
An Interaction Effect Analysis of Thermodilution-Guided Hemodynamic Optimization, Patient Condition, and Mortality after Successful Cardiopulmonary Resuscitation

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
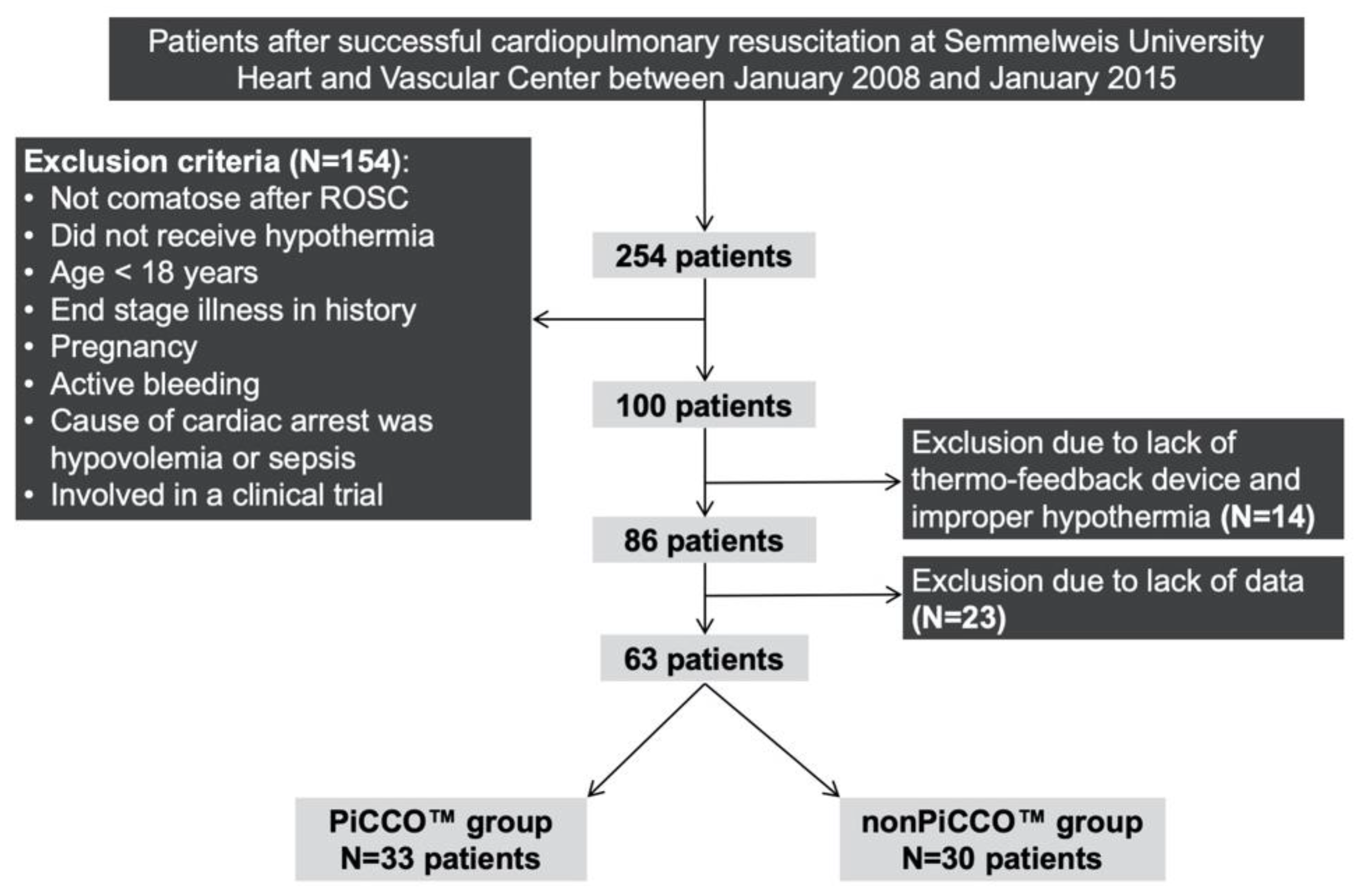
2.2. Patients
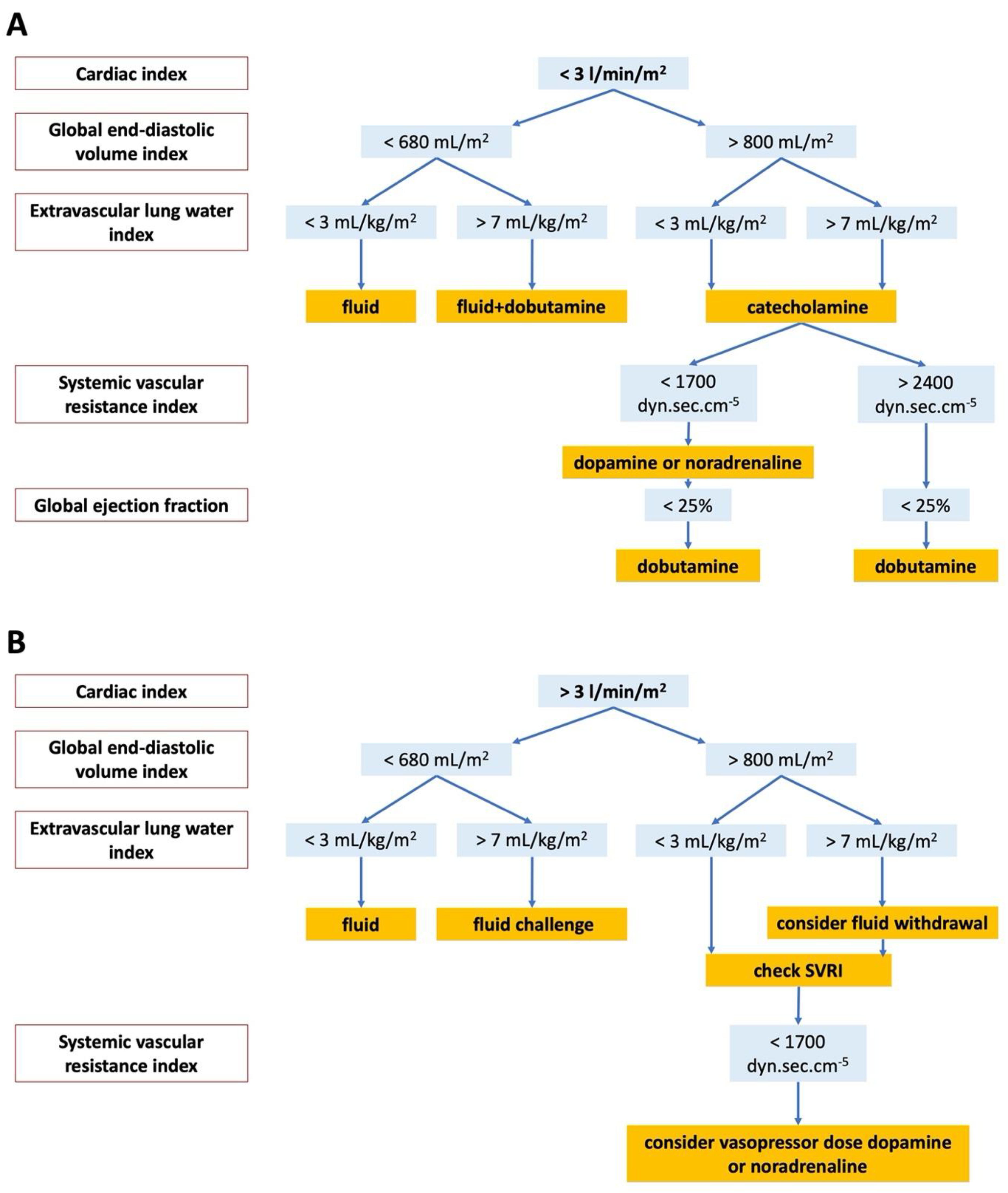
2.3. Initial Therapy
2.4. Patient Outcomes
2.5. Statistical Analysis
3. Results
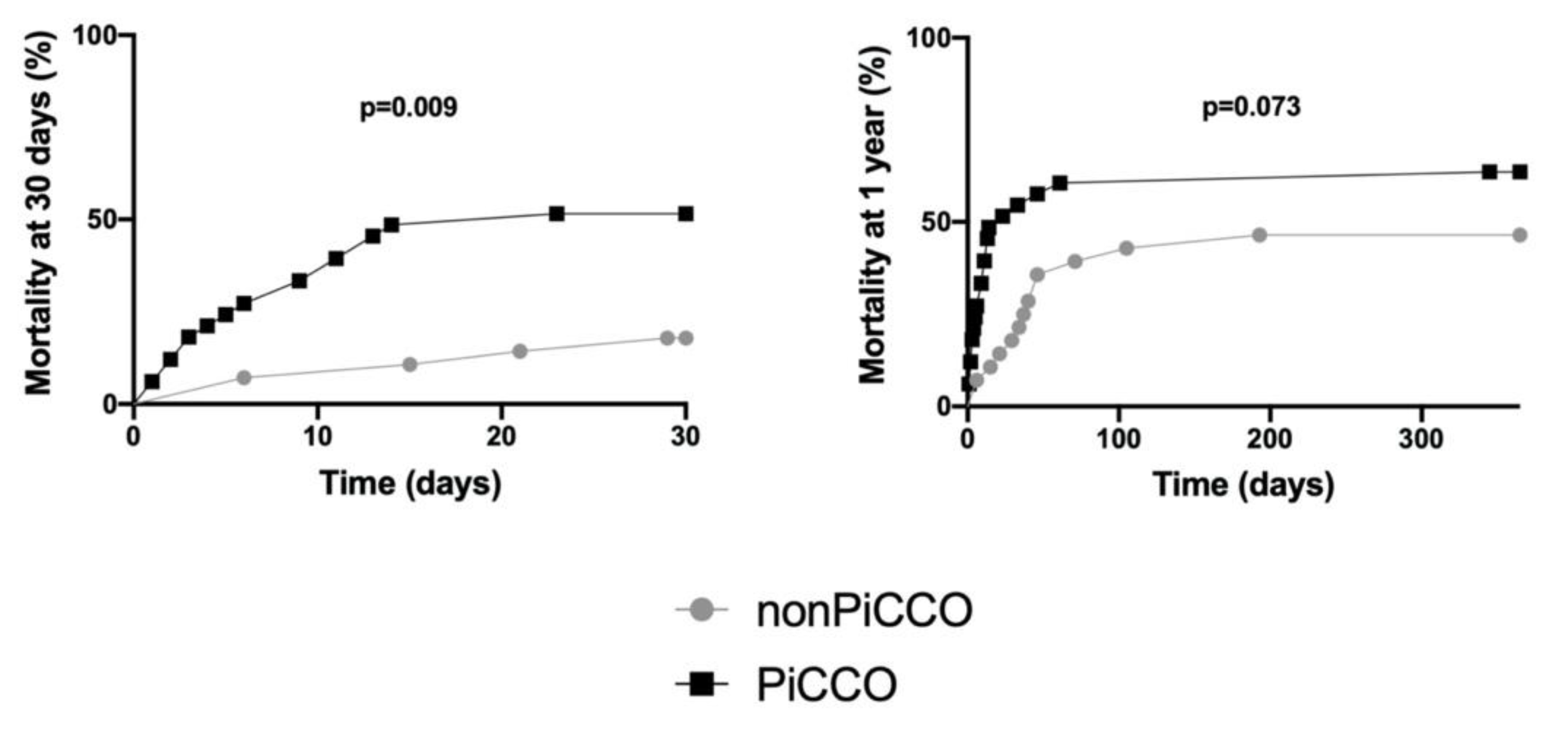
3.1. Characteristics of Patients, PiCCO™ Use, 30 Day and 1 Year Mortality
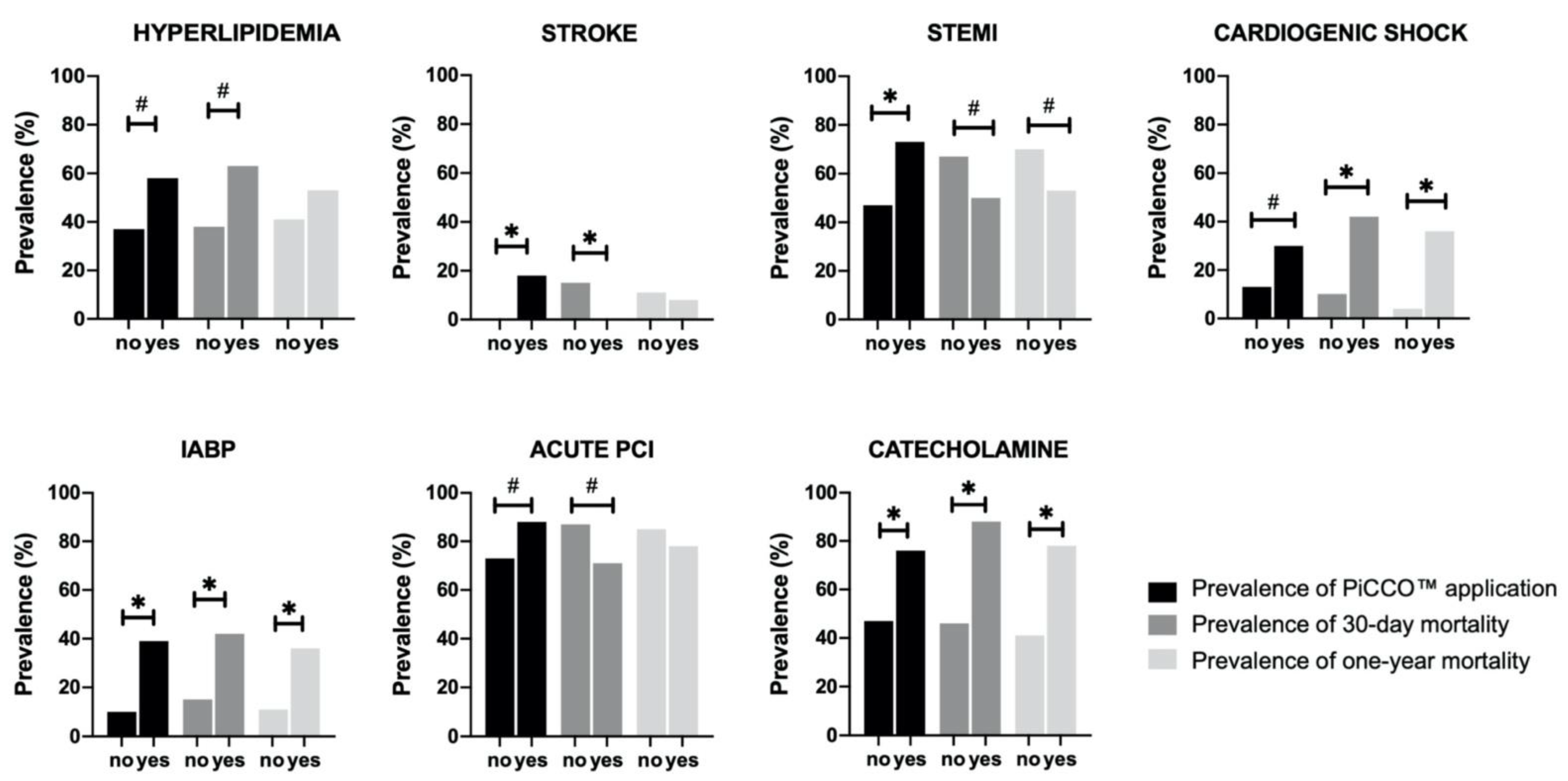
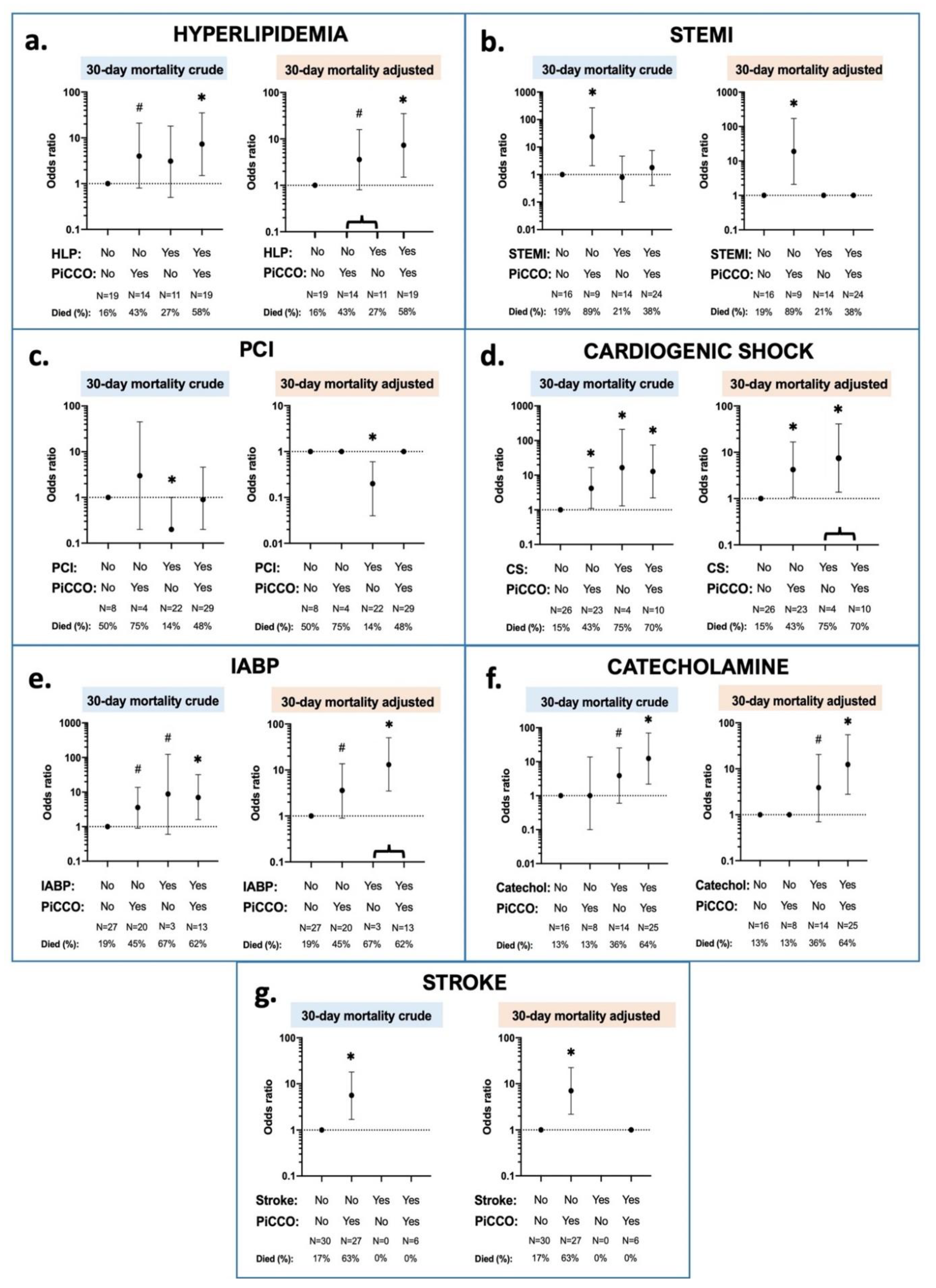
3.2. Interaction Effects between 30 Day Mortality, PiCCO™ Use and Patient Characteristics
3.3. Interaction Effects between 1 Year Mortality, PiCCO™ Use and Patient Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grasner, J.T.; Wnent, J.; Herlitz, J.; Perkins, G.D.; Lefering, R.; Tjelmeland, I.; Koster, R.W.; Masterson, S.; Rossell-Ortiz, F.; Maurer, H.; et al. Survival after out-of-hospital cardiac arrest in Europe—Results of the EuReCa TWO study. Resuscitation 2020, 148, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Kiguchi, T.; Okubo, M.; Nishiyama, C.; Maconochie, I.; Ong, M.E.H.; Kern, K.B.; Wyckoff, M.H.; McNally, B.; Christensen, E.F.; Tjelmeland, I.; et al. Out-of-hospital cardiac arrest across the World: First report from the International Liaison Committee on Resuscitation (ILCOR). Resuscitation 2020, 152, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Handley, A.J.; Koster, R.W.; Castren, M.; Smyth, M.A.; Olasveengen, T.; Monsieurs, K.G.; Raffay, V.; Grasner, J.T.; Wenzel, V.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 2. Adult basic life support and automated external defibrillation. Resuscitation 2015, 95, 81–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nolan, J.P.; Neumar, R.W.; Adrie, C.; Aibiki, M.; Berg, R.A.; Bottiger, B.W.; Callaway, C.; Clark, R.S.; Geocadin, R.G.; Jauch, E.C.; et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation 2008, 79, 350–379. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Soar, J.; Cariou, A.; Cronberg, T.; Moulaert, V.R.; Deakin, C.D.; Bottiger, B.W.; Friberg, H.; Sunde, K.; Sandroni, C. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines for Post-resuscitation Care 2015: Section 5 of the European Resuscitation Council Guidelines for Resuscitation 2015. Resuscitation 2015, 95, 202–222. [Google Scholar] [CrossRef] [PubMed]
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N. Engl. J. Med. 2002, 346, 549–556. [Google Scholar] [CrossRef]
- Bernard, S.A.; Gray, T.W.; Buist, M.D.; Jones, B.M.; Silvester, W.; Gutteridge, G.; Smith, K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N. Engl. J. Med. 2002, 346, 557–563. [Google Scholar] [CrossRef]
- Nielsen, N.; Wetterslev, J.; Cronberg, T.; Erlinge, D.; Gasche, Y.; Hassager, C.; Horn, J.; Hovdenes, J.; Kjaergaard, J.; Kuiper, M.; et al. Targeted temperature management at 33 degrees C versus 36 degrees C after cardiac arrest. N. Engl. J. Med. 2013, 369, 2197–2206. [Google Scholar] [CrossRef] [Green Version]
- Kovacs, E.; Jenei, Z.; Horvath, A.; Geller, L.; Szilagyi, S.; Kiraly, A.; Molnar, L.; Sotonyi, P., Jr.; Merkely, B.; Zima, E. Physiologic effects of hypothermia. Orv. Hetil. 2011, 152, 171–181. [Google Scholar] [CrossRef]
