
Abstract
Worry is a central process in a wide range of psychopathological and somatic conditions. Three studies (N = 856) were used to test whether a subscale composed of five items of the most commonly used trait anxiety questionnaire, Spielberger’s State Trait Anxiety Inventory-Trait version (STAI-T), is appropriate to measure worry. Results showed that the subscale, named the Brief Worry Scale (BWS), had excellent internal consistency and temporal stability. Convergent and divergent validity were supported by correlation analyses using worry questionnaires and measures of anxious arousal and depression. The BWS was a particularly good predictor of the pathogenic aspects of worry, including worry perseveration in daily life (study 1), measures of clinical worry (study 2) and the uncontrollability of experimentally induced worry (study 3). Taken together, these studies demonstrate that the BWS might be a valuable scale for pathological worry, for which many researchers already have data.
Similar content being viewed by others

Introduction
Perseverative cognition, such as excessive worry and rumination, has been recognized as a central pathogenic process in psychopathology (Harvey et al., 2004) and somatic illness (Brosschot et al., 2006). According to the perseverative cognition hypothesis (Brosschot et al., 2006), perseverative cognition prolongs the psychophysiological stress response, by prolonging the mental representation of stressful events beyond their actual presence. This prolonged stress response has been suggested to lead to somatic as well as psychological stress related pathology, including health complaints (Brosschot & Van Der Doef, 2006), cardiovascular disease (Kubzansky et al., 1997) and mood and anxiety disorders. A recent meta-analysis showed that perseverative cognition was related to a range of physiological concomitants including increased heart rate, blood pressure, cortisol, and lower heart rate variability (Ottaviani et al., 2016).
Despite the mounting evidence supporting this hypothesis, more studies are needed that precisely investigate how perseverative cognition contributes to psychopathology and somatic illness. For this purpose there are several questionnaires available that measure worry and the related construct of rumination, all of which show promising psychometric properties. These questionnaires include the Penn State Worry Questionnaire (PSWQ), assessing the pathological aspects of worrying, such as its uncontrollability and the Worry Domains Questionnaire (WDQ) which measures worry content (see Verkuil et al., 2007; Davey, 1993). To measure rumination, the Ruminative Response Scale (RRS) is often used (Treynor et al., 2003; Bagby et al., 2004). However, there might be much more evidence available in existing datasets. The Trait Anxiety subscale of the State Trait Anxiety Inventory (STAI-T) is one of the most frequently used instruments in studies of the effects of stress and anxiety on health outcomes (see for example Fisher and Durham (1999) for a short overview of studies using the STAI-T in evaluating effectiveness of GAD treatments).
The STAI-T contains five items that also seem to measure worry, especially its pathological aspects, i.e., worry perseveration (‘I worry too much over something that really doesn’t matter’; ‘I have disturbing thoughts’; ‘Some unimportant thought runs through my head and that bothers me’; ‘I take disappointments so keenly that I can’t put them out of my mind’ and ‘I get in a state of tension or turmoil if I think over my recent concerns and interests’). If these items can be used to reliably measure worry, the aforementioned datasets are theoretically open to explore relationships of worry with several health outcomes. It is not yet clear whether these five items form a scale that reliably predicts worry, although in a previous study it has been suggested that these items measure aspects of anxiety whereas the other remaining items of the STAI-T seem to tap into general negative affect or even depressive affect (Bieling et al., 1998). Most studies that have used the STAI-T have typically looked at anxiety as one construct, instead of investigating the independent effects of perseverative cognition (worry) and affect (anxiety) on health outcomes. Anxious apprehension (worry) and anxious arousal are considered separate constructs (Sharp et al., 2015), and worry, especially its perseveration is believed to be the central pathogenic element of anxiety and several other psychopathologies (Harvey et al., 2004; Davey & Levy, 1998; Borkovec et al., 1998). Moreover, in the somatic pathology domain, worry seems to have adverse effects on cardiac functioning independent of negative affect (Brosschot et al., 2007; Pieper et al., 2007; Ottaviani et al., 2016).
Previously, we provided evidence that of the PSWQ, the WDQ and the STAI-T, the PSWQ is the best predictor of worry in daily life. In the first study, using the same data plus additional subjects from subsequent waves of the study, we more specifically investigate the psychometric quality of the five worry items of the STAI-T, termed Brief Worry Scale (BWS), and whether the BWS can be used to measure trait worry (as measured by the PSWQ), as well as worry in daily life (as measured using ecological momentary assessments). Furthermore, the PSWQ was found to explain only 24% of the variance of daily worry. Therefore, a second goal was to examine whether such a brief, STAI-based questionnaire might in fact explain additional variance in daily worry behavior.
In the second study, we extend this further by examining if the five worry items of the STAI-T, taken together, are related to other measures assessing the same construct, and if it is unrelated to measures evaluating constructs that should have no relationship. Specifically, we expected that the BWS would be highly related to measures of pathological worry (PSWQ and the Generalized Anxiety Disorder Questionnaire for DSM-IV (GADQ-IV; Newman et al., 2002), but not correlated, or much weaker, to measures merely tapping into anxious-arousal and depressive affect. As the GADQ-IV can be used as a screening device to determine whether GAD diagnosis is likely present (Newman et al., 2002), we tested if higher scores on the BWS were associated with an increased likelihood of a GAD diagnosis. Additionally, the second study was completed across three time points, where the BWS measure was used across each time point, allowing us to examine the test-retest reliability of the BWS. Because the GADQ-IV was also collected across these three time points, we were also able to test the ability of the BWS to predict changes in GAD symptoms. Thus, the second study aimed to establish the convergent and divergent validity of the BWS, as well as the test-retest reliability.
In a third study, we tested if the BWS is associated with the uncontrollability of worry when this worrying is induced in an experimental setting. If the BWS indeed taps into pathological aspects of worry, it should be predictive of its uncontrollability, a cardinal feature of worry in GAD patients (Craske et al., 1989).
