
CFD Simulations of Radioembolization: A Proof-of-Concept Study on the Impact of the Hepatic Artery Tree Truncation

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients: Hepatic State and Radioembolization
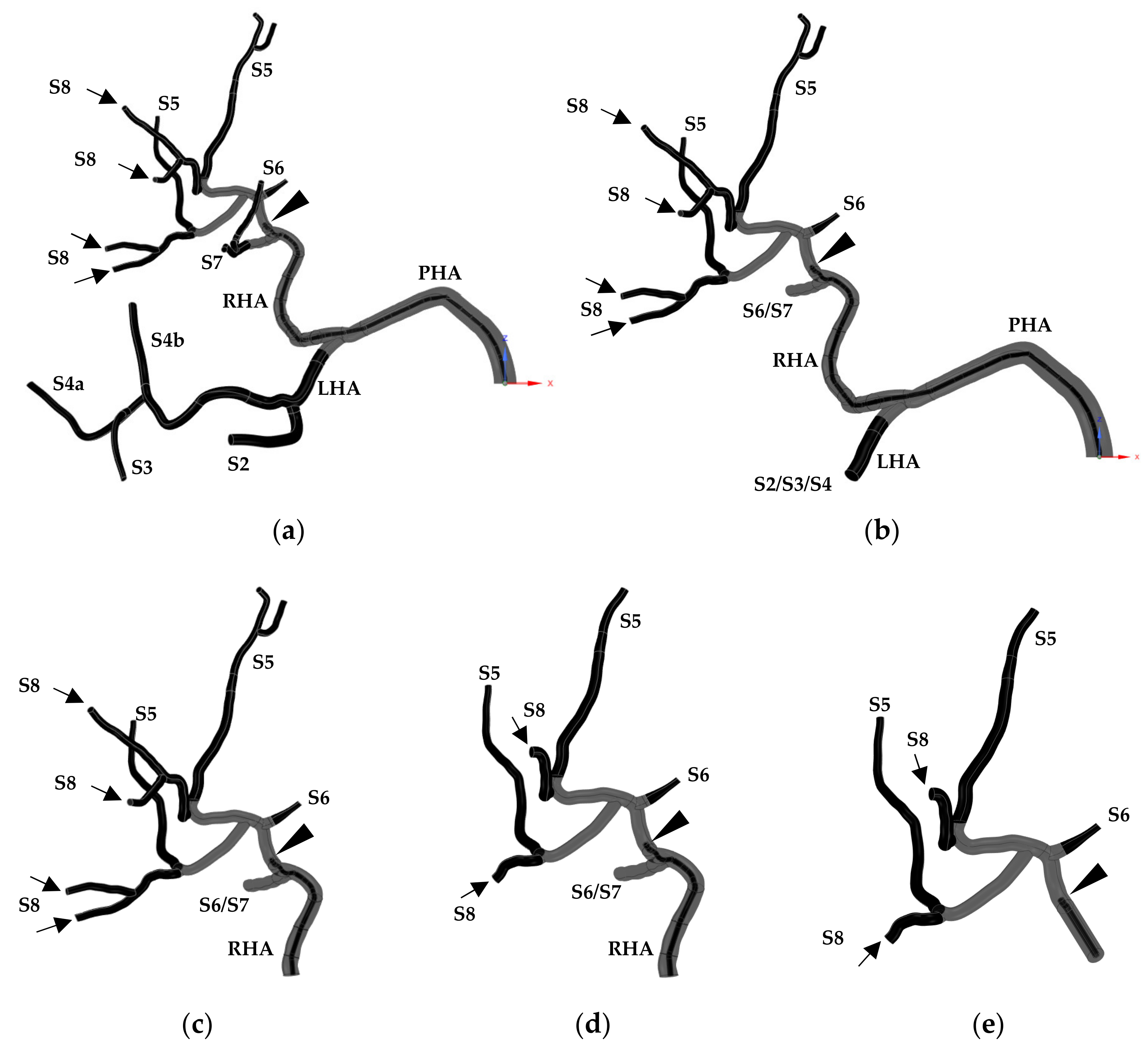
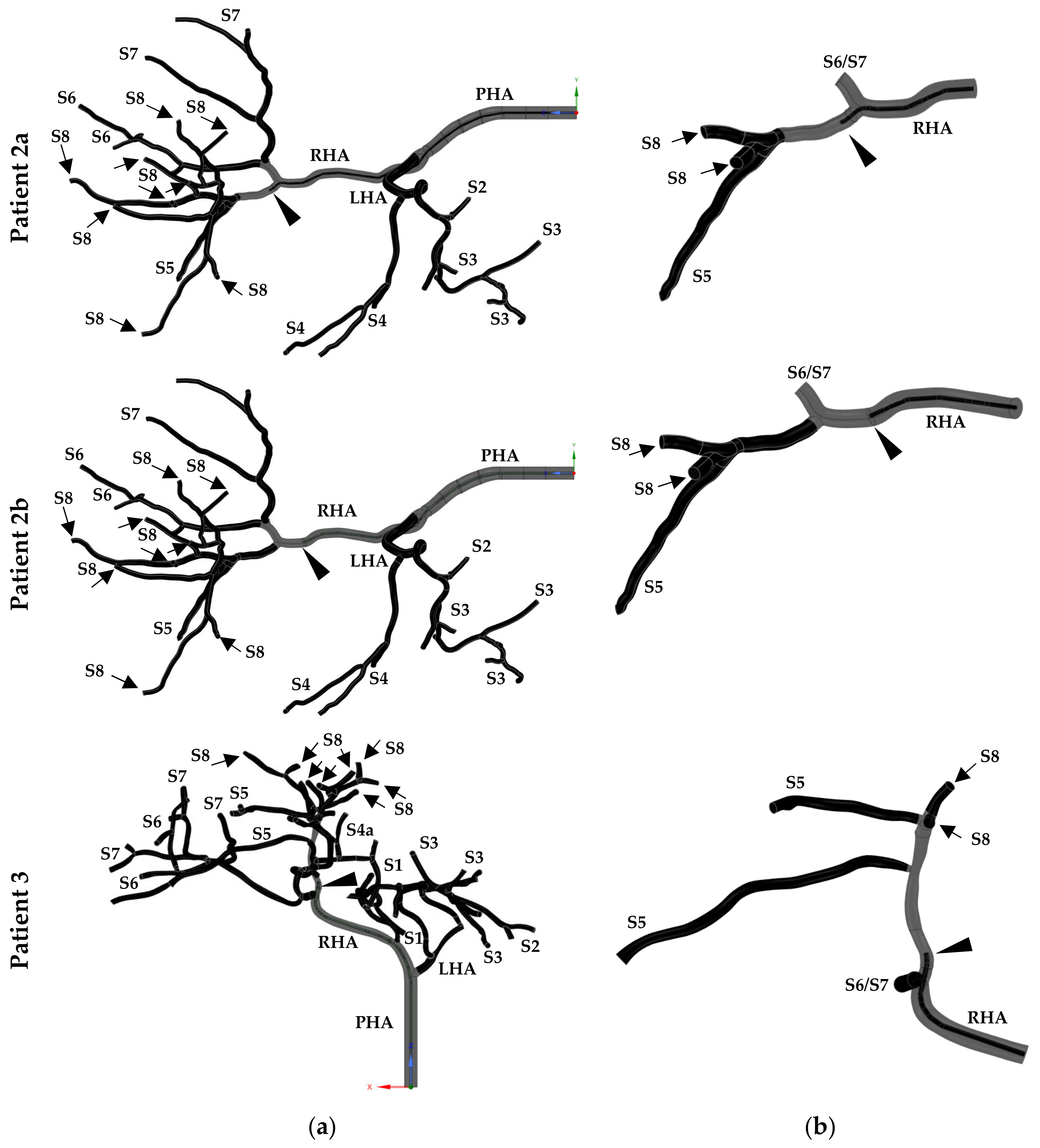
2.2. Baseline and Simplified Hepatic Artery Geometries
