
Treatment with Oral Ondansetron for Ultramarathon-Associated Nausea: The TOO FUN Study



1
Silver Sage Center for Family Medicine, Reno, NV 89521, USA
2
Department of Family and Community Medicine, Reno School of Medicine, University of Nevada, Reno, NV 89557, USA
3
Reno School of Medicine, University of Nevada, Reno, NV 89557, USA
4
Physical Medicine and Rehabilitation Service, Department of Veterans Affairs, Northern California Health Care System, Sacramento, CA 95655, USA
5
Department of Physical Medicine and Rehabilitation, University of California Davis, Sacramento, CA 95616, USA
*
Author to whom correspondence should be addressed.
Sports 2021, 9(3), 35; https://doi.org/10.3390/sports9030035
Submission received: 24 December 2020
/
Revised: 28 February 2021
/
Accepted: 1 March 2021
/
Published: 3 March 2021
Abstract
:Nausea and vomiting are common for runners during ultramarathons and often contribute to non-finishes. We aimed to determine the efficacy of ondansetron, a commonly used antiemetic, to treat nausea and vomiting in runners during an ultramarathon. Runners who had a previous history of frequent nausea or vomiting during races and entered in 160, 80, and 55 km ultramarathons in 2018 and 2019 were randomized in a double-blind fashion to 4 mg ondansetron or placebo capsules to use if they developed nausea or vomiting during the race with the ability to take three additional doses. Study participants completed a post-race online survey to assess medication use and efficacy. Of 62 study participants, 31 took either ondansetron (20) or placebo (11). In this small study, there were no group differences in those reporting any improvement in nausea and vomiting (p = 0.26) or in the amount of improvement (p = 0.15). We found no evidence that ondansetron capsules improve nausea and vomiting during ultramarathons.
1. Introduction
Athletes running in ultramarathon events commonly have upper gastrointestinal (GI) distress, with nausea present in up to 60% [1]. Nausea or vomiting is the primary reason for not finishing a 161-km ultramarathon, and even among those completing the race, over a third reported, it impacted their race performance [2].
During exercise, GI distress has a wide range of etiologies, including dehydration, heat stress, catecholamine secretion, use of non-steroidal anti-inflammatories, altitude exposure, hyponatremia, competition anxiety, and the amount and content of food and beverage consumed [3,4,5]. In one study of runners during an ultramarathon [6], those who ingested a higher percentage of calories from fat and drank more fluids had less nausea and vomiting, perhaps due in part to improving the distribution of blood flow to the GI tract [7].
Treating upper GI distress in runners during an ultramarathon is challenging. Ondansetron, commonly used to treat nausea and vomiting, is a serotonin 5-HT3 receptor antagonist. It is used in various settings such as chemotherapy, gastroenteritis, and postoperative nausea and vomiting [8,9]. Anecdotally, ondansetron may help exercise-related nausea and vomiting; however, there has been no randomized control trial to support this claim [10]. In a small unblinded pilot study at the Tahoe Rim Trail Endurance Races (TRTER), 66% of 21 runners felt their symptoms improved after taking a 4 mg orally dissolvable ondansetron tablet sublingually [11]. One of the concerns about using ondansetron in ultramarathons is a theoretical risk of it contributing to heat-related illnesses. Ondansetron, however, has not been shown to affect thermoregulation in hot settings [12].
As the etiology of nausea and vomiting in endurance athletes may differ from nausea and vomiting in other settings, we felt that the pilot study’s findings warranted further exploration. We have been unable to find other studies examining the effectiveness of ondansetron in this setting. Thus, the purpose of this double-blind, randomized control trial was to evaluate the effectiveness of ondansetron at treating ultramarathon-associated nausea or vomiting.
2. Materials and Methods
Pre-race recruitment and randomization: We recruited runners from the 2018 and 2019 TRTER. The TRTER has over 600 runners competing in 55, 80, and 160 km races, with approximately 200 runners in each event. Pre-race emails, sent to all competitors, invited them to consider enrolling in the study if they had nausea or vomiting during previous races. Before enrollment, we screened study participants for previous reactions to ondansetron or medications that could interact with ondansetron. Weather conditions, aid station food choices, and sports drinks supplied at the race were similar between years.
