
Protective Face Masks: Effect on the Oxygenation and Heart Rate Status of Oral Surgeons during Surgery

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
- Duration of the operations was up to 20 min, (n = 25);
- Duration of the operation was between 20–40 min (n = 20);
- Duration of the operations was between 40–120 min (n = 15);
- Duration of the operations was between 120–240 min (n = 4).
Statistical Analysis
3. Results
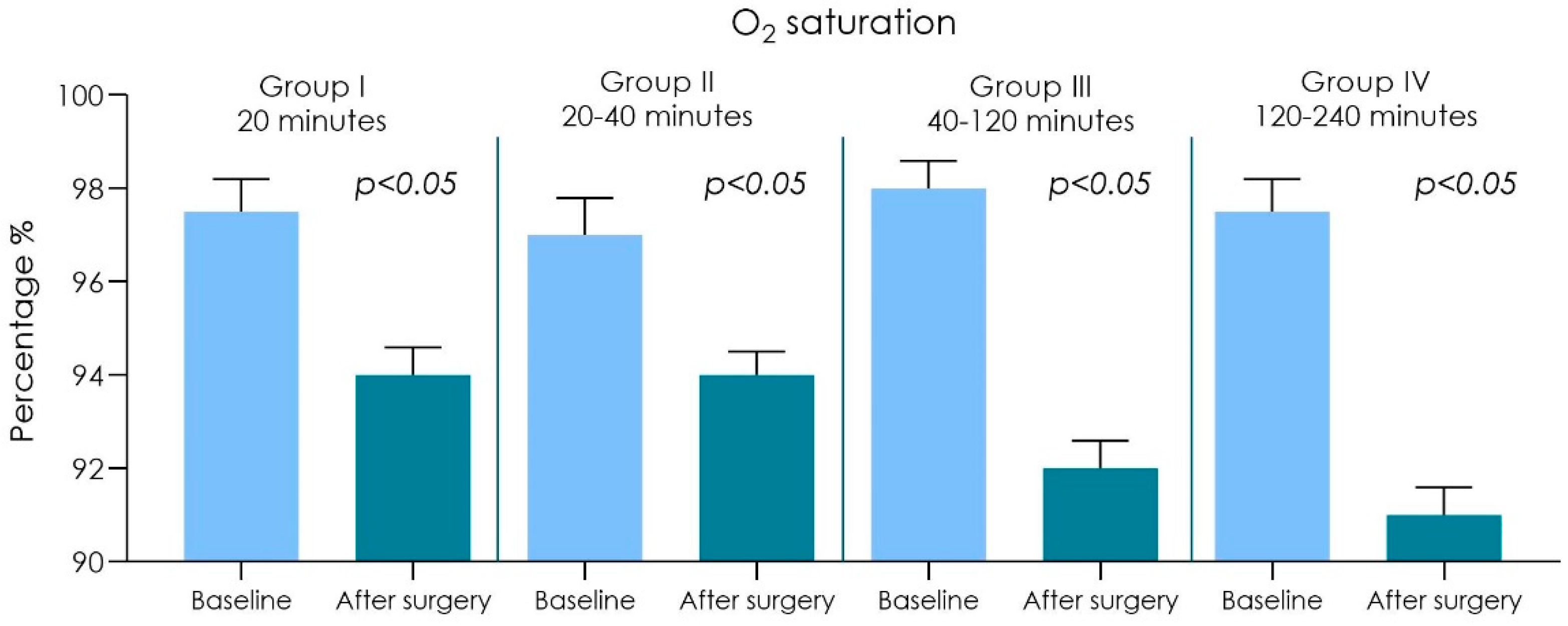
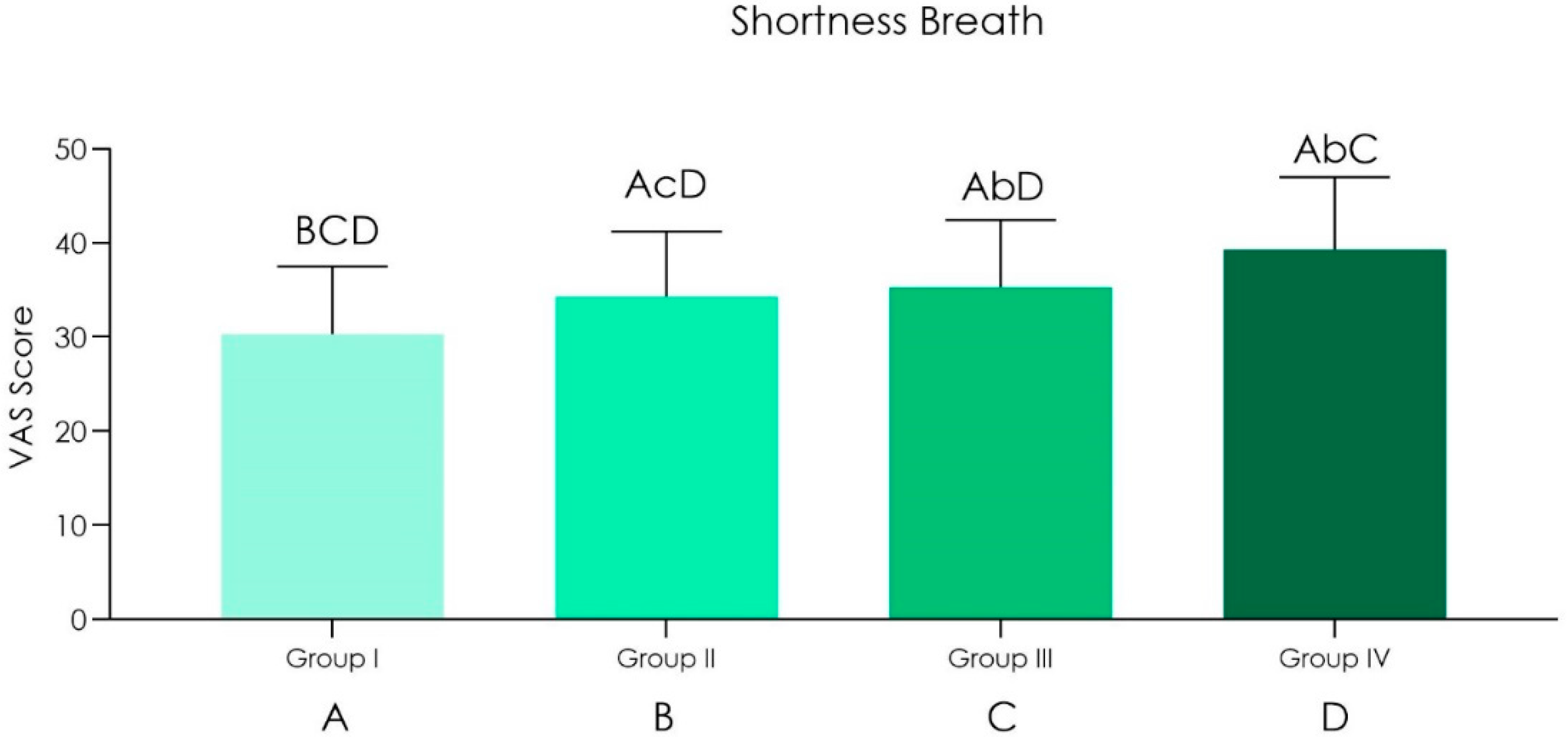
