
Survival and Characteristics of Bladder Cancer: Analysis of the Malaysian National Cancer Registry

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Study Design
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
3.1. Characteristics
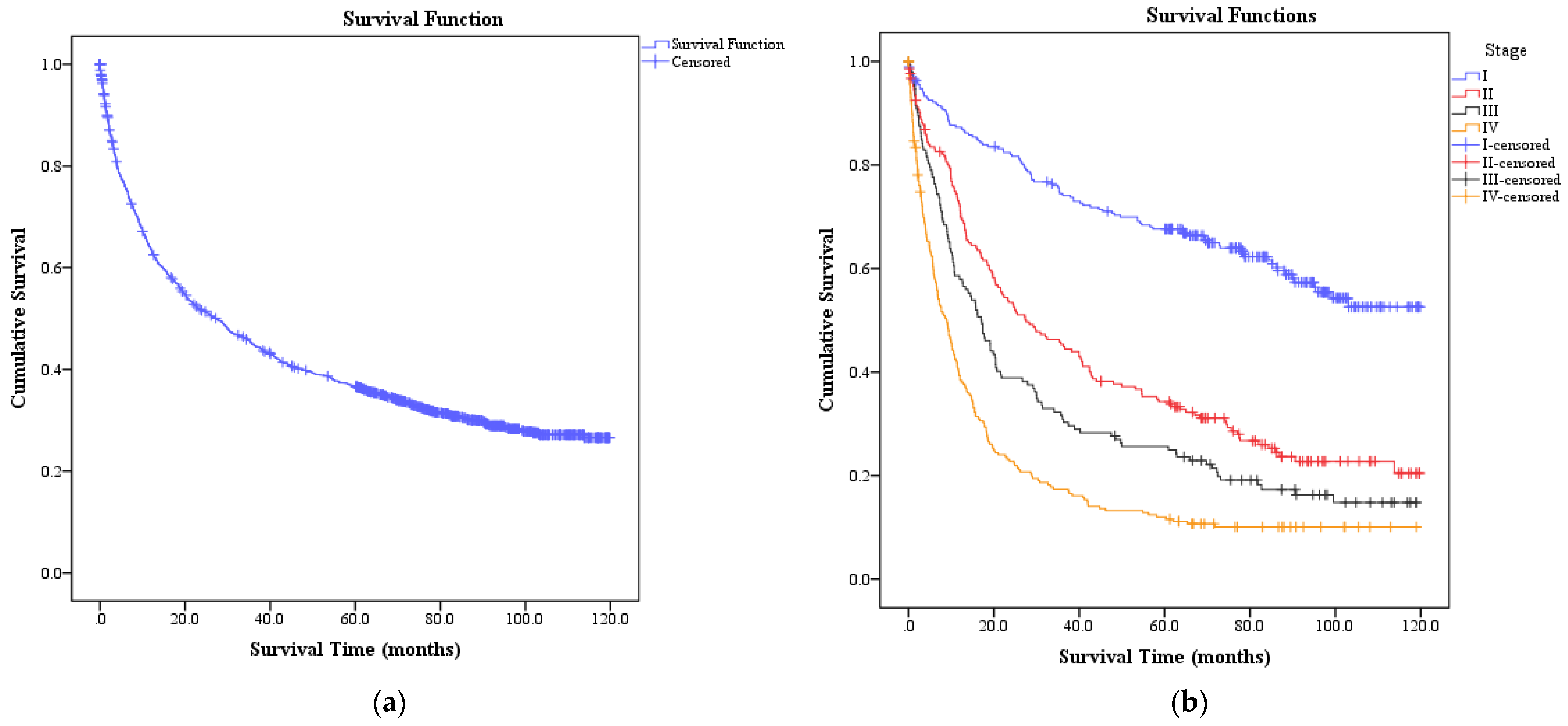
3.2. Five-Year Observed Survival
3.3. Median Survival Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Noone, A.; Howlader, N.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M. SEER Cancer Statistics Review, 1975–2015; Based on November 2017 SEER Data Submission, Posted to the SEER Web Site, April 2018; National Cancer Institute: Bethesda, MD, USA, 2018.