Study participants were randomized using a random number generator to either ondansetron 4 mg oral capsules or placebo (cellulose capsule) [13]. A local compounding pharmacy prepared the capsules. Each runner was given four capsules to carry with them during the race with instructions to take one capsule if they developed symptoms. They could then take an additional capsule every 4 h as needed based on recommended dosing. A total of 62 runners elected to participate in the study. Of these, the average age was 45 years old (range 21–78). With respect to gender, 25 were women, and 37 were men.
Race day logistics: Runners encounter medical staff two, four, and nine times in the 55, 80, and 160 km races, respectively. The medical staff were blinded to group allocation, but if a study participant presented with persistent GI symptoms after taking a study capsule, the medical staff could break the blinding to allow for additional treatment options. We asked the runners to record their distance and the time of day or elapsed race time when taking capsules.
Post-Race evaluation: Within 24 h of the race finish, emails were sent to study participants with a link to an online post-race survey, with follow up emails at three and seven days if needed The post-race survey involved 26 questions (available as Supplementary Materials). Included were questions inquiring about previous experiences with nausea and vomiting and their racing history. Runners were asked if they felt the treatment helped (Yes/No/Not sure). They were also asked about the severity of symptoms and improvement of symptoms after treatment on a 1 to 100-point scale. For medication effectiveness, 1 = no help at all and 100 = complete resolution of symptoms. For symptom severity, 1 = very mild symptoms and 100 = severe symptoms. They were also asked to rate the severity of their nausea and vomiting on the same scale before taking the medication, one hour after taking the medication, and at the end of the race.
Assuming a placebo effect of 30% and a 30% greater effect of ondansetron (60% effectiveness) as clinically significant, we would have needed 28 runners in each group to show a statistical effect. We chose 60% effectiveness of ondansetron based on the amount of improvement seen in our pilot study [11].
Group comparisons of ordinal data were made with two-tailed unpaired t-tests or the Mann–Whitney test when data were found to be skewed by the D’Agostino and Pearson omnibus normality test. Group comparisons of categorical data were made with the Fisher’s exact test.
3. Results
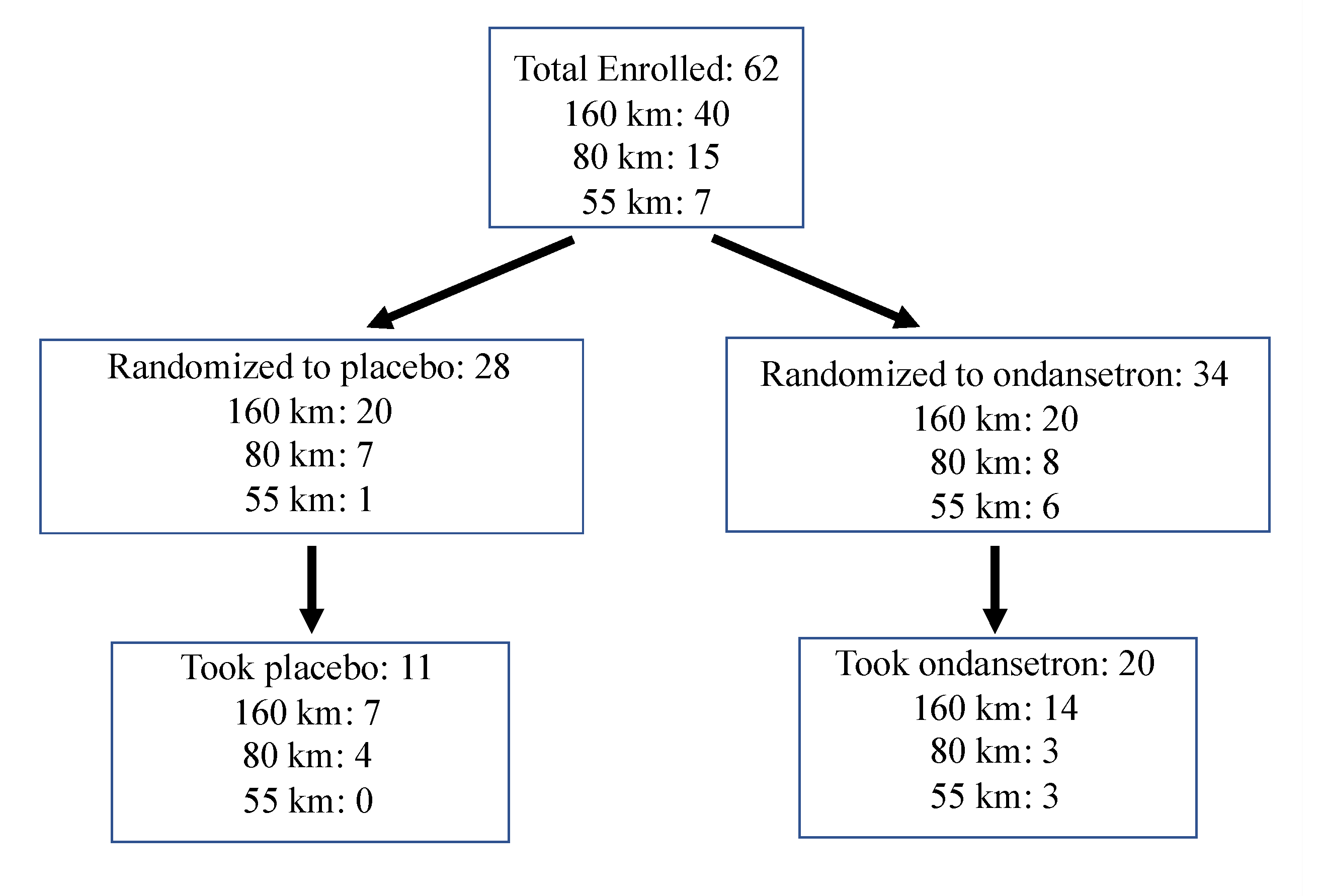
All 62 runners completed the post-race survey within seven days, and 36 completed it within three days of the race finish. Of the runners who enrolled in the study, 31 (50%) had GI symptoms prompting them to take the treatment. Of those 31 runners, 20 were in the ondansetron arm, and 11 were in the placebo arm. Details on the number of study participants and race distances are in Figure 1