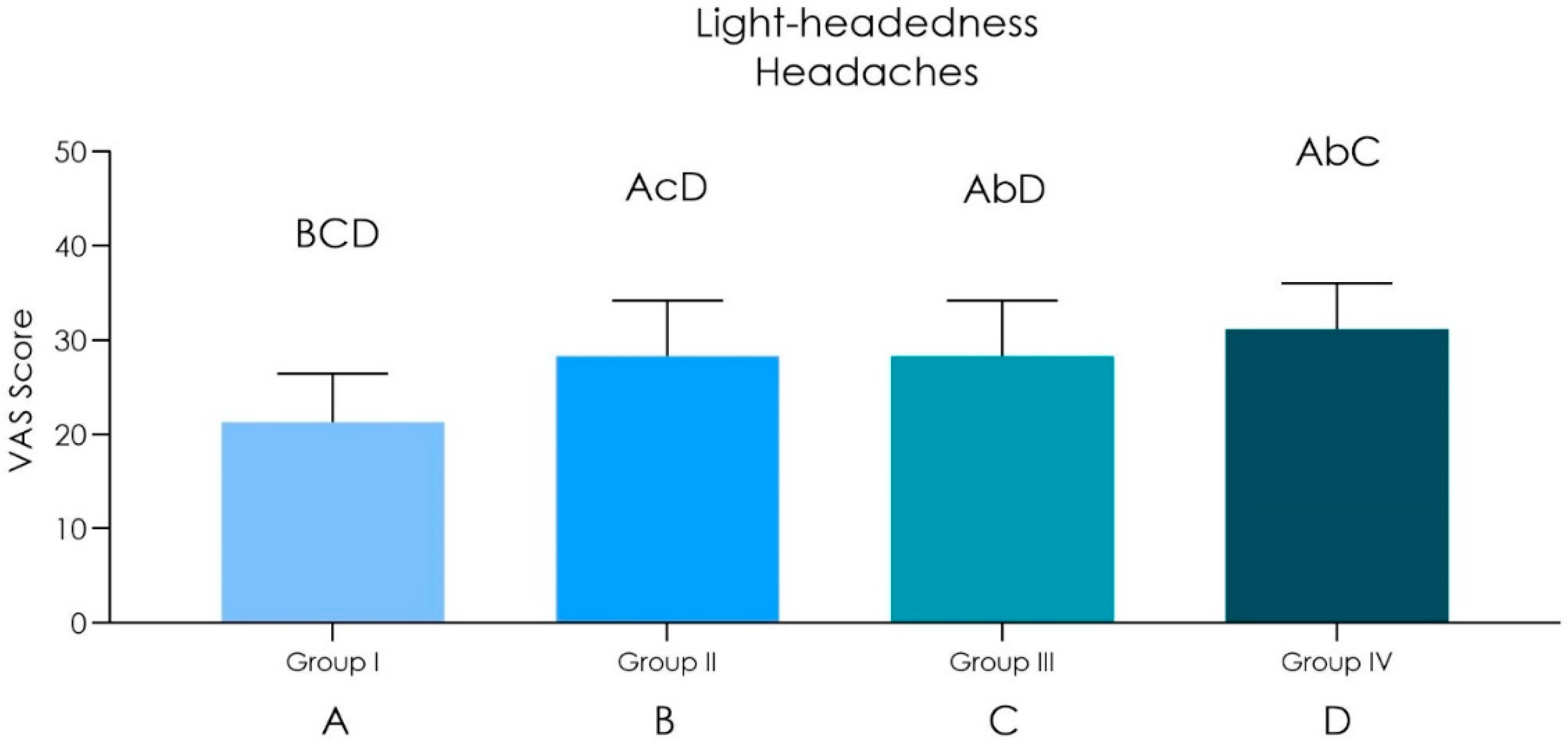
- Duration of the operations was up to 20 min (n = 25): an arterial O2 saturation was recorded from around 97.5% before surgery to 94% after surgery. Heart rate from 60 ± 9 bpm before surgery to 83 ± 12 bpm after surgery was also noted. Shortness of breath scored 30.33 ± 7.17 while light-headedness and headaches scored 21.33 ± 5.85.
- Duration of the operations was in between 20–40 min (n = 20): an arterial O2 saturation was recorded from around 97% before surgery to 94% after surgery. Heart rate from 61 ± 7 bpm before surgery to 85 ± 11 bpm after surgery was also noted. Shortness of breath scored 34.33 ± 6.91 while light-headedness and headaches scored 24.33 ± 5.11.
- Duration of the operations was in between 40–120 min (n = 15): an arterial O2 saturation was recorded from around 98% before surgery to 92% after surgery. Heart rate from 61 ± 8 bpm before surgery to 95 ± 10 bpm after surgery was also noted. Shortness of breath scored 35.33 ± 7.17 while light-headedness and headaches scored 28.33 ± 5.87.
