
Biomechanical Symmetry during Drop Jump Landing and Takeoff in Adolescent Athletes Following Recent Anterior Cruciate Ligament Reconstruction

 ,
,  ,
,
Abstract
:1. Introduction
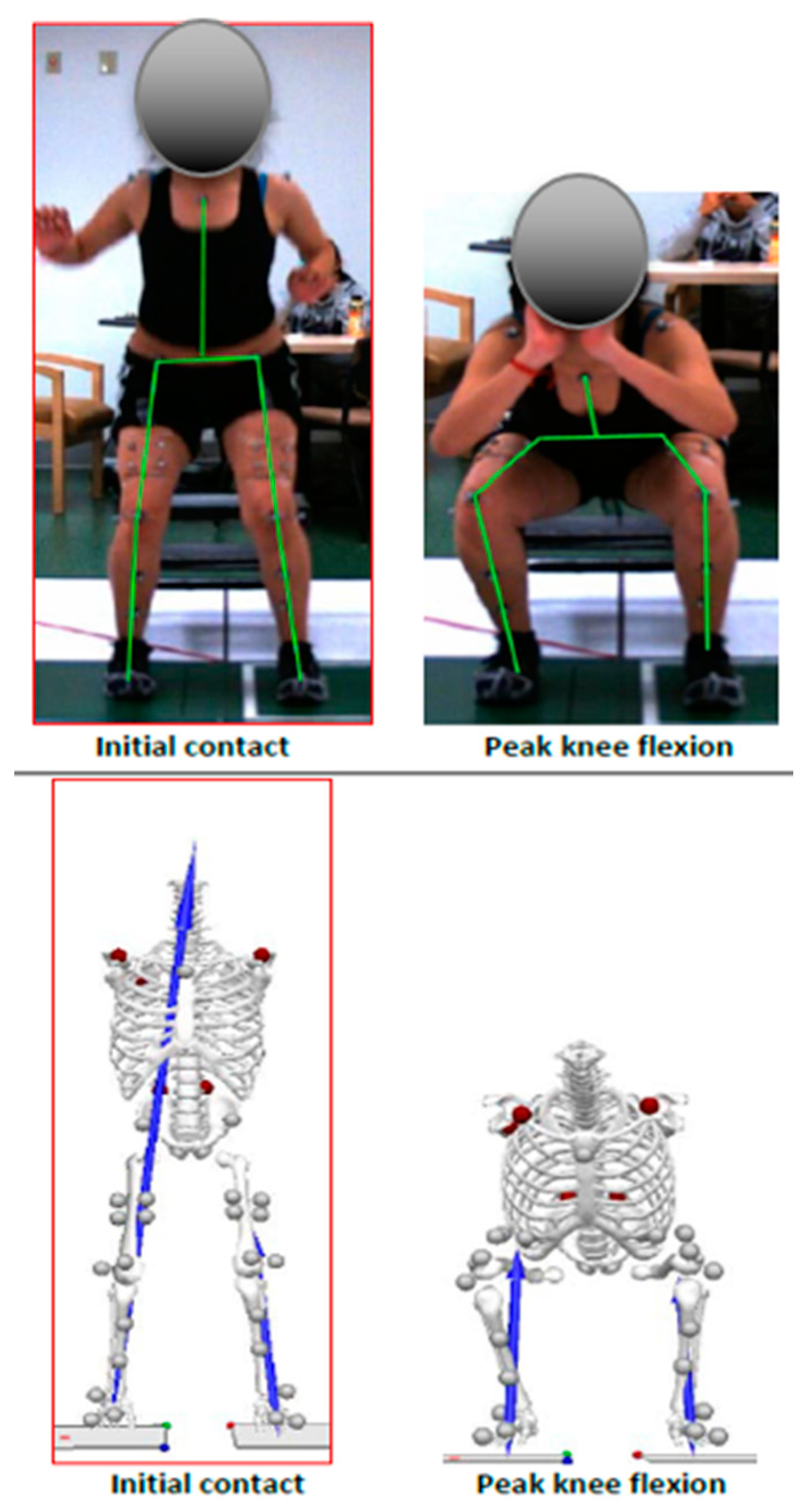
2. Materials and Methods
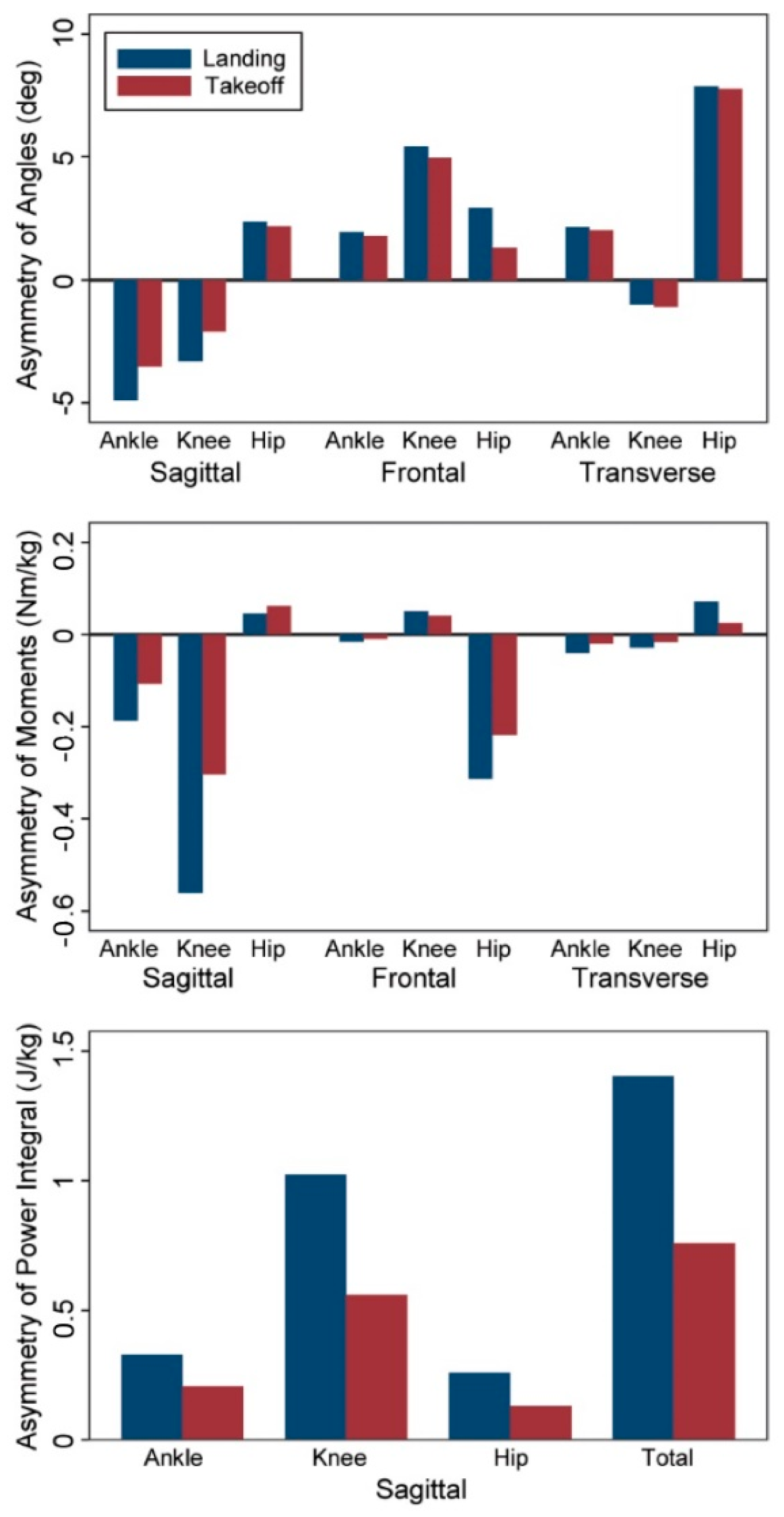
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- LaBella, C.R.; Hennrikus, W.; Hewett, T.E. Anterior Cruciate Ligament Injuries: Diagnosis, Treatment, and Prevention. Pediatrics 2014, 133, e1437–e1450. [Google Scholar] [CrossRef] [Green Version]
- Beck, N.A.; Lawrence, J.T.R.; Nordin, J.D.; DeFor, T.A.; Tompkins, M. ACL Tears in School-Aged Children and Adolescents Over 20 Years. Pediatrics 2017, 139, e20161877. [Google Scholar] [CrossRef] [Green Version]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Heidt, R.S.; Colosimo, A.J.; McLean, S.G.; Van den Bogert, A.J.; Paterno, M.V.; Succop, P. Biomechanical Measures of Neuromuscular Control and Valgus Loading of the Knee Predict Anterior Cruciate Ligament Injury Risk in Female Athletes: A Prospective Study. Am. J. Sports Med. 2005, 33, 492–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leppänen, M.; Pasanen, K.; Krosshaug, T.; Kannus, P.; Vasankari, T.; Kujala, U.M.; Bahr, R.; Perttunen, J.; Parkkari, J. Sagittal Plane Hip, Knee, and Ankle Biomechanics and the Risk of Anterior Cruciate Ligament Injury: A Prospective Study. Orthop. J. Sport. Med. 2017, 5. [Google Scholar] [CrossRef] [Green Version]
- Myer, G.D.; Paterno, M.V.; Ford, K.R.; Quatman, C.E.; Hewett, T.E. Rehabilitation After Anterior Cruciate Ligament Reconstruction: Criteria-Based Progression Through the Return-to-Sport Phase. J. Orthop. Sport Phys. Ther. 2006, 36, 385–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyman, S.; Koulouvaris, P.; Sherman, S.; Do, H.; Mandl, L.A.; Marx, R.G. Epidemiology of Anterior Cruciate Ligament Reconstruction. J. Bone Jt. Surg. Am. Vol. 2009, 91, 2321–2328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, K.L.; Lam, K.C.; Valovich McLeod, T.C. Early Operative Versus Delayed or Nonoperative Treatment of Anterior Cruciate Ligament Injuries in Pediatric Patients. J. Athl. Train. 2016, 51, 425–427. [Google Scholar] [CrossRef] [Green Version]