- Delhaye, C.; Mahmoudi, M.; Waksman, R. Hypothermia therapy: Neurological and cardiac benefits. J. Am. Coll. Cardiol. 2012, 59, 197–210. [Google Scholar] [CrossRef] [Green Version]
- Sundgreen, C.; Larsen, F.S.; Herzog, T.M.; Knudsen, G.M.; Boesgaard, S.; Aldershvile, J. Autoregulation of cerebral blood flow in patients resuscitated from cardiac arrest. Stroke 2001, 32, 128–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oren-Grinberg, A. The PiCCO Monitor. Int. Anesthesiol. Clin. 2010, 48, 57–85. [Google Scholar] [CrossRef]
- Werner, M.; Wernly, B.; Lichtenauer, M.; Franz, M.; Kabisch, B.; Muessig, J.M.; Masyuk, M.; Schulze, P.C.; Hoppe, U.C.; Kelm, M.; et al. Real-world extravascular lung water index measurements in critically ill patients: Pulse index continuous cardiac output measurements: Time course analysis and association with clinical characteristics. Wien. Klin. Wochenschr. 2019, 131, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Huber, W.; Umgelter, A.; Reindl, W.; Franzen, M.; Schmidt, C.; von Delius, S.; Geisler, F.; Eckel, F.; Fritsch, R.; Siveke, J.; et al. Volume assessment in patients with necrotizing pancreatitis: A comparison of intrathoracic blood volume index, central venous pressure, and hematocrit, and their correlation to cardiac index and extravascular lung water index. Crit. Care Med. 2008, 36, 2348–2354. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Cui, N.; Su, L.; Long, Y.; Wang, X.; Zhou, X.; Chai, W.; Liu, D. Prognostic value of extravascular lung water and its potential role in guiding fluid therapy in septic shock after initial resuscitation. J. Crit. Care 2016, 33, 106–113. [Google Scholar] [CrossRef]
- Goepfert, M.S.; Reuter, D.A.; Akyol, D.; Lamm, P.; Kilger, E.; Goetz, A.E. Goal-directed fluid management reduces vasopressor and catecholamine use in cardiac surgery patients. Intensive Care Med. 2007, 33, 96–103. [Google Scholar] [CrossRef]
- Tagami, T.; Kushimoto, S.; Tosa, R.; Omura, M.; Hagiwara, J.; Hirama, H.; Yokota, H. The precision of PiCCO(R) measurements in hypothermic post-cardiac arrest patients. Anaesthesia 2012, 67, 236–243. [Google Scholar] [CrossRef]
