



Obsessive–compulsive personality disorder (OCPD) and obsessive–compulsive disorder (OCD) can be considered as OCD spectrum disorders given their similarities in multiple factors such as symptom profiles, inheritance in families, and a similar response to selective serotonin reuptake inhibitors (Fineberg, Saxena, Zohar, & Craig, Reference Fineberg, Saxena, Zohar and Craig2007; Hollander, Kim, Braun, Simeon, & Zohar, Reference Hollander, Kim, Braun, Simeon and Zohar2009; Phillips et al., Reference Phillips, Stein, Rauch, Hollander, Fallon, Barsky and Leckman2010). From an etiological perspective, these similarities may be understood from a shared underlying liability (De Caluwé, Rettew, & De Clercq, Reference De Caluwé, Rettew and De Clercq2014) that is potentially genetically driven (Maina, Albert, Salvi, Pessina, & Bogetto, Reference Maina, Albert, Salvi, Pessina and Bogetto2008) and might include common neurobiological underpinnings between both disorders (Hollander et al., Reference Hollander, Kim, Braun, Simeon and Zohar2009). One candidate phenotypic representation of this shared underlying dispositional tendency is perfectionism, since both disorders seem to be substantially related to this psychological feature (for a review, see Egan, Wade, & Shafran, Reference Egan, Wade and Shafran2011). Yet, studies considering childhood perfectionism, its development and outcome in view of understanding the occurrence of both disorders, are still lacking.
OCPD is characterized by “the preoccupation with orderliness, perfectionism, and mental and interpersonal control, at the expense of flexibility, openness, and efficiency” (American Psychiatric Association [APA], 2013, p. 723). The role of perfectionism is crucial in case of OCPD, which is reflected in the current OCPD Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria requiring the trait “rigid perfectionism” to be present beyond at least two of the following three other OCPD traits: perseveration, intimacy avoidance, and restricted affectivity (APA, 2013, pp. 768–769). Hence, the fifth edition of DSM (DSM-5) highlights perfectionism as an essential and necessary feature of OCPD, whereas other features may be either present or absent. Despite the fact that the association between OCPD and perfectionism is clear, studies exploring the role of perfectionism as a potential childhood antecedent of OCPD are still lacking.
OCD is defined in DSM-5 as “a disorder that is characterized by the presence of obsessions and/or compulsions”. Further, “obsessions are recurrent and persistent thoughts, urges, or images that are experienced as intrusive and unwanted, whereas compulsions are repetitive behaviors or mental acts that an individual feels driven to perform in response to an obsession or according to rules that must be applied rigidly” (APA, 2013, p. 235). OCD is characterized by various dysfunctional beliefs, such as “an inflated sense of responsibility and the tendency to overestimate threat; perfectionism and intolerance of uncertainty; and over-importance of thoughts and the need to control thoughts” (APA, 2013, p. 238). Further, there is a “distressing sense of ‘incompleteness’ or uneasiness until things look, feel, or sound ‘just right’” (APA, 2013, p. 239), also reflecting the presence of perfectionism in these individuals. However, perfectionism has not yet been empirically considered as potential childhood antecedent for OCD psychopathology and such consideration was only stated at a conceptual level (see Janet, Reference Janet1903; Kagan, Reznick, & Snidman, Reference Kagan, Reznick and Snidman1987).
Perfectionism is a multidimensional construct (Frost, Heimberg, Holt, Mattia, & Neubauer, Reference Frost, Heimberg, Holt, Mattia and Neubauer1993; Frost, Marten, Lahart, & Rosenblate, Reference Frost, Marten, Lahart and Rosenblate1990; Hewitt & Flett, Reference Hewitt and Flett1991; cf. below) and cross-sectional studies have shown that these multidimensional perfectionism scores – and especially the socially prescribed subdimension (i.e., others putting pressure on a person to be perfect) – are associated with adult OCPD (Hewitt, Flett, & Turnbull, Reference Hewitt, Flett and Turnbull1992; Iketani et al., Reference Iketani, Kiriike, Stein, Nagao, Nagata, Minamikawa and Fukuhara2002; Stoeber, Reference Stoeber2014) and OCD (Antony, Purdon, Huta, & Swinson, Reference Antony, Purdon, Huta and Swinson1998; Buhlmann, Etcoff, & Wilhelm, Reference Buhlmann, Etcoff and Wilhelm2008; Frost & Steketee, Reference Frost and Steketee1997; Frost, Steketee, Cohn, & Griess, Reference Frost, Steketee, Cohn and Griess1994; Sassaroli et al., Reference Sassaroli, Lauro, Ruggiero, Mauri, Vinai and Frost2008). Although the relevance of perfectionism for both OCPD and OCD is established cross-sectionally in adults and conceptually acknowledged at a taxonomic level (i.e., in DSM-5), empirical evidence on the relative significance of perfectionism for understanding the clinical richness of both disorders shows some inconsistence. For instance, Halmi et al. (Reference Halmi, Tozzi, Thornton, Crow, Fichter, Kaplan and Bulik2005) found that two perfectionism dimensions, namely concerns over mistakes and doubts about actions, were better predictors of OCPD compared to OCD. Conversely, some researchers emphasized the role of these perfectionism dimensions as a unique predictor of OCD instead of OCPD (Frost, Novara, & Rhéaume, Reference Frost, Novara, Rhéaume, Frost and Steketee2002). From a developmental perspective, it can be argued that exploring the predictive value of childhood perfectionism for both OCPD and OCD outcomes may shed a new light on this debate and contribute to our knowledge on the unique versus shared importance of perfectionism in the etiology of both disorders.