- McCullough, K.A.; Phelps, K.D.; Spindler, K.P.; Matava, M.J.; Dunn, W.R.; Parker, R.D.; MOON Group; Reinke, E.K. Return to High School- and College-Level Football After Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2012, 40, 2523–2529. [Google Scholar] [CrossRef]
- Wiggins, A.J.; Grandhi, R.K.; Schneider, D.K.; Stanfield, D.; Webster, K.E.; Myer, G.D. Risk of Secondary Injury in Younger Athletes After Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2016, 44, 1861–1876. [Google Scholar] [CrossRef] [Green Version]
- Simon, D.; Mascarenhas, R.; Saltzman, B.M.; Rollins, M.; Bach, B.R.; MacDonald, P. The Relationship between Anterior Cruciate Ligament Injury and Osteoarthritis of the Knee. Adv. Orthop. 2015, 2015, 928301. [Google Scholar] [CrossRef]
- Krosshaug, T.; Steffen, K.; Kristianslund, E.; Nilstad, A.; Mok, K.-M.; Myklebust, G.; Andersen, T.E.; Holme, I.; Engebretsen, L.; Bahr, R. The Vertical Drop Jump Is a Poor Screening Test for ACL Injuries in Female Elite Soccer and Handball Players. Am. J. Sports Med. 2016, 44, 874–883. [Google Scholar] [CrossRef] [Green Version]
- Meyer, C.A.G.; Gette, P.; Mouton, C.; Seil, R.; Theisen, D. Side-to-side asymmetries in landing mechanics from a drop vertical jump test are not related to asymmetries in knee joint laxity following anterior cruciate ligament reconstruction. Knee Surg. Sport Traumatol. Arthrosc. 2018, 26, 381–390. [Google Scholar] [CrossRef] [Green Version]
- Myer, G.D.; Martin, L.; Ford, K.R.; Paterno, M.V.; Schmitt, L.C.; Heidt, R.S.; Colosimo, A.; Hewett, T.E. No Association of Time From Surgery with Functional Deficits in Athletes After Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2012, 40, 2256–2263. [Google Scholar] [CrossRef] [Green Version]
- Ardern, C.L.; Webster, K.E.; Taylor, N.F.; Feller, J.A. Return to sport following anterior cruciate ligament reconstruction surgery: A systematic review and meta-analysis of the state of play. Br. J. Sports Med. 2011, 45, 596–606. [Google Scholar] [CrossRef] [PubMed]