2.3. Preprocessing
2.3.1. Spatial Domain Discretization
2.3.2. Mathematical Modeling
2.3.3. Boundary Conditions
2.4. Solver Settings
2.5. Postprocessing
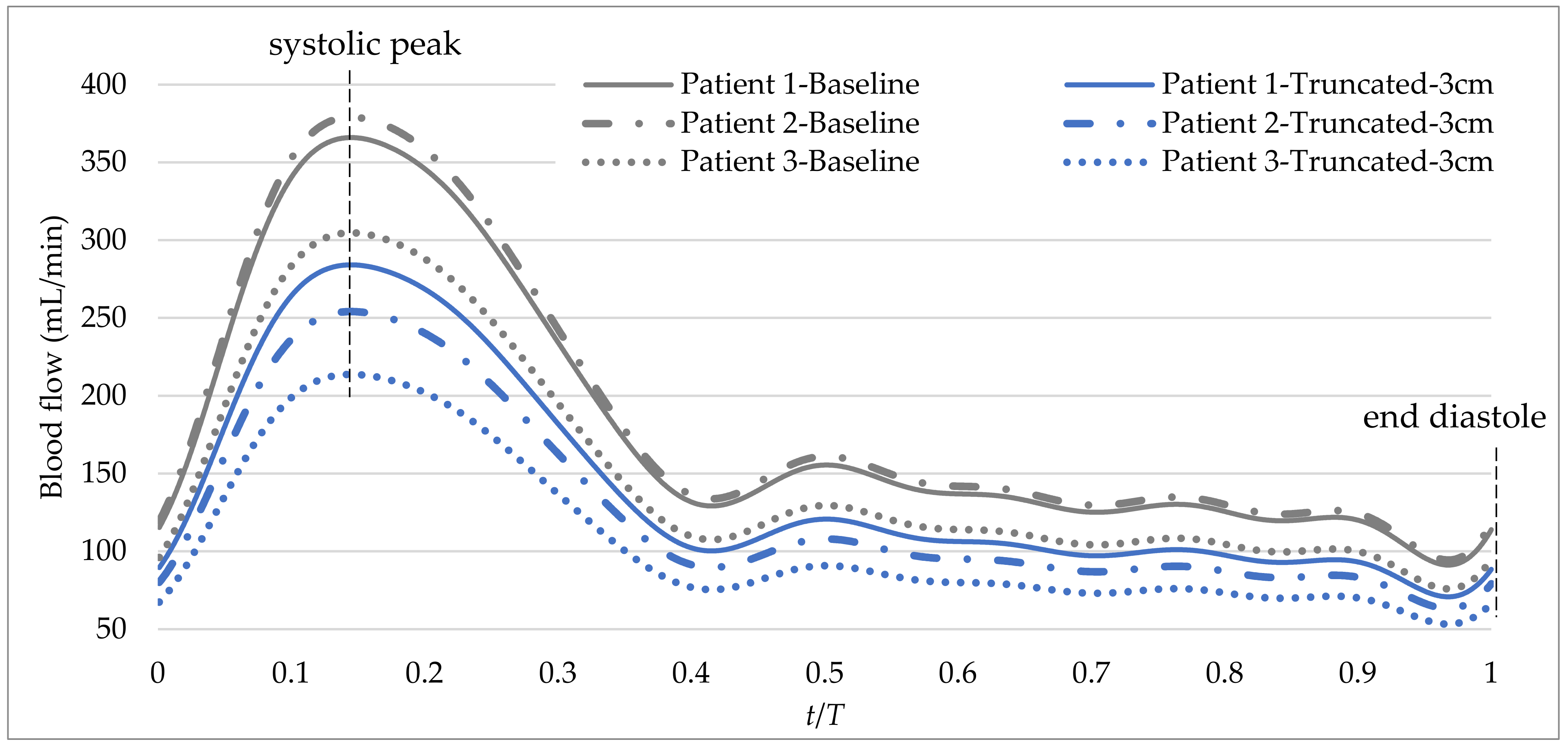
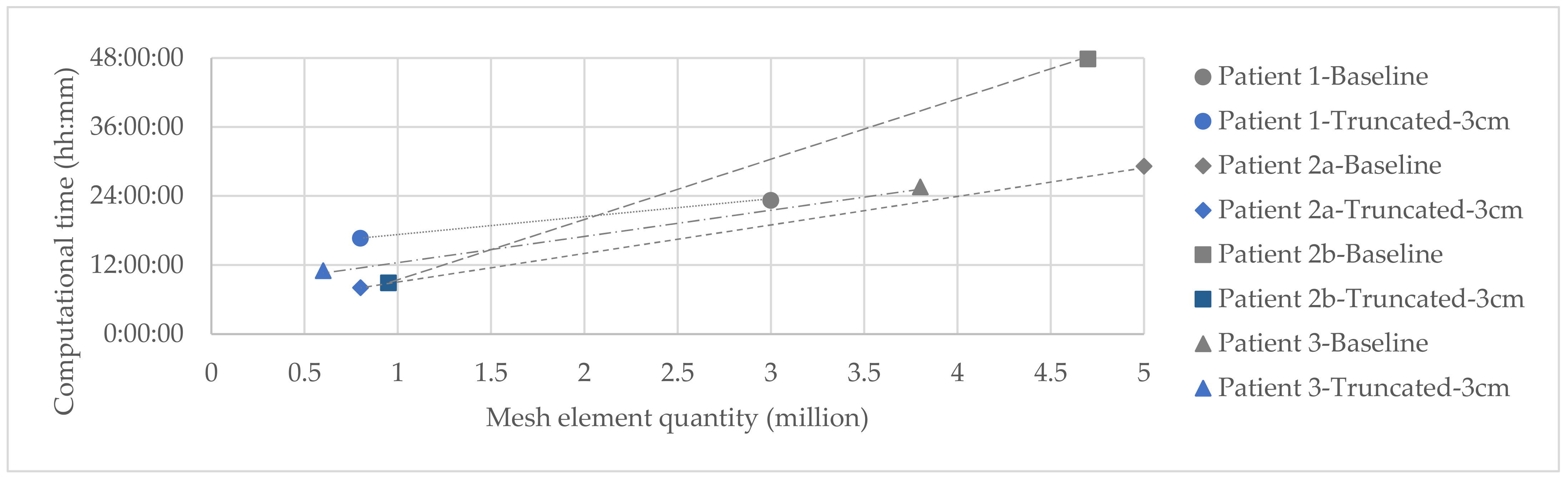
- Cycle-to-cycle computational time: to quantitatively assess the cost (in time) of each of the cycles.