- Nielsen, M.E.; Smith, A.B.; Meyer, A.-M.; Kuo, T.-M.; Tyree, S.; Kim, W.Y.; Milowsky, M.I.; Pruthi, R.S.; Millikan, R.C. Trends in stage-specific incidence rates for urothelial carcinoma of the bladder in the United States: 1988 to 2006. Cancer 2014, 120, 86–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joung, J.Y.; Lim, J.; Oh, C.-M.; Jung, K.-W.; Cho, H.; Kim, S.H.; Seo, H.K.; Park, W.S.; Chung, J.; Lee, K.H.; et al. Current Trends in the Incidence and Survival Rate of Urological Cancers in Korea. Cancer Res. Treat. 2017, 49, 607–615. [Google Scholar] [CrossRef] [Green Version]
- Department of Statistics Malaysia. Press Release Population Projection (Revised), Malaysia, 2010–2040; Department of Statistics: Putrajaya, Malaysia, 2016. Available online: https://www.dosm.gov.my/v1/index.php?r=column/cthemeByCat&cat=118&bul_id=Y3kwU2tSNVFDOWp1YmtZYnhUeVBEdz09&menu_id=L0pheU43NWJwRWVSZklWdzQ4TlhUUT09 (accessed on 15 March 2019).
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur. Urol. 2017, 71, 96–108. [Google Scholar] [CrossRef]
- Ploeg, M.; Aben, K.K.; Hulsbergen-van de Kaa, C.A.; Schoenberg, M.P.; Witjes, J.A.; Kiemeney, L.A. Clinical Epidemiology of Nonurothelial Bladder Cancer: Analysis of The Netherlands Cancer Registry. J. Urol. 2010, 183, 915–920. [Google Scholar] [CrossRef] [PubMed]
- Royce, T.J.; Lin, C.C.; Gray, P.J.; Shipley, W.U.; Jemal, A.; Efstathiou, J.A. Clinical characteristics and outcomes of nonurothelial cell carcinoma of the bladder: Results from the National Cancer Data Base. Urol. Oncol. Semin. Orig. Investig. 2018, 36, 78.e1–78.e12. [Google Scholar] [CrossRef]
- Kong, C.H.C.; Singam, P.; Hong, G.E.; Cheok, L.B.; Azrif, M.; Tamil, A.M.; Zainuddin, Z.M. Clinicopathological features of bladder tumours in a single institution in Malaysia. Asian Pac. J. Cancer Prev. 2010, 11, 149–152. [Google Scholar]
- Singapore Cancer Registry. Singapore Cancer Registry Cancer Survival in Singapore 1973–2012; National Registry of Diseases Office, Ministry of Health: Singapore, 2015. Available online: https://www.nrdo.gov.sg/publications/cancer (accessed on 7 October 2018).
- Zaitsu, M.; Toyokawa, S.; Tonooka, A.; Nakamura, F.; Takeuchi, T.; Homma, Y.; Kobayashi, Y. Sex differences in bladder cancer pathology and survival: Analysis of a population-based cancer registry. Cancer Med. 2015, 4, 363–370. [Google Scholar] [CrossRef]
- Belgian Cancer Registry. Cancer Survival in Belgium; Belgian Cancer Registry: Brussel, Belgium, 2012; Available online: http://www.kankerregister.org/media/docs/publications/CancerSurvivalinBelgium.PDF (accessed on 24 September 2018).
- ISD Scotland. Cancer Survival in Scotland 1987–2011; Information Services Division (ISD), NHS Scotland: Scotland, UK, 2015; Available online: https://www.isdscotland.org/Health-Topics/Cancer/Publications/2015-03-03/2015-03-03-CancerSurvival-Report.pdf? (accessed on 7 October 2018).
- Lund, L.; Erichsen, R.; Nørgaard, M.; Larsen, E.; Borre, M.; Jacobsen, J. Survival of invasive bladder cancer patients, 1998-2009; a central and northern Denmark population-based cohort study. Clin. Epidemiol. 2011, 3, 47–51. [Google Scholar] [CrossRef] [Green Version]
- Mokhtar, A.; Al Alawi, M.M.; Al Taweel, W.M.; Al Othman, K.; Kattan, S.A.; Al Otaibi, M.F. Is survival after radical cystectomy for bladder cancer in Saudi patients different from that of Western patients? Ann. Saudi Med. 2017, 37, 194–200. [Google Scholar] [CrossRef] [Green Version]
- Supit, W.; Mochtar, C.A.; Santoso, R.B.; Umbas, R. Outcomes of radical cystectomy and bladder preservation treatment for muscle-invasive urothelial carcinoma of the bladder. Asian J. Surg. 2014, 37, 184–189. [Google Scholar] [CrossRef] [Green Version]
- Vahedian-Ardakani, H.-A.; Moghimi, M.; Shayestehpour, M.; Doosti, M.; Alimohammadi, F. Survival Rate of Patients with Bladder Cancer in Yazd, Central Province of Iran. 2018. Available online: https://www.scopus.com/inward/record.uri?eid=2-s2.0-85048710356&doi=10.5812%2Fijcm.61436&partnerID=40&md5=f6daf89cf694d7e6ebafcebc489857c5 (accessed on 7 October 2018).