- Müller, U.; Krüger-Franke, M.; Schmidt, M.; Rosemeyer, B. Predictive parameters for return to pre-injury level of sport 6 months following anterior cruciate ligament reconstruction surgery. Knee Surg. Sport Traumatol. Arthrosc. 2015, 23, 3623–3631. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, L.C.; Paterno, M.V.; Ford, K.R.; Myer, G.D.; Hewett, T.E. Strength Asymmetry and Landing Mechanics at Return to Sport after Anterior Cruciate Ligament Reconstruction. Med. Sci. Sport Exerc. 2015, 47, 1426–1434. [Google Scholar] [CrossRef] [Green Version]
- Minetti, A.E.; Ardigo, L.P.; Susta, D.C. Using leg muscles as shock absorbers: Theoretical predictions and experimental results of drop landing performance. Ergonomics 1998, 41, 1771–1791. [Google Scholar] [CrossRef] [PubMed]
- Mueske, N.; Katzel, M.J.; Chadwick, K.P.; VandenBerg, C.; Pace, J.L.; Zaslow, T.; Edison, B.; O’Callahan, B.G.; Nakata, H.L.; Wren, T. Biomechanical Symmetry During Drop Jump and Single-leg Hop Landing in Uninjured Adolescent Athletes. Orthop. J. Sport Med. 2019, 7. [Google Scholar] [CrossRef]
- Mueske, N.M.; VandenBerg, C.D.; Pace, J.L.; Katzel, M.J.; Zaslow, T.L.; Padilla, R.A.; Wren, T.A. Comparison of drop jump landing biomechanics and asymmetry among adolescents with hamstring, patellar and quadriceps tendon autografts for anterior cruciate ligament reconstruction. Knee 2018, 25, 1065–1073. [Google Scholar] [CrossRef]
- Renstrom, P.; Ljungqvist, A.; Arendt, E.; Beynnon, B.; Fukubayashi, T.; Garrett, W.; Georgoulis, T.; Hewett, T.E.; Johnson, R.; Krosshaug, T.; et al. Non-contact ACL injuries in female athletes: An International Olympic Committee current concepts statement. Br. J. Sports Med. 2008, 42, 394–412. [Google Scholar] [CrossRef] [Green Version]
- Boden, B.P.; Dean, G.S.; Feagin, J.A., Jr.; Garrett, W.E., Jr. Mechanisms of Anterior Cruciate Ligament Injury. Orthopedics 2000, 23, 573–578. [Google Scholar] [CrossRef]
- Paterno, M.V.; Schmitt, L.C.; Ford, K.R.; Rauh, M.J.; Myer, G.D.; Hewett, T.E. Effects of Sex on Compensatory Landing Strategies Upon Return to Sport After Anterior Cruciate Ligament Reconstruction. J. Orthop. Sport Phys. Ther. 2011, 41, 553–559. [Google Scholar] [CrossRef]
