
Chronic Obstructive Pulmonary Disease Patients’ Acceptance in E-Health Clinical Trials

 ,
, 
 and
and
Abstract
:1. Introduction
2. Methods
2.1. The Inclusion Criteria
- Controlled clinical trials with or without randomization that examined TH interventions;
- Studies that include patients diagnosed with COPD (defined as forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio < 70%, FEV1 < 80% predicted);
- The intervention included in this review is telehealth. As telehealth interventions have different labels (e.g., telemonitoring, telerehabilitation) in the literature, no restrictions have been applied on intervention labeling. TH interventions with different labels which use internet or electronic health information and communication technologies to support distance health care and/or exchange information between patients and healthcare providers were included.
2.2. The Exclusion Criteria
- Studies that targeted non-COPD individuals and/or a general population;
- Trials published in a language other than English;
- Studies that did not describe TH, including the content of the intervention, delivery method, mode of administration, and frequency of data transmission;
- Studies that did not report the number of COPD individuals who were approached, consented, and dropped out.
2.3. Search Strategy
2.4. Search Procedures
2.5. Data Extraction
2.6. Data Analysis
3. Results
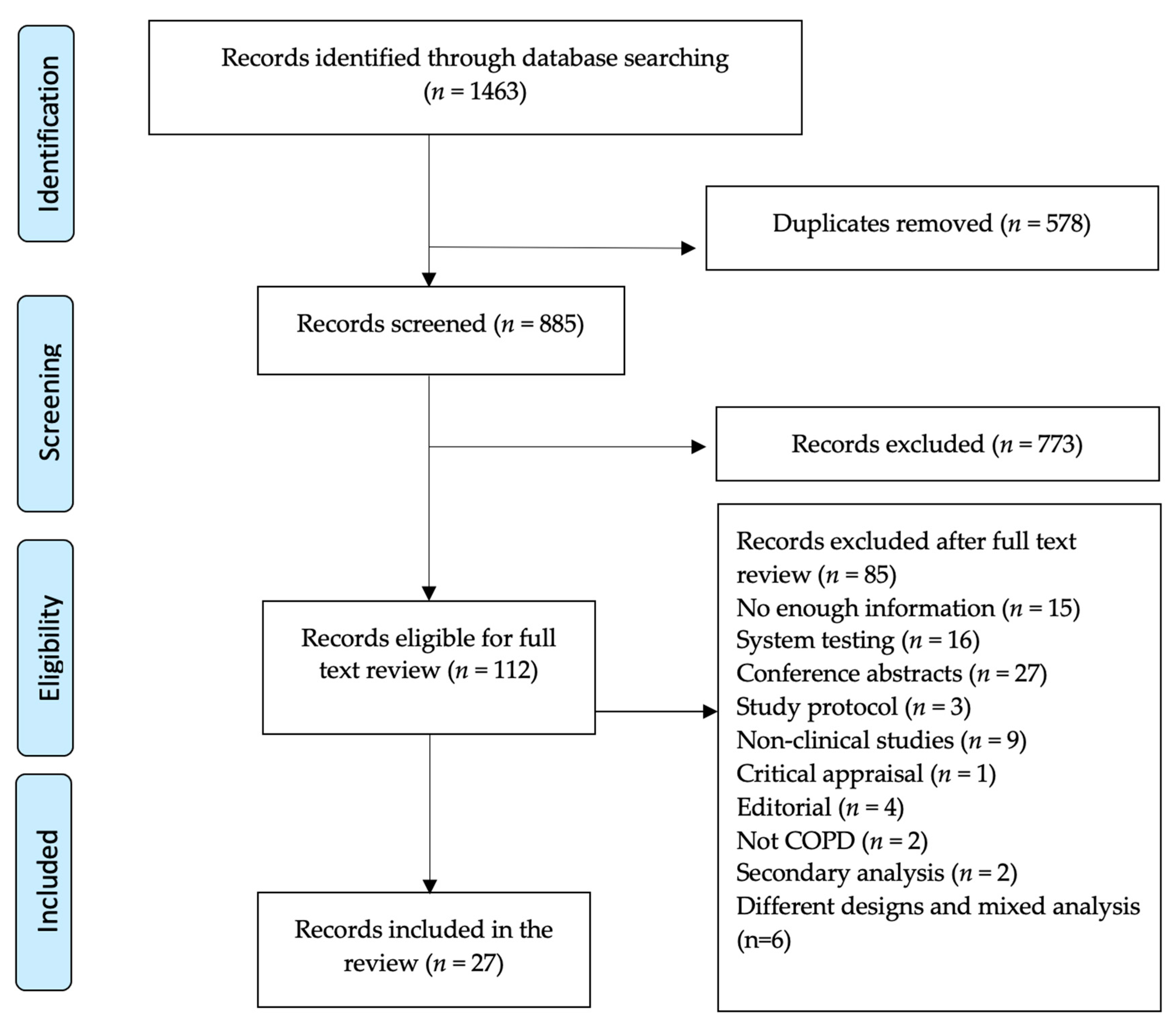
3.1. Study Selection
3.2. Study Characteristics
3.3. Patient Characteristics
3.4. TH Intervention Characteristics
3.5. Acceptance and Dropout Rates
3.6. Meta-Analysis
3.7. Reasons for Dropout
3.8. Quality Assessment
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TH | Telehealth |
| TM | Telemonitoring |
| SF | Self-management |
| COPD | Chronic Obstructive Pulmonary Disease |
| RCT | Randomized control trials |
| NRCT | Non-randomized control trials |
References
- Mathers, C.D.; Loncar, D. Projections of global mortality and the burden of disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [Green Version]
- Buist, A.S.; McBurnie, M.A.; Vollmer, W.M.; Gillespie, S.; Burney, P.; Mannino, D.M.; Menezes, A.M.; Sullivan, S.D.; A Lee, T.; Weiss, K.B.; et al. International variation in the prevalence of COPD (The BOLD Study): A population-based prevalence study. Lancet 2007, 370, 741–750. [Google Scholar] [CrossRef]
- World Health Organization Fact Sheet for Chronic Obstructive Lung Disease. World Health Organization 2017. Available online: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(COPD) (accessed on 22 October 2020).
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2020 Report). 2020. Available online: https://goldcopd.org/ (accessed on 23 October 2020).
- Fletcher, M.J.; Upton, J.; Taylor-Fishwick, J.; Buist, S.A.; Jenkins, C.; Hutton, J.; Barnes, N.; Van Der Molen, T.; Walsh, J.W.; Jones, P.; et al. COPD uncovered: An international survey on the impact of chronic obstructive pulmonary disease [COPD] on a working age population. BMC Public Health 2011, 11, 612. [Google Scholar] [CrossRef] [Green Version]