Given sufficient psychometric qualities established by the three studies, a brief worry scale would be available for many researchers, and a huge number of existing datasets might potentially be reanalyzed to examine the psychopathological and pathophysiological effects of worry.
Study 1
Participants
As part of a first year course in psychology, 1030 students were asked to complete the trait questionnaires and keep a log of their worries (see below). However, after the six-day registration period, 24.8% of the sample failed to return their worry logs. Complete data were available for 683 participants. We previously reported on the first 432 of the subjects in a different study. The mean age of the sample was 21.73 (SD = 5.83) and 76.7% of the sample was female. Participants received course credit for their participation.
Questionnaires
State-Trait Anxiety Inventory-Trait Form (STAI-T; Dutch version: Defares, Van der Ploeg, & Spielberger, 1980). To measure trait anxiety we administered the trait version of the State-Trait Anxiety Inventory. It consists of 20 self-report items that are rated on a Likert scale ranging from 1 (almost never) to 4 (almost always). Earlier use has shown good internal consistency and validity (van der Ploeg et al., 1980). For the purpose of this study we divided the STAI-T into two subscales: the Brief Worry Scale (BWS; by summing up the scores on items 9, 11, 17, 18 and 20; see Table 2) and the remaining negative affectivity items (NA).
Penn State Worry Questionnaire (PSWQ; Meyer et al., 1990; Dutch Translation: Van Rijsoort, Emmelkamp, & Vervaeke, 1999). This questionnaire consists of 16 self-report items. Items are directed at the excessiveness, duration and uncontrollability of worry as experienced in clients diagnosed with GAD, for example: “Once I start worrying, I can’t stop”. Each item is rated on a 1–5 scale, with anchors at 1 (Not at all typical), 3 (Somewhat typical) and 5 (Very typical). The total sum score on the PSWQ has demonstrated high reliability as well as high temporal stability and substantial validity in the assessment of trait worry (Meyer et al., 1990; van Rijsoort et al., 1999).
Worry Log. The worry log is a one-page A4 form validated in previous studies by Brosschot and Van Der Doef (2006), Verkuil et al. (2007) and Versluis et al. (2016). On this form an adapted version of Borkovec et al.’s (1983) working definition of worry is given. In the present study, all participants were instructed to register their worries during six days by tallying each worry episode. More specifically, they were instructed to register a worry episode whenever they noticed that they were worrying, or immediately after they had been worrying. At the end of each day they were asked to estimate the total number of worry episodes (daily worry frequency) and the total duration of these episodes (in minutes), based on their tallies. Each morning, they were requested to estimate the frequency and total duration of any nightly worry episodes (worry frequency and duration in the night-time). To obtain measures of worry perseveration, we decided to regress worry duration (total and during the nighttime) on worry frequency (total and during the nighttime) and to use the residuals of these models as indices of total worry perseveration and worry perseveration during the nighttime. The residuals from these analyses reflected the variance in worry duration that is not simply accounted for by frequently occurring worry episodes - frequent but short worry episodes might reflect successful problem solving - but more purely by their perseveration. Subsequently, these worry perseveration indices were regressed on the trait questionnaires.
Statistical Analyses
Data were screened for normality and outliers. The distributions of the worry duration and worry frequency variables were positively skewed and were transformed using square root transformations.
Psychometric aspects of the BWS were analyzed using reliability analysis (to test internal consistency) and a confirmatory factor analysis (CFA; to test for the proposed unidimensional factor structure of the BWS). To correct for deviations of multivariate normality of the item-data (which are scores on Likert scales), we used diagonally weighted least squares (WLSMV) to estimate the parameters of the CFA model, which is specifically designed for ordinal data. The comparative fit index (CFI), Tucker–Lewis index (TLI), the root mean square error of approximation (RMSEA), and the standardized root mean squared residual index (SRMR) were used to assess model fit. The cutoffs for good model fit were CFI and TFI values of 0.95 or greater (Hu & Bentler, 1998), RMSEA and SRMR values of 0.08 or lower (Browne & Cudeck, 1992). The predictability of worry duration, worry frequency and worry perseveration by trait questionnaires was analyzed with Pearson correlations and linear regression analyses. To test if the association between the BWS and the PSWQ was stronger than the association between the BWS and the NA items of the STAI-T, Steiger’s z-tests were used (Steiger, 1980). CFA analyses were conducted using R studio, version 1.3.1093 (RStudio Team, 2020), using the lavaan package (Rosseel, 2012). The remaining analyses were done using SPSS.
Results Study 1
Descriptive Statistics
Means and standard deviations of the main variables are presented in Table 1. Missing values resulted in the exclusion of some participants from some analyses; listwise exclusion of participants with missing values led to a sample size of 683 – results remained similar when using this dataset.
The mean scores on the PSWQ (M = 44.11, SD = 12.76) and the STAI-T (M = 37.31, SD = 8.95) are within the normal range for healthy subjects and are comparable with mean scores found in other studies (Brosschot & Van Der Doef, 2006; Tallis et al., 1994). On average, participants worried 144 min, which means 24 min on average per day, which is comparable to previous studies using momentary assessments of worry (Verkuil et al., 2007; Brosschot & Van Der Doef, 2006). The participants that did not return their worry logs did not significantly differ on the PSWQ and the STAI-T from those who did return their logs.
Psychometric Aspects of the BWS
The mean score on the BWS was 9.15 (SD = 3.00). The mean score on the remaining NA items of the STAI-T was 28.16 (SD = 6.59). To examine the internal consistency of the two subscales of the STAI-T, two reliability analyses were conducted. Results showed that Cronbach’s α of the BWS was .83, suggesting a satisfactory internal reliability. Removal of any of the five items led to decreases in reliability (alpha; see Table 2). In addition, Cronbach’s α of the NA items was .88.
