Article Text

Abstract
Background Although complete resolution and recovery occurs in most children with an initial attack of acute pancreatitis (AP), a subset of children may progress to recurrent AP (RAP). RAP has serious effects to the individual and the socioeconomic burden. The aim of this project was to identify the independent risk factors for pediatric RAP so as to provide evidence for its prevention, early diagnosis and treatment.
Methods A retrospective cohort study of children discharged from Tianjin Children’s Hospital from June 2017 to January 2020 was performed. Demographic and clinical variables, treatment strategies, clinical course and outcomes were collected. Independent risk factors of RAP were identified using the logistic regression model.
Results Of the total 96 enrolled children, 30 (31.3%) developed RAP during the follow-up period. The majority (27/30, 90%) of the children with AP developed RAP within 6 months of their first AP attack. The presence of systemic inflammatory response syndrome (SIRS) [odds ratio (OR)=6.652, 95% confidence interval (CI) 1.989 to 22.247], fasting time (OR=1.267, 95% CI 1.104 to 1.583), whether meet all three AP diagnostic criteria (OR=7.438, 95% CI 1.346 to 41.103) and abnormal amylase/lipase value on the seventh day of hospitalization (OR=3.601, 95% CI 0.972 to 13.342) were independent risk factors of RAP in children.
Conclusions Most children who developed RAP had progressed within 6 months after their first episode of AP. RAP was more common in children who met all three AP diagnostic criteria at initial attack and in children with SIRS, long fasting time and abnormal amylase/lipase value on the seventh day of hospitalization.
- gastroenterology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Acute pancreatitis (AP) is increasing in incidence among pediatric population.
A subset of children with AP might progress to recurrent AP (RAP), the natural history of which is poorly understood.
What are the new findings?
Most children who developed RAP had progressed within 6 months after their first episode of AP.
The presence of systemic inflammatory response syndrome, fasting time, whether meet all three AP diagnostic criteria and abnormal amylase/lipase on the seventh day of hospitalization were independent risk factors of RAP in children.
How might it impact on clinical practice in the foreseeable future?
Close follow-up within 6 months after discharge is very necessary.
Enteral nutrition should be started as early as possible provided gastrointestinal function is tolerated in pediatric AP.
Introduction
Acute pancreatitis (AP) is an inflammatory disease characterized by pancreatic enzyme activation. Pediatric AP has increased in incidence to the current estimate of 3.6–13.2/100 0001 in the last two decades.2–4 Its etiology is quite different from that of adults.5 Gallstones, medications, idiopathic and systemic illness are the most common causes of pediatric AP.6 Some AP will develop recurrent AP (RAP), which usually occurs within 5 months of discharge from the hospital.7
RAP has serious effects for the individual on both body and mind; besides, the socioeconomic burden of RAP is significant given the consumption of labor and financial resources. Therefore, identifing risk factors of pediatric RAP is of great significance. The present study collected clinical data of 96 pediatric AP patients that were followed up to determine whether RAP appeared after discharge. Risk factors of RAP were also analyzed using univariate and multiple logistic regressions so as to provide evidence for RAP’s prevention, early diagnosis and treatment.
Methods
Patient characteristics
We conducted a retrospective cohort study of pediatric AP patients discharged from Tianjin Children’s Hospital from June 2017 to January 2020. Identified children were confirmed to have the diagnosis of AP by having two out of three criteria as defined by International Study Group of Pediatric Pancreatitis: in Search for a Cure (INSPPIRE)8: (A) abdominal pain characteristic of pancreatic origin, (B) serum amylase and/or lipase values ≥3 times the upper limit of normal and (C) imaging showing evidence of pancreatitis. Children without complete clinical data or complete treatment (transfer to another hospital), those with previous history of AP and who underwent surgical treatment from admission to the end of follow-up were excluded.
Data collection
Demographic and clinical variables, as well as laboratory parameters (measured within 24 hours after admission), type of images and interpretations, treatment strategies, clinical course and outcomes were recorded based on the hospital files. The severity of AP was classified as mild AP, moderately severe AP or severe AP (SAP) according to the criteria defined by NASPGHAN.9 Systemic inflammatory response syndrome (SIRS) was defined by meeting at least two of the four criteria: tachycardia/bradycardia, tachypnea, hyperthermia/hypothermia or leukocytosis/leukopenia.