- Halbert, R.J.; Natoli, J.L.; Gano, A.; Badamgarav, E.; Buist, A.S.; Mannino, D.M. Global burden of COPD: Systematic review and meta-analysis. Eur. Respir. J. 2006, 28, 523–532. [Google Scholar] [CrossRef]
- Yang, F.; Xiong, Z.-F.; Yang, C.; Li, L.; Qiao, G.; Wang, Y.; Zheng, T.; He, H.; Hu, H. Continuity of care to prevent readmissions for patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis. COPD J. Chronic Obstr. Pulm. Dis. 2017, 14, 251–261. [Google Scholar] [CrossRef]
- Selzler, A.-M.; Wald, J.; Sedeno, M.; Jourdain, T.; Janaudis-Ferreira, T.; Goldstein, R.; Bourbeau, J.; Stickland, M.K. Telehealth pulmonary rehabilitation: A review of the literature and an example of a nationwide initiative to improve the accessibility of pulmonary rehabilitation. Chronic Respir. Dis. 2017, 15, 41–47. [Google Scholar] [CrossRef]
- Zwerink, M.; Brusse-Keizer, M.; Van Der Valk, P.D.; Zielhuis, G.A.; Monninkhof, E.M.; Van Der Palen, J.A.M.; Frith, P.A.; Effing, T. Self management for patients with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2014, 2014, CD002990. [Google Scholar] [CrossRef]
- Alghamdi, S.M.; Alqahtani, J.S.; Aldhahir, A.M. Current status of telehealth in Saudi Arabia during COVID-19. J. Fam. Community Med. 2020, 27, 208–211. [Google Scholar] [CrossRef]
- Alghamdi, S.; Alqahtani, J.; Aldhahir, A.; Alrajeh, A.; Aldabayan, Y. Effectiveness of telehealth-based interventions with chronic obstructive pulmonary disease: A systematic review and meta-analysis. Am. Thorac. Soc. 2020. [Google Scholar] [CrossRef]
- Alwashmi, M.; Hawboldt, J.; Davis, E.; Marra, C.; Gamble, J.-M.; Abu Ashour, W. The effect of smartphone interventions on patients with chronic obstructive pulmonary disease exacerbations: A systematic review and meta-analysis. JMIR mHealth uHealth 2016, 4, e105. [Google Scholar] [CrossRef]
- Alghamdi, S.M.; Aldhahir, A.M.; Alqahtani, J.S.; Aldabayan, Y.S.; Al Rajeh, A.M. Telemonitoring parameters used in home-based rehabilitation with COPD: A systematic review. Respir. Care 2020, 65, 344226. [Google Scholar]
- Almojaibel, A.A. Delivering pulmonary rehabilitation for patients with chronic obstructive pulmonary disease at home using telehealth: A review of the literature. Saudi J. Med. Med Sci. 2016, 4, 164. [Google Scholar] [CrossRef]
- Burkow, T.M.; Vognild, L.K.; Østengen, G.; Johnsen, E.; Risberg, M.J.; Bratvold, A.; Hagen, T.; Brattvoll, M.; Krogstad, T.; Hjalmarsen, A. Internet-enabled pulmonary rehabilitation and diabetes education in group settings at home: A preliminary study of patient acceptability. BMC Med. Inform. Decis. Mak. 2013, 13, 33. [Google Scholar] [CrossRef] [Green Version]
- Holland, A.E.; Hill, C.J.; Rochford, P.; Fiore, J.; Berlowitz, D.J.; McDonald, C.F. Telerehabilitation for people with chronic obstructive pulmonary disease: Feasibility of a simple, real time model of supervised exercise training. J. Telemed. Telecare 2013, 19, 222–226. [Google Scholar] [CrossRef]
