due to time constraints. However, this limitation is unlikely to have resulted in low power of the study because of the slightly higher incidence of negative skin swabs—than what was estimated while calculating the sample size—in the control group (95.6% vs 94%). With all other assumptions remaining the same and substituting the incidence of negative skin swabs in both groups to be 95.6%, we actually needed to have only 265 samples in each group. Second, we could have assessed more clinically relevant outcomes like catheter colonisation or blood culture contamination rates. We had low enrolment in the gestation age group of 260/7 to 276/7 weeks, thus making it difficult to generalise the findings to neonates born at this gestation. We measured the plasma chlorhexidine concentration in only a subset due to feasibility issues. A higher number of measurements could have lent more precise answers.
Conclusion
In this randomised trial for skin antisepsis in neonates, we could not prove the non-inferiority of 1% aqueous chlorhexidine over 2% aqueous chlorhexidine for skin antisepsis in neonates. No serious adverse skin reactions were noted. Plasma chlorhexidine was detectable in all neonates who were sampled, the implications for which are unclear as no safe threshold has been established in neonates.
Data availability statement
Data are available on reasonable request. Deidentified individual participant data (including data dictionaries) that underlie the results reported in this article will be made available on publication to researchers who provide a methodologically sound proposal for use in achieving the goals of the approved proposal. Proposals should be submitted to ra.aiims@gmail.com.
Ethics statements
Patient consent for publication
Acknowledgments
We thank Dr Ujjwal Kumar for helping in the chlorhexidine plasma assay by HPLC-MS/MS experiment. We are indebted to Dr Rakesh Lodha, Dr Anjan Kumar Dhua and Dr Ajay Verma for allowing enrolment of neonates from the paediatric and paediatric surgical intensive care units. We thank Dr Arti Kapil for overseeing and enabling the timely processing of microbiological samples. We thank all the babies and their families for being part of the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AS designed the study, recruited participants, collected and analysed data, drafted the initial manuscript, and reviewed and revised the manuscript. SK participated in the design of the study, analysed and provided interpretation of the data, and reviewed and revised the manuscript. RA, AT and MJS conceptualised the study, participated in the design of the study, provided interpretation of data, and reviewed and revised the manuscript. TV contributed to study design, estimated plasma chlorhexidine concentrations, analysed data, and reviewed and revised the manuscript. SM participated in the design of the study, estimated the colony counts from the swab cultures, provided interpretation to the data, and reviewed and revised the manuscript. AKD and MB participated in the design of study, provided interpretation of data, and reviewed and revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.