Evaluation strategy
The evaluation strategies were not different between AP and RAP. Initial treatment was conservative in all children, including fasting, fluid resuscitation (normal saline), gastrointestinal decompression, acid suppression (using 20 mg omeprazole once a day), parenteral nutrition, antibiotic prophylactic treatment (children without pancreatic necrosis or exudation: using 20 mg/kg latamoxef twice a day; children with pancreatic necrosis or exudation: using 10 mg/kg meropenem every 8 hours with a maximum of 500 mg), trypsin secretion and activity inhibitor (using octreotide at a speed of 0.025 mg/hour with continuous intravenous drip; using ulinastatin at a speed of 0.25 mg/hour with continuous intravenous drip). None of the included patients received radical etiological treatment during their hospitalization. The changes of illness state were closely monitored during the treatment. During the treatment, treatment strategy might vary slightly depending on individual situation. Children would be discharged when their symptoms were completely relieved and the serum amylase and lipase levels droped below three times the upper limit of normal or imaging changes of pancreas were significantly improved .
Follow-up
All children were followed up by outpatient, readmission or telephone. The follow-up content included: (A) whether there was an episode of RAP after discharge and its duration and frequency and (B) whether the children underwent surgical treatment. RAP was defined as two attacks with at least 1 month free interval or less than 1 month if symptoms resolve with complete normalization of enzymes.10
Statistical analysis
Data were analyzed using IBM SPSS V. 26.0 (IBM SPSS Statistics for MAC, USA). Quantitative variables are reported in terms of mean and standard deviation (SD) or median and interquartile range (IQR), according to their distribution. Categorical variables were summarized as frequency counts with percentages. They were compared using the χ2 test or the Fisher’s exact test for categorical variables, and Student’s t-test (normally distributed data) or Mann-Whitney U test (non-normally distributed data) for quantitative variables. Multiple logistic regression models were used to examine the independent predictors of RAP. The covariates incorporated into the multiple regression analysis were the variables that reached p<0.05 in an univariate regression analysis. Results were interpreted based on a level of statistical significance of 0.05.
Results
Characteristics of enrolled children
A total of 156 children met the INSPPIRE criteria for AP from June 2017 to January 2020. Medical records before June 2017 cannot be obtained because of incomplete documentation in electronic medical records. Forty-five were excluded from the study for incomplete clinical data (n=11), incomplete treatment (n=8), previous history of AP (n=22) or undergoing surgical treatment without conservative therapy during hospitalization (n=4). Nine patients undergoing surgery after conservative surgery during follow-up and six patients lost to follow-up were both excluded. Finally, 96 children were included in this study (figure 1). Characteristics of all enrolled children were shown in table 1.
Characteristics of all enrolled children

Children inclusion process. AP, acute pancreatitis; RAP, recurrent acute pancreatitis.
Recurrent episodes of AP
During the follow-up period (median=17.9 months, IQR=9.3–25.3 months), 30 (31.3%) of the 96 children with AP progressed to RAP. The median duration from the time of AP to the onset of RAP was 2.8 months (IQR=1.5–5.0 months). The majority (27/30, 90%) of the children with AP developed RAP within 6 months of their first AP attack (figure 2).
