
Abstract
Background
Although aortic valve replacement (AVR) when successfully performed boasts low mortality rates in selected patients, prosthesis–patient mismatch (PPM) can be found in the majority of these individuals. Limited research is available supporting the benefit of two-dimensional speckle tracking echocardiography (2D-STE) in patients with severe PPM. This study sought to assess myocardial strain using 2D-STE to determine the relationship between subclinical left ventricular (LV) dysfunction and aortic PPM in patients undergoing AVR with preserved LV ejection fraction.
Material and methods
We retrospectively examined all consecutive patients with isolated AVR who presented to our center from 2005 to 2018. The data of 1086 patients were analyzed. Severe PPM was defined as an indexed effective orifice area of 0.65 cm2/m2 or less. As a result of the detailed assessment, 54 patients meeting the eligibility criteria were included in the study. Baseline data were collected and compared between the two groups of patients with severe PPM (n = 27) and those with normofunctional aortic prosthesis valve as a control group (n = 27). All patients underwent baseline echocardiography. Global longitudinal strain (GLS) and global circumferential strain (GCS) were evaluated by 2D-STE.
Results
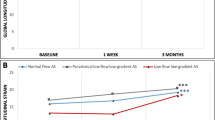
When compared with controls, patients with severe PPM had significantly decreased GLS (18.6 ± 2.9 vs. 21.4 ± 2.1; p < 0.01) and GCS (17.2 ± 3.6 vs. 21.7 ± 2.1; p < 0.01) values.
Conclusion
In addition to standard clinical and echocardiographic parameters, GLS and GCS suggest subclinical dysfunction and have incremental value in patients with severe PPM.
Zusammenfassung
Hintergrund
Auch wenn der Aortenklappenersatz („aortic valve replacement“, AVR) bei erfolgreicher Durchführung niedrige Mortalitätsraten bei ausgewählten Patienten aufweist, findet sich bei der Mehrzahl dieser Personen ein fehlender Abgleich zwischen Prothese und Patient („prosthesis-patient mismatch“, PPM). Es gibt nur wenige Studien, die auf den Nutzen der 2‑dimensionalen Speckle-Tracking-Echokardiographie (2-D-STE) bei Patienten mit schwerem PPM hinweisen. Ziel der vorliegenden Studie war es, die myokardiale Deformierung mittels 2‑D-STE zu bestimmen, um das Verhältnis zwischen subklinischer linksventrikulärer (LV‑)Dysfunktion und Aorten-PPM bei Patienten mit AVR und erhaltener LV-Ejektionsfraktion zu untersuchen.
Material und Methoden
Dazu wurden alle konsekutiven Patienten mit isolierter AVR retrospektiv untersucht, die sich 2005–2018 in der Klinik der Autoren vorstellten. Die Daten von 1086 Patienten wurden ausgewertet. Ein schwerer PPM wurde als eine indizierte effektive Öffnungsfläche von 0,65 cm2/m2 oder weniger definiert. Nach detaillierter Untersuchung wurden 54 Patienten, welche die Eignungskriterien erfüllten, in diese Studie einbezogen. Die Ausgangsdaten wurden erhoben und zwischen der Patientengruppe mit schwerem PPM (n = 27) sowie Patienten mit normofunktionaler Aortenprothesenklappe als Kontrollgruppe verglichen (n = 27). Bei allen Patienten wurde zu Studienbeginn eine Echokardiographie durchgeführt. Der globale longitudinale Strain (GLS) und der globale zirkumferenzielle Strain (GCS) wurden mittels 2‑D-STE bestimmt.
Ergebnisse
Im Vergleich zu den Kontrollen wiesen die Patienten mit schwerem PPM signifikant verminderte GLS- (18,6 ± 2,9 vs. 21,4 ± 2,1; p < 0,01) und GCS-Werte (17,2 ± 3,6 vs. 21,7 ± 2,1; p < 0,01) auf.
Schlussfolgerung
Zusätzlich zu klinischen und echokardiographischen Standardparametern dienen GLS und GCS als Hinweis auf eine subklinische Dysfunktion und haben inkrementellen Wert bei Patienten mit schwerem PPM.