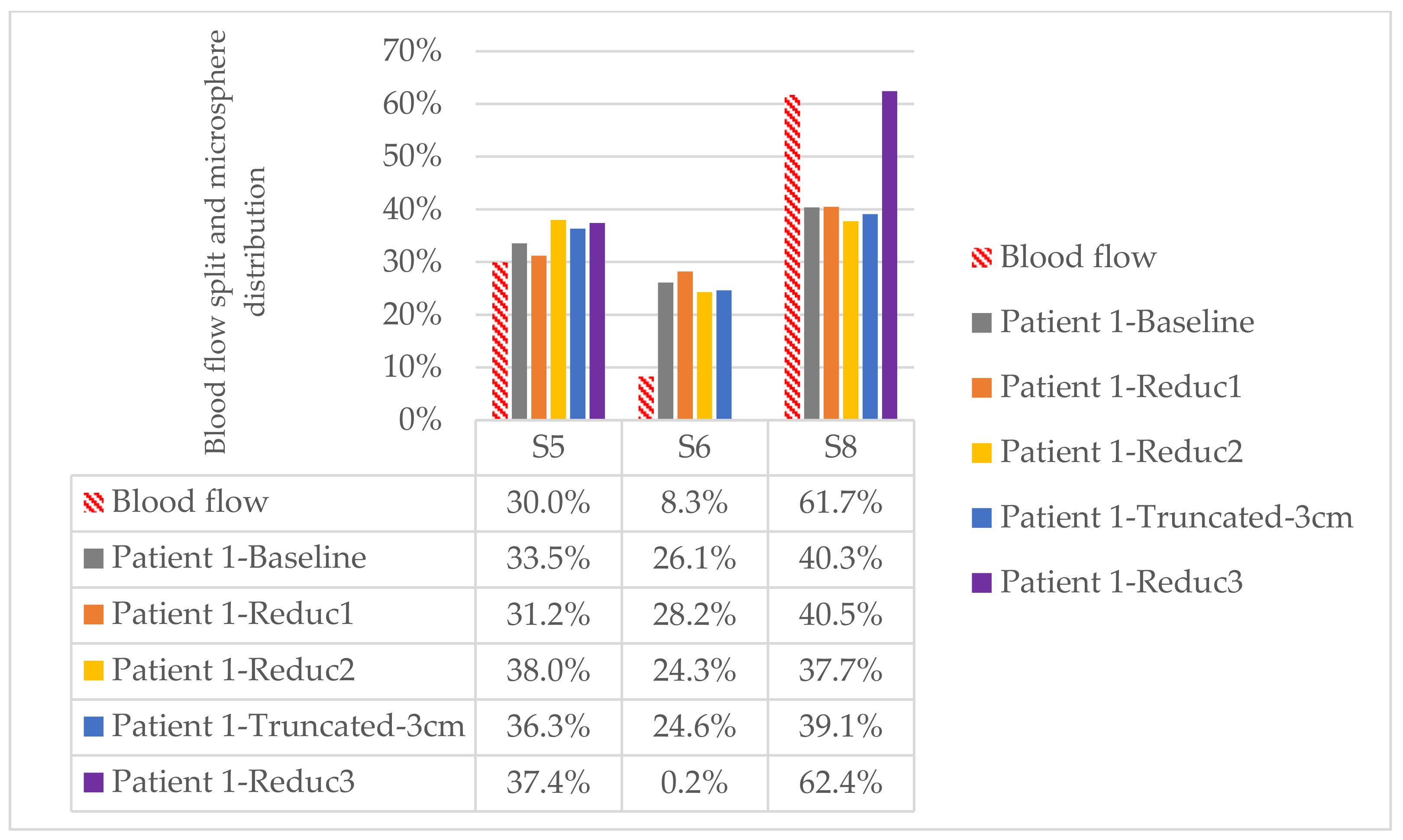
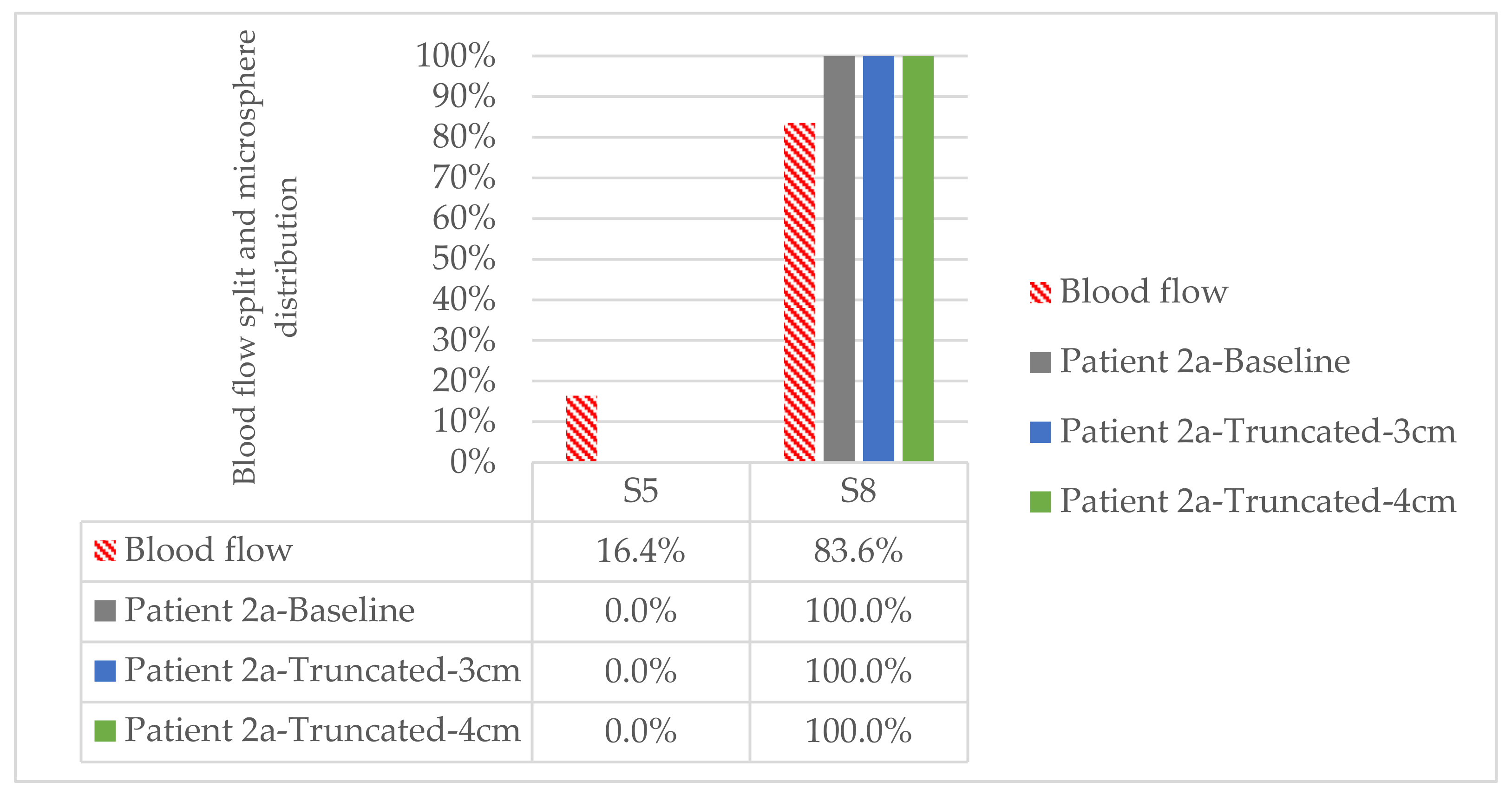
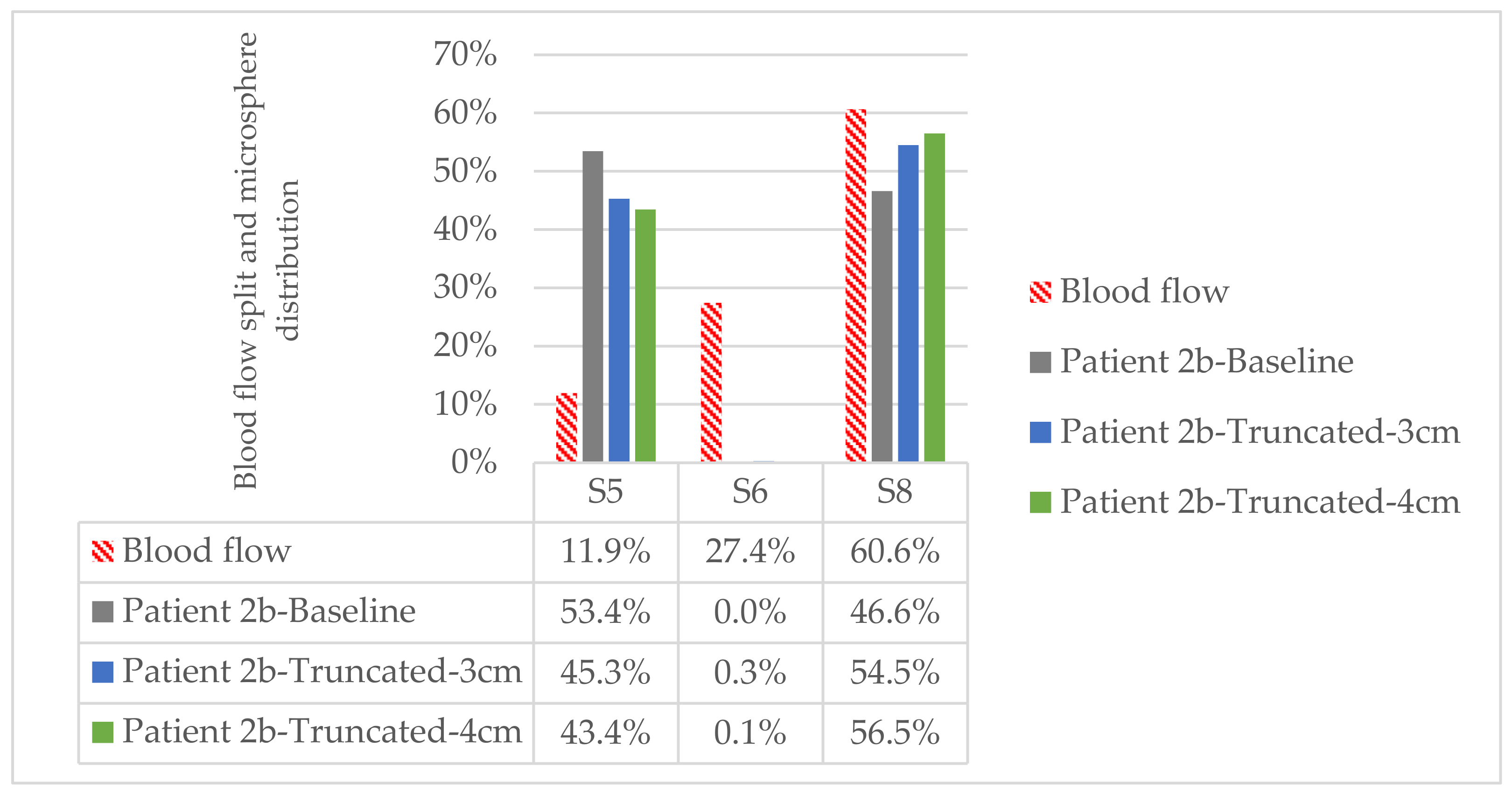
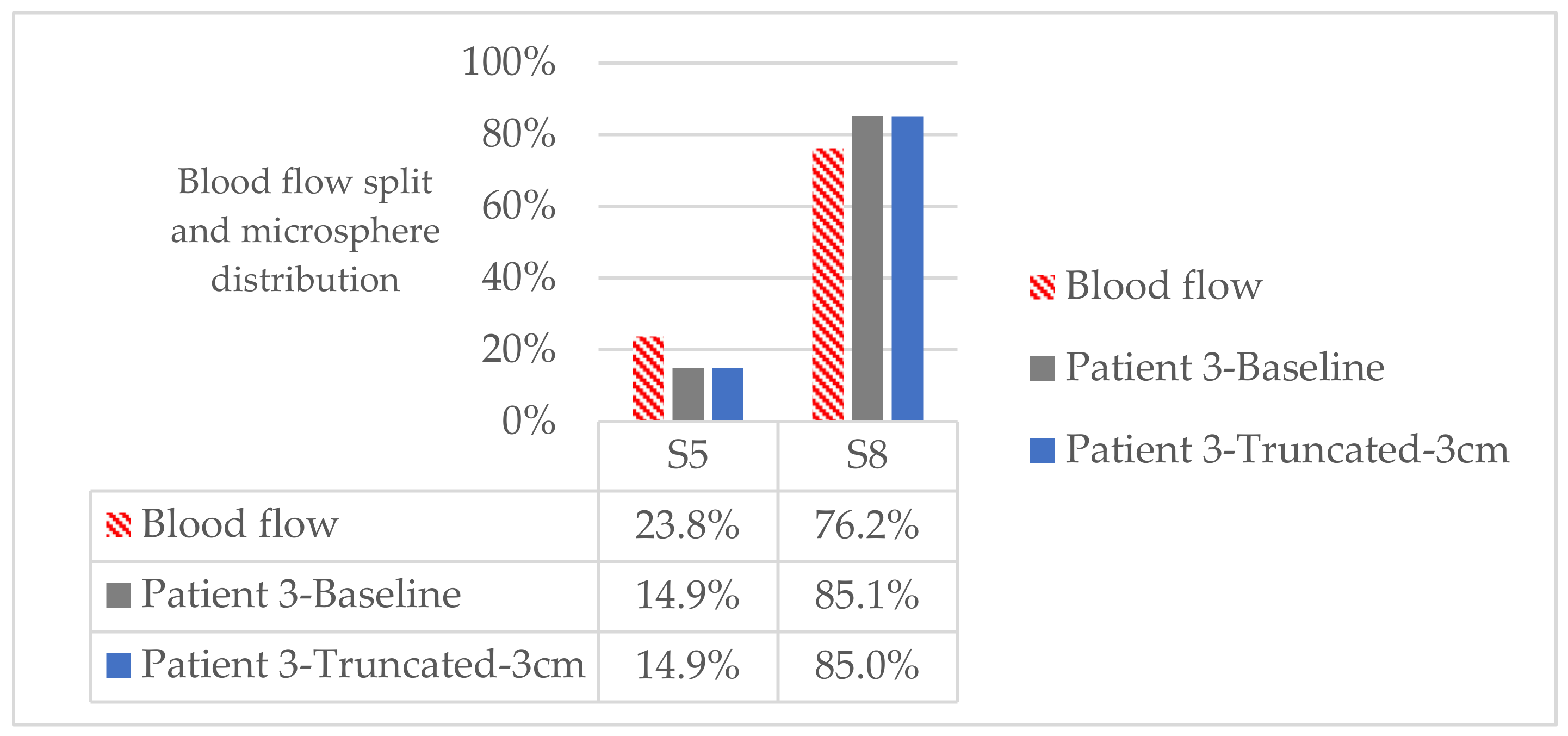
- Segment-to-segment microsphere distribution: to qualitatively assess the segment-to-segment microsphere distribution at the end of the treatment. This is calculated from the cumulative number of microspheres exiting through each outlet. The final outlet-to-outlet microsphere distribution is translated into the segment-to-segment microsphere distribution, which is the important parameters due to its clinical implication.