To examine the structural validity of the BWS a CFA (using WLSMV to estimate the parameters) was conducted. A good fit was observed for the model where all items loaded on one latent factor (for factor loadings see Table 2; CFI = 0.999, TLI = 0.998, RMSEA = 0.016 [90% CI: 0.00–0.057], SRMR = 0.010).
Association of the BWS with Trait Worry and Daily Worry
Table 3 shows the correlations between the trait questionnaires. The BWS was significantly associated with the PSWQ (r(681) = .795, p < .001) and, to a lesser extent, also with the negative affectivity items of the STAI-T (r(681) = .698, p < .001). The negative affectivity items were also associated with the PSWQ (r(681) = .682, p < .001). When controlling for negative affectivity, the partial correlation between the BWS and the PSWQ was still substantial and significant (r(680) = .608, p < .001). To test whether the BWS was more strongly associated with the PSWQ than with the NA items, Steiger’s z tests were conducted (Steiger, 1980). The results indicated that the association between the BWS and the PSWQ was significantly stronger than the association between the BWS and the NA items (z = 5.40, p < .001). The difference between the association between NA and the BWS and the association between the NA items and the PSWQ was not statistically significant (z = .94, p = .34).
Next, we examined the predictive validity of the BWS by examining the associations with worry in daily life. Correlations between the BWS, PSWQ and the NA-items with worry frequency and worry duration in daily life are presented in Table 4. Results show that worry duration was associated with the PSWQ, the BWS and the NA-items respectively, whereas worry frequency was associated with the PSWQ, the NA-items, and the BWS respectively.
Linear forced entry regression analyses were conducted to examine whether the BWS predicted total worry duration in daily life, independent of negative affectivity and the PSWQ. We therefore entered NA and the BWS in the first step, followed by the PSWQ in the second step. Results are presented in Table 3. Total worry duration was predicted by the PSWQ (β = .24, p < .001), the BWS (β = .16, p = .008), and by NA (β = .13, p = .006). With respect to total worry frequency, the predictive strength of the BWS seemed to be accounted for by the PSWQ, as the BWS only predicted worry frequency in the first step (β = .17, p < .001), but not when the PSWQ was entered into the model. In the final model total worry frequency was predicted by the PSWQ (β = .20, p = .001) and NA (β = .19, p < .001), and not by the BWS (β = .05, p = .42).
To examine if the BWS predicted the worry perseveration indices, linear regression analyses were conducted. Results showed that total worry perseveration was best predicted by the BWS (β = .17, p = .009), the PSWQ (β = .13, p = .036), but not by the NA-items (β = .01, ns; see also Table 5). Furthermore, worry perseveration in the night was best predicted by the BWS (β = .14, p = .036), but not by the PSWQ (β = .10, ns) and the NA-items (β = −.02, ns).
Study 2
In a second study we aimed to extend these finding by further examining the convergent and divergent validity of the BWS. Specifically, we expected that the BWS would be highly related to measures of pathological worry (PSWQ and the Generalized Anxiety Disorder Questionnaire for DSM-IV (GADQ-IV; Newman et al., 2002), but not correlated, or much weaker, to measures merely tapping into anxious-arousal and depressive affect.
Participants
Participants were 143 undergraduate students at a large Mid-western university, ages 18–40 years old (M = 19.16, SD = 2.23). Data were collected across three sessions, at two 3-week (M = 20.15 days, SD = 3.71) intervals and one 6-week (M = 40.21 days, SD = 3.13) interval. Complete data were available for 120 participants. Participants were taking part in a larger study on the risk factors associated with depression. To increase the likelihood that the sample would include participants who were at elevated risk for depressive symptoms, potential participants were screened using the Persistence and Low Distraction subscale of the Effortful Control Scale (ECS-PLD; Lonigan, 1998) and the trait version of the Positive and Negative Affect Schedule (T-PANAS; Watson et al., 1988) and recruited based on their scores (see Vasey et al., 2014). Specifically, all individuals in the prescreening pool who scored above the median or in the lower quartile on negative affect (i.e., those high or low on negative affect) and in the upper or lower quartiles on ECS-PLD (i.e., those high or low in effortful control) and positive affect (i.e., those high or low in positive affect) were invited to participate along with a random subset of 10 % of the remainder of the sample. Thus, this sample varied widely in risk for depressive symptoms. Participants came to the laboratory near the beginning, middle, and end of the quarter and received course credit for their participation.
Questionnaires
State-Trait Anxiety Inventory-Trait Form (STAI-T; Spielberger et al., 1983)
To measure anxiety, a subscale of the STAI-T was utilized–the Brief Worry Scale (BWS; items 9, 11, 17, 18 and 20; see Table 2). The remaining items made up the negative affectivity subscale (STAI-NA). All items were rated by the participants on a Likert scale ranging from 1 (almost never) to 4 (almost always).
The Generalized Anxiety Disorder Questionnaire for DSM-IV (GADQ-IV; Newman et al., 2002)
The GADQ-IV is comprised of 9 items, with five yes/no questions assessing the occurrence of excessive, uncontrollable worry (e.g., “Do you find it difficult to control your worry (or stop worrying) once it starts?”), the number of endorsed worry themes and physical symptoms (e.g., muscle tension, irritability), and two questions assessing the amount of interference and distress caused by worry and its symptoms, scored on a 0 (none) to 8 (very severe) scale. The GADQ-IV has demonstrated good sensitivity (83%) and specificity (89%) for structure interview-based diagnosis of GAD, adequate test-retest reliability (κ = .67) as well as both convergent and discriminant validity (Newman et al., 2002). There are several ways to score the GADQ-IV. As described by Newman et al. (2002), items 7–9 are not scored for participants not endorsing the 6-month duration criterion (i.e., item 6). A cut-off score of 5.7 on this scale has been suggested to achieve optimal sensitivity (83%) and specificity (89%) when screening for the presence and absence of diagnosable GAD in student samples (Newman et al., 2002).