- Mueske, N.M.; Patel, A.R.; Pace, J.L.; Zaslow, T.L.; VandenBerg, C.D.; Katzel, M.J.; Edison, B.R.; Wren, T.A. Improvements in landing biomechanics following anterior cruciate ligament reconstruction in adolescent athletes. Sport Biomech. 2018, 19, 738–749. [Google Scholar] [CrossRef]
- Leppänen, M.; Pasanen, K.; Kujala, U.M.; Vasankari, T.; Kannus, P.; Äyrämö, S.; Krosshaug, T.; Bahr, R.; Avela, J.; Perttunen, J.; et al. Stiff Landings Are Associated With Increased ACL Injury Risk in Young Female Basketball and Floorball Players. Am. J. Sports Med. 2017, 45, 386–393. [Google Scholar] [CrossRef]
- Boden, B.P.; Sheehan, F.T.; Torg, J.S.; Hewett, T.E. Noncontact Anterior Cruciate Ligament Injuries: Mechanisms and Risk Factors. Am. Acad. Orthop. Surg. 2010, 18, 520–527. [Google Scholar] [CrossRef] [Green Version]
- Hughes, G.; Musco, P.; Caine, S.; Howe, L. Lower Limb Asymmetry After Anterior Cruciate Ligament Reconstruction in Adolescent Athletes: A Systematic Review and Meta-Analysis. J. Athl. Train. 2020, 55, 811–825. [Google Scholar] [CrossRef] [PubMed]
- Ford, K.R.; Myer, G.D.; Smith, R.L.; Byrnes, R.N.; Dopirak, S.E.; Hewett, T.E. Use of an Overhead Goal Alters Vertical Jump Performance and Biomechanics. J. Strength Cond. Res. 2005, 19, 394. [Google Scholar] [CrossRef] [Green Version]
- Ford, K.; Myer, G.; Brent, J.; Hewett, T. Hip and knee extensor moments predict vertical jump height in adolescent girls. J. Strength Cond. Res 2009, 23, 1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Health and Human Services. Body Mass Index: Considerations for Practitioner; Department of Health and Human Services Center for Disease Control and Prevention: Atlanta, GA, USA, 2014; pp. 1–4.
- Wren, T.A.L.; O’Callahan, B.; Katzel, M.J.; Zaslow, T.L.; Edison, B.R.; VandenBerg, C.D.; Conrad-Forrest, A.; Mueske, N.M. Movement variability in pre-teen and teenage athletes performing sports related tasks. Gait Posture 2020, 80, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Linthorne, N.P. Analysis of standing vertical jumps using a force platform. Am. J. Phys. 2001, 69, 1198–1204. [Google Scholar] [CrossRef] [Green Version]
