
Access to Refugee and Migrant Mental Health Care Services during the First Six Months of the COVID-19 Pandemic: A Canadian Refugee Clinician Survey

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Research Team and Reflexivity
2.3. Participants and Setting
2.4. Questionnaire
2.5. Data Collection
2.6. Analysis
3. Results
3.1. Description of Participants
3.2. Main Themes
3.3. Effects of the Pandemic on Refugee Health
3.3.1. Negative Mental Health Outcomes
“The city we are in looks like it is under siege and some have commented that it appears as a war struck area, instigating their PTSD.”—Urban Family Physician with over 15 years of experience caring for refugees and migrants.
“Most of my clients disclosed that the pandemic triggers them, because they have to stay inside, and this reminded them of the war time, as they should hide from the conflicts and the death outside their doors.”—Clinical Counsellor with less than 5 years of experience caring for refugees and migrants.
3.3.2. Exacerbation of Social Determinants of Health
“Scared, unsure, confused, worried. Families are living in cramped quarters. Children have nowhere to go. Food at times was short. Access to any type of health care curtailed. Poverty is exemplified in such a situation.”—Suburban Nurse Practitioner with 10–15 years of experience caring for refugees and migrants.
3.3.3. Decreased Access to Health Care Services
3.4. Challenges with Managing Refugee and Migrant Mental Health Conditions
3.4.1. Access to Mental Health Care Services
“The already limited available services for counselling support became even more unavailable during the pandemic, exactly at the time when we needed them more.”—Small-city Family Physician with 10–15 years of experience caring for refugees and migrants.
“Due to fear many of the services that help these people are closed. Due to fear we left the most vulnerable exposed and alone. Never mind delivery of mental healthcare we barely delivered any care at all.”—Nurse Practitioner with 10–15 years of experience caring for refugees and migrants.
3.4.2. Virtual Primary Care
“Given there is often also a language barrier, they have more difficulty in calling the office and getting complex instructions on how to set up virtual care on their end. If they are successful at all, it will frequently end up being a phone call appointment as opposed to a video appointment, and I feel with this particular population a lot can be missed if we lack the visual cues that I often rely on to better understand my patient and make myself understood as well.”—Family Physician with 5–10 years of experience caring for refugees and migrants.
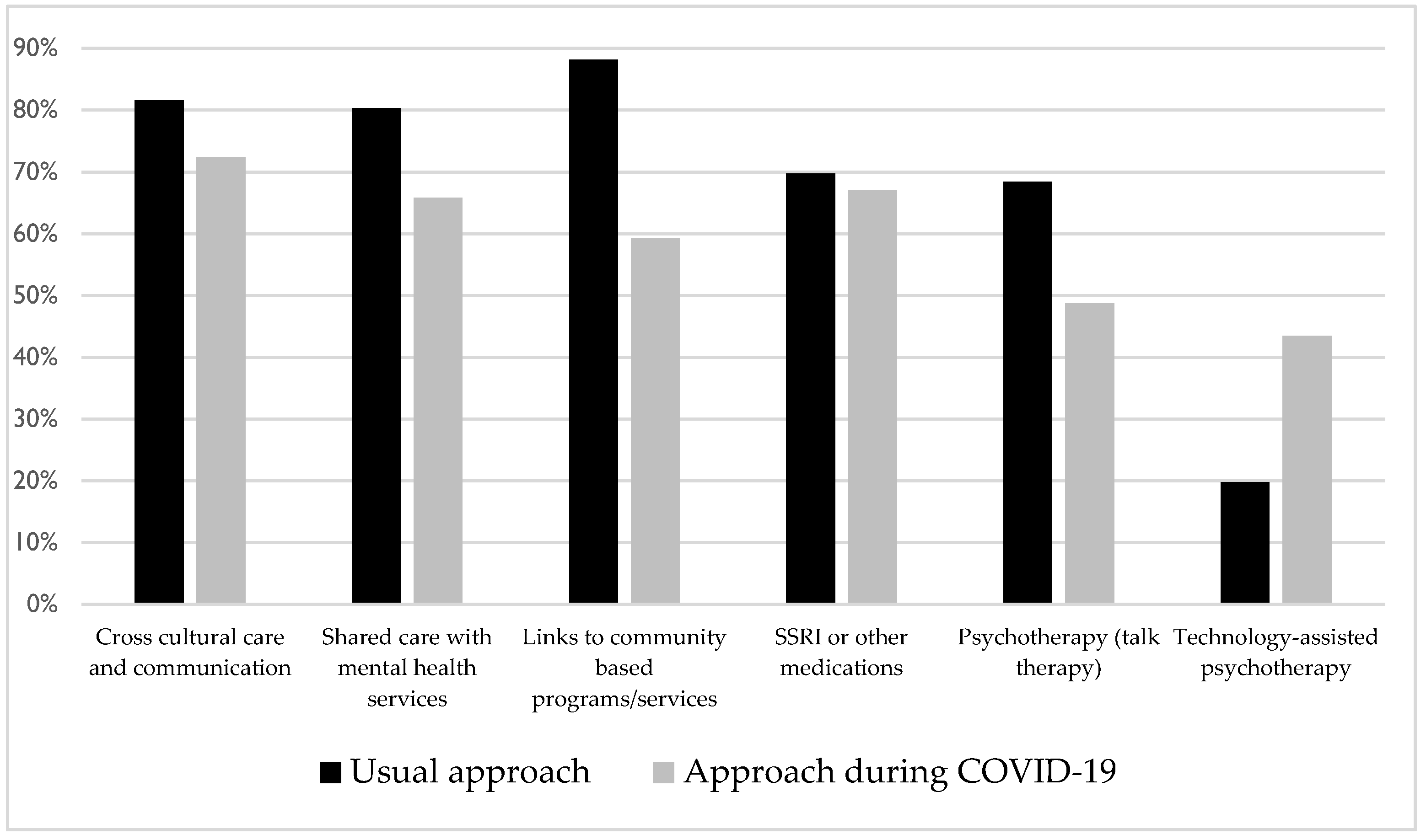
3.5. Improving Care for Refugees and Migrants