The Depression, Anxiety, and Stress Scale (DASS; Lovibond & Lovibond, 1995)
The DASS is a 42-item self-report questionnaire designed to measure the three related negative emotional states of depression, anxiety and stress. Each of the three DASS scales contains 14 items, rated on a 0–3 Likert scale based on how much or how often they applied during the past week (never - almost always). The Depression scale (DASS-D) assesses dysphoria, hopelessness, devaluation of life, self-deprecation, lack of interest/involvement, anhedonia, and inertia. The Anxiety scale (DASS-A) measures primarily symptoms of autonomic hyperarousal (i.e., anxious arousal). The Stress scale (DASS-S) captures difficulty relaxing, nervous arousal, irritability, and impatience. Scores for the Depression, Anxiety and Stress subscales are calculated by summing the scores for the relevant items. This scale has been shown to possess adequate psychometric properties (Lovibond & Lovibond, 1995). In contrast to the DASS-A and DASS-D, DASS-S scores are significantly elevated in GAD patients (Brown, Chorpita, Korotitsch, & Barlow, 1997).
Penn State Worry Questionnaire (PSWQ; Meyer et al., 1990)
This questionnaire consists of 16 self-report items, assessing the tendency to worry excessively and uncontrollably. Each item is rated on a 1–5 scale, with anchors at 1 (not at all typical), 3 (somewhat typical) and 5 (very typical). The PSWQ has demonstrated high reliability as well as high temporal stability and substantial validity in the assessment of trait worry (Meyer et al., 1990).
Statistical Analyses
To examine the internal consistency of the two subscales of the STAI-T, reliability analyses were conducted. To assess the test-retest reliability of the BWS across the three time points, Pearson correlations were computed. To test the convergent and divergent validity of the BWS, partial correlations were computed. To assess convergent validity, partial correlations were conducted to investigate the relationship between the BWS and the GADQ-IV, PSWQ, and DASS-S, controlling for the STAI-NA. To investigate divergent validity partial correlations between the BWS and the DASS-A and DASS-D, when controlling for the STAI-NA were computed. (Logistic) regression analyses were performed to test if the BWS was associated with changes in GAD symptoms across time and with diagnostic status. All analyses were conducted using SPSS.
Results Study 2
Descriptive Statistics
At T1, the mean scores on the PSWQ (M = 47.78, SD = 16.84) and the STAI-T (M = 42.48, SD = 12.07) were within the normal range for healthy subjects. However, consistent with a sampling strategy emphasizing risk for depressive symptoms, independent t-tests showed that these scores were significantly higher than in study 1 (PSWQ: t(801) = 2.75, p = .006; STAI-T: t(801) = 5.50, p < .001).
Reliability of the BWS
To examine the internal consistency of the two subscales of the STAI-T, reliability analyses were conducted for each time point. Results indicated a Cronbach’s α for the BWS of .84 at the first time point, .88 at the second time point, and .87 at the third time point. These findings suggest a satisfactory internal reliability.
To examine the test-retest reliability of the BWS assessed at the three data collection sessions across two 3-week intervals and one 6-week interval, correlations were computed. Results indicated strong test-retest reliability, with significant correlations between the BWS at session 1 and session 2 (r(118) = .830, p < .001); session 2 and session 3 (r(118) = .815, p < .001); and session 1 and session 3 (r(118) = .784, p < .001).
Convergent and Divergent Validity
To test the convergent and divergent validity of the BWS, zero-order and partial correlations were conducted. These correlations are presented in Table 6. In examining convergent validity, the relationship between the BWS T1 and the GADQ-IV (T1 and T3), PSWQ T1, and DASS-S T1 were assessed, controlling for STAI-NA T1. The results suggest that the BWS is uniquely and significantly positively correlated with the GADQ-IV, PSWQ, and DASS-S, indicating convergent validity. In assessing divergent validity, the association between the BWS and the DASS-D and DASS-A were examined, controlling for STAI-NA. As expected, the correlations between the BWS, DASS-D and DASS-A are weaker, with the BWS and DASS-D being uncorrelated, when controlling for trait NA. In contrast, the partial correlation between DASS-D and STAI-NA was r(117) = .602, p < .001, when controlling for the BWS.
BWS and GAD Symptoms
To examine if the BWS was associated with changes in GAD symptoms, a regression analysis was conducted. This showed that the BWS at T1 significantly predicted GADQ-IV at T3 (β = .263, p = .006) above and beyond GADQ-IV at T1 (β = .598, p < .001). In contrast, the NA score did not (β = −.021, p = .807).
Having demonstrated a strong association between the BWS and the severity of GAD symptoms, we additionally tested if the BWS was associated with the likelihood of a GAD diagnosis. This was done to illustrate the potential clinical significance of the findings (Rutledge & Loh, 2004). Using the cut-off score of 5.7 on the GADQ-IV showed that in 25% (n = 30) of the participants a diagnosis of GAD was likely present. GADQ-IV based diagnostic status was used as dependent variable in a logistic regression, with the BWS as predictor. The results showed that every 1-point increase on the BWS was associated with a 76% increase in risk for receiving a GAD diagnosis (OR = 1.762, 95% CI 1.436–2.160, p < .001). Compared to the odds of participants scoring below the median of 11 on the BWS, the odds of a GAD diagnosis was 27 times higher in participants scoring above the median (OR = 27.818, 95% CI 7.688–100.657, p < .001). When looking at the likelihood of a GAD diagnosis at T3, a 1-point increase in the BWS at T1 increases odds of a diagnosis at T3 by 33% (OR = 1.331, 95% CI 1.111–1.594, p = .002) above and beyond what was predicted by diagnosis at T1 (OR = 7.028, 95% CI 1.993–24.776, p = .002).
Study 3
If the BWS indeed taps into pathological aspects of worry, it should be predictive of its uncontrollability, a cardinal feature of worry in GAD patients (Craske et al., 1989). In a third study, we therefore tested if the BWS is associated with the uncontrollability of worry when this worrying is induced in an experimental setting.