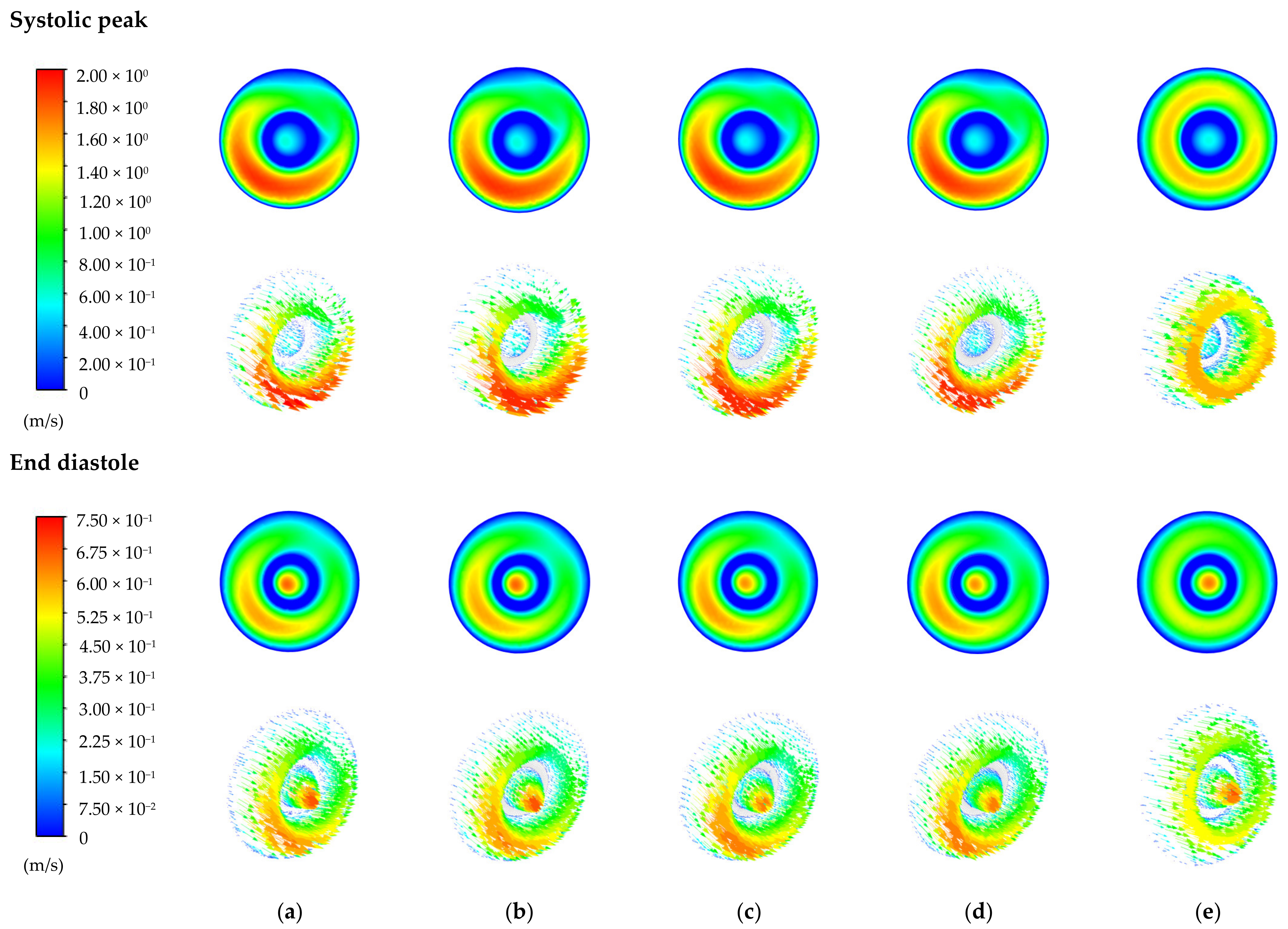
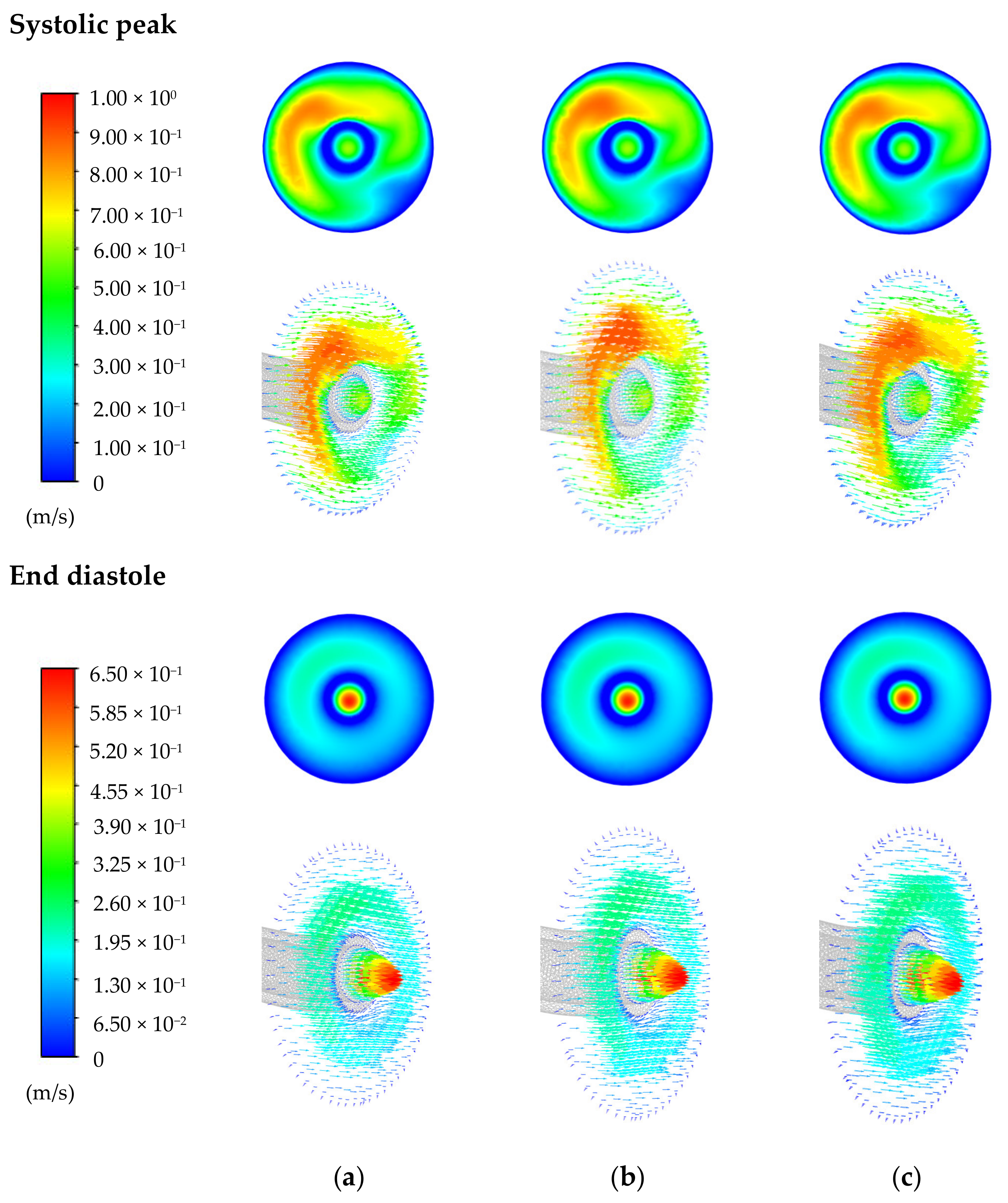
- Velocity magnitude contours and velocity vectors at the systolic peak and end diastole (see Figure 3) at the cross-section of the microcatheter tip: to qualitatively analyze important changes in the blood-flow pattern near the microcatheter tip. The important postprocessing is the segment-to-segment microsphere distribution for its clinical implications, but blood-flow patterns should be similar between the baseline and truncated geometries so that the microsphere distribution is also similar.