- Duration of the operations was in between 120–240 min (n = 4): an arterial O2 saturation was recorded from around 97.5% before surgery to 91% after surgery. Heart rate from 60 ± 7 bpm before surgery to 98 ± 12 bpm after surgery was also noted. Shortness of breath scored 39.33 ± 7.64 while light-headedness and headaches scored 31.18 ± 4.85.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Rational Use of Personal Protective Equipment for Coronavirus Disease (COVID-19) and Considerations during Severe Shortages: Interim Guidance, 6 April 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Li, Y.; Tokura, H.; Guo, Y.P.; Wong, A.S.W.; Wong, T.; Chung, J.; Newton, E. Effects of Wearing N95 and Surgical Facemasks on Heart Rate, Thermal Stress and Subjective Sensations. Int. Arch. Occup. Environ. Health 2005, 78, 501–509. [Google Scholar] [CrossRef]
- Romney, M.G. Surgical Face Masks in the Operating Theatre: Re-Examining the Evidence. J. Hosp. Infect. 2001, 47, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Chen, J. Pathogenicity and Transmissibility of 2019-NCoV-A Quick Overview and Comparison with Other Emerging Viruses. Microbes Infect. 2020, 22, 69–71. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Bordea, I.R.; Xhajanka, E.; Candrea, S.; Bran, S.; Onișor, F.; Inchingolo, A.D.; Malcangi, G.; Pham, V.H.; Inchingolo, A.M.; Scarano, A.; et al. Coronavirus (SARS-CoV-2) Pandemic: Future Challenges for Dental Practitioners. Microorganisms 2020, 8, 1704. [Google Scholar] [CrossRef] [PubMed]
- Bellocchio, L.; Bordea, I.R.; Ballini, A.; Lorusso, F.; Hazballa, D.; Isacco, C.G.; Malcangi, G.; Inchingolo, A.D.; Dipalma, G.; Inchingolo, F.; et al. Environmental Issues and Neurological Manifestations Associated with COVID-19 Pandemic: New Aspects of the Disease? Int. J. Environ. Res. Public Health 2020, 17, 8049. [Google Scholar] [CrossRef]
- Lorusso, F.; Inchingolo, F.; Scarano, A. The impact of Covid-19 on the scientific production spread: A five-MONTH bibliometric report of the worldwide research community. Acta Med. Mediterr. 2020, 36, 3357–3360. [Google Scholar]
- Lee, V.J.; Aguilera, X.; Heymann, D.; Wilder-Smith, A. Lancet Infectious Diseases Commission Preparedness for Emerging Epidemic Threats: A Lancet Infectious Diseases Commission. Lancet Infect. Dis. 2020, 20, 17–19. [Google Scholar] [CrossRef] [Green Version]
- Critical care committee of Chinese Association of Chest Physician. Conventional Respiratory Support Therapy for Severe Acute Respiratory Infections (SARI): Clinical Indications and Nosocomial Infection Prevention and Control. Zhonghua Jie He He Hu Xi Za Zhi 2020, 43, 189–194. [Google Scholar]
- Kohanski, M.A.; Palmer, J.N.; Cohen, N.A. Aerosol or Droplet: Critical Definitions in the COVID-19 Era. Int. Forum Allergy Rhinol. 2020. [Google Scholar] [CrossRef]
- Xie, X.; Li, Y.; Sun, H.; Liu, L. Exhaled Droplets Due to Talking and Coughing. J. R. Soc. Interface 2009, 6 (Suppl. 6), S703–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacIntyre, C.R.; Chughtai, A.A.; Rahman, B.; Peng, Y.; Zhang, Y.; Seale, H.; Wang, X.; Wang, Q. The Efficacy of Medical Masks and Respirators against Respiratory Infection in Healthcare Workers. Influenza Other Respir. Viruses 2017, 11, 511–517. [Google Scholar] [CrossRef]