- Dai, B.; Butler, R.J.; Garrett, W.E.; Queen, R.M. Using ground reaction force to predict knee kinetic asymmetry following anterior cruciate ligament reconstruction. Scand. J. Med. Sci. Sports 2014, 24, 974–981. [Google Scholar] [CrossRef] [Green Version]
- Englund, M. The role of biomechanics in the initiation and progression of OA of the knee. In Best Practice and Research: Clinical Rheumatology; Elsevier Ltd.: Amsterdam, The Netherlands, 2010; Volume 24, pp. 39–46. [Google Scholar] [CrossRef]
- Øiestad, B.E.; Holm, I.; Aune, A.K.; Gunderson, R.; Myklebust, G.; Engebretsen, L.; Aarsland Fosdahl, M.; Risberg, M.A. Knee Function and Prevalence of Knee Osteoarthritis after Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2010, 38, 2201–2210. [Google Scholar] [CrossRef]
- Delahunt, E.; Sweeney, L.; Chawke, M.; Kelleher, J.; Murphy, K.; Patterson, M.; Prendiville, A. Lower limb kinematic alterations during drop vertical jumps in female athletes who have undergone anterior cruciate ligament reconstruction. J. Orthop. Res. 2012, 30, 72–78. [Google Scholar] [CrossRef]
- Decker, M.J.; Torry, M.R.; Wyland, D.J.; Sterett, W.I.; Richard Steadman, J. Gender differences in lower extremity kinematics, kinetics and energy absorption during landing. Clin. Biomech. 2003, 18, 662–669. [Google Scholar] [CrossRef]
- Renner, K.E.; Franck, C.T.; Miller, T.K.; Queen, R.M. Limb asymmetry during recovery from anterior cruciate ligament reconstruction. J. Orthop. Res. 2018, 36, 1887–1893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pratt, K.A.; Sigward, S.M. Knee Loading Deficits During Dynamic Tasks in Individuals Following Anterior Cruciate Ligament Reconstruction. J. Orthop. Sport Phys. Ther 2017, 47. [Google Scholar] [CrossRef] [PubMed]
- Sigward, S.M.; Chan, M.S.M.; Lin, P.E.; Almansouri, S.Y.; Pratt, K.A. Compensatory strategies that reduce knee extensor demand during a bilateral squat change from 3 to 5 months following anterior cruciate ligament reconstruction. J. Orthop. Sports Phys. Ther. 2018, 48, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Wren, T.A.L.; Mueske, N.M.; Brophy, C.H.; Pace, J.L.; Katzel, M.J.; Edison, B.R.; Vandenberg, C.D.; Zaslow, T.L. Hop Distance Symmetry Does Not Indicate Normal Landing Biomechanics in Adolescent Athletes With Recent Anterior Cruciate Ligament Reconstruction. J. Orthop. Sport Phys. Ther. 2018, 48, 622–629. [Google Scholar] [CrossRef]