3. Results
3.1. Patient 1
3.2. Patient 2
3.2.1. Patient 2a
3.2.2. Patient 2b
3.3. Patient 3
3.4. Computational Times
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Bajwa, R.; Madoff, D.C.; Kishore, S.A. Embolotherapy for Hepatic Oncology: Current Perspectives and Future Directions. Dig. Dis. Interv. 2020, 4, 134–147. [Google Scholar] [CrossRef]
- Aramburo, J.; Antón, R.; Rivas, A.; Ramos, J.C.; Sangro, B.; Bilbao, J.I. Liver Radioembolization: An Analysis of Parameters that Influence the Catheter-Based Particle-Delivery via CFD. Curr. Med. Chem. 2020, 27, 1600–1615. [Google Scholar] [CrossRef]
- Xu, Z.; Jernigan, S.; Kleinstreuer, C.; Buckner, G.D. Solid Tumor Embolotherapy in Hepatic Arteries with an Anti-reflux Catheter System. Ann. Biomed. Eng. 2015, 44, 1036–1046. [Google Scholar] [CrossRef] [PubMed]
- Aramburu, J.; Antón, R.; Rivas, A.; Ramos, J.C.; Sangro, B.; Bilbao, J.I. Computational assessment of the effects of the catheter type on particle–hemodynamics during liver radioembolization. J. Biomech. 2016, 49, 3705–3713. [Google Scholar] [CrossRef]
- Aramburu, J.; Antón, R.; Rivas, A.; Ramos, J.C.; Sangro, B.; Bilbao, J.I. The role of angled-tip microcatheter and microsphere injection velocity in liver radioembolization: A computational particle–hemodynamics study. Int. J. Numer. Methods Biomed. Eng. 2017, 33. [Google Scholar] [CrossRef] [PubMed]
- Basciano, C.A.; Kleinstreuer, C.; Kennedy, A.S.; Dezarn, W.A.; Childress, E. Computer Modeling of Controlled Microsphere Release and Targeting in a Representative Hepatic Artery System. Ann. Biomed. Eng. 2010, 38, 1862–1879. [Google Scholar] [CrossRef]
- Aramburu, J.; Antón, R.; Rivas, A.; Ramos, J.C.; Sangro, B.; Bilbao, J.I. Computational particle-haemodynamics analysis of liver radioembolization pretreatment as an actual treatment surrogate. Int. J. Numer. Methods Biomed. Eng. 2016, 33, e02791. [Google Scholar] [CrossRef] [PubMed]
- Bomberna, T.; Koudehi, G.A.; Claerebout, C.; Verslype, C.; Maleux, G.; Debbaut, C. Transarterial drug delivery for liver cancer: Numerical simulations and experimental validation of particle distribution in patient-specific livers. Expert Opin. Drug Deliv. 2020, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Kleinstreuer, C. Drug-targeting methodologies with applications: A review. World J. Clin. Cases 2014, 2, 742–756. [Google Scholar] [CrossRef]
- Roncali, E.; Taebi, A.; Foster, C.; Vu, C.T. Personalized Dosimetry for Liver Cancer Y-90 Radioembolization Using Computational Fluid Dynamics and Monte Carlo Simulation. Ann. Biomed. Eng. 2020, 48, 1499–1510. [Google Scholar] [CrossRef] [PubMed]
- Childress, E.M.; Kleinstreuer, C. Impact of Fluid–Structure Interaction on Direct Tumor-Targeting in a Representative Hepatic Artery System. Ann. Biomed. Eng. 2013, 42, 461–474. [Google Scholar] [CrossRef] [PubMed]
- Couinaud, C. The anatomy of the liver. Ann. Ital. Chir. 1992, 63, 693–697. [Google Scholar] [PubMed]
- Oktar, S.O.; Yücel, C.; Demirogullari, T.; Uner, A.; Benekli, M.; Erbas, G.; Ozdemir, H. Doppler Sonographic Evaluation of Hemodynamic Changes in Colorectal Liver Metastases Relative to Liver Size. J. Ultrasound Med. 2006, 25, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Mise, Y.; Satou, S.; Shindoh, J.; Conrad, C.; Aoki, T.; Hasegawa, K.; Sugawara, Y.; Kokudo, N. Three-dimensional volumetry in 107 normal livers reveals clinically relevant inter-segment variation in size. HPB 2014, 16, 439–447. [Google Scholar] [CrossRef] [Green Version]
- Aramburu, J.; Antón, R.; Rivas, A.; Ramos, J.C.; Sangro, B.; Bilbao, J.I. Liver cancer arterial perfusion modelling and CFD boundary conditions methodology: A case study of the haemodynamics of a patient-specific hepatic artery in literature-based healthy and tumour-bearing liver scenarios. Int. J. Numer. Methods Biomed. Eng. 2016, 32, e02764. [Google Scholar] [CrossRef]
- Yang, H.F.; Du, Y.; Ni, J.X.; Zhou, X.P.; Li, J.D.; Zhang, Q.; Xu, X.X.; Li, Y. Perfusion computed tomography evaluation of angiogenesis in liver cancer. Eur. Radiol. 2010, 20, 1424–1430. [Google Scholar] [CrossRef]
- Tsushima, Y.; Funabasama, S.; Aoki, J.; Sanada, S.; Endo, K. Quantitative perfusion map of malignant liver tumors, created from dynamic computed tomography data. Acad. Radiol. 2004, 11, 215–223. [Google Scholar] [CrossRef]
- Sirtex Medical Limited. SIR-Spheres ® Y-90 Resin Microspheres (Yttrium-90 Microspheres). Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwjVj_uy4dzuAhVxRhUIHe0VCrUQFjAAegQI-Ax-AC&url=https%3A%2F%2Fwww.sirtex.com%2Fmedia%2F169247%2Fssl-us-14-sir-spheres-microspheres-ifu-us.pdf&usg=AOvVaw1W0waSBfewI6noitPu_xzW (accessed on 9 February 2021).