Participants
The sample consisted of 18 male and 35 female students, aged 17–50 (M = 24.4) that we have previously reported on (Verkuil et al., 2009). The main aim of the study was to compare cardiac responses to induced worry versus problem solving. Here, to further test the validity of the BWS, we tested the associations between the BWS, STAI-NA, PSWQ and the uncontrollability of worry experienced during the induced worry bout. Participants were recruited by advertisement. After the experimental conditions, the participants completed questionnaires and were paid 6 euros or received course credits.
Procedure
After giving informed consent, all participants took part in three experimental tasks: a worry induction, a cognitive problem solving task and a relaxation induction (we report only on the worry induction task). The experimental conditions were presented in counterbalanced order. Each condition lasted 10 min. During the whole experiment cardiac activity was recorded. Participants also completed the PSWQ and the STAI-T (as in the previous studies).
Worry Induction
Following the work of Borkovec and others (Lyonfields et al., 1995; Thayer et al., 1996), participants were asked to write down three personal worry topics, before receiving further instructions. To minimize participant’s social evaluative concerns about writing down a personal worry topic, they were notified that they could take home or destroy the paper on which they wrote their worry topic. Thereafter, participants were asked ‘to worry as you usually do’ for ten minutes.
(Un)Controllability of Induced Worry
After the worry induction, participants were asked to rate the extent to which they felt their worrisome thoughts were controllable, on a scale from 0 (not at all) to 10 (very much).
Statistical Analyses
Associations between the BWS, STAI-NA, PSWQ and the uncontrollability of worry were analyzed with Pearson correlations and linear regression analyses. For all analyses, SPSS was used.
Results Study 3
Descriptive Statistics
The mean scores on the PSWQ (M = 47.30, SD = 13.77) and the STAI-T (M = 40.65, SD = 10.85) are within the normal range for healthy subjects. The mean uncontrollability of the worrisome thoughts was 5.07 (SD = 1.91, range: 2–10).
Reliability of the BWS
The mean score on BWS was 9.73 (SD = 3.30). The mean score on the remaining NA items of the STAI-T was 30.90 (SD = 8.06). The reliability analyses indicated a Cronbach’s α for the BWS of .85, suggesting a satisfactory internal reliability.
BWS and Controllability of Worrying
Pearson correlations showed that controllability of induced worry was negatively associated with the BWS (r(51) = −.662, p < .001), the PSWQ (r(51) = −.645, p < .001) and the STAI-NA (r(50) = −.574, p < .001) respectively.
Linear forced entry regression analyses were conducted to examine whether the BWS predicted controllability of worry during the worry episode, independent of negative affectivity and the PSWQ. We therefore entered NA and the BWS in the first step, followed by the PSWQ in the second step. In step 1, worry intensity was predicted by the BWS (β = −.546, p < .01)), but not the STAI-NA (β = −.150, p > .37). In the second step, both the BWS (β = −.389, p < .05) and the PSWQ (β = −.337, p < .05) predicted controllability of worry, but the STAI-NA did not.
General Discussion
The results of these three studies make clear that five worry-related items of the STAI-T can be used to reliably measure trait worry and state worry in daily life, independent of negative affect. This implies that a huge number of existing datasets might be reanalyzed to examine how the different elements of anxiety (worry and negative affect) affect psychological and somatic illness. We also observed that the BWS was the best predictor of the worry perseveration index, that is, worry duration in daily life corrected for the total number of worry episodes, and it did so even better than the most often used measure of pathological worry, the PSWQ. Moreover, the BWS was the only one of the trait measures that predicted nightly worry. Worry perseveration – the prolongation of worry episodes regardless of its frequency – and nocturnal worry are perhaps the most pathological characteristics of worry, with respect to psychological as well as somatic health (Borkovec et al., 1983; Brosschot et al., 2006). The BWS therefore seems particularly suited to measure the pathological aspects of worry. However, future studies are warranted to replicate this finding, as our measure of worry perseveration is not yet a standardized measure.
In this first study, we also found that the BWS predicted the frequency of worry episodes, although it did so to a lesser extent than the NA items. Moreover, after taking the PSWQ into account, the association between the BWS and worry frequency was not significant. It is perhaps not surprising that the PSWQ, consisting of 16 items, is sensitive to a broader array of features of worry – including frequency - than the shorter BWS. However, as argued above, frequency of worry seems less important as a pathogenic factor. This is also consistent with a study by Thielsch et al. (2015) who found, in a sample of patients suffering from GAD, that momentarily assessed uncontrollability ratings of worry (i.e., pathogenic negative metacognitions about worry) did not predict subsequent worry frequency but did predict worry duration. Frequent but short worry episodes might reflect successful problem solving and seems less detrimental to health, while duration of worry reflects difficulty in stopping worry and involves prolonged stress responses (Brosschot & van der Doef, 2006; Brosschot et al., 2007).
In addition, in the second study we observed a pattern of associations that was consistent with convergent validity. The BWS positively correlated with the GADQ-IV and the PSWQ. These two questionnaires are established measures of pathological worry. The BWS also predicted GADQ-IV scores after 6-weeks above and beyond GADQ-IV at baseline (which the NA items did not). The GADQ-IV is a reliable questionnaire measuring symptoms of GAD, including items on its excessiveness, uncontrollability, and the amount of impairment due to the symptoms. Yet, not every participant scoring above the clinical cut-off of 5.7 will endorse all symptoms of GAD, and a GADQ-IV-based analog diagnosis is probably over-inclusive. That is, even in a sample stratified for levels of depressive symptoms, a 25% base rate of GAD in this sample is considerably higher than would be expected based on base rates in the general population (Somers et al., 2006). Still, the finding that with every 1-point increase in BWS scores there was an associated 76% increased risk for a current GAD diagnosis, and a 33% increased risk for a diagnosis 6 weeks later, over and above what is predicted by current diagnostic status, expresses the potential clinical significance of the BWS.