The Structure and Measurement of Childhood Perfectionism
It is generally accepted that perfectionism is already present during childhood and adolescence (Flett & Hewitt, Reference Flett, Hewitt, Flett and Hewitt2002; Hewitt et al., Reference Hewitt, Caelian, Flett, Sherry, Collins and Flynn2002). At a trait level, perfectionism can be situated at the high end of conscientiousness and neuroticism (Flett & Hewitt, Reference Flett and Hewitt2007; for a review see Smith et al., Reference Smith, Sherry, Vidovic, Saklofske, Stoeber and Benoit2019). Flett, Hewitt, Oliver, and Macdonald (Reference Flett, Hewitt, Oliver and Macdonald2002) suggested that perfectionism develops along transactional processes between multiple etiological factors, including parenting and other socialization factors, and childhood temperament. Perfectionism is mostly conceptualized as a multidimensional construct (Hewitt, Flett, & Mikail, Reference Hewitt, Flett and Mikail2017). Studies have identified two dimensions of childhood perfectionism: self-oriented perfectionism versus socially prescribed perfectionism (measured by the Children–Adolescent Perfectionism Scale; CAPS; Flett et al., Reference Flett, Hewitt, Besser, Su, Vaillancourt, Boucher and Gale2016). However, when a three-factor approach is followed (McCreary, Joiner, Schmidt, & Ialongo, Reference McCreary, Joiner, Schmidt and Ialongo2004; O'Connor, Dixon, & Rasmussen, Reference O'Connor, Dixon and Rasmussen2009), the following dimensions appear: self-oriented striving, self-oriented critical, and socially prescribed. The self-oriented perfectionism dimension (including the striving and critical subcomponents) is characterized by setting extreme standards to oneself while also evaluating the performance of oneself stringently. It is considered as an “extreme form of compulsive striving or hyper-conscientiousness” in which individuals also give extreme importance to attaining perfection (Hewitt et al., Reference Hewitt, Flett and Mikail2017; Hill, Reference Hill2017). Items asking about individuals’ extreme standards tap into a self-oriented striving aspect, whereas items asking about self-criticism tap into a self-oriented criticism aspect (McCreary et al., Reference McCreary, Joiner, Schmidt and Ialongo2004; O'Connor et al., Reference O'Connor, Dixon and Rasmussen2009). Further, socially prescribed perfectionism refers to the degree of the belief that significant others set unrealistic standards for the person and evaluate him or her harshly, also by using pressure (Hewitt & Flett, Reference Hewitt and Flett1991). Socially prescribed perfectionism is generally considered as a maladaptive feature, whereas there is an ongoing debate regarding the adaptiveness/maladaptiveness of the self-oriented perfectionism dimension (see Hill, Reference Hill2014, Reference Hill2017; Stoeber & Otto, Reference Stoeber and Otto2006).
Perfectionism in childhood has also been conceptualized from the widely accepted Five-Factor Model perspective (De Clercq, De Fruyt, & Widiger, Reference De Clercq, De Fruyt and Widiger2009) along the age-specific maladaptive Dimensional Personality Symptom Item Pool (DIPSI) taxonomy (De Clercq, De Fruyt, & Mervielde, Reference De Clercq, De Fruyt and Mervielde2003; De Clercq, De Fruyt, Van Leeuwen, & Mervielde, Reference De Clercq, De Fruyt, Van Leeuwen and Mervielde2006). Based upon stringent empirical strategies, the DIPSI conceptualizes “perfectionism” as one of the facets of the higher-order compulsivity domain in children. Based on a comparison of the items, it could be suggested that DIPSI perfectionism aligns with self-oriented perfectionism (in particular the striving items).
The Development of Childhood Perfectionism
Overall, studies investigating the development of perfectionism have focused on etiological factors of self-oriented and socially prescribed perfectionism dimensions, such as parental influences (Damian, Stoeber, Negru, & Băban, Reference Damian, Stoeber, Negru and Băban2013) or dispositional liabilities (Stoeber, Otto, & Dalbert, Reference Stoeber, Otto and Dalbert2009). In contrast, less is known about mean-level trajectories of perfectionism itself, with only two studies explicitly focusing on the developmental trajectories of perfectionism in childhood/adolescent samples (i.e., Herman, Wang, Trotter, Reinke, & Ialongo, Reference Herman, Wang, Trotter, Reinke and Ialongo2013; Hong et al., Reference Hong, Lee, Chng, Zhou, Tsai and Tan2017). These studies investigated mean-level changes in the self-oriented critical and socially prescribed dimensions and found multiple developmental trajectories that were overall defined as increasing, decreasing or stable (Herman et al., Reference Herman, Wang, Trotter, Reinke and Ialongo2013; Hong et al., Reference Hong, Lee, Chng, Zhou, Tsai and Tan2017).
Relying on latent growth curve analysis, Hong et al. (Reference Hong, Lee, Chng, Zhou, Tsai and Tan2017) focused on the developmental trajectories of self-oriented critical and socially prescribed dimensions of perfectionism in a sample of 8-year-old children up until the age of 11 and identified six different trajectories: “high increasing”, “high decreasing”, “low increasing”, and “low stable” trajectories for the self-oriented critical perfectionism dimension as well as the “high decreasing” and “low stable” trajectories for the socially prescribed perfectionism dimension.
Herman et al. (Reference Herman, Wang, Trotter, Reinke and Ialongo2013) investigated the developmental trajectories of the same two perfectionism dimensions in African American adolescents, and also identified statistically significant variability in starting points and growth rates of adolescents for both self-oriented critical and socially prescribed perfectionism dimensions, overall structured in “high”, “decreasing”, “increasing”, and “low” developmental pathways for each of the perfectionism dimensions.