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. ApartTogether Survey: Preliminary Overview of Refugees and Migrants Self-Reported Impact of COVID-19; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Kirmayer, L.J.; Narasiah, L.; Munoz, M.; Rashid, M.; Ryder, A.G.; Guzder, J.; Hassan, G.; Rousseau, C.; Pottie, K. Common mental health problems in immigrants and refugees: General approach in primary care. CMAJ 2011, 183, E959–E967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guttmann, A.; Gandhi, S.; Wanigaratne, S.; Lu, H.; Ferreira-Legere, L.; Paul, J.; Gozdyra, P.; Campbell, T.; Chung, H.; Fung, K. COVID-19 in Immigrants, Refugees and Other Newcomers in Ontario: Characteristics of Those Tested and Those Confirmed Positive, as of June 13, 2020; ICES: Toronto, ON, Canada, 2020. [Google Scholar]
- Glover, R.E.; van Schalkwyk, M.C.I.; Akl, E.A.; Kristjannson, E.; Lotfi, T.; Petkovic, J.; Petticrew, M.P.; Pottie, K.; Tugwell, P.; Welch, V. A framework for identifying and mitigating the equity harms of COVID-19 policy interventions. J. Clin. Epidemiol. 2020, 128, 35–48. [Google Scholar] [CrossRef] [PubMed]
- Syed, I.U. Labor exploitation and health inequities among market migrants: A political economy perspective. J. Int. Migr. Integr. 2016, 17, 449–465. [Google Scholar] [CrossRef]
- Smith, J.A.; de Dieu Basabose, J.; Brockett, M.; Browne, D.T.; Shamon, S.; Stephenson, M. Family Medicine with Refugee Newcomers During the COVID-19 Crisis. Can. Fam. Phys. 2020, 34, S210–S216. [Google Scholar]
- O’Cathain, A.; Murphy, E.; Nicholl, J. The quality of mixed methods studies in health services research. J. Health Serv. Res. Policy 2008, 13, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Borkan, J.M. Mixed methods studies: A foundation for primary care research. Ann. Fam. Med. 2004, 2, 4–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Cathain, A.; Murphy, E.; Nicholl, J. Why, and how, mixed methods research is undertaken in health services research in England: A mixed methods study. BMC Health Serv. Res. 2007, 7, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jull, J.; Petticrew, M.; Kristjansson, E.; Yoganathan, M.; Petkovic, J.; Tugwell, P.; Welch, V. Engaging knowledge users in development of the CONSORT-Equity 2017 reporting guideline: A qualitative study using in-depth interviews. Res. Involv. Engagem. 2018, 4, 34. [Google Scholar] [CrossRef] [PubMed]
- Francis, J.J.; Johnston, M.; Robertson, C.; Glidewell, L.; Entwistle, V.; Eccles, M.P.; Grimshaw, J.M. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol. Health 2010, 25, 1229–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacFarlane, A.; Huschke, S.; Pottie, K.; Hauck, F.R.; Griswold, K.; Harris, M.F. Barriers to the use of trained interpreters in consultations with refugees in four resettlement countries: A qualitative analysis using normalisation process theory. BMC Fam. Pract. 2020, 21, 259. [Google Scholar] [CrossRef] [PubMed]
- Otter.ai. Otter Voice Meeting Notes. 2020. Available online: https://otter.ai (accessed on 22 June 2020).