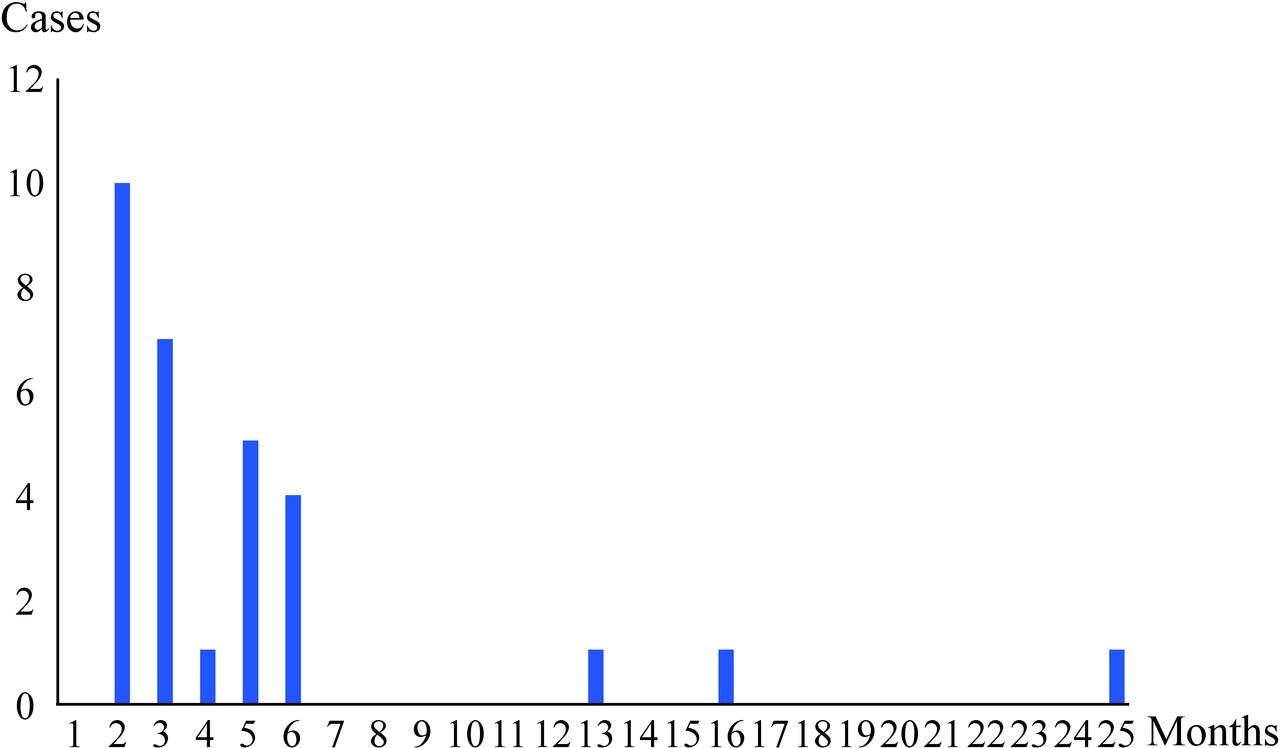
Frequency histogram of RAP after the first attack of AP. AP, acute pancreatitis; RAP, recurrent acute pancreatitis.
Univariate analysis of factors involved in RAP
Several variables were compared between patients with or without RAP. Patients with RAP had longer fasting time than those without RAP (p<0.001). All enrolled children were divided into two groups according to whether they corresponded to all three diagnostic criteria, defined as complete AP (64/96, 66.7%) and incomplete AP (32/96, 33.3%), respectively. The proportion of RAP was higher in children with complete AP than those with incomplete AP (p<0.001). White cell count, the levels of serum amylase and lipase were higher in patients with RAP than that in patients without RAP (p=0.004, 0.025 and 0.015, respectively). The proportion of children with SIRS and abnormal amylase/lipase (above the upper limit of normal) on the seventh day of hospitalization were higher in patients with RAP than that of those without RAP (p<0.001 and p=0.025). Statistically significant variables in table 2 were included in the multiple logistic regression analysis.