- Haque, W.; Verma, V.; Butler, E.B.; Teh, B.S. Radical Cystectomy Versus Chemoradiation for Muscle-invasive Bladder Cancer: Impact of Treatment Facility and Sociodemographics. Anticancer Res. 2017, 37, 5603–5608. [Google Scholar]
- Kozak, K.R.; Hamidi, M.; Manning, M.; Moody, J.S. Bladder preservation for localised muscle-invasive bladder cancer: The survival impact of local utilisation rates of definitive radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.B.; Deal, A.M.; Woods, M.E.; Wallen, E.M.; Pruthi, R.S.; Chen, R.C.; Milowsky, M.I.; Nielsen, M.E. Muscle-invasive bladder cancer: Evaluating treatment and survival in the National Cancer Data Base. BJU Int. 2014, 114, 719–726. [Google Scholar] [CrossRef]
- Zakaria, A.S.; Santos, F.; Kassouf, W.; Tanguay, S.; Aprikian, A. Survival after Radical Cystectomy for Bladder Cancer in Relation to Prior Non-Muscle Invasive Disease in Quebec. Urol. Int. 2016, 97, 49–53. [Google Scholar] [CrossRef]
- Fisher, M.D.; Shenolikar, R.; Miller, P.J.; Fenton, M.; Walker, M.S. Treatment Patterns and Outcomes in Stage IV Bladder Cancer in a Community Oncology Setting: 2008–2015. Clin. Genitourin. Cancer 2018, 16, e1171–e1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flannery, K.; Cao, X.; He, J.; Zhong, Y.; Shah, A.Y.; Kamat, A.M. Survival Rates and Health Care Costs for Patients With Advanced Bladder Cancer Treated and Untreated With Chemotherapy. Clin. Genitourin. Cancer 2018, 16, e909–e917. [Google Scholar] [CrossRef] [Green Version]
- Haque, W.; Verma, V.; Butler, E.B.; Teh, B.S. National Practice Patterns and Outcomes for T4b Urothelial Cancer of the Bladder. Clin. Genitourin. Cancer 2018, 16, 42–49.e1. [Google Scholar] [CrossRef]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global surveillance of trends in cancer survival 2000–2014 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Institute Ministry of Health Malaysia. Malaysian Study on Cancer Survival (MySCan); National Cancer Institute Ministry of Health Malaysia: Putrajaya, Malaysia, 2018. Available online: http://nci.moh.gov.my/index.php/ms/main-menu-2/laporan (accessed on 7 October 2018).
- Roubaud, G.; Brouste, V.; Beuzeboc, P.; Fléchon, A.; Tosi, D.; Lavau-Denes, S.; Chevreau, C.; Culine, S.; Oudard, S.; Quivy, A.; et al. Early objective response may not be a prognostic factor of survival for patients with metastatic urothelial carcinoma: From a retrospective analysis of a cohort of 113 patients. J. Negat. Results Biomed. 2015, 14, 1–7. [Google Scholar] [CrossRef]
- Krause, F.S.; Walter, B.; Ott, O.J.; Häberle, L.; Weiss, C.; Rödel, C.; Wullich, B.; Sauer, R. 15-Year Survival Rates After Transurethral Resection and Radiochemotherapy or Radiation in Bladder Cancer Treatment. Anticancer Res. 2011, 31, 985–990. [Google Scholar]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keck, B.; Ott, O.J.; Häberle, L.; Kunath, F.; Weiss, C.; Rödel, C.; Sauer, R.; Fietkau, R.; Wullich, B.; Krause, F.S. Female sex is an independent risk factor for reduced overall survival in bladder cancer patients treated by transurethral resection and radio- or radiochemotherapy. World J. Urol. 2013, 31, 1023–1028. [Google Scholar] [CrossRef]
- Cumberbatch, M.G.K.; Noon, A.P. Epidemiology, aetiology and screening of bladder cancer. Transl. Androl. Urol. 2019, 8, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Dobruch, J.; Daneshmand, S.; Fisch, M.; Lotan, Y.; Noon, A.P.; Resnick, M.J.; Shariat, S.F.; Zlotta, A.R.; Boorjian, S.A. Gender and Bladder Cancer: A Collaborative Review of Etiology, Biology, and Outcomes. Eur. Urol. 2016, 69, 300–310. [Google Scholar] [CrossRef] [PubMed]