The Present Study
Corroborating this existing evidence, this study aimed to contribute the research field of perfectionism development in different ways. First, the present study used an age-sensitive maladaptive trait operationalization of perfectionism that has been empirically constructed and validated across childhood and adolescence as part of an omnibus measure of maladaptive trait pathology (DIPSI; De Clercq et al., Reference De Clercq, De Fruyt, Van Leeuwen and Mervielde2006) The DIPSI perfectionism construct resembles the self-oriented perfectionism dimension (and in particular the striving component). This perspective may add to the literature that mainly explored developmental trajectories of self-oriented critical and socially prescribed dimensions, but did not include the self-oriented striving perfectionism dimension in their designs.
Second, in the current study we based our hypothesis on the changes that have been reported for higher-order personality constructs measured by the DIPSI (De Clercq, Van Leeuwen, Van den Noortgate, De Bolle, & De Fruyt, Reference De Clercq, Van Leeuwen, Van den Noortgate, De Bolle and De Fruyt2009; De Clercq, Verbeke, De Caluwé, Vercruysse, & Hofmans, Reference De Clercq, Verbeke, De Caluwé, Vercruysse and Hofmans2017). The established findings on decreases in childhood maladaptive personality traits – including disagreeableness, emotional instability/neuroticism oddity, and compulsivity – were conceptually explained by normative maturation and socialization processes throughout childhood and adolescence. Of particular relevance for the current study, is the normative declining course of the higher-order trait domain of compulsivity, because the DIPSI perfectionism construct is a core compulsivity facet. Therefore, we expected to observe a similar overall declining trend for perfectionism from childhood through adolescence.
Third, the present study included starting levels and the rates of change in DIPSI perfectionism as a predictor of both adolescent OCPD and OCD. The idea that childhood perfectionism and its development could predict both OCPD and OCD outcomes in adolescence is in line with the idea of Cicchetti and Rogosch (Reference Cicchetti and Rogosch1996), indicating that multiple pathological outcomes could be predicted by the same vulnerability. The significance of perfectionism in multiple psychopathologies (Egan et al., Reference Egan, Wade and Shafran2011) supports its shared role for leading or contributing to various pathological outcomes. It is at this point plausible to expect that perfectionism will most strongly predict the components of OCPD and OCD that are conceptually closest to DIPSI childhood perfectionism. Therefore, among all the adolescent OCPD traits (i.e., rigid perfectionism, perseveration, intimacy avoidance and restricted affectivity), we expected adolescent rigid perfectionism to be the OCPD trait that is the strongest associated with childhood perfectionism. Further, among all the 10 OCD symptom facets and three higher-order OCD symptom domains that were investigated, we expected the adolescent perfectionism facet as well as the order/clean/perfect domain of OCD to demonstrate the strongest associations with childhood perfectionism. Although the potential value of childhood perfectionism in the prediction of both OCPD and OCD pathologies later in life is clear, only a limited number of longitudinal studies investigated the potential outcomes or correlates of the change in self-oriented perfectionism in general (i.e., not making the distinction between the critical and striving subcomponents) or socially prescribed perfectionism. Although these studies used various well-being and psychopathology variables, they did not yet include OCPD and OCD as potential outcome variables (Damian et al., Reference Damian, Stoeber, Negru and Băban2013; Herman et al., Reference Herman, Wang, Trotter, Reinke and Ialongo2013; Hong et al., Reference Hong, Lee, Chng, Zhou, Tsai and Tan2017; Levine, Green-Demers, Werner, & Milyavskaya, Reference Levine, Green-Demers, Werner and Milyavskaya2019; Nilsson, Sundbom, & Hägglöf, Reference Nilsson, Sundbom and Hägglöf2008; O'Connor et al., Reference O'Connor, Dixon and Rasmussen2009; Soenens et al., Reference Soenens, Luyckx, Vansteenkiste, Luyten, Duriez and Goossens2008; Stoeber et al., Reference Stoeber, Otto and Dalbert2009).
Aims and Hypotheses
To summarize, the present study investigated the baseline, growth and outcomes of childhood perfectionism. More specifically, developmental trajectories of childhood DIPSI perfectionism were investigated using latent growth curve analysis. Further, the outcomes of these baseline trajectories regarding OCPD traits and OCD symptoms in adolescence were examined. The first research aim was to explore how mean-level trajectories of childhood perfectionism occur over time. Based on the normative maturation hypothesis by Roberts, Walton, and Viechtbauer (Reference Roberts, Walton and Viechtbauer2006) and the evidence for decreasing trends in higher-order maladaptive DIPSI traits in other studies (De Clercq, Van Leeuwen et al., Reference De Clercq, Van Leeuwen, Van den Noortgate, De Bolle and De Fruyt2009; De Clercq et al., Reference De Clercq, Verbeke, De Caluwé, Vercruysse and Hofmans2017), we expected a general decline in perfectionism (Hypothesis 1). The second research aim was to investigate to what extent childhood perfectionism is a shared versus a unique predictor for OCPD traits and OCD symptoms, thereby exploring the multifinality principle (Cicchetti & Rogosch, Reference Cicchetti and Rogosch1996). Previous research has indicated cross-sectional associations between general multidimensional perfectionism and socially prescribed perfectionism scores with OCPD (Hewitt et al., Reference Hewitt, Flett and Turnbull1992; Iketani et al., Reference Iketani, Kiriike, Stein, Nagao, Nagata, Minamikawa and Fukuhara2002; Stoeber, Reference Stoeber2014) and OCD (Antony et al., Reference Antony, Purdon, Huta and Swinson1998; Buhlmann et al., Reference Buhlmann, Etcoff and Wilhelm2008; Frost & Steketee, Reference Frost and Steketee1997; Frost et al., Reference Frost, Steketee, Cohn and Griess1994; Sassaroli et al., Reference Sassaroli, Lauro, Ruggiero, Mauri, Vinai and Frost2008). Based on this, we expected that childhood perfectionism would predict both OCPD traits and OCD symptoms (Hypothesis 2). Finally, we expected the strongest predictions for the OCPD rigid perfectionism trait, the OCD order/clean/perfect domain (compared to the obsessive and compulsive domains), and the OCD perfectionism facet (compared to the other nine facets) because of their conceptual similarity to the DIPSI perfectionism predictor (Hypothesis 3).