- Lepley, A.S.; Kuenze, C.M. Hip and Knee Kinematics and Kinetics During Landing Tasks After Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-Analysis. J. Athl. Train. 2018, 53, 144–159. [Google Scholar] [CrossRef] [Green Version]
- Chmielewski, T.L. Asymmetrical Lower Extremity Loading After ACL Reconstruction: More Than Meets the Eye. J. Orthop. Sport Phys. Ther. 2011, 41, 374–376. [Google Scholar] [CrossRef] [Green Version]
- Young, W.; Pryor, J.; Wilson, G. Effect of instructions on characteristics of countermovement and drop jump performance. J. Strength Cond. Res. 1995, 9, 232–236. [Google Scholar]
- Seminati, E.; Nardello, F.; Zamparo, P.; Ardigò, L.P.; Faccioli, N.; Minetti, A.E. Anatomically Asymmetrical Runners Move More Asymmetrically at the Same Metabolic Cost. Carrier D, editor. PLoS ONE 2013, 8, e74134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hewett, T.E.; Myer, G.D.; Ford, K.R. Anterior Cruciate Ligament Injuries in Female Athletes. Am. J. Sports Med. 2006, 34, 299–311. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Sex | |
| Female | 16 (48%) |
| Male | 17 (52%) |
| Age (years) | 15.9 (1.3) |
| Height (cm) | 170.2 (10.4) |
| Weight (kg) | 69.6 (17.4) |
| BMI (kg/m2) | 24.0 (5.4) |
| Time since surgery (months) | 7.4 (1.2) |
| Graft type (all autograph) | |
| Hamstring tendon | 13 (39%) |
| Patella tendon | 13 (39%) |
| Quadriceps tendon | 6 (18%) |
| Iliotibial band | 1 (3%) |
| Surgical side | |
| Left | 22 (67%) |
| Right | 11 (33%) |
| Meniscal involvement * | |
| None | 18 (56%) |
| Repair | 13 (24%) |
| Menisectomy | 3 (9%) |
| Single sport | 19 (59%) |
| Multiple Sports | 14 (41%) |
| Landing | Takeoff | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Injured, Mean (SD) | Contralateral, Mean (SD) | Asymmetry, Mean (SE) | p | Injured, Mean (SD) | Contralateral, Mean (SD) | Asymmetry, Mean (SE) | p | P Asymmetry TO vs. Landing | |