- Paneroni, M.; Colombo, F.; Papalia, A.; Colitta, A.; Borghi, G.; Saleri, M.; Cabiaglia, A.; Azzalini, E.; Vitacca, M. Is telerehabilitation a safe and viable option for patients with COPD? A feasibility study. COPD J. Chronic Obstr. Pulm. Dis. 2014, 12, 217–225. [Google Scholar] [CrossRef]
- Tabak, M.; Van Der Valk, P.; Hermens, H.; Vollenbroek-Hutten, M.; Brusse-Keizer, M. A telehealth program for self-management of COPD exacerbations and promotion of an active lifestyle: A pilot randomized controlled trial. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 935. [Google Scholar] [CrossRef] [Green Version]
- Zanaboni, P.; Lien, L.A.; Hjalmarsen, A.; Wootton, R. Long-term telerehabilitation of COPD patients in their homes: Interim results from a pilot study in Northern Norway. J. Telemed. Telecare 2013, 19, 425–429. [Google Scholar] [CrossRef]
- Cruz, J.; Brooks, D.; Marques, A. Home telemonitoring in COPD: A systematic review of methodologies and patients’ adherence. Int. J. Med. Inform. 2014, 83, 249–263. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Arafah, A.M.; Bouchard, V.; Mayo, N.E. Enrolling and keeping participants in multiple sclerosis self-management interventions: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 809–823. [Google Scholar] [CrossRef]
- Alghamdi, S.M.; Barker, R.E.; Alsulayyim, A.S.S.; Alasmari, A.M.; Banya, W.A.S.; I Polkey, M.; Birring, S.S.; Hopkinson, N.S. Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: A systematic review and meta-analysis. Thorax 2020, 75, 855–863. [Google Scholar] [CrossRef]
- Heerema-Poelman, A.; Stuive, I.; Wempe, J.B. Adherence to a maintenance exercise program one year after pulmonary rehabilitation: What are the predictors of dropout? J. Cardiopulm. Rehabil. Prev. 2013, 33, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.T.; Hitchcock, J.; Schumann, C.; Wells, J.M.; Dransfield, M.T.; Bhatt, S.P. Determinants of successful completion of pulmonary rehabilitation in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 391. [Google Scholar]
- Selzler, A.-M.; Simmonds, L.; Rodgers, W.M.; Wong, E.Y.; Stickland, M.K. Pulmonary rehabilitation in chronic obstructive pulmonary disease: Predictors of program completion and success. COPD J. Chronic Obstr. Pulm. Dis. 2012, 9, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Juretic, M.; Hill, R.; Hicken, B.; Luptak, M.; Rupper, R.; Bair, B. Predictors of attrition in older users of a home-based monitoring and health information delivery system. Telemed. e-Health 2012, 18, 709–712. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.; Wright, E.; Mendella, L.; Anthonisen, N. Predictors of patient adherence to long-term home nebulizer therapy for COPD. Chest 1995, 108, 394–400. [Google Scholar] [CrossRef]
- Milner, S.C.; Bourbeau, J.; Ahmed, S.; Janaudis-Ferreira, T. Improving acceptance and uptake of pulmonary rehabilitation after acute exacerbation of COPD: Acceptability, feasibility, and safety of a PR “taster” session delivered before hospital discharge. Chronic Respir. Dis. 2019, 16, 1479973119872517. [Google Scholar] [CrossRef] [Green Version]