Method
Participants and procedure
Children were recruited by psychology undergraduates of Ghent University (Belgium) in the course of the Personality and Affect Longitudinal Study (PALS; De Caluwé, De Clercq, De Bolle, & De Wolf, Reference De Caluwé, De Clecq, De Bolle and De Wolf2014). To maximize the variability in symptom scores, the sample was a mixed sample (N = 485, 55.5% girls, 7.17–14.78 years old, Mage = 10.74, SD = 1.50) of community (n = 339) and referred children (n = 146). With 1-year intervals, three waves of data were collected. Four to six years after the first wave, a fourth follow up was organized (n = 344, 61% girls, 12–20 years old, Mage = 16.06, SD = 1.76). In this last wave, families were rewarded for their efforts by an unannounced 5-euro voucher. Participants were informed that confidentiality was guaranteed, and that the data would only be used for research purposes. All participants provided written informed consent and the study was approved by the Ghent University Ethical Review Board (protocol number 2012/01).
Community sample
Flemish-speaking children between 8 and 14 years old were recruited by students. Students from Ghent University live all-around Flanders and this ensured some geographical distribution of our participants. Intellectual disability and physical constraint or disabilities were set as exclusion criteria. Families received the necessary information including aims, procedure, and ethics of the study during home visits, which were made by the students. Each child completed the questionnaires independently from their mother in a separate room. Students were told that they should not assist participants. They were only allowed to explain the meaning of the items or words if the child or mother asked for clarification. This community subsample from PALS started with 339 children at Wave 1 (56.9% girls, Mage = 10.69, SD = 1.34) with still 243 adolescents (63.7% girls, Mage = 16.45, SD = 1.60) in Wave 4 (i.e., 72% of the initial sample). The ages of the mothers at Wave 1 ranged from 29.17 to 56 years old (Mage = 40.81, SD = 4.37). The mothers indicated their highest education levels as primary education (1.2%), special primary education (.3%), lower vocational secondary education (2.4%), lower technical secondary education (2.4%), lower general secondary education (1.2%), higher vocational secondary education (9.4%), higher technical secondary education (13.6%), higher general secondary education (10.6%), special secondary education (.3%) higher nonuniversity education (41.3%), university education (15.9%), and other (1.2%), with one person's information not available. The age of the children did not predict the dropouts for adolescents, F (1, 337) = 0.48, p = .49; however, there were significant gender differences between the individuals who continued and the ones who did not, indicating that girls were more likely to dropout than boys, F (1, 337) = 15.09, p = .001. Moreover, children who dropped out also had slightly lower academic achievement levels, Welch F (1, 125.19) = 8.39, p < .01 followed by lower levels of socioeconomic status (SES) of mothers, F (1, 323) = 12.35, p < .01 and fathers, F (1, 329) = 5.05, p < .05.
Referred sample
This sample was recruited using an online directory coming from registered primary health care services in Flanders. In this sample, all children were registered to a mental program or waiting to be registered after intake and screening. Similar exclusion criteria as with the community sample were used. There were no further specifications required for symptomatology, hence a sample with various emotional and behavioral problems was targeted. Junior undergraduate psychology students made calls to psychologists in the health care services and informed them about the aims, procedure, and ethics of the present study. In order to guarantee randomization, psychologists asked the first families on their appointment schedules to participate to the study. Those families who agreed received a consent form, information letter, and questionnaires. In the next appointment, they brought back the signed consent forms with completed questionnaires in a sealed envelope. At the first wave of the study, this referred subsample of PALS consisted of 146 children (52.1% girls, Mage = 10.87, SD = 1.84). Seventy one percent of these children were receiving a treatment at that moment while 75% were registered for the first time to the mental health services. Main referral reasons were anxiety symptomatology (20.7%), depressive symptomatology (14.5%), grief or emotional problems as a result of parental divorce (11.3%), behavioral difficulties (10.7%), personality pathology or identity issues (7.6%), developmental disorders (6.9%), psychosomatic complaints (6.3.0%), learning difficulties (5.0%), social problems (3.8%), attention or concentration problems (2.5%), sleep problems (1.9%), eating problems (1.3%), and self-injury (0.6%). The referral reason was not available for the remaining 6.9%. In Wave 4, 101 adolescents (55% girls, Mage = 15.14 years, SD = 1.79) continued their participation (i.e., 69%). Ages of the mothers from the referred sample in Wave 1 ranged from 26.70 to 57.16 years old (Mage = 40.29, SD = 5.26). The mothers indicated their highest education levels as follows: pre-school education (1.4%), primary education (.7%), special primary education (1.4%), lower vocational secondary education (3.4%), lower technical secondary education (4.1%), lower general secondary education (2.7%), higher vocational secondary education (11.6%), higher technical secondary education (14.4%), higher general secondary education (9.6%), special secondary education (.7%), higher nonuniversity education (37.7%), university education (8.2%) and other (3.4%), with one person's information not available. No significant differences were found between the group of individuals who continued and the ones who dropped out regarding age, F (1, 144) = 0.00, p = .99, gender, F (1, 144) = 1.50, p = .22, academic achievement, Welch F (1, 56.68) = 3.66, p = .06, and SES of fathers, F (1, 137) = 3.48, p = .06 and SES of mothers, F (1, 116) = 0.85, p = .36.