Out of the three DASS subscales, the BWS most strongly related to the DASS-S subscale, which has previously been shown to be the DASS subscale most closely related to measures of worry and GAD (Brown et al., 1997). The BWS was less strongly related to the DASS-A subscale. The DASS-A subscale primarily measures symptoms of anxious arousal (trembling, difficulty breathing; although one item is focused on worry about having a panic attack). The association between worry and anxious arousal should be modest on average (see Vasey et al., 2017).Footnote 1 In addition, when controlling for negative affect, the association between the BWS and the DASS Depression subscale was not significant anymore. This is indicative of divergent validity, as we would expect a measure of depression to be less related to an index of worry when negative affectivity is partialled out. Taken together these findings demonstrate a pattern of correlations that provide support for the BWS, and its convergent and divergent validity.
With regard to the third study, several studies have demonstrated that people suffering from GAD experience their worries as more uncontrollable than healthy controls (Craske et al., 1989; Hoyer et al., 2001). In the third study, we observed that the BWS predicted the (un)controllability of worrying, experienced during an experimental worry bout, whereas negative affect did not. Even though this was a relatively small non-clinical sample, these data also suggest that the BWS items tap into this pathological aspect of worry. What’s more, the BWS was an equally strong predictor of uncontrollability as the standard measure of pathological worry, the PSWQ, which provides further evidence for the validity of the BWS.
Limitations
There are several methodological limitations. First, all studies were conducted in non-clinical and largely female samples, and one could raise the question to what extent the BWS is useful in measuring pathological worry, as it is observed in clinical populations, especially in GAD patients. Although we did not screen for GAD diagnoses using clinical interviews, several studies suggest that student samples are suitable to investigate worry on the full severity range (Borkovec & Roemer, 1995; Roemer et al., 1995; Ruscio, 2002) and indeed all samples seemed to cover the full worry range. Moreover, Ruscio (2002) showed that although high levels of worry are a main characteristic of GAD, a large group of people who show high levels of worry do not receive a full GAD diagnosis. Still, further validation studies might be conducted that use clinical populations and try to elucidate whether the BWS indeed is a good predictor of pathological worry. Studies with clinical populations could also examine whether the combination of the BWS with the PSWQ leads to a more sensitive measurement of GAD worry and whether this also leads to a better screening instrument for the detection of GAD. Furthermore, although momentary assessments of worry are less prone to retrospective bias than trait questionnaires, the end of day measurements of worry duration that we used in the first study could still lead to overestimations in time spent worrying. This hypothesis could be addressed in future momentary assessment studies using time based random sampling, for example with handheld computers. Finally, the first study was formally restricted to worry, while we assumed that it related to more general perseverative cognition that is central in many psychopathologies. However, we did not include related measures of perseverative cognitions, such as rumination, that is, experiencing repetitive negative thoughts about one’s negative mood (Nolen-Hoeksema, 2000), or measures of intrusive / obsessional thoughts. On the other hand, rumination and intrusive thoughts are closely associated with worry, and may share the same underlying processes (Watkins et al., 2005; Langlois et al., 2000; Segerstrom et al., 2003).
Future Directions
Given that these findings provide preliminary evidence for the reliability and validity of the BWS, existing datasets might potentially be reanalyzed to examine the effects of worry on mental and somatic health. Since the BWS seems to be particularly associated with worry perseveration, the BWS might be a valuable instrument for studying the shared cognitive, neural and affective processes that constitute general perseverative thinking processes.
Recently, during the review process of this paper, a study by Zsido and colleagues was published, in which they set out to develop a short version of the STAI-T. They used a data-driven item-response theory approach to search for 5 items from the 13 non-reversed scored items of the STAI-T that could measure trait anxiety. Four of the final items that were selected (9, 17, 18 and 20) are also present in the BWS. The distinction in the proposed scales is made by a fifth item, which in the BWS is “I have disturbing thoughts” and in the brief STAI-T “I feel that difficulties are piling up so that I cannot overcome them”. These items pertain to different aspects of anxiety, with the former being more clearly directed towards the cognitive aspect of anxiety: worry. This suggests that the BWS might be a more consistent measure of worry, when compared to the brief STAI-T. This idea was backed up by an additional CFA on the brief STAI-T in the first sample, in which the fifth brief STAI-T item – loaded less on the latent factor (.62) than the fifth BWS item (.74). For researchers aiming to specifically measure worry, the BWS might therefore be preferred.
Conclusions
In short, we provided evidence that a short, easy to administer subscale of the STAI-T can be used to measure worry in daily life, especially worry uncontrollability, duration and worry perseveration, which are believed to be central processes in mental as well as somatic health. A questionnaire that reliably predicts perseverative thinking in daily life seems to be of great potential importance. We hope that the findings of the present studies will encourage researchers to inspect existing datasets that include the STAI-T to test the effects of worry perseveration on mental and somatic health outcomes.
Data Availability
The datasets generated during and analyzed during the current study are available in the Open Science Framework repository: https://osf.io/tzf5j/?view_only=5d7b55dbbef84a33bea861ffe531cdcd
Notes
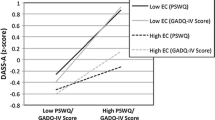
Whereas the Cognitive Avoidance Model (Borkovec et al., 2004) posits that worry is associated with blunted levels of anxious-arousal, the Contrast Avoidance Model (Newman & Llera, 2011) asserts that worry is associated with high levels of anxious-arousal. In fact, both patterns have been observed. The Cognitive Control Model (Vasey et al., 2017) predicts that worry is associated with low levels of anxious-arousal among individuals having sufficient cognitive control to constrain their worry to a verbal mode of processing. In contrast, individuals lacking such control worry predominantly in imagery form. Such worrisome images activate anxious-arousal. Consistent with the latter model, when we tested a regression model predicting DASS-A scores using the BWS and NA scores plus a measure of effortful control (i.e., the Effortful Control Scale – Persistence and Low Distraction subscale [see Vasey et al., 2017], EC was found to significantly moderate the association between the BWS and DASS-A (semi-partial r = −.15, p = .018). BWS scores were significantly positively associated with DASS-A scores only when EC was −.20 SDs below the sample mean or less.