- Antoniades, N.C.; Rochford, P.D.; Pretto, J.J.; Pierce, R.J.; Gogler, J.; Steinkrug, J.; Sharpe, K.; McDonald, C.F. Pilot study of remote telemonitoring in COPD. Telemed. e-Health 2012, 18, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Berkhof, F.F.; Berg, J.W.V.D.; Uil, S.M.; Kerstjens, H.A. Telemedicine, the effect of nurse-initiated telephone follow up, on health status and health-care utilization in COPD patients: A randomized trial. Respirology 2015, 20, 279–285. [Google Scholar] [CrossRef] [Green Version]
- Calvo, G.S.; Gómez-Suárez, C.; Soriano, J.; Zamora, E.; Gónzalez-Gamarra, A.; González-Béjar, M.; Jordán, A.; Tadeo, E.; Sebastián, A.; Fernández, G.; et al. A home telehealth program for patients with severe COPD: The PROMETE study. Respir. Med. 2014, 108, 453–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cameron-Tucker, H.L.; Wood-Baker, R.; Joseph, L.; Walters, J.A.; Schüz, N.; Walters, E.H. A randomized controlled trial of telephone-mentoring with home-based walking preceding rehabilitation in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 1991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chau, J.P.-C.; Lee, D.T.-F.; Yu, D.S.-F.; Chow, A.Y.-M.; Yu, W.-C.; Chair, S.-Y.; Lai, A.S.; Chick, Y.-L. A feasibility study to investigate the acceptability and potential effectiveness of a telecare service for older people with chronic obstructive pulmonary disease. Int. J. Med. Inform. 2012, 81, 674–682. [Google Scholar] [CrossRef]
- De San Miguel, K.; Smith, J.; Lewin, G. Telehealth remote monitoring for community-dwelling older adults with chronic obstructive pulmonary disease. Telemed. e-Health 2013, 19, 652–657. [Google Scholar] [CrossRef]
- Dinesen, B.; Haesum, L.K.; Soerensen, N.; Nielsen, C.; Grann, O.; Hejlesen, O.; Toft, E.; Ehlers, L. Using preventive home monitoring to reduce hospital admission rates and reduce costs: A case study of telehealth among chronic obstructive pulmonary disease patients. J. Telemed. Telecare 2012, 18, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Farmer, A.; Williams, V.; Velardo, C.; Shah, S.A.; Yu, L.-M.; Rutter, H.; Jones, L.; Williams, N.; Heneghan, C.; Price, J.; et al. Self-management support using a digital health system compared with usual care for chronic obstructive pulmonary disease: Randomized controlled trial. J. Med. Internet Res. 2017, 19, e144. [Google Scholar] [CrossRef] [Green Version]
- Halpin, D.M.G.; Laing-Morton, T.; Spedding, S.; Levy, M.L.; Coyle, P.; Lewis, J.; Newbold, P.; Marno, P. A randomised controlled trial of the effect of automated interactive calling combined with a health risk forecast on frequency and severity of exacerbations of COPD assessed clinically and using EXACT PRO. Prim. Care Respir. J. 2011, 20, 324–331. [Google Scholar] [CrossRef]
- Ho, T.-W.; Huang, C.-T.; Chiu, H.-C.; Ruan, S.-Y.; Tsai, Y.-J.; Yu, C.-J.; Lai, F. Effectiveness of telemonitoring in patients with chronic obstructive pulmonary disease in Taiwan—A randomized controlled trial. Sci. Rep. 2016, 6, 23797. [Google Scholar] [CrossRef] [Green Version]