As shown in Table 1, the two groups were comparable in individual and during race characteristics, including the proportion that were unblinded during the race. Those taking ondansetron received no benefit compared with placebo. While not reaching significance, there were trends towards the placebo group having more improvement and more side effects than the ondansetron group. On average, 160 km runners took the treatment during the second quartile of the race by distance when ambient temperatures were highest. Weather both years was relatively mild and relatively similar; in 2018, temperatures ranged from 12 to 25 °C, and in 2019, temperatures ranged from 10 to 23 °C near the start/finish line.
4. Discussion
Ondansetron did not improve participants’ symptoms of nausea and vomiting during an ultramarathon. Although it did not reach statistical significance, the placebo group tended to have more benefit and more side effects than the ondansetron group, suggesting that a larger subject group was unlikely to demonstrate a benefit of ondansetron. The side effects due to ondansetron were low, and there was no pattern for particular side effects.
The trend of the placebo group towards having greater benefit and more side effects is likely a reflection of low statistical power. However, it is interesting to see such a high placebo effect. Placebos have been shown to have an equal benefit to active medications, and up to 26% of people will have side effects from placebos [14]. In studies on postoperative nausea and vomiting, while aromatherapy treatment is not statistically superior to placebo, symptom scores often improve in both groups [15]. Perhaps, given the nature of nausea and vomiting during endurance events, athletes might be even more susceptible to a similar placebo/nocebo effect.
Study power was limited, as only 31 (50%) of the study participants had symptoms prompting them to take the treatment. The limited numbers also made the subgroup comparison difficult to interpret. Based on previous studies showing high GI distress rates, we anticipated a higher percentage would try the treatment [1,2,11]. Some subjects may have been concerned about trying a new medication during a race. It may have been beneficial to provide sample ondansetron to study participants to try during training in advance of the study. We report the data before reaching the desired sample size because there was no suggestion of potential benefit from the active treatment.
Another limitation was that we asked runners retrospectively about their nausea and vomiting. We chose this approach as it would have been logistically challenging to capture these data before runners took the medication during the race as the racecourse covers 80 km, and the investigators had limited access to the runners. Except for the few runners who were unblinded during the race, runners were still blinded to their study group when they filled out the survey, which helped reduce response bias.