References
Bagby, R. M., Rector, N. A., Bacchiochi, J. R., & McBride, C. (2004). The stability of the response styles questionnaire rumination scale in a sample of patients with major depression. Cognitive Therapy and Research, 28, 527–538.
Bieling, P. J., Antony, M. M., & Swinson, R. P. (1998). The state-trait anxiety inventory, trait version: Structure and content re-examined. Behaviour Research and Therapy, 36, 777–788.
Borkovec, T. D., Alcaine, O. M., & Behar, E. (2004). Avoidance theory of worry and generalized anxiety disorder. Generalized anxiety disorder: Advances in research and practice (pp. 77–108). Guilford.
Borkovec, T. D., Ray, W. J., & Stöber, J. (1998). Worry: A cognitive phenomenon intimately linked to affective, physiological, and interpersonal behavioral processes. Cognitive Therapy and Research, 22, 561–576.
Borkovec, T. D., Robinson, E., Pruzinsky, T., & DePree, J. A. (1983). Preliminary exploration of worry: Some characteristics and processes. Behaviour Research and Therapy, 21(1), 9–16.
Borkovec, T. D., & Roemer, L. (1995). Perceived functions of worry among generalized anxiety disorder subjects: Distraction from more emotionally distressing topics? Journal of Behavior Therapy and Experimental Psychiatry, 26, 25–30.
Brosschot, J. F., Gerin, W., & Thayer, J. F. (2006). The perseverative cognition hypothesis: A review of worry, prolonged stress-related physiological activation, and health. Journal of Psychosomatic Research, 60, 113–124.
Brosschot, J. F., & Van Der Doef, M. (2006). Daily worrying and somatic health complaints: Testing the effectiveness of a simple worry reduction intervention. Psychology & Health, 21, 19–31.
Brosschot, J. F., van Dijk, E., & Thayer, J. F. (2007). Daily worry is related to low heart rate variability during waking and the subsequent nocturnal sleep period. International Journal of Psychophysiology, 63, 39–47.
Browne, M. W., & Cudeck, R. (1992). Alternative ways of assessing model fit. Sociological Methods & Research, 21(2), 230–258.
Brown, T. A., Chorpita, B. F., Korotitsch, W., & Barlow, D. H. (1997). Psychometric properties of the Depression Anxiety Stress Scales (DASS) in clinical samples. Behaviour Research and Therapy, 35(1), 79–89.
Craske, M. G., Rapee, R. M., Jackel, L., & Barlow, D. H. (1989). Qualitative dimensions of worry in DSM-III-R generalized anxiety disorder subjects and nonanxious controls. Behaviour Research and Therapy, 27(4), 397–402.
Davey, G. C. L. (1993). A comparison of three worry questionnaires. Behaviour Research and Therapy, 31, 51–56.
Davey, G. C. L., & Levy, S. (1998). Catastrophic worrying: Personal inadequacy and a perseverative iterative style as features of the catastrophizing process. Journal of Abnormal Psychology, 107, 576–586.
Defares, P. B., Van der Ploeg, H. M., & Spielberger, C. D. (1980). Handleiding bij de Zelf-beoordelings Vragenlijst ZBV. Een Nederlandstalige bewerking van de Spielberger State-Trait Anxiety Inventory.
Fisher, P. L., & Durham, R. C. (1999). Recovery rates in generalized anxiety disorder following psychological therapy: An analysis of clinically significant change in the STAI-T across outcome studies since 1990. Psychological Medicine, 29, 1425–1434.
Harvey, A., Watkins, E., Mansell, W., & Shafran, R. (2004). Cognitive behavioural processes across psychological disorders: A transdiagnostic approach to research and treatment. Oxford University Press.
Hoyer, J., Becker, E. S., & Roth, W. T. (2001). Characteristics of worry in GAD patients, social phobics, and controls. Depression and Anxiety, 13(2), 89–96.
Hu, L. T., & Bentler, P. M. (1998). Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychological Methods, 3(4), 424.
Kubzansky, L. D., Kawachi, I., Spiro III, A., Weiss, S. T., Vokonas, P. S., & Sparrow, D. (1997). Is worrying bad for your heart?: A prospective study of worry and coronary heart disease in the normative aging study. Circulation, 95, 818–824.
Langlois, F., Freeston, M. H., & Ladouceur, R. (2000). Differences and similarities between obsessive intrusive thoughts and worry in a non-clinical population: Study 2. Behaviour Research and Therapy, 38, 175–189.
Lonigan, C. J. (1998). Development of a measure of effortful control in school-age children. Unpublished raw data. Florida State University.
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behaviour Research and Therapy, 33(3), 335–343.
Lyonfields, J. D., Borkovec, T. D., & Thayer, J. F. (1995). Vagal tone in generalized anxiety disorder and the effects of aversive imagery and worrisome thinking. Behavior Therapy, 26(3), 457–466.
Meyer, T. J., Miller, M. L., Metzger, R. L., & Borkovec, T. D. (1990). Development and validation of the Penn State worry questionnaire. Behaviour Research and Therapy, 28(6), 487–495.
Newman, M. G., & Llera, S. J. (2011). A novel theory of experiential avoidance in generalized anxiety disorder: A review and synthesis of research supporting a contrast avoidance model of worry. Clinical Psychology Review, 31(3), 371–382.
Newman, M. G., Zuellig, A. R., Kachin, K. E., Constantino, M. J., Przeworski, A., Erickson, T., & Cashman-McGrath, L. (2002). Preliminary reliability and validity of the generalized anxiety disorder questionnaire-IV: A revised self-report diagnostic measure of generalized anxiety disorder. Behavior Therapy, 33(2), 215–233.