Measures
Dimensional personality symptom item pool (DIPSI)
Across the first three waves, mothers completed the DIPSI (De Clercq et al., Reference De Clercq, De Fruyt, Van Leeuwen and Mervielde2006) to describe children's maladaptive personality traits. The DIPSI consists of 172 items that are rated on a 5-point Likert scale with answering options ranging from 1 (not characteristic) to 5 (highly characteristic). It contains four higher-order domains, which are emotional instability, introversion, disagreeableness, and compulsivity. These domains comprise 27 lower-order facets, with perfectionism as one of the four facets of the compulsivity domain. This perfectionism facet consists of the following items: “Wants life to be perfectly organized”, “Devotes too much of him/herself to tasks”, “Finds it important to do all things perfectly”, “Always makes detailed plans when doing something”, “Loses a lot of time trying to be perfect”. The DIPSI demonstrated a clear factor structure, high reliability, and validity (De Clercq, Van Leeuwen, De Fruyt, Van Hiel, & Mervielde, Reference De Clercq, Van Leeuwen, De Fruyt, Van Hiel and Mervielde2008; De Clercq et al., Reference De Clercq, De Fruyt, Van Leeuwen and Mervielde2006). In the present study, perfectionism showed reliability beyond the acceptable levels – that is .70 (Nunally & Bernstein, Reference Nunally and Bernstein1994), across the three waves as indicated by the Cronbach's αs of .78 (Wave 1), .77 (Wave 2) and .81 (Wave 3).
Personality inventory for DSM-5 (PID-5)
In the fourth wave, adolescents completed the Dutch version of the PID-5 (De Clercq et al., Reference De Clercq, De Fruyt, De Bolle, Van Hiel, Markon and Krueger2014), originally developed to describe maladaptive personality traits (Krueger, Derringer, Markon, Watson, & Skodol, Reference Krueger, Derringer, Markon, Watson and Skodol2012) according to DSM-5 section III (APA, 2013). The PID-5 has 220 items rated on a 4-point rating scale, ranging from very false (0) to very true (3). Items are structured in 25 facets and further clustered into five higher-order domains, defined as negative affectivity, detachment, antagonism, disinhibition, and psychoticism. In order to diagnose OCPD, DSM-5 suggests that the maladaptive personality trait “rigid perfectionism” must be present in addition to at least two of the following traits: perseveration, intimacy avoidance and restricted affectivity. Hence, DSM-5 highlights these four maladaptive personality traits as being the core of OCPD. The PID-5 was originally developed for adult populations, but acceptable psychometric features and a similar factor structure were also found in community (De Clercq et al., Reference De Clercq, De Fruyt, De Bolle, Van Hiel, Markon and Krueger2014) and referred adolescent samples (De Caluwé, Verbeke, Van Aken, Van der Heijden, & De Clercq, Reference De Caluwé, Verbeke, Van Aken, Van der Heijden and De Clercq2019). In the present study, adolescent reports showed adequate Cronbach's αs ranging from .78 (intimacy avoidance) to .89 (rigid perfectionism), and an overall Cronbach α of .92 for the OCPD mean score.
Youth obsessive–compulsive symptoms scale (YOCSS)
In the fourth (i.e., the last) wave, adolescents completed the YOCSS (De Caluwé & De Clercq, Reference De Caluwé and De Clercq2014), a self-report measure for assessing youth OCD symptoms and impairment in an age-specific and dimensional way. The YOCSS has 68 items, rated on a 5-point Likert scale with answering options ranging from 1 (this is not at all typical for me) to 5 (this is very typical for me). Fifty-seven items measure the presence of OCD symptoms (total score), organized along 10 symptom facets (aggression, guilt, sensitivity to physical appearance, somatization, repeating, magic games, hoarding, orderliness, cleanliness, and perfectionism) that are hierarchically clustered in three symptom domains (obsessive, compulsive, and order/clean/perfect domains). Next to these 57 items, 11 separate items are used to calculate a total score for impairment associated with OCD symptoms. Previous research suggested that the YOCSS has acceptable to adequate reliability, as well as convergent and divergent validity (De Caluwé & De Clercq, Reference De Caluwé and De Clercq2014). In the current sample, alpha reliability coefficients were adequate both at the total symptoms level (Cronbach's α = .95), as well as at the domain level, with values of .95 for the obsessive domain, .90 for the order/clean/perfect domain and .89 for the compulsive domain. The Cronbach's αs of the 10 facets ranged between .75 (aggression facet) and .84 (magic games facet).
Statistical analyses
In a first step, three independent confirmatory factor analyses (CFAs) were conducted (i.e., one for each measurement wave) using Mplus version 7.0 (Muthén & Muthén, Reference Muthén and Muthén2012). In each of the CFAs, it was tested whether all five childhood DIPSI perfectionism items loaded on one latent perfectionism factor. The model fit was checked along two fit indices, which were the comparative fit index (CFI) and the root mean square error of approximation (RMSEA). The lower bound critical value for CFI was 0.90, with values of 0.95 indicating a good fit for the model (Kline, Reference Kline2015). The RMSEA upper bound is 0.10 in which values less than 0.08 indicate a satisfactory fit (Kline, Reference Kline2015). The chi-square (χ2) test statistic was not used as an index for informing the model fit or misfit given its sensitivity to sample size (Kline, Reference Kline2015). Therefore, it was reported, but not used for deciding on model fit or misfit in the present paper.
A prerequisite to examining growth is to establish measurement invariance of the construct of interest across time (i.e., DIPSI perfectionism). Therefore, in the initial step, it was examined whether the same factor configuration held for all three measurement points (configural invariance). In order to achieve that, a model with three latent perfectionism variables (one latent variable for each wave) was tested and all factor loadings were freely estimated. Moreover, covariances of the consequent waves were included in the model (i.e., the covariances of the same items between Wave 1 and 2 as well as between Wave 1 and 3, and between Wave 2 and 3) and latent factor scores were standardized in order to simplify the model by setting the residual variances of all three latent factors to 1 and intercepts to 0. In the following step, in order to test the metric invariance, factor loadings were set equal across waves. Consequently, to examine scalar invariance, intercepts of the same items were also set equal across waves. Following to each step of measurement invariance analyses, the χ2 difference tests were performed, and each test was adjusted according to the Satorra–Bentler scaling correction (Satorra & Bentler, Reference Satorra and Bentler2010). To evaluate model differences, ΔCFI (differences in the CFI values) should not exceed 0.010 and ΔRMSEA (differences in the RMSEA values) should not be larger than 0.015 (Chen, Reference Chen2007).