Our study used ondansetron capsules that require gastric absorption instead of orally dissolvable tablets, which allow for buccal absorption. It is certainly possible that runners given ondansetron were not able to absorb the medication due to vomiting. During exercise, as blood is shunted from the GI tract to muscle, absorption of medications in the stomach may be limited. We made this choice as we were unable to find orally dissolvable placebo tablets that could be packaged to prevent breaking apart during an ultramarathon. In our non-blinded pilot study using orally dissolvable tablets, we saw more improvement in nausea and vomiting; this study does not exclude the possibility of buccally absorbed ondansetron effectiveness. It may have also been beneficial to use an 8 mg dose, which is commonly used in clinical practice, as opposed to a 4 mg dose [13].
In summary, while ondansetron did not show benefit, the study was limited due to the number of runners who chose to take the intervention and perhaps by the form and dose of ondansetron used. Further research on the use of ondansetron should consider these issues in study design.
Supplementary Materials
The following are available online at https://www.mdpi.com/2075-4663/9/3/35/s1, Tahoe Rim Nausea and Vomiting survey.
Author Contributions
Conceptualization, A.V.P., A.I. and D.F.; methodology, A.V.P., A.I., D.F. and M.D.H.; formal analysis, M.D.H.; investigation, A.V.P.; resources, A.V.P.; data curation, A.V.P. and M.D.H.; writing–original draft preparation, A.V.P. and S.T.; writing—review and editing, A.V.P., D.F., A.I., S.T. and M.D.H.; visualization, A.V.P. and M.D.H.; supervision, A.V.P.; project administration, A.V.P.; funding acquisition, A.V.P., A.I. and D.F. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the Ultra Sports Science Foundation Grant Program. This material is the result of work supported with resources and the use of facilities at the VA Northern California Health Care System. The contents reported here do not represent the views of the Department of Veterans Affairs or the United States.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of the University of Nevada, Reno (protocol code 1208535-2. Approved 18 June 2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data from this study are available upon request of the first author.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Stuempfle, K.J.; Hoffman, M.D. Gastrointestinal distress is common during a 161-km ultramarathon. J. Sports Sci. 2015, 414, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.D.; Fogard, K. Factors related to successful completion of a 161-km ultramarathon. Int. J. Sports Physiol. Perform. 2011, 6, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Peters, H.P.F. Potential benefits and hazards of physical activity and exercise on the gastrointestinal tract. Gut 2001, 48, 435–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simrén, M. Physical activity and the gastrointestinal tract. Eur. J. Gastroenterol. Hepatol. 2002, 14, 1053–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, P.B. ‘I think I’m gonna hurl’: A Narrative Review of the Causes of Nausea and Vomiting in Sport. Sports 2019, 7, 162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuempfle, K.J.; Hoffman, M.D.; Hew-Butler, T. Association of gastrointestinal distress in ultramarathoners with race diet. Int. J. Sport Nutr. Exerc. Metab. 2013, 23, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Ter Steege, R.W.F.; Kolkman, J.J. Review article: The pathophysiology and management of gastrointestinal symptoms during physical exercise, and the role of splanchnic blood flow. Aliment. Pharmacol. Ther. 2012, 35, 516–528. [Google Scholar] [CrossRef] [PubMed]
- Canziani, B.C.; Uestuener, P.; Fossali, E.F.; Lava, S.A.; Bianchetti, M.G.; Agostoni, C.; Milani, G.P. Clinical Practice: Nausea and vomiting in acute gastroenteritis: Physiopathology and management. Eur. J. Pediatr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Golembiewski, J.; Chernin, E.; Chopra, T. Prevention and treatment of postoperative nausea. Am. J. Health Pharm. 2005, 62, 1247–1260. [Google Scholar] [CrossRef]
- Hoffman, M.D.; Pasternak, A.; Rogers, I.R.; Khodaee, M.; Hill, J.C.; Townes, D.A.; Scheer, B.V.; Krabak, B.J.; Basset, P.; Lipman, G.S. Medical services at ultra-endurance foot races in remote environments: Medical issues and consensus guidelines. Sports Med. 2014. [Google Scholar] [CrossRef] [PubMed]
- Pasternak, A.V.; Fiore, D.C.; Islas, A.A. Use of Ondansetron for nausea and vomiting during an ultra-endurance run. Int. J. Sports Physiol. Perform. 2018, 13, S1–S6. [Google Scholar]
- McLellan, T.M.; Ducharme, M.B.; Bateman, W.A. Influence of ondansetron on thermoregulation during exercise in the heat wearing combat clothing. Aviat. Space Environ. Med. 1994, 65, 35–40. [Google Scholar]
- Drugs for Vomiting Caused by Cancer Chemotherapy. Med. Lett. 1993, 35, 124–126.