Similar content being viewed by others


References
Rahimtoola SH (1978) The problem of valve prosthesis-patient mismatch. Circulation 58:20–24
Ross J Jr. (1976) Afterload mismatch and preload reserve: a conceptual framework for the analysis of ventricular function. Prog Cardiovasc Dis 18:255–264
Lester SJ, Heilbron B, Gin K et al (1998) The natural history and rate of progression of aortic stenosis. Chest 113:1109–1114
Pibarot P, Dumesnil JG (2006) Prosthesis-patient mismatch: definition, clinical impact, and prevention. Heart 92:1022–1029
Mihaljevic T, Nowicki ER, Rajeswaran J et al (2008) Survival after valve replacement for aortic stenosis: implications for decision making. J Thorac Cardiovasc Surg 135:1270–1278
Pai RG, Varadajan P, Razzouk A (2008) Survival benefit of aortic valve replacement in patients with severe aortic stenosis with low ejection fraction and low gradient with normal ejection fraction. Ann Thorac Surg 86:1781–1789
Perk G, Tunick PA, Kronzon I (2007) Non-doppler two-dimensional strain imaging by echocardiography-from technical considerations to clinical applications. J Am Soc Echocardiogr 20:234–243
Delgado V, Tops LF, van Bommel RJ et al (2009) Strain analysis in patients with severe aortic stenosis and preserved left ventricular ejection fraction undergoing surgical valve replacement. Eur Heart J 30:3037–3047
Kearney LG, Lu K, Ord M et al (2012) Global longitudinal strain is a strong independent predictor of all-cause mortality in patients with aortic stenosis. Eur Heart J Cardiovasc Imaging 13:827–833
Cheitlin MD, Armstrong WF, Aurigemma GP et al (2003) ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography—summary article: a report of the American college of cardiology/American heart association task force on practice guidelines (ACC/AHA/ASE committee to update the 1997 guidelines for the clinical application of echocardiography). J Am Coll Cardiol 42:954–970
Lang RM, Bierig M, Devereux RB et al (2005) Recommendations for chamber quantification: a report from the American society of echocardiography’s guidelines and standards committee and the chamber Quantification writing group, developed in conjunction with the European association of echocardiography, a branch of the European society of cardiology. J Am Soc Echocardiogr 18:1440–1463
Devereux RB, Alonso DR, Lutas EM et al (1986) Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol 57:450–458
Schiller NB, Shah PM, Crawford M et al (1989) Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. American society of echocardiography committee on standards, subcommittee on quantitation of two-dimensional echocardiograms. J Am Soc Echocardiogr 2:358–367
Sanderson JE, Wang M, Yu CM (2004) Tissue Doppler imaging for predicting outcome in patients with cardiovascular disease. Curr Opin Cardiol 19:458–463
Daneshvar S, Rahimtoola SH (2012) Valve prosthesis-patient mismatch (VP-PM): a long-term perspective. J Am Coll Cardiol 60:1123–1135
Pibarot P, Dumesnil JG (2000) Hemodynamic and clinical impact of prosthesis-patient mismatch in the aortic valve position and its prevention. J Am Coll Cardiol 36:1131–1141
Rao V, Jamieson WRE, Ivanov J et al (2000) Prosthesis-patient mismatch affects survival after aortic valve replacement. Circulation 102:5–9
Moon MR, Pasque MK, Munfakh NA et al (2006) Prosthesis-patient mismatch after aortic valve replacement: impact of age and body size on late survival. Ann Thorac Surg 81:481–488
Jin XY, Zhang ZM, Gibson DG et al (1996) Effects of valve substitute on changes in left ventricular function and hypertr ophy after aortic valve replacement. Ann Thorac Surg 62:683–690
Vicchio M, De Santo LS, Della Corte A et al (2008) Aortic valve replacement with 19-mm bileaflet prostheses in the elderly: left ventricular mass regression and quality of life. J Heart Valve Dis 17:216–221
Garatti A, Mori F, Innocente F et al (2011) Aortic valve replacement with 17-mm mechanical prostheses: is patient-prosthesis mismatch a relevant phenomenon? Ann Thorac Surg 91:71–77
Florath I, Albert A, Rosendahl U et al (2008) Impact of valve prosthesis-patient mismatch estimated by echocardiographic determined effective orifice area on long-term outcome after aortic valve replacement. Am Heart J 155:1135–1132
Mohty-Echahidi D, Malouf JF, Girard SE et al (2006) Impact of prosthesis-patient mismatch on long-term survival in patients with small St Jude Medical mechanical prostheses in the aortic position. Circulation 113:420–426
Staron A, Bansal M, Kalakoti P et al (2013) Speckle tracking echocardiography derived 2‑dimensional myocardial strain predicts left ventricular function and mass regression in aortic stenosis patients undergoing aortic valve replacement. Int J Cardiovasc Imaging 29:797–808
Mizia-Stec K, Mizia M, Sikora-Puz A et al (2016) Prosthesis-patient mismatch and left ventricle systolic strain in patients with severe degenerative aortic stenosis who are undergoing surgical valve replacement. Kardiol Pol 74:537–546
Pibarot P, Weissman NJ, Stewart WJ et al (2014) Incidence and sequelae of prosthesis-patient mismatch in transcatheter versus surgical valve replacement in high-risk patients with severe aortic stenosis: a PARTNER trial cohort—a analysis. J Am Coll Cardiol 64:1323–1334
Poulin F, Yingchoncharoen T, Wilson WM et al (2016) Impact of prosthesis patient mismatch on left ventricular myocardial mechanics after transcatheter aortic valve replacement. J Am Heart Assoc 5(2):e2866
Schoen FJ, Levy RJ (1999) Founder’s award, 25th annual meeting of the society for biomaterials, perspectives. Providence, RI, April 28-May 2, 1999. Tissue heart valves: current challenges and future research perspectives. J Biomed Mater Res 47:439–465
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
A. Ösken, Ş. Ünal Dayı, K.S. Özcan, M. Keskin, T. Kemaloğlu Öz, E. Poyraz, U. Gürkan, H. Akgöz and N. Çam declare that they have no competing interests.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional informed consent was obtained from all individual participants for whom identifying information is included in this article.
Rights and permissions
About this article

Cite this article
Ösken, A., Ünal Dayı, Ş., Özcan, K.S. et al. Speckle tracking echocardiography in severe patient–prosthesis mismatch. Herz 46, 375–380 (2021). https://doi.org/10.1007/s00059-021-05031-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00059-021-05031-4
Keywords
- Aortic valve replacement
- Left ventricular function
- Myocardial strain imaging
- Prosthetic valve
- Strain rate