- Sonix Inc. Sonix. 2020. Available online: https://sonix.ai/ (accessed on 12 July 2020).
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Driedger, M.; Mayhew, A.; Welch, V.; Agbata, E.; Gruner, D.; Greenaway, C.; Noori, T.; Sandu, M.; Sangou, T.; Mathew, C.; et al. Accessibility and Acceptability of Infectious Disease Interventions Among Migrants in the EU/EEA: A CERQual Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 2329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pottie, K.; Greenaway, C.; Feightner, J.; Welch, V.; Swinkels, H.; Rashid, M.; Narasiah, L.; Kirmayer, L.J.; Ueffing, E.; MacDonald, N.E.; et al. Evidence-based clinical guidelines for immigrants and refugees. Can. Med. Assoc. J. 2011, 183, E824–E925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dempster, H.; Ginn, T.; Graham, J.; Ble, M.G.; Jayasinghe, D.; Shorey, B. Locked down and Left behind: The Impact of COVID-19 on Refugees’ Economic Inclusion; Center for Global Development, Refugees International, and International Rescue Committee: Washington, DC, USA, 2020. [Google Scholar]
- International Labour Organization. ILO Warns of COVID-19 Migrant ‘Crisis within a Crisis’. Available online: https://www.ilo.org/global/about-the-ilo/newsroom/news/WCMS_748992/lang--en/index.htm (accessed on 15 October 2020).
- Gruner, D.; Magwood, O.; Bair, L.; Duff, L.; Adel, S.; Pottie, K. Understanding Supporting and Hindering Factors in Community-Based Psychotherapy for Refugees: A Realist-Informed Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4618. [Google Scholar] [CrossRef] [PubMed]
- Becker, A.E.; Kleinman, A. Mental health and the global agenda. N. Engl. J. Med. 2013, 369, 66–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canadian Medical Association. Virtual Care in Canada: Discussion Paper; Canadian Medical Association: Ottawa, ON, Canada, 2019; Available online: https://www.cma.ca/sites/default/files/pdf/News/Virtual_Care_discussionpaper_v2EN.pdf (accessed on 22 September 2020).