- Cecconi, M.; De Backer, D.; Antonelli, M.; Beale, R.; Bakker, J.; Hofer, C.; Jaeschke, R.; Mebazaa, A.; Pinsky, M.R.; Teboul, J.L.; et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014, 40, 1795–1815. [Google Scholar] [CrossRef]
- Nolan, J.P.; Hazinski, M.F.; Aickin, R.; Bhanji, F.; Billi, J.E.; Callaway, C.W.; Castren, M.; de Caen, A.R.; Ferrer, J.M.; Finn, J.C.; et al. Part 1: Executive summary: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2015, 95, e1–e31. [Google Scholar] [CrossRef]
- Koster, R.W.; Sayre, M.R.; Botha, M.; Cave, D.M.; Cudnik, M.T.; Handley, A.J.; Hatanaka, T.; Hazinski, M.F.; Jacobs, I.; Monsieurs, K.; et al. Part 5: Adult basic life support: 2010 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation 2010, 81 (Suppl. 1), e48–e70. [Google Scholar] [CrossRef]
- Pulsion Medical System, PiCCO2 Technical Datasheet Ref: MPI850305_R05. Available online: https://www.getinge.com/dam/hospital/documents/english/picco_technology_brochure-en-non_us.pdf (accessed on 13 May 2021).