After measurement invariance was demonstrated, latent growth curve model parameters were added to this full invariant model. After the latent growth curve model was successfully established, the estimated latent growth factors (i.e., intercept and slope) were used to predict OCPD and OCD outcomes at different levels of the symptom hierarchy.
Results
The results of the three independent CFAs showed that a one-factor model fitted the data well across all three measurement occasions (χ2 = 11.10, df = 5, CFI = 0.986, RMSEA = 0.050 for Wave 1; χ2 = 7.95, df = 5, CFI = 0.991, RMSEA = 0.042 for Wave 2; χ2 = 14.86, df = 5, CFI = 0.971, RMSEA = 0.079 for Wave 3).
Next, it was tested whether the same factor configuration was present across the three waves (i.e., configural invariance). Therefore, all measurement occasions were included in the same CFA model simultaneously. All item loadings were freely estimated across three waves. In addition, the variance of the latent factors was set to 1 and the means of the latent factors were set to 0 in order to simplify the model (as a standardization method; Little, Reference Little2013). Moreover, the covariances between the items of the consequent waves were included in the model as well. This model resulted in acceptable levels of CFI and RMSEA fit values (χ2 = 242.19, df = 77, p < .001, CFI = 0.918, RMSEA = 0.067).
In the following step, the metric measurement invariance was tested by additionally setting the factor loadings equal across the three waves for the same items. Including these constraints to the model led to significant χ2 difference test results (Satorra–Bentler Scaled χ2 = 25.72, df = 10, p < .05). However, the ΔCFI did not exceed 0.010 and the ΔRMSEA was not larger than 0.015 (ΔCFI = 0.008, ΔRMSEA = 0.001). The model in this step also had acceptable CFI and RMSEA values (χ2 = 268.99, df = 87, p < .001, CFI = 0.910, RMSEA = 0.066), altogether reflecting metric measurement invariance.
In the last step of the measurement invariance analyses, scalar measurement invariance was tested by setting the intercept of the same items equal across all three waves. Adding these constraints to the previous model resulted in significant χ2 difference test results (Satorra–Bentler Scaled χ2 = 25.43, df = 9, p < .05). However, again, the ΔCFI did not exceed 0.010 and the ΔRMSEA was not larger than 0.015 (ΔCFI = 0.008, ΔRMSEA = 0.001). The model showed also acceptable levels of CFI and RMSEA values (χ2 = 294.94, df = 96, p < .001, CFI = 0.902, RMSEA = 0.065), altogether reflecting scalar measurement invariance. Overall, these results indicated that the measurement of perfectionism in the present study was fully invariant across the three waves, which enables the use of the latent growth curve model in the further analyses.
After full measurement invariance was achieved in the previous steps, latent growth curve modeling was applied to the model in order to test Hypothesis 1. The latent growth curve model had a good fit (χ2 = 6.42, df = 1, p < .05, CFI = 0.986). However, the RMSEA showed above threshold levels, but the confidence interval of the estimate was very wide (RMSEA = 0.106, 95% CI [0.040, 1.190]). Further inspection of the latent growth curve model revealed important characteristics of the developmental trajectories of childhood perfectionism. Individuals on average had a significant, though small, decrease in their perfectionism scores across time (mean slope = −0.050, p < .05). Moreover, the variance of the latent intercept was significant (s2 = 0.42, p < .001), indicating that there were significant individual differences among the participants in their levels of childhood DIPSI perfectionism at the first measurement point. However, the slope variance was not significant (s2 = 0.01, p = .549), meaning that there were no significant inter-individual differences in the decrease of perfectionism. After the latent growth curve model was established, only the latent intercept factor was used to predict the OCPD and the OCD symptom scores, since the variance estimate of the slope factor in the base latent growth curve model (model without the regressions) was not significant.
In order to test Hypotheses 2 and 3 of the present study, the two outcome variables (OCPD mean and OCD symptom mean) were regressed on the latent intercept factor of the latent growth curve model of childhood perfectionism (see Table 1). Since the variance of the slope factor of the base latent growth curve model was not significant, it was still estimated but constrained to .001 in these subsequent models in order to establish the growth model.
Table 1. Overview of standardized regression coefficients when regressing obsessive–compulsive personality disorder (OCPD) and obsessive–compulsive disorder (OCD) variables on intercept values from latent growth model for perfectionism
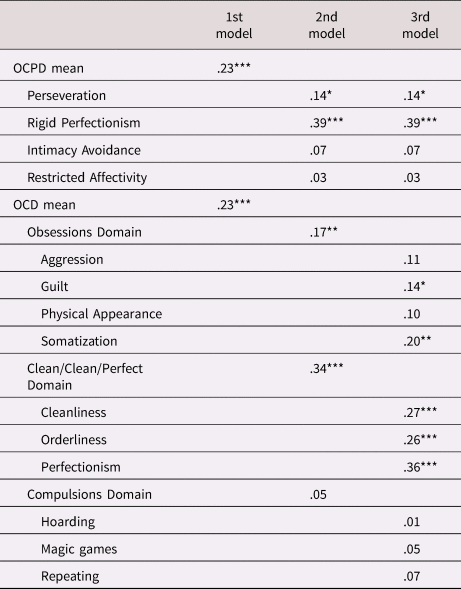
* p < .05. **p < .01. ***p < .001.