- Hassan, A.; Sharif, K. Efficacy of Telepsychiatry in Refugee Populations: A Systematic Review of the Evidence. Cureus 2019, 11, e3984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blower, J. Exploring Innovative Migrant Integration Practices in Small and Mid-Sized Cities across Canada; Ryerson University: Toronto, ON, Canada, 2020. [Google Scholar]


{kind=link}
| Characteristic | N | % |
|---|---|---|
| Profession | ||
| Physician Family Physician (29), Psychiatrist (9), Pediatrician (5), Emergency Physician (3), Internist (3) | 49 | 63.64 |
| Nurse or Nurse Practitioner | 12 | 15.58 |
| Psychologist or Counselor | 12 | 15.58 |
| Other Social Worker (2), Program Lead (1), Client Advocate (1) | 4 | 5.19 |
| Gender | ||
| Female | 56 | 72.73 |
| Male | 20 | 25.97 |
| Prefer not to say | 1 | 1.30 |
| Length of Time Caring for Refugees | ||
| <5 years | 22 | 28.57 |
| 5–10 years | 25 | 32.47 |
| 10–15 years | 10 | 12.99 |
| 15+ years | 20 | 25.97 |
| Province or Territory | ||
| Alberta | 11 | 14.29 |
| British Columbia | 11 | 14.29 |
| Newfoundland and Labrador | 1 | 1.30 |
| Nova Scotia | 7 | 9.09 |
| Ontario | 42 | 54.55 |
| Prince Edward Island | 1 | 1.30 |
| Quebec | 3 | 3.90 |
| Saskatchewan | 3 | 3.90 |
| Nunavut | 1 | 1.30 |
| Yukon | 1 | 1.30 |
| Received Training in Refugee Mental Health Care Approaches | ||
| Yes | 48 | 62.34 |
| No | 29 | 37.66 |
| Psychologists or Psychiatrists Working Within or Linked to Clinic | ||
| Yes | 51 | 67.11 |
| No | 25 | 32.89 |
| Availability of Medical Interpretation Services Within Clinic | ||
| Yes | 66 | 85.71 |
| No | 10 | 12.99 |
| Don’t Know | 1 | 1.30 |
| Survey Question | N | Yes n (%) | No n (%) | Don’t Know n (%) |
|---|---|---|---|---|
| Has the pandemic resulted in an increase in refugee and other migrant patients requesting anxiety or mental health support? | 77 | 40 (51.95) | 21 (27.27) | 16 (20.78) |
| During COVID-19 have you noted increased tension and conflict within refugee family relationships? | 77 | 37 (48.05) | 20 (25.97) | 20 (25.97) |
| Survey Question | N | Higher n (%) | Similar n (%) | Lower n (%) | Don’t Know n (%) |
|---|---|---|---|---|---|
| Do you have the impression that your refugee and other migrant patients have a higher, lower or similar rate of unemployment during COVID-19 compared to pre-COVID-19? | 77 | 41 (53.25) | 10 (12.99) | 12 (15.58) | 14 (18.18) |
| Do you have the impression that refugees and other migrants have a higher, lower or similar rate of homelessness or precarious housing during COVID-19 compared to pre-COVID-19? | 77 | 21 (27.27) | 36 (46.75) | 6 (7.79) | 14 (18.18) |
| Do you have the impression that refugees and other migrants in your practice have a higher, lower or similar rate of access to care during COVID-19 compared to pre-COVID-19? | 76 | 4 (5.26) | 17 (22.37) | 52 (68.42) | 3 (3.95) |
| Survey Question | N | Yes n (%) | No n (%) | Don’t Know n (%) |
|---|---|---|---|---|
| Is technology-assisted psychotherapy feasible to arrange for refugees and other migrants? | 75 | 49 (65.33) | 12 (16.00) | 14 (18.67) |
| Is technology-assisted psychotherapy acceptable for refugees and other migrants? | 74 | 48 (64.86) | 7 (9.46) | 19 (25.68) |
| Would technology-assisted psychotherapy increase health equity for refugees and other migrants? | 75 | 50 (66.67) | 9 (12.00) | 16 (21.33) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benjamen, J.; Girard, V.; Jamani, S.; Magwood, O.; Holland, T.; Sharfuddin, N.; Pottie, K. Access to Refugee and Migrant Mental Health Care Services during the First Six Months of the COVID-19 Pandemic: A Canadian Refugee Clinician Survey. Int. J. Environ. Res. Public Health 2021, 18, 5266. https://doi.org/10.3390/ijerph18105266
Benjamen J, Girard V, Jamani S, Magwood O, Holland T, Sharfuddin N, Pottie K. Access to Refugee and Migrant Mental Health Care Services during the First Six Months of the COVID-19 Pandemic: A Canadian Refugee Clinician Survey. International Journal of Environmental Research and Public Health. 2021; 18(10):5266. https://doi.org/10.3390/ijerph18105266
Chicago/Turabian StyleBenjamen, Joseph, Vincent Girard, Shabana Jamani, Olivia Magwood, Tim Holland, Nazia Sharfuddin, and Kevin Pottie. 2021. "Access to Refugee and Migrant Mental Health Care Services during the First Six Months of the COVID-19 Pandemic: A Canadian Refugee Clinician Survey" International Journal of Environmental Research and Public Health 18, no. 10: 5266. https://doi.org/10.3390/ijerph18105266