Nolen-Hoeksema, S. (2000). The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. Journal of Abnormal Psychology, 109, 504–511.
Ottaviani, C., Thayer, J. F., Verkuil, B., Lonigro, A., Medea, B., Couyoumdjian, A., & Brosschot, J. F. (2016). Physiological concomitants of perseverative cognition: A systematic review and meta-analysis. Psychological Bulletin, 142(3), 231–259.
Pieper, S., Brosschot, J. F., van der Leeden, R., & Thayer, J. F. (2007). Cardiac effects of momentary assessed worry episodes and stressful events. Psychosomatic Medicine, 69, 901–909.
Roemer, L., Borkovec, M., Posa, S., & Borkovec, T. D. (1995). A self-report diagnostic measure of generalized anxiety disorder. Journal of Behavior Therapy and Experimental Psychiatry, 26, 345–350.
Rosseel, Y. (2012). Lavaan: An R package for structural equation modeling. Journal of Statistical Software, 48(2), 1–36 http://www.jstatsoft.org/v48/i02/.
RStudio Team (2020). RStudio: Integrated development for R. RStudio, PBC, URL http://www.rstudio.com/.
Ruscio, A. M. (2002). Delimiting the boundaries of generalized anxiety disorder: Differentiating high worriers with and without GAD. Journal of Anxiety Disorders, 16, 377–400.
Rutledge, T., & Loh, C. (2004). Effect sizes and statistical testing in the determination of clinical significance in behavioral medicine research. Annals of Behavioral Medicine, 27(2), 138–145.
Segerstrom, S. C., Stanton, A. L., Alden, L. E., & Shortridge, B. E. (2003). A multidimensional structure for repetitive thought: What's on your mind, and how, and how much? Journal of Personality & Social Psychology, 85, 909–921.
Sharp, P. B., Miller, G. A., & Heller, W. (2015). Transdiagnostic dimension of anxiety: Neural mechanisms, executive functions, and new directions. International Journal of Psychophysiology, 98, 365–377.
Somers, J. M., Goldner, E. M., Waraich, P., & Hsu, L. (2006). Prevalence and incidence studies of anxiety disorders: A systematic review of the literature. The Canadian Journal of Psychiatry, 51(2), 100–113.
Spielberger, C. D., Gorsuch, R. L., Lushene, R., Vagg, P. R., & Jacobs, G. A. (1983). State-trait anxiety inventory for adults. Mind Garden.
Steiger, J. H. (1980). Tests for comparing elements of a correlation matrix. Psychological Bulletin, 87, 245–251.
Tallis, F., Davey, G. C. L., & Capuzzo, N. (1994). The phenomenology of non-pathological worry: A preliminary investigation. John Wiley and Sons.
Thayer, J. F., Friedman, B. H., & Borkovec, T. D. (1996). Autonomic characteristics of generalized anxiety disorder and worry. Biological Psychiatry, 39(4), 255–266.
Thielsch, C., Ehring, T., Nestler, S., Wolters, J., Kopei, I., Rist, F., Gerlach, A. L., & Andor, T. (2015). Metacognitions, worry and sleep in everyday life: Studying bidirectional pathways using ecological momentary assessment in GAD patients. Journal of Anxiety Disorders, 33, 53–61.
Treynor, W., Gonzalez, R., & Nolen-Hoeksema, S. (2003). Rumination reconsidered: A psychometric analysis. Cognitive Therapy and Research, 27, 247–259.
van Rijsoort, S., Emmelkamp, P., & Vervaeke, G. (1999). The Penn state worry questionnaire and the worry domains questionnaire: Structure, reliability and validity. Clinical Psychology & Psychotherapy: An International Journal of Theory & Practice, 6(4), 297–307.
Vasey, M. W., Chriki, L., & Toh, G. Y. (2017). Cognitive control and anxious arousal in worry and generalized anxiety: An initial test of an integrative model. Cognitive Therapy and Research, 41, 155–169.
Vasey, M. W., Harbaugh, C. N., Fisher, L. B., Heath, J. H., Hayes, A. F., & Bijttebier, P. (2014). Temperament synergies in risk for and protection against depressive symptoms: A prospective replication of a three-way interaction. Journal of Research in Personality, 53, 134–147.
Verkuil, B., Brosschot, J. F., Borkovec, T. D., & Thayer, J. F. (2009). Acute autonomic effects of experimental worry and cognitive problem solving: Why worry about worry? International Journal of Clinical and Health Psychology, 9(3).
Verkuil, B., Brosschot, J. F., & Thayer, J. F. (2007). Capturing worry in daily life: Are trait questionnaires sufficient? Behaviour Research and Therapy, 45, 1835–1844.
Versluis, A., Verkuil, B., & Brosschot, J. F. (2016). Reducing worry and subjective health complaints: A randomized trial of an internet-delivered worry postponement ontervention. British Journal of Health Psychology, 21(2), 318–335.
Watkins, E., Moulds, M., & Mackintosh, B. (2005). Comparisons between rumination and worry in a non-clinical population. Behaviour Research and Therapy, 43, 1577–1585.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063–1070.
Financial Interests
the authors declare they have no financial or non-financial interests.
Funding
This research was supported by grants from The Ohio State University, Department of Psychology. Bart Verkuil received support from a research grant by the Netherlands Organization for Scientific Research (NWO Veni Grant 451–14-013).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Bart Verkuil, Michael Vasey and Briana Brownlow. The first draft of the manuscript was written by Bart Verkuil and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical Statement and Informed Consent
All procedures performed in the studies were in accordance with the ethical standards of the institutional research committees of the respective study sites and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The studies were approved by the Institutional research committees. Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
all authors report no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Verkuil, B., Brownlow, B.N., Vasey, M.W. et al. A brief scale of pathological worry that everyone already has. Curr Psychol 42, 2868–2879 (2023). https://doi.org/10.1007/s12144-021-01603-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-021-01603-z