| FRONTAL PLANE | |||||||||
| Ankle inversion | 9.3 (4.5) | 7.3 (4.2) | 2.0 (0.7) | 0.01 | 10.9 (4.5) | 9.0 (4.2) | 1.8 (0.7) | 0.01 | 0.61 |
| Knee adduction | 8.8 (7.1) | 3.4 (6.5) | 5.4 (1.1) | <0.0001 | 7.6 (7.0) | 2.7 (6.2) | 5.0 (1.1) | 0.0001 | 0.22 |
| Hip adduction | −8.2 (8.1) | −11.1 (6.8) | 2.9 (1.3) | 0.04 | −7.8 (7.5) | −9.1 (6.5) | 1.3 (1.1) | 0.26 | 0.02 |
| Ankle inversion moment | 0.03 (0.06) | 0.05 (0.08) | −0.02 (0.01) | 0.20 | 0.09 (0.06) | 0.10 (0.08) | −0.01 (0.01) | 0.34 | 0.47 |
| Knee adduction moment | −0.17 (0.18) | −0.22 (0.25) | 0.05 (0.04) | 0.18 | −0.10 (0.13) | −0.14 (0.19) | 0.04 (0.03) | 0.16 | 0.69 |
| Hip adduction moment | −0.11 (0.22) | 0.20 (0.21) | −0.31 (0.05) | <0.0001 | −0.02 (0.21) | 0.20 (0.20) | −0.22 (0.04) | <0.0001 | 0.0001 |
| TRANSVERSE PLANE | |||||||||
| Ankle adduction | 3.4 (4.5) | 1.3 (5.2) | 2.2 (0.9) | 0.02 | 2.9 (4.7) | 0.9 (4.9) | 2.0 (0.9) | 0.02 | 0.63 |
| Knee rotation | −10.6 (10.3) | −9.5 (9.0) | −1.0 (1.4) | 0.47 | −12.8 (9.3) | −11.7 (8.6) | −1.1 (1.2) | 0.37 | 0.87 |
| Hip rotation | 12.1 (7.9) | 4.2 (6.7) | 7.9 (1.2) | <0.0001 | 11.3 (8.4) | 3.5 (7.5) | 7.8 (1.2) | <0.0001 | 0.86 |
| Ankle adduction moment | 0.11 (0.06) | 0.15 (0.06) | −0.04 (0.01) | 0.002 | 0.16 (0.06) | 0.18 (0.07) | −0.02 (0.01) | 0.03 | 0.02 |
| Knee rotation moment | 0.001 (0.04) | 0.03 (0.07) | −0.03 (0.01) | 0.05 | 0.01 (0.04) | 0.03 (0.05) | −0.02 (0.01) | 0.13 | 0.21 |
| Hip rotation moment | 0.03 (0.11) | −0.04 (0.11) | 0.07 (0.02) | 0.001 | −0.02 (0.10) | −0.05 (0.10) | 0.02 (0.02) | 0.12 | 0.003 |
| SAGITTAL PLANE | |||||||||
| Ankle dorsiflexion | 17.2 (5.7) | 22.1 (5.2) | −4.9 (0.8) | <0.0001 | 15.0 (5.5) | 18.6 (5.9) | −3.5 (0.6) | <0.0001 | 0.006 |
| Knee flexion | 85.5 (13.0) | 88.8 (11.9) | −3.3 (0.7) | 0.0001 | 79.3 (12.2) | 81.5 (11.7) | −2.1 (0.5) | 0.0001 | 0.02 |
| Hip flexion | 84.9 (11.7) | 82.6 (12.0) | 2.4 (0.7) | 0.001 | 77.5 (11.1) | 75.3 (11.0) | 2.2 (0.6) | 0.0009 | 0.61 |
| Ankle dorsiflexion moment | 0.65 (0.17) | 0.84 (0.27) | −0.19 (0.04) | 0.0002 | 0.74 (0.19) | 0.84 (0.23) | −0.11 (0.03) | 0.0002 | 0.03 |