- Jakobsen, A.S.; Laursen, L.C.; Rydahl-Hansen, S.; Østergaard, B.; Gerds, T.A.; Emme, C.; Schou, L.H.; Phanareth, K. Home-Based telehealth hospitalization for exacerbation of chronic obstructive pulmonary disease: Findings from “The Virtual Hospital” trial. Telemed. e-Health 2015, 21, 364–373. [Google Scholar] [CrossRef] [Green Version]
- Koff, P.; Jones, R.H.; Cashman, J.M.; Voelkel, N.F.; Vandivier, R. Proactive integrated care improves quality of life in patients with COPD. Eur. Respir. J. 2009, 33, 1031–1038. [Google Scholar] [CrossRef] [Green Version]
- Lewis, K.E.; Annandale, J.A.; Warm, D.L.; Rees, S.E.; Hurlin, C.; Blyth, H.; Syed, Y.; Lewis, L. Does home telemonitoring after pulmonary rehabilitation reduce healthcare use in optimized COPD?? A pilot randomized trial. COPD J. Chronic Obstr. Pulm. Dis. 2011, 7, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Lilholt, P.H.; Udsen, F.W.; Ehlers, L.; Hejlesen, O.K. Telehealthcare for patients suffering from chronic obstructive pulmonary disease: Effects on health-related quality of life: Results from the Danish ‘TeleCare North’ cluster-randomised trial. BMJ Open 2017, 7, e014587. [Google Scholar] [CrossRef] [PubMed]
- McDowell, J.E.; McClean, S.; FitzGibbon, F.; Tate, S. A randomised clinical trial of the effectiveness of home-based health care with telemonitoring in patients with COPD. J. Telemed. Telecare 2015, 21, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Nield, M.; Hoo, G.W.S. Real-time telehealth for COPD self-management using Skype™. COPD J. Chronic Obstr. Pulm. Dis. 2012, 9, 611–619. [Google Scholar] [CrossRef]
- Pedone, C.; Chiurco, D.; Scarlata, S.; Incalzi, R.A. Efficacy of multiparametric telemonitoring on respiratory outcomes in elderly people with COPD: A randomized controlled trial. BMC Heal Serv. Res. 2013, 13, 82. [Google Scholar] [CrossRef] [Green Version]
- Pinnock, H.; Hanley, J.; McCloughan, L.; Todd, A.; Krishan, A.; Lewis, S.; Stoddart, A.; Van Der Pol, M.; MacNee, W.; Sheikh, A.; et al. Effectiveness of telemonitoring integrated into existing clinical services on hospital admission for exacerbation of chronic obstructive pulmonary disease: Researcher blind, multicentre, randomised controlled trial. BMJ 2013, 347, f6070. [Google Scholar] [CrossRef] [Green Version]
- Ringbæk, T.; Green, A.; Laursen, L.C.; Frausing, E.; Brøndum, E.; Ulrik, C.S. Effect of telehealth care on exacerbations and hospital admissions in patients with chronic obstructive pulmonary disease: A randomized clinical trial. Int. J. Chronic Obstr. Pulm. Dis. 2015, 10, 1801. [Google Scholar]
- Ringbaek, T.J.; Lavesen, M.; Lange, P. Tablet computers to support outpatient pulmonary rehabilitation in patients with COPD. Eur. Clin. Respir. J. 2016, 3, 31016. [Google Scholar] [CrossRef]
- Schou, L.; Østergaard, B.; Rydahl-Hansen, S.; Rasmussen, L.S.; Emme, C.; Jakobsen, A.S.; Phanareth, K. A randomised trial of telemedicine-based treatment versus conventional hospitalisation in patients with severe copd and exacerbation–effect on self-reported outcome. J. Telemed. Telecare 2013, 19, 160–165. [Google Scholar] [CrossRef]