- Laurent, I.; Monchi, M.; Chiche, J.D.; Joly, L.M.; Spaulding, C.; Bourgeois, B.; Cariou, A.; Rozenberg, A.; Carli, P.; Weber, S.; et al. Reversible myocardial dysfunction in survivors of out-of-hospital cardiac arrest. J. Am. Coll. Cardiol. 2002, 40, 2110–2116. [Google Scholar] [CrossRef] [Green Version]
- Pellis, T.; Sanfilippo, F.; Ristagno, G. The optimal hemodynamics management of post-cardiac arrest shock. Best Pract. Res. Clin. Anaesthesiol. 2015, 29, 485–495. [Google Scholar] [CrossRef]
- Kozar, M.; Javorka, K.; Javorka, M.; Matasova, K.; Zibolen, M. Changes of cardiovascular regulation during rewarming in newborns undergoing whole-body hypothermia. Neuro Endocrinol. Lett. 2015, 36, 434–438. [Google Scholar] [PubMed]
- Demirgan, S.; Erkalp, K.; Sevdi, M.S.; Aydogmus, M.T.; Kutbay, N.; Firincioglu, A.; Ozalp, A.; Alagol, A. Cardiac condition during cooling and rewarming periods of therapeutic hypothermia after cardiopulmonary resuscitation. BMC Anesthesiol. 2014, 14, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sunde, K.; Pytte, M.; Jacobsen, D.; Mangschau, A.; Jensen, L.P.; Smedsrud, C.; Draegni, T.; Steen, P.A. Implementation of a standardised treatment protocol for post resuscitation care after out-of-hospital cardiac arrest. Resuscitation 2007, 73, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Gaieski, D.F.; Band, R.A.; Abella, B.S.; Neumar, R.W.; Fuchs, B.D.; Kolansky, D.M.; Merchant, R.M.; Carr, B.G.; Becker, L.B.; Maguire, C.; et al. Early goal-directed hemodynamic optimization combined with therapeutic hypothermia in comatose survivors of out-of-hospital cardiac arrest. Resuscitation 2009, 80, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Beylin, M.E.; Perman, S.M.; Abella, B.S.; Leary, M.; Shofer, F.S.; Grossestreuer, A.V.; Gaieski, D.F. Higher mean arterial pressure with or without vasoactive agents is associated with increased survival and better neurological outcomes in comatose survivors of cardiac arrest. Intensive Care Med. 2013, 39, 1981–1988. [Google Scholar] [CrossRef]
- Kilgannon, J.H.; Roberts, B.W.; Jones, A.E.; Mittal, N.; Cohen, E.; Mitchell, J.; Chansky, M.E.; Trzeciak, S. Arterial blood pressure and neurologic outcome after resuscitation from cardiac arrest*. Crit. Care Med. 2014, 42, 2083–2091. [Google Scholar] [CrossRef]
- Walters, E.L.; Morawski, K.; Dorotta, I.; Ramsingh, D.; Lumen, K.; Bland, D.; Clem, K.; Nguyen, H.B. Implementation of a post-cardiac arrest care bundle including therapeutic hypothermia and hemodynamic optimization in comatose patients with return of spontaneous circulation after out-of-hospital cardiac arrest: A feasibility study. Shock 2011, 35, 360–366. [Google Scholar] [CrossRef]
- Litton, E.; Morgan, M. The PiCCO monitor: A review. Anaesth. Intensive Care 2012, 40, 393–409. [Google Scholar] [CrossRef] [Green Version]
- Swan, H.J.; Ganz, W.; Forrester, J.; Marcus, H.; Diamond, G.; Chonette, D. Catheterization of the heart in man with use of a flow-directed balloon-tipped catheter. N. Engl. J. Med. 1970, 283, 447–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gassanov, N.; Caglayan, E.; Nia, A.; Erdmann, E.; Er, F. Hemodynamic monitoring in the intensive care unit: Pulmonary artery catheter versus PiCCO. Dtsch. Med. Wochenschr. 2011, 136, 376–380. [Google Scholar] [CrossRef]
- Gassanov, N.; Caglayan, E.; Nia, A.; Erdmann, E.; Er, F. The PiCCO catheter. Dtsch. Med. Wochenschr. 2010, 135, 2311–2314. [Google Scholar] [CrossRef]
- Monnet, X.; Teboul, J.L. Transpulmonary thermodilution: Advantages and limits. Crit. Care 2017, 21, 147. [Google Scholar] [CrossRef] [PubMed]
- Lichtwarck-Aschoff, M.; Zeravik, J.; Pfeiffer, U.J. Intrathoracic blood volume accurately reflects circulatory volume status in critically ill patients with mechanical ventilation. Intensive Care Med. 1992, 18, 142–147. [Google Scholar] [CrossRef]