Univariate analysis of factors involved in RAP
Multiple logistic regression of factors involved in RAP
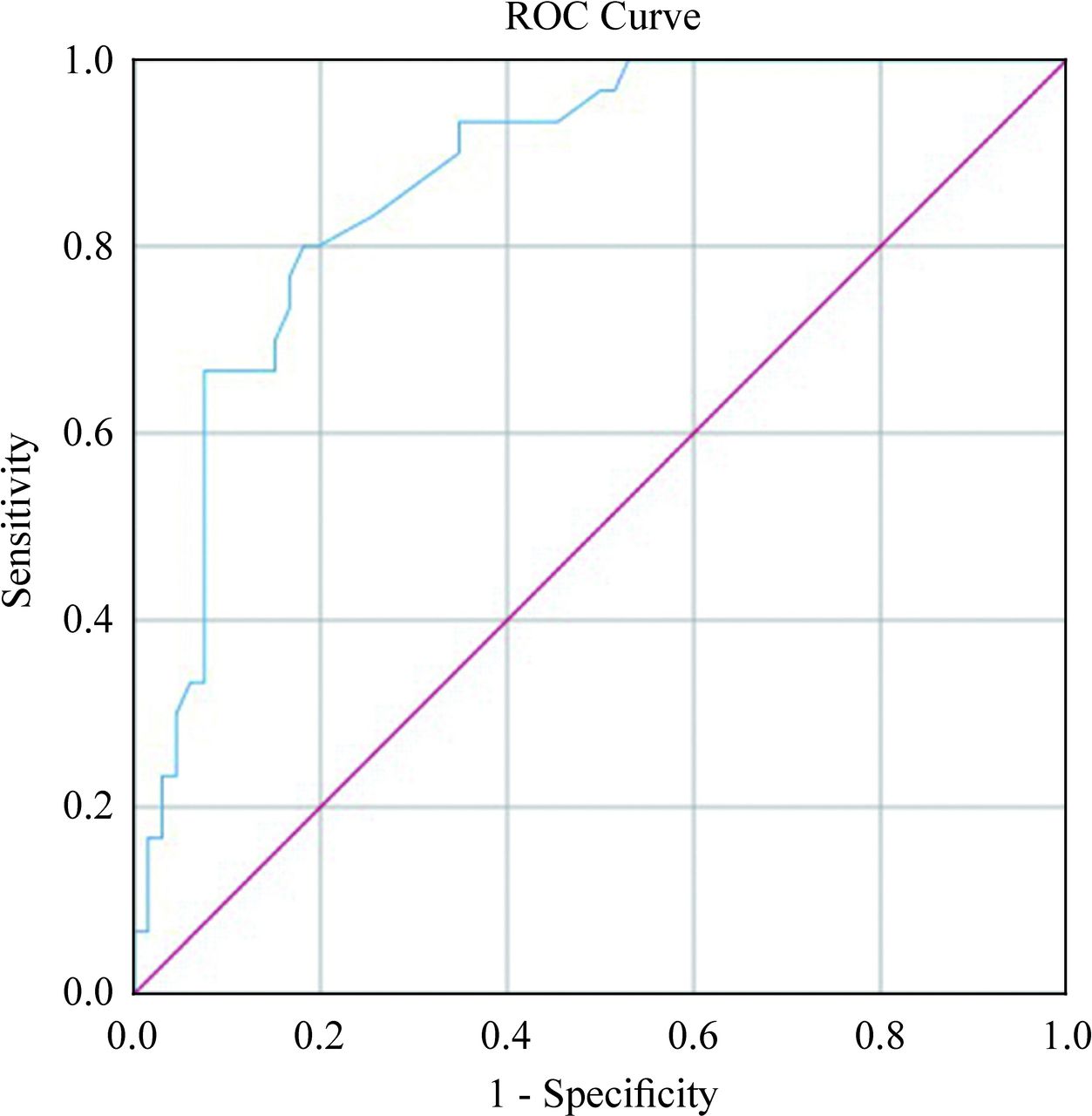
Multiple logistic regression analysis revealed that the presence of SIRS, fasting time, whether meet all three AP diagnostic criteria and abnormal amylase/lipase (above the upper limit of normal) on the seventh day of hospitalization remained significant. Patients who met all three AP diagnostic criteria, with SIRS and abnormal amylase/lipase on the seventh day of hospitalization had higher risk of RAP [odds ratio (OR)=7.438, 6.652 and 3.601, respectively; p<0.001). The risk of RAP in children increased 1.267 times for each additional day of fasting time. These risk factors were considered to be independent predictors of RAP in patients with AP (table 3). The area under the receiver operating characteristic curve of the model was 0.871 (figure 3).
Multiple logistic regression of factors involved in RAP
{kind=link}
{kind=link}
{kind=link}
ROC curve analyses. The AUC of the discrimination model was 0.871. AUC, area under the receiver operating characteristic curve, ROC, receiver operating characteristic curve.
Discussion
Although complete resolution and recovery occurs in most children with an initial attack of AP, a subset of children might progress to RAP.11 12 In this study, we identified a total of 30 (31.3%) children that progressed from AP to RAP, which is consistent with previously published recurrence rates of 10%–35% in the pediatric population13 14 and of 10%–32% in adults.15 16 We also found that the majority of the children (27/30, 90%) that developed RAP had progressed within 6 months after first episode of AP. This finding suggests that close follow-up within 6 months after discharge is very necessary and should be emphasized when giving parental counseling and anticipatory guidance of children.