This model fitted the data well (χ2 = 12.04, df = 6, p = .06, CFI = 0.989, RMSEA = 0.046). The results of the regressions that included the intercept factor as the independent variable indicated that the individual differences in the starting levels (intercept) significantly predicted mean OCPD (β = 0.23, p < .001) and OCD scores (β = 0.23 p < .001). These two standardized regression coefficients were equal, indicating that higher levels of baseline childhood DIPSI perfectionism equally predicted OCPD traits and OCD symptoms in adolescence.
Further, to obtain a more detailed picture, the four OCPD traits and three OCD domains were entered in the model to be regressed on the latent intercept factor of childhood DIPSI perfectionism trajectories. This model also fitted the data well (χ2 = 21.75, df = 16, p = .15, CFI = 0.995, RMSEA = 0.027). Childhood DIPSI perfectionism predicted the adolescent rigid perfectionism trait best among all four OCPD traits (β = 0.39, p < .001). Moreover, differences in the initial childhood DIPSI perfectionism levels predicted the order/clean/perfect domain of the OCD symptoms best (β = 0.34, p < .001). These results were followed by childhood DIPSI perfectionism significantly predicting the OCD obsessions domain (β = 0.17 p < .01) and the OCPD trait perseveration (β = 0.14, p < .05). Interestingly, differences in initial DIPSI perfectionism levels in childhood did not predict the OCD compulsions domain in adolescence (β = 0.05, p = .35).
Besides the three higher-order OCD domains, we also focused on the 10 lower-order OCD facets. To examine which of the 10 OCD symptom facets could be predicted by childhood DIPSI perfectionism, the four OCPD traits and the 10 OCD facets were together regressed on the childhood DIPSI perfectionism latent intercept. The reason for including the four OCPD traits in this model was to achieve comparability between this model and the previous models we tested since those models also included OCPD scores. This model fitted the data well (χ2 = 44.72, df = 30, p = .04, CFI = 0.993, RMSEA = 0.03). Again, in this model the adolescent OCPD trait rigid perfectionism was the best predicted outcome trait by the variance in the initial childhood DIPSI perfectionism scores (β = 0.39, p < .001). The OCPD trait perseveration was also significantly predicted by childhood DIPSI perfectionism (β = 0.14, p < .01). Moreover, among all 10 OCD symptom facets, starting levels of childhood DIPSI perfectionism best predicted the adolescent perfectionism facet of OCD symptoms (β = 0.36, p < .001), which is slightly less compared to the adolescent rigid perfectionism OCPD trait (β = 0.39 p < .001). These results were followed by childhood DIPSI perfectionism starting scores significantly predicting the facets cleanliness (β = 0.27, p < .001) and orderliness (β = 0.26, p < .001) from the order/clean/perfect domain of the OCD symptoms as well as somatization (β = 0.20, p < .01) and guilt symptom facets (β = 0.14, p < .05) from the obsessions domain of the OCD symptoms. However, the five remaining facets of OCD symptoms (i.e., aggression, hoarding, magic games, repeating, and sensitivity to physical appearance) could not be predicted by baseline childhood DIPSI perfectionism.Footnote 1
Discussion
The current study aimed to investigate the baseline and growth of childhood DIPSI perfectionism in relation to OCPD traits and OCD symptomatology in adolescence. In the present research, we modeled mean levels and individual differences in starting points and growth rates of DIPSI perfectionism. No significant individual differences were observed in the slope of childhood DIPSI perfectionism decrease among the participants in the present data, but significant individual differences in starting positions of childhood DIPSI perfectionism were found and were used to predict the later OCPD and OCD outcomes.
Results showed that childhood DIPSI perfectionism overall decreases from middle childhood up until mid-adolescence. These results confirm our first hypothesis, indicating that established evidence on mean-level decreases of higher-order maladaptive traits from childhood through adolescence (De Clercq, Van Leeuwen et al., Reference De Clercq, Van Leeuwen, Van den Noortgate, De Bolle and De Fruyt2009; De Clercq et al., Reference De Clercq, Verbeke, De Caluwé, Vercruysse and Hofmans2017), translate towards the facet-level of personality pathology and can be extended toward the more specific facet of perfectionism. Beyond this overall decrease, no significant individual differences were observed in the rate of change in childhood DIPSI perfectionism. This nonsignificant slope variance indicates that the differences between participants in their change in DIPSI perfectionism followed a similar declining pattern. This finding contrasts with previous studies that observed individual differences in self-oriented critical and socially prescribed dimensions of multidimensional perfectionism (Herman et al., Reference Herman, Wang, Trotter, Reinke and Ialongo2013; Hong et al., Reference Hong, Lee, Chng, Zhou, Tsai and Tan2017). The differences between the present and previous results might be due to the fact that we focused on a different conceptualization of perfectionism. More specifically, the content of the DIPSI perfectionism items resembles the self-oriented perfectionism items from the CAPS (Flett et al., Reference Flett, Hewitt, Besser, Su, Vaillancourt, Boucher and Gale2016; McCreary et al., Reference McCreary, Joiner, Schmidt and Ialongo2004; O'Connor et al., Reference O'Connor, Dixon and Rasmussen2009) and particularly the striving subdimension, and hence differ from previous conceptualizations focusing on self-oriented critical and socially prescribed perfectionism.
Concerning our second hypothesis, significant individual differences were detected in starting positions in childhood DIPSI perfectionism levels that related to both the OCPD and OCD outcomes. The strengths of these associations were completely identical to each other. These results confirm our second hypothesis and provide evidence for the developmental principle of multifinality (Cicchetti & Rogosch, Reference Cicchetti and Rogosch1996), meaning that childhood perfectionism predicts multiple outcomes in adolescence – in this case, OCPD and OCD. However, these results also contradict previous findings, suggesting that various perfectionism dimensions, for instance concern over mistakes and doubt about actions, are more related to OCPD than OCD (Halmi et al., Reference Halmi, Tozzi, Thornton, Crow, Fichter, Kaplan and Bulik2005) or vice versa (Frost et al., Reference Frost, Novara, Rhéaume, Frost and Steketee2002). Most probably, the current results differ from previous ones because the current measure of perfectionism (the DIPSI) especially captures self-oriented striving aspects of perfectionism which are less related to concerns about mistakes and doubt about actions compared to socially prescribed perfectionism (Frost et al., Reference Frost, Heimberg, Holt, Mattia and Neubauer1993). All in all, our study found that, adolescent OCPD and OCD could be equally predicted by the individual differences in the initial levels of childhood perfectionism as measured by the DIPSI.