- Rose, T.L.; Deal, A.M.; Nielsen, M.E.; Smith, A.B.; Milowsky, M.I. Sex disparities in use of chemotherapy and survival in patients with advanced bladder cancer. Cancer 2016, 122, 2012–2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minicozzi, P.; Innos, K.; Sánchez, M.J.; Trama, A.; Walsh, P.M.; Marcos-Gragera, R.; Dimitrova, N.; Botta, L.; Visser, O.; Rossi, S.; et al. Quality analysis of population-based information on cancer stage at diagnosis across Europe, with presentation of stage-specific cancer survival estimates: A EUROCARE-5 study. Eur. J. Cancer 2017, 84, 335–353. [Google Scholar] [CrossRef]
- Andreassen, B.K.; Aagnes, B.; Gislefoss, R.; Andreassen, M.; Wahlqvist, R. Incidence and Survival of urothelial carcinoma of the urinary bladder in Norway 1981–2014. BMC Cancer 2016, 16, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, M.I.; Bang, A.; Gillett, D.; Cheluvappa, R.; Smith, D.P. Poor survival of females with bladder cancer is limited to those aged 70 years or over: A population-wide linkage study, New South Wales, Australia. Cancer Med. 2015, 4, 1145–1152. [Google Scholar] [CrossRef] [Green Version]
- Marcos-Gragera, R.; Mallone, S.; Kiemeney, L.A.; Vilardell, L.; Malats, N.; Allory, Y.; Sant, M.; Hackl, M.; Zielonke, N.; Oberaigner, W.; et al. Urinary tract cancer survival in Europe 1999–2007: Results of the population-based study EUROCARE-5. Eur. J. Cancer 2015, 51, 2217–2230. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | n (%) |
|---|---|
| Age (mean, SD) | 64.9 (12.5) |
| Sex | |
| Male | 1438 (78.7) |
| Female | 390 (21.3) |
| Ethnicity | |
| Malay | 903 (49.4) |
| Chinese | 684 (37.4) |
| Indian | 107 (5.9) |
| Iban | 36 (2.0) |
| Kadazan | 17 (0.9) |
| Others | 81 (4.4) |
| Morphology | |
| Urothelial carcinoma | 1430 (78.2) |
| Squamous cell carcinoma | 57 (3.1) |
| Adenocarcinoma | 150 (8.2) |
| Sarcoma | 10 (0.6) |
| Others | 7 (0.4) |
| Nonspecific | 174 (9.5) |
| Stage | |
| I | 270 (14.8) |
| II | 216 (11.8) |
| III | 153 (8.4) |
| IV | 250 (13.7) |
| Unrecorded | 939 (51.4) |
| Surgery | |
| Yes | 902 (49.3) |
| No | 297 (16.3) |
| Unrecorded | 629 (34.4) |
| Radiotherapy | |
| Yes | 221 (12.1) |
| No | 573 (31.3) |
| Unrecorded | 1034 (56.6) |
| Chemotherapy | |
| Yes | 191 (10.5) |
| No | 587 (32.1) |
| Unrecorded | 1050 (57.4) |
| Stage | Five-Year Survival % (95% CI) | Median Survival Time Months (95% CI) |
|---|---|---|
| I | 67.6 (62.0, 73.3) | - |
| II | 34.3 (27.9, 40.8) | 27.6 (18.1, 37.0) |
| III | 25.7 (18.7, 32.6) | 17.0 (13.3, 20.7) |
| IV | 12.2 (8.1, 16.3) | 8.8 (7.0, 10.7) |
| Unrecorded | 36.9 (33.7, 40.1) | 29.3 (23.5, 31.0) |
| All | 36.9% (95% CI: 34.6, 39.1) | 27.3 (23.6, 31.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nik Ab Kadir, M.N.; Mohd Hairon, S.; Yaacob, N.M.; Ab Manan, A.; Ali, N. Survival and Characteristics of Bladder Cancer: Analysis of the Malaysian National Cancer Registry. Int. J. Environ. Res. Public Health 2021, 18, 5237. https://doi.org/10.3390/ijerph18105237
Nik Ab Kadir MN, Mohd Hairon S, Yaacob NM, Ab Manan A, Ali N. Survival and Characteristics of Bladder Cancer: Analysis of the Malaysian National Cancer Registry. International Journal of Environmental Research and Public Health. 2021; 18(10):5237. https://doi.org/10.3390/ijerph18105237
Chicago/Turabian StyleNik Ab Kadir, Mohd Nasrullah, Suhaily Mohd Hairon, Najib Majdi Yaacob, Azizah Ab Manan, and Nabihah Ali. 2021. "Survival and Characteristics of Bladder Cancer: Analysis of the Malaysian National Cancer Registry" International Journal of Environmental Research and Public Health 18, no. 10: 5237. https://doi.org/10.3390/ijerph18105237