In this study, RAP was more common in children who met all three AP diagnostic criteria at initial attack and with SIRS, long fasting time and abnormal amylase/lipase (above the upper limit of normal) value on the seventh day of hospitalization. Previous literatures reported that local pancreatic or systemic complications at initial attack and severity of first-time AP were associated with pediatric RAP.7 17 18 However, no literature has been reported about these three factors as independent risk factors of RAP in children.
It has been reported that RAP is closely related to the etiology of the first episode of AP19 and that pancreaticobiliary maljunction (PBM) was one of the major causes of RAP in adults.16 However, we did not observe this conclusion in the present study of our pediatric population. First, only children with abnormal ultrasound/ CT finding may receive MRI examination (n=26) in this center, which may result in the omission of biliopancreatic disease. In addition, some children received radical surgical treatment during hospitalization (n=4) or within a short time after discharge (n=9), which might cover up RAP and bias the results. Through follow-up, we found that these children had a good prognosis without RAP. Therefore, etiological surgical treatment for AP can effectively prevent RAP.
Children with AP were confirmed by meeting at least two of three INSPPIRE criteria.8 However, there are many pediatric AP patients that meet only two diagnostic criteria. We found that these children had a faster recovery and a better prognosis given the mild condition. At present, the treatment of pediatric AP is controversial. Early enteral nutrition is thought to be beneficial20 21 but is rarely performed.22 It is accepted that no antibiotic treatment should be given unless there is clear evidence of infection.23 In addition, the efficacy of protease inhibitors24 25 and somatostatin 26 27 is uncertain. Therefore, grouping children in this way can be considered in future research to explore more favorable treatment methods. Incomplete AP may not require complex management that necessitates longer hospitalization.
SIRS status can be used to identify children at risk for the development of SAP.28 Serum amylase and lipase are the most widely used enzymes for assessment of AP. In our cohort, children were retested on the fourth and seventh day of hospitalization. Abnormal amylase/lipase were found in 49 (51%) children on the fourth and 19 (19.8%) children on the seventh day of hospitalization. We found that SIRS and abnormal amylase/lipase on the seventh day of hospitalization were both independent risk factors of RAP, which reflected a severe inflammatory response and severe pancreatic injury. SIRS and elevated amylase/lipase levels are caused by the release of large amounts of cytokines and trypsin into the blood. The presence of SIRS indicates local inflammation spreading throughout the system, which leaves potential inflammatory factors even after effective treatment and can cause RAP under certain triggers. These factors may offer an objective metric to assess for those children at risk of developing RAP.
The start time of enteral nutrition is of great significance. At present, it is believed that the earlier the enteral nutrition begins, the better the prognosis of the disease. It can prevent ectopic intestinal flora, reduce the risk of complications (mortality, infection and multiple organ failure) and shorten hospital stay.20 21 29 We found that longer fasting time is one of the independent risk factors of pediatric RAP. Moreover, there was a significant correlation between fasting time and hospitalization time (p<0.0001, r2=0.5961). Therefore, enteral nutrition should be started as early as possible provided gastrointestinal function is tolerated in pediatric AP.
There are limitations to our study worth noting. This is a retrospective cohort study, so that there was no initial protocol and led to partial missing clinical data. MRI was not performed in all children, which might have caused some of the cases to be erroneously labeled as idiopathic AP. Moreover, the sample size is small, so that the results may not be generalizable, and some variables cannot be statistically processed. The number of RAP was small, which may limit the statistical processing and bias the results.
In conclusion, most children who developed RAP had progressed within 6 months after their first episode of AP. Patients with AP who met all three AP diagnostic criteria at initial attack and with SIRS, longer fasting time and abnormal amylase/lipase value on the seventh day of hospitalization are associated with higher risk of RAP.
References
Footnotes
QZ and XY contributed equally.
Contributors QZ and XY contributed to conceptualisation and writing original draft. LG, SZhang and YS were involved in investigation. JJ, SZhao, XX, RD, QG and JZhao contributed to formal analysis. JZhan contributed to resources, writing review and editing.
Funding This study was funded by the National Natural Science Foundation of China (grant number 81570471), Xinjiang Uygur Autonomous Region Science Foundation Projects (grant number 2019D01A12) and Tianjin Health Bureau special grant (grant number 14KG129).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the local ethical committee (L2020-24).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data included in this paper are available on reasonable request.