Finally, in line with our third hypothesis, we found that maternal rated childhood perfectionism most strongly predicted outcomes that are conceptually closest to the predictor variable, as reflected in the self-reported adolescent rigid perfectionism trait (from the OCPD traits) and the order/clean/perfect domain as well as the perfectionism facet (from the OCD symptoms).
In addition, baseline childhood perfectionism levels also positively predicted the OCPD perseveration trait as well as the OCD obsessions domain in adolescence. The most impairing aspect of OCD, namely the compulsions domain (De Caluwé et al., Reference De Caluwé, Rettew and De Clercq2014) could not be predicted by childhood perfectionism in the present study. These results indicate that DIPSI childhood perfectionism may not be a vulnerability factor for developing compulsions later in life, although it may contribute to the emergence of other OCD-related symptoms.
Besides these results, baseline DIPSI childhood perfectionism was also positively associated with the OCD cleanliness, orderliness, somatization, and guilt facets. These findings are in line with previous research in clinical (Calleo, Hart, Björgvinsson, & Stanley, Reference Calleo, Hart, Björgvinsson and Stanley2010; Tolin, Brady, & Hannan, Reference Tolin, Brady and Hannan2008; Wheaton, Abramowitz, Berman, Riemann, & Hale, Reference Wheaton, Abramowitz, Berman, Riemann and Hale2010) and nonclinical samples (Viar, Bilsky, Armstrong, & Olatunji, Reference Viar, Bilsky, Armstrong and Olatunji2011), indicating that higher scores on “perfectionism/certainty beliefs” as measured by the Obsessional-Beliefs Questionnaire (OBQ; Obsessive Compulsive Cognitions Working Group, 2005) were positively related to contamination (Viar et al., Reference Viar, Bilsky, Armstrong and Olatunji2011), ordering (Calleo et al., Reference Calleo, Hart, Björgvinsson and Stanley2010; Tolin et al., Reference Tolin, Brady and Hannan2008), and symmetry (Viar et al., Reference Viar, Bilsky, Armstrong and Olatunji2011; Wheaton et al., Reference Wheaton, Abramowitz, Berman, Riemann and Hale2010). Studies also found associations between “perfectionism cognitions” measured by The Perfectionism Cognitions Inventory (PCI; Flett, Hewitt, Whelan, & Martin, Reference Flett, Hewitt, Whelan and Martin2007) and psychosomatic symptoms (e.g., Flett, Molnar, Nepon, & Hewitt, Reference Flett, Molnar, Nepon and Hewitt2012). In addition to this established evidence, DIPSI childhood perfectionism also successfully predicted the presence of guilt-themed OCD obsession outcomes. This can be understood from the fact that guilt-related obsessions are inherently related to the mental focus on not repeating mistakes, preventing any possible future failures, and being prone to feelings of guilt, as captured by self-oriented perfectionism tendencies (Hewitt & Flett, Reference Hewitt and Flett1991; Hewitt et al., Reference Hewitt, Flett and Mikail2017). Our findings indicate at this point that the self-oriented perfectionistic aspect of guilt-related obsessions in adolescence can be traced back towards childhood.
An important clinical implication of the current results is that childhood perfectionism as measured by the DIPSI can be used to portray potential OCPD and OCD outcomes, and may constitute a practical measure for alerting clinical experts when they encounter highly perfectionistic children in their clinical practice. There is evidence at this point, showing that early interventions targeting the severity of perfectionism are helpful to decrease OCD-related symptoms (Lloyd, Schmidt, Khondoker, & Tchanturia, Reference Lloyd, Schmidt, Khondoker and Tchanturia2015). Moreover, it was also shown that preventing the increase of perfectionism in pre-adolescent populations is possible (Fairweather-Schmidt & Wade, Reference Fairweather-Schmidt and Wade2015). Combining the latter with the present results, it appears that early interventions during childhood that target decreases in DIPSI perfectionism could be effective to decrease the odds of developing OCPD traits and OCD symptoms later in life.
The current study also has some limitations. First, the present design did not include any baseline measurements for either OCPD or OCD variables (those were only measured in Wave 4). Moreover, our predictor and outcome measures were reported by different informants. Childhood perfectionism measure was rated by mothers, whereas the OCPD and OCD measures during adolescence were resulting from self-reports. However, this cross-informant design may allow to avoid any response bias and inflation of associations that could arise from single-informant designs. Second, future prospective studies should preferably use more than three measurement points to explore trajectories of perfectionism from childhood onwards. Such studies may also benefit from measuring children's baseline OCPD and OCD levels, since this will provide more clarity on whether children demonstrate increases on those variables from childhood through adolescence. Moreover, including control variables such as childhood neuroticism might help to show to what extent results of the present predictions could be attributed to childhood perfectionism as an early maladaptive trait beyond neuroticism levels.
All in all, our study showed a general decreasing perfectionism trend from childhood through adolescence, in line with normative maturation processes. Children with high scores on self-oriented (striving) perfectionism levels are generally seen more vulnerable for developing OCPD-related trait pathology and OCD symptomatology in adolescence, indicating that perfectionism is a shared though a-specific vulnerability factor for OCPD and OCD outcomes.
Conflicts of Interest
None
Funding Statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.


 Open access
Open access