- Shany, T.; Hession, M.; Pryce, D.; Roberts, M.; Basilakis, J.; Redmond, S.; Lovell, N.; Schreier, G. A small-scale randomised controlled trial of home telemonitoring in patients with severe chronic obstructive pulmonary disease. J. Telemed. Telecare 2017, 23, 650–656. [Google Scholar] [CrossRef]
- Stickland, M.K.; Jourdain, T.; Wong, E.Y.; Rodgers, W.M.; Jendzjowsky, N.G.; Macdonald, G.F. Using Telehealth technology to deliver pulmonary rehabilitation to patients with chronic obstructive pulmonary disease. Can. Respir. J. 2011, 18, 216–220. [Google Scholar] [CrossRef]
- Trappenburg, J.C.; Niesink, A.; Oene, G.H.D.W.-V.; Van Der Zeijden, H.; Van Snippenburg, R.; Peters, A.; Lammers, J.-W.J.; Schrijvers, A.J. Effects of telemonitoring in patients with chronic obstructive pulmonary disease. Telemed. e-Health 2008, 14, 138–146. [Google Scholar] [CrossRef]
- Tsai, L.L.Y.; McNamara, R.J.; Moddel, C.; Alison, J.A.; McKenzie, D.K.; McKeough, Z.J. Home-based telerehabilitation via real-time videoconferencing improves endurance exercise capacity in patients with COPD: The randomized controlled TeleR Study. Respirology 2017, 22, 699–707. [Google Scholar] [CrossRef] [Green Version]
- Vianello, A.; Fusello, M.; Gubian, L.; Rinaldo, C.; Dario, C.; Concas, A.; Saccavini, C.; Battistella, L.; Pellizzon, G.; Zanardi, G.; et al. Home telemonitoring for patients with acute exacerbation of chronic obstructive pulmonary disease: A randomized controlled trial. BMC Pulm. Med. 2016, 16. [Google Scholar] [CrossRef] [Green Version]
- Al-Samarraie, H.; Ghazal, S.; Alzahrani, A.I.; Moody, L. Telemedicine in middle eastern countries: Progress, barriers, and policy recommendations. Int. J. Med. Inform. 2020, 141, 104232. [Google Scholar] [CrossRef]
- Poenaru, C.; Poenaru, E.; Vinereanu, D. Current perception of Telemedicine in an EU Country. Maedica 2014, 9, 367–374. [Google Scholar]
- Huang, B.; De Vore, D.; Chirinos, C.; Wolf, J.; Low, D.; Willard-Grace, R.; Tsao, S.; Garvey, C.; Donesky, D.; Su, G.; et al. Strategies for recruitment and retention of underrepresented populations with chronic obstructive pulmonary disease for a clinical trial. BMC Med. Res. Methodol. 2019, 19, 39. [Google Scholar] [CrossRef] [PubMed]
- Irving, S.Y.; Curley, M.A. Challenges to conducting multicenter clinical research: Ten points to consider. AACN Adv. Crit. Care 2008, 19, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, M.T.; Sousa, C.S.; Morais-Almeida, M.; Simões, M.J.; Mendes, P. Telemedicine in COPD: An overview by topics. COPD J. Chronic Obstr. Pulm. Dis. 2020, 17, 601–617. [Google Scholar] [CrossRef]
- Fan, K.G.; Mandel, J.; Agnihotri, P.; Tai-Seale, M. Remote patient monitoring technologies for predicting chronic obstructive pulmonary disease exacerbations: Review and comparison. JMIR mHealth uHealth 2020, 8, e16147. [Google Scholar] [CrossRef] [PubMed]