| Knee flexion moment | 0.84 (0.34) | 1.40 (0.36) | −0.56 (0.09) | <0.0001 | 0.70 (0.27) | 1.00 (0.24) | −0.30 (0.05) | <0.0001 | <0.0001 |
| Hip flexion moment | 1.05 (0.19) | 1.01 (0.34) | 0.05 (0.06) | 0.44 | 1.10 (0.23) | 1.03 (0.24) | 0.06 (0.03) | 0.04 | 0.76 |
| Power integral ankle | 0.51 (0.14) | 0.83 (0.32) | −0.32 (0.05) | <0.0001 | 0.78 (0.19) | 0.97 (0.23) | −0.19 (0.03) | <0.0001 | 0.005 |
| Power integral knee | 1.10 (0.52) | 2.07 (0.54) | −0.97 (0.13) | <0.0001 | 1.03 (0.46) | 1.55 (0.38) | −0.52 (0.07) | <0.0001 | <0.0001 |
| Power integral hip | 0.98 (0.24) | 1.02 (0.40) | −0.05 (0.06) | 0.46 | 1.17 (0.36) | 1.17 (0.38) | 0.002 (0.03) | 0.94 | 0.01 |
| Power integral total | 2.59 (0.65) | 3.92 (0.95) | −1.33 (0.21) | <0.0001 | 2.98 (0.80) | 3.68 (0.80) | −0.70 (0.09) | <0.0001 | 0.0002 |
| Surgical | Contralateral | Asymmetry | ||||
|---|---|---|---|---|---|---|
| R | p | R | p | R | p | |
| Ankle power integral | 0.40 | 0.02 | 0.41 | 0.02 | −0.12 | 0.52 |
| Knee power integral | 0.34 | 0.05 | 0.50 | 0.003 | −0.09 | 0.63 |
| Hip power integral | 0.50 | 0.003 | 0.45 | 0.009 | 0.05 | 0.77 |
| Power integral total | 0.51 | 0.002 | 0.57 | 0.0005 | −0.02 | 0.90 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciccodicola, E.M.; Mueske, N.M.; Katzel, M.J.; VandenBerg, C.D.; Pace, J.L.; Wren, T.A.L. Biomechanical Symmetry during Drop Jump Landing and Takeoff in Adolescent Athletes Following Recent Anterior Cruciate Ligament Reconstruction. Symmetry 2021, 13, 639. https://doi.org/10.3390/sym13040639
Ciccodicola EM, Mueske NM, Katzel MJ, VandenBerg CD, Pace JL, Wren TAL. Biomechanical Symmetry during Drop Jump Landing and Takeoff in Adolescent Athletes Following Recent Anterior Cruciate Ligament Reconstruction. Symmetry. 2021; 13(4):639. https://doi.org/10.3390/sym13040639
Chicago/Turabian StyleCiccodicola, Eva M., Nicole M. Mueske, Mia J. Katzel, Curtis D. VandenBerg, James Lee Pace, and Tishya A. L. Wren. 2021. "Biomechanical Symmetry during Drop Jump Landing and Takeoff in Adolescent Athletes Following Recent Anterior Cruciate Ligament Reconstruction" Symmetry 13, no. 4: 639. https://doi.org/10.3390/sym13040639