- Colloca, L.; Barsky, A.J. Placebo and nocebo effects. N. Engl. J. Med. 2020, 382, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Hines, S.; Steels, E.; Chang, A.; Gibbons, K. Aromatherapy for treatment of postoperative nausea and vomiting. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Diagram showing number of study participants and race distances from recruitment through intervention.
Figure 1.
Diagram showing number of study participants and race distances from recruitment through intervention.


{kind=link}
Table 1.
Comparison of the two study groups.
| Characteristic or Variable | Ondansetron (n = 20) | Placebo (n = 11) | p-Value |
|---|---|---|---|
| Subject Characteristic | |||
| Age (years) | 48 ± 9 | 46 ± 8 | 0.62 |
| Sex (% men) | 60 | 27 | 0.14 |
| Average weekly running distance (km) a | 80 ± 18 | 72 ±16 | 0.24 |
| Highest weekly running distance (km) b | 112 (96–135) | 120 (86–128) | 0.88 |
| Longest training run or race (km) b | 65 (50–100) | 80 (50–100) | 0.40 |
| Seen physician for GI issues during running (%) | 15 | 36 | 0.21 |
| Frequently have nausea and vomiting during races (%) | 80 | 73 | 0.68 |
| Previously dropped out of ultramarathon (%) | 55 | 27 | 0.26 |
| During Race Characteristic | |||
| Had vomiting during the race (%) | 45 | 18 | 0.24 |
| Distance treatment taken (km) | 60 (42–79) | 51 (32–64) | 0.37 |
| Severity of GI symptoms before treatment (points) c | 60 ± 27 | 60 ± 26 | 0.99 |
| Took own medications during the race (%) | 30 | 9 | 0.37 |
| Received care at an aid station (%) | 35 | 18 | 0.43 |
| Unblinded during the race (%) | 30 | 18 | 0.68 |
| Finished race (%) | 75 | 55 | 0.42 |
| Treatment Outcome Variable | |||
| Reported treatment benefit (%) | 30 | 55 | 0.26 |
| Treatment benefit (points) c | 31 ± 32 | 50 ± 42 | 0.15 |
| Treatment benefit 1-h post-treatment (points) c | 35 (20–78) | 40 (5–90) | 0.90 |
| Severity of GI symptoms at the finish (points) c | 34 ± 32 | 53 ± 43 | 0.21 |
| Reported side effects from treatment (%) | 15 | 36 | 0.21 |
| Thought they took active medications (%) | 63 | 73 | 0.70 |
Ordinal data are reported as mean ± SD or median (interquartile range) if skewed. Categorical data are reported as a percentage. a During the prior year. b During training for this race. c On 100-point scale. Abbreviation: GI, gastrointestinal.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Pasternak, A.V.; Fiore, D.; Islas, A.; Toti, S.; Hoffman, M.D. Treatment with Oral Ondansetron for Ultramarathon-Associated Nausea: The TOO FUN Study. Sports 2021, 9, 35. https://doi.org/10.3390/sports9030035
AMA Style
Pasternak AV, Fiore D, Islas A, Toti S, Hoffman MD. Treatment with Oral Ondansetron for Ultramarathon-Associated Nausea: The TOO FUN Study. Sports. 2021; 9(3):35. https://doi.org/10.3390/sports9030035
Chicago/Turabian StylePasternak, Andrew V., David Fiore, Arthur Islas, Sarah Toti, and Martin D. Hoffman. 2021. "Treatment with Oral Ondansetron for Ultramarathon-Associated Nausea: The TOO FUN Study" Sports 9, no. 3: 35. https://doi.org/10.3390/sports9030035
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.