- Watson, N.L.; Heffner, J.L.; Mull, K.E.; McClure, J.B.; Bricker, J.B. Comparing treatment acceptability and 12-month cessation rates in response to web-based smoking interventions among smokers who do and do not screen positive for affective disorders: Secondary analysis. J. Med. Internet Res. 2019, 21, e13500. [Google Scholar] [CrossRef] [PubMed]
- Naughton, F.; Jamison, J.; Boase, S.; Sloan, M.; Gilbert, H.; Prevost, A.T.; Mason, D.; Smith, S.; Brimicombe, J.; Evans, R.; et al. Randomized controlled trial to assess the short-term effectiveness of tailored web-and text-based facilitation of smoking cessation in primary care (i Quit in Practice). Addiction 2014, 109, 1184–1193. [Google Scholar] [CrossRef] [Green Version]
- Early, F.; Wellwood, I.; Kuhn, I.; Deaton, C.; Fuld, J. Interventions to increase referral and uptake to pulmonary rehabilitation in people with COPD: A systematic review. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 3571–3586. [Google Scholar] [CrossRef] [Green Version]
- Dixon, L.J.; Linardon, J. A systematic review and meta-analysis of dropout rates from dialectical behaviour therapy in randomized controlled trials. Cogn. Behav. Ther. 2020, 49, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Alwashmi, M.F.; Fitzpatrick, B.; Farrell, J.; Gamble, J.-M.; Davis, E.; Van Nguyen, H.; Farrell, G.; Hawboldt, J. Perceptions of patients regarding mobile health interventions for the management of chronic obstructive pulmonary disease: Mixed methods study. JMIR mHealth uHealth 2020, 8, e17409. [Google Scholar] [CrossRef]
- Alrajeh, A.M.; Aldabayan, Y.S.; Aldhahir, A.; Pickett, E.; Quaderi, S.A.; Alqahtani, J.S.; Lipman, M.; Hurst, J.R. Global use, utility, and methods of tele-health in COPD: A health care provider survey. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 1713–1719. [Google Scholar] [CrossRef] [Green Version]
- Al Rajeh, A.; Steiner, M.C.; Aldabayan, Y.; Aldhahir, A.; Pickett, E.; Quaderi, S.; Hurst, J.R. Use, utility and methods of telehealth for patients with COPD in England and Wales: A healthcare provider survey. BMJ Open Respir. Res. 2019, 6. [Google Scholar] [CrossRef] [Green Version]
- Gaveikaite, V.; Grundstrom, C.; Winter, S.; Chouvarda, I.; Maglaveras, N.; Priori, R. A systematic map and in-depth review of European telehealth interventions efficacy for chronic obstructive pulmonary disease. Respir. Med. 2019, 158, 78–88. [Google Scholar] [CrossRef]
- Wedzicha, J.A.; Miravitlles, M.; Hurst, J.R.; Calverley, P.M.; Albert, R.K.; Anzueto, A.; Criner, G.J.; Papi, A.; Rabe, K.F.; Rigau, D.; et al. Management of COPD exacerbations: A European respiratory society/American thoracic society guideline. Eur. Respir. J. 2017, 49, 1600791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopkinson, N.S.; Molyneux, A.; Pink, J.; Harrisingh, M.C. Chronic obstructive pulmonary disease: Diagnosis and management: Summary of updated NICE guidance. BMJ 2019, 366, l4486. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE) Guideline. Chronic Obstructive Pulmonary Disease in Over 16s: Diagnosis and Management. 2018. Available online: nice.org.uk/guidance/ng115 (accessed on 19 October 2020).