- Zhang, Y.B.; Zhang, Z.Z.; Li, J.X.; Wang, Y.H.; Zhang, W.L.; Tian, X.L.; Han, Y.F.; Yang, M.; Liu, Y. Application of pulse index continuous cardiac output system in elderly patients with acute myocardial infarction complicated by cardiogenic shock: A prospective randomized study. World J. Clin. Cases 2019, 7, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Feneck, R.O.; Sherry, K.M.; Withington, P.S.; Oduro-Dominah, A.; European Milrinone Multicenter Trial, G. Comparison of the hemodynamic effects of milrinone with dobutamine in patients after cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2001, 15, 306–315. [Google Scholar] [CrossRef]
- De Backer, D.; Biston, P.; Devriendt, J.; Madl, C.; Chochrad, D.; Aldecoa, C.; Brasseur, A.; Defrance, P.; Gottignies, P.; Vincent, J.L.; et al. Comparison of dopamine and norepinephrine in the treatment of shock. N. Engl. J. Med. 2010, 362, 779–789. [Google Scholar] [CrossRef] [Green Version]
- Hamzaoui, O.; Jozwiak, M.; Geffriaud, T.; Sztrymf, B.; Prat, D.; Jacobs, F.; Monnet, X.; Trouiller, P.; Richard, C.; Teboul, J.L. Norepinephrine exerts an inotropic effect during the early phase of human septic shock. Br. J. Anaesth. 2018, 120, 517–524. [Google Scholar] [CrossRef] [Green Version]
- Friesenecker, B.E.; Tsai, A.G.; Martini, J.; Ulmer, H.; Wenzel, V.; Hasibeder, W.R.; Intaglietta, M.; Dunser, M.W. Arteriolar vasoconstrictive response: Comparing the effects of arginine vasopressin and norepinephrine. Crit. Care 2006, 10, R75. [Google Scholar] [CrossRef] [Green Version]
- Bai, X.; Yu, W.; Ji, W.; Lin, Z.; Tan, S.; Duan, K.; Dong, Y.; Xu, L.; Li, N. Early versus delayed administration of norepinephrine in patients with septic shock. Crit. Care 2014, 18, 532. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Total |
|---|---|
| n (%) | |
| or | |
| Median (IQR) | |
| Total | 63 (100%) |
| Age | 64 (56, 69) |
| Gender (female in %) | 19 (30%) |
| IHCA | 11 (17 %) |
| Prior history: | |
| Hypertension | 45 (71%) |
| Diabetes | 18 (29%) |
| Hyperlipidemia | 30 (48%) |
| AMI | 15 (24%) |
| Stroke | 6 (10%) |
| Circumstances of CPR: | |
| Patient on monitor when collapsed | 9 (14%) |
| BLS performed by bystanders | 49 (78%) |
| Time to ROSC (minutes) | 20 (15, 30) |
| Initial rhythm: | |
| VF | 42 (67%) |
| VT | 2 (3%) |
| PEA | 10 (16%) |
| Asystole | 9 (14%) |
| Cause of cardiac arrest: | |
| STEMI | 38 (60%) |
| NSTEMI | 8 (13%) |
| Cardiac condition after ROSC: | |
| Cardiogenic shock (clinical signs) | 14 (22%) |
| EF after ROSC (%) | 36 (29, 48) |
| Therapy after ROSC: | |
| Catecholamine therapy | 39 (62%) |
| Acute PCI | 51 (81%) |
| Levosimendan | 7 (11%) |
| IABP use | 16 (25%) |
| Time to reach target temperature (hours) | 3,8 (2.0, 5.1) |
| PiCCO™ application rate | 33 (52%) |
| Died at 30 days | 24 (38%) |
| Died at 1 year | 36 (57%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovács, E.; Gyarmathy, V.A.; Pilecky, D.; Fekete-Győr, A.; Szakál-Tóth, Z.; Gellér, L.; Hauser, B.; Gál, J.; Merkely, B.; Zima, E. An Interaction Effect Analysis of Thermodilution-Guided Hemodynamic Optimization, Patient Condition, and Mortality after Successful Cardiopulmonary Resuscitation. Int. J. Environ. Res. Public Health 2021, 18, 5223. https://doi.org/10.3390/ijerph18105223
Kovács E, Gyarmathy VA, Pilecky D, Fekete-Győr A, Szakál-Tóth Z, Gellér L, Hauser B, Gál J, Merkely B, Zima E. An Interaction Effect Analysis of Thermodilution-Guided Hemodynamic Optimization, Patient Condition, and Mortality after Successful Cardiopulmonary Resuscitation. International Journal of Environmental Research and Public Health. 2021; 18(10):5223. https://doi.org/10.3390/ijerph18105223
Chicago/Turabian StyleKovács, Enikő, Valéria Anna Gyarmathy, Dávid Pilecky, Alexandra Fekete-Győr, Zsófia Szakál-Tóth, László Gellér, Balázs Hauser, János Gál, Béla Merkely, and Endre Zima. 2021. "An Interaction Effect Analysis of Thermodilution-Guided Hemodynamic Optimization, Patient Condition, and Mortality after Successful Cardiopulmonary Resuscitation" International Journal of Environmental Research and Public Health 18, no. 10: 5223. https://doi.org/10.3390/ijerph18105223