- Kenner, T. The measurement of blood density and its meaning. Basic Res. Cardiol. 1989, 84, 111–124. [Google Scholar] [CrossRef]
- Basciano, C.A. Computational Particle-Hemodynamics Analysis Applied to an Abdominal Aortic Aneurysm with Thrombus and Microsphere-Targeting of Liver Tumors. Ph.D. Thesis, North Carolina State University, Raleigh, NC, USA, 2010. [Google Scholar]
- Basciano, C.A.; Kleinstreuer, C.; Kennedy, A.S. Computational Fluid Dynamics Modeling of 90Y Microspheres in Human Hepatic Tumors. J. Nucl. Med. Radiat. Ther. 2011, 1. [Google Scholar] [CrossRef]
- Kleinstreuer, C.; Basciano, C.A.; Childress, E.M.; Kennedy, A.S. A New Catheter for Tumor Targeting With Radioactive Microspheres in Representative Hepatic Artery Systems. Part I: Impact of Catheter Presence on Local Blood Flow and Microsphere Delivery. J. Biomech. Eng. 2012, 134. [Google Scholar] [CrossRef] [PubMed]
- Childress, E.M.; Kleinstreuer, C.; Kennedy, A.S. A New Catheter for Tumor-Targeting with Radioactive Microspheres in Representative Hepatic Artery Systems—Part II: Solid Tumor-Targeting in a Patient-Inspired Hepatic Artery System. J. Biomech. Eng. 2012, 134. [Google Scholar] [CrossRef]
- Childress, E.M.; Kleinstreuer, C. Computationally Efficient Particle Release Map Determination for Direct Tumor-Targeting in a Representative Hepatic Artery System. J. Biomech. Eng. 2013, 136. [Google Scholar] [CrossRef]
- Antón, R.; Antoñana, J.; Aramburu, J.; Ezponda, A.; Prieto, E.; Andonegui, A.; Ortega, J.; Vivas, I.; Sancho, L.; Sangro, B.; et al. A proof-of-concept study of the in-vivo validation of a computational fluid dynamics model of personalized radioembolization. Sci. Rep. 2021, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Aramburu, J. Liver Radioembolization: Computational Particle-Hemodynamics Studies in a Patient-Specific Hepatic Artery under Literature-Based Cancer Scenarios. Ph.D. Thesis, Universidad de Navarra, Pamplona, Spain, 2016. [Google Scholar]
- Umbarkar, T.S.; Kleinstreuer, C. Computationally Efficient Fluid-Particle Dynamics Simulations of Arterial Systems. Commun. Comput. Phys. 2015, 17, 401–423. [Google Scholar] [CrossRef]
- Aramburu, J.; Antón, R.; Rivas, A.; Ramos, J.C.; Larraona, G.S.; Sangro, B.; Bilbao, J.I. Numerical zero-dimensional hepatic artery hemodynamics model for balloon-occluded transarterial chemoembolization. Int. J. Numer. Methods Biomed. Eng. 2018, 34, e2983. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Segment | Healthy Tissue Volume (mL) | Tumor Volume (mL) | Volumetric Flow Rate (mL/min) |
|---|---|---|---|
| S1 | - | - | - |
| S2 | 241 | - | 24.1 |
| S3 | 96 | - | 9.6 |
| S4a | 24 | - | 2.4 |
| S4b | 48 | - | 4.8 |
| S5 | 330 | - | 33 |
| S6 | 183 | - | 18.3 |
| S7 | 228 | - | 22.8 |
| S8 | 340 | 68 | 68 |
| Total | 1490 | 68 | 183 |
| Segment | Healthy Tissue Volume (mL) | Tumor Volume (mL) | Volumetric Flow Rate (mL/min) |
|---|---|---|---|
| S1 | - | - | - |
| S2 | 157.8 | - | 15.8 |
| S3 | 157.4 | - | 15.7 |
| S4 | 309.4 | - | 30.9 |
| S5 | 151.7 | - | 15.2 |
| S6 | 193.1 | - | 19.3 |
| S7 | 155.3 | - | 15.5 |
| S8 | 385.4 | 77.1 | 77.1 |
| Total | 1510 | 77.1 | 189.5 |
| Segment | Healthy Tissue Volume (mL) | Tumor Volume (mL) | Volumetric Flow Rate (mL/min) |
|---|---|---|---|
| S1 | 62 | - | 6.2 |
| S2 | 128 | - | 12.8 |
| S3 | 181 | - | 18.1 |
| S4a | 73 | - | 7.3 |
| S4b | 11 | - | 1.1 |
| S5 | 124 | - | 12.4 |
| S6 | 169 | - | 16.9 |
| S7 | 373 | - | 37.3 |
| S8 | 204 | 39.8 | 40.3 |
| Total | 1325 | 39.8 | 152.4 |
| Patient | Baseline Geometry | Truncated Geometry |
|---|---|---|
| Patient 1 | 3 | 0.8 |
| Patient 2a | 5 | 0.8 |
| Patient 2b | 4.7 | 0.95 |
| Patient 3 | 3.8 | 0.6 |
| Cycle | Relative Computational Time |
|---|---|
| Cycle 1: Convergence | 11.6% |
| Cycle 2: Injection | 34.1% |
| Cycle 3: Extra cycle 1 | 28.0% |
| Cycle 4: Extra cycle 2 | 26.3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lertxundi, U.; Aramburu, J.; Ortega, J.; Rodríguez-Fraile, M.; Sangro, B.; Bilbao, J.I.; Antón, R. CFD Simulations of Radioembolization: A Proof-of-Concept Study on the Impact of the Hepatic Artery Tree Truncation. Mathematics 2021, 9, 839. https://doi.org/10.3390/math9080839
Lertxundi U, Aramburu J, Ortega J, Rodríguez-Fraile M, Sangro B, Bilbao JI, Antón R. CFD Simulations of Radioembolization: A Proof-of-Concept Study on the Impact of the Hepatic Artery Tree Truncation. Mathematics. 2021; 9(8):839. https://doi.org/10.3390/math9080839
Chicago/Turabian StyleLertxundi, Unai, Jorge Aramburu, Julio Ortega, Macarena Rodríguez-Fraile, Bruno Sangro, José Ignacio Bilbao, and Raúl Antón. 2021. "CFD Simulations of Radioembolization: A Proof-of-Concept Study on the Impact of the Hepatic Artery Tree Truncation" Mathematics 9, no. 8: 839. https://doi.org/10.3390/math9080839