- Dunphy, E.; Gardner, E.C. Telerehabilitation to Address the rehabilitation gap in anterior cruciate ligament care: Survey of patients. JMIR Form. Res. 2020, 4, e19296. [Google Scholar] [CrossRef] [PubMed]
- Loeckx, M.; A Rabinovich, R.; Demeyer, H.; Louvaris, Z.; Tanner, R.; Rubio, N.; Frei, A.; De Jong, C.; Gimeno-Santos, E.; Rodrigues, F.M.; et al. Smartphone-based physical activity telecoaching in chronic obstructive pulmonary disease: Mixed-methods study on patient experiences and lessons for implementation. JMIR mHealth uHealth 2018, 6, e200. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Factors | Number of Studies (%) | TH Acceptance Rate (Mean ± SD) | TH Dropout Rate (Mean ± SD) |
|---|---|---|---|
| Trial-related factors | |||
| Place of the study | |||
| Europe | 18 (65%) | 82% ± 14% | 19% ± 14% |
| Non-Europe | 9 (35%) | 76% ± 14% | 19% ± 16% |
| Study design | |||
| Randomized clinical trial | 24 (88%) | 81% ± 14% | 18% ± 14% |
| Non-Randomized clinical trial | 3 (12%) | 77% ± 18% | 27% ± 14% |
| Recruitment location | |||
| One location | 21 (78%) | 79% ± 14% | 20% ± 14% |
| More than one | 6 (22%) | 83% ± 19% | 16% ± 19% |
| Sociodemographic factors | |||
| COPD status at recruitment | |||
| Stable | 18 (65%) | 80% ± 16% | 19% ± 16% |
| Non-stable | 9 (35%) | 81% ± 12% | 18% ± 12% |
| Smoking history | |||
| Yes | 18 (65%) | 82% ±14% | 17% ± 14% |
| No | 9 (35%) | 76% ±16% | 23% ± 15% |
| Age | |||
| <69 | 5 (18%) | 83% ± 10% | 16% ± 10% |
| ≥69 | 22(81%) | 80% ± 15% | 20% ± 15% |
| Intervention-related factors | |||
| Telehealth component (s) | |||
| One component | 7 (25%) | 78% ± 18% | 21% ± 18% |
| More than one | 20 (75%) | 81% ± 13% | 18% ± 13% |
| Methods of delivery | |||
| Web-based | 14 (51%) | 78% ± 17% | 21% ± 17% |
| Other | 13 (49%) | 82% ± 13% | 17% ± 13% |
| Interactive display | |||
| Interactive | 14 (51%) | 78% ± 17% | 21% ± 17% |
| Not interactive | 13 (49%) | 83% ± 11% | 16% ± 11% |
| Frequency of TH | |||
| Daily | 18 (65%) | 81% ± 16% | 18% ± 16% |
| Weekly | 9 (35%) | 78% ± 12% | 21% ± 12% |
| Duration of TH | |||
| 20 weeks or less | 11 (40%) | 86% ± 12% | 14% ± 12% |
| More than 20 weeks | 16 (60%) | 77% ± 12% | 23% ± 12% |
| Overall Rates | Weighted (Estimation) | S.E. | p-Value | 95% CIs |
|---|---|---|---|---|
| Acceptance rate in TH | 51% | 0.2 | <0.001 | 49% to 52% |
| Acceptance rate in control | 49% | 0.3 | <0.001 | 48% to 51% |
| Dropout rate in TH | 63% | 0.2 | <0.001 | 60% to 67% |
| Dropout rate in control | 37% | 0.3 | <0.001 | 33% to 40% |
| Dropout Reasons | Number of Patients (%) |
|---|---|
| TH-related reasons | |
| Technical difficulties | 122 (24%) |
| Complicated system | 117 (23%) |
| Time constraints | 9 (2%) |
| Individual-related reasons | |
| Hospital admission | 138 (27%) |
| Deceased | 68 (13%) |
| Not interested in continuing | 45 (9%) |
| Moved from the study location | 14 (3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alghamdi, S.M.; Rajah, A.M.A.; Aldabayan, Y.S.; Aldhahir, A.M.; Alqahtani, J.S.; Alzahrani, A.A. Chronic Obstructive Pulmonary Disease Patients’ Acceptance in E-Health Clinical Trials. Int. J. Environ. Res. Public Health 2021, 18, 5230. https://doi.org/10.3390/ijerph18105230
Alghamdi SM, Rajah AMA, Aldabayan YS, Aldhahir AM, Alqahtani JS, Alzahrani AA. Chronic Obstructive Pulmonary Disease Patients’ Acceptance in E-Health Clinical Trials. International Journal of Environmental Research and Public Health. 2021; 18(10):5230. https://doi.org/10.3390/ijerph18105230
Chicago/Turabian StyleAlghamdi, Saeed M., Ahmed M. Al Rajah, Yousef S. Aldabayan, Abdulelah M. Aldhahir, Jaber S. Alqahtani, and Abdulaziz A. Alzahrani. 2021. "Chronic Obstructive Pulmonary Disease Patients’ Acceptance in E-Health Clinical Trials" International Journal of Environmental Research and Public Health 18, no. 10: 5230. https://doi.org/10.3390/ijerph18105230