- Bourouiba, L. Turbulent Gas Clouds and Respiratory Pathogen Emissions: Potential Implications for Reducing Transmission of COVID-19. JAMA 2020, 323, 1837–1838. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Inchingolo, F.; Lorusso, F. Facial Skin Temperature and Discomfort When Wearing Protective Face Masks: Thermal Infrared Imaging Evaluation and Hands Moving the Mask. Int. J. Environ. Res. Public Health 2020, 17, 4624. [Google Scholar] [CrossRef] [PubMed]
- Radonovich, L.J.; Simberkoff, M.S.; Bessesen, M.T.; Brown, A.C.; Cummings, D.A.T.; Gaydos, C.A.; Los, J.G.; Krosche, A.E.; Gibert, C.L.; Gorse, G.J.; et al. N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial. JAMA 2019, 322, 824–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarano, A.; Carinci, F.; Lorusso, F.; Festa, F.; Bevilacqua, L.; Santos de Oliveira, P.; Maglione, M. Ultrasonic vs Drill Implant Site Preparation: Post-Operative Pain Measurement Through VAS, Swelling and Crestal Bone Remodeling: A Randomized Clinical Study. Materials 2018, 11, 2516. [Google Scholar] [CrossRef] [Green Version]
- Piattelli, A.; Piattelli, M.; Scarano, A. Simultaneous Demonstration of Alkaline and Acid Phosphatase Activity in Bone, at Bone-Implant Interfaces and at the Epiphyseal Growth Plate in Plastic-Embedded Undemineralized Tissues. Biomaterials 1997, 18, 545–549. [Google Scholar] [CrossRef]
- ADA Develops Guidance on Dental Emergency, Nonemergency Care. Available online: Https://Www.Ada.Org/En/Publications/Ada-News/2020-Archive/March/Ada-Develops-Guidance-on-Dental-Emergency-Nonemergency-Care (accessed on 29 June 2020).
- Eggers, M.; Koburger-Janssen, T.; Eickmann, M.; Zorn, J. In Vitro Bactericidal and Virucidal Efficacy of Povidone-Iodine Gargle/Mouthwash against Respiratory and Oral Tract Pathogens. Infect. Dis. Ther. 2018, 7, 249–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission Routes of 2019-NCoV and Controls in Dental Practice. Int. J. Oral Sci. 2020, 12, 9. [Google Scholar] [CrossRef]
- Scarano, A.; Inchingolo, F.; Lorusso, F. Environmental Disinfection of a Dental Clinic during the Covid-19 Pandemic: A Narrative Insight. Biomed. Res. Int. 2020, 2020, 8896812. [Google Scholar] [CrossRef]
- Dominiak, M.; Rózyło-Kalinowska IGedrange, T.; Konopka, T.; Hadzik, J.; Bednarz, W.; Matys Jacek Lella, A.; Rayad, S.; Maksymowicz, R.; Kuźniarski, A. COVID-19 and Professional Dental Practice. The Polish Dental Association Working Group Recommendations for Procedures in Dental Office during an Increased Epidemiological Risk. J. Stomatol. 2020, 73, 1–10. [Google Scholar] [CrossRef]
- Weber, W.M.; Elfadel, I.M.; Barker, S.J. Low Perfusion-Resistant Pulse Oximetry. J. Clin. Monit. 1995, 11, 284. [Google Scholar]
- Place, B. Pulse Oximetry in Adults. Nurs. Times 1998, 94, 48. [Google Scholar] [PubMed]
- Jubran, A.; Tobin, M.J. Monitoring during Mechanical Ventilation. Clin. Chest Med. 1996, 17, 453–473. [Google Scholar] [CrossRef]
- Pretto, J.J.; Roebuck, T.; Beckert, L.; Hamilton, G. Clinical Use of Pulse Oximetry: Official Guidelines from the T Horacic S Ociety of A Ustralia and N Ew Z Ealand. Respirology 2014, 19, 38–46. [Google Scholar] [CrossRef]
- Chan, E.D.; Chan, M.M.; Chan, M.M. Pulse Oximetry: Understanding Its Basic Principles Facilitates Appreciation of Its Limitations. Respir. Med. 2013, 107, 789–799. [Google Scholar] [CrossRef] [Green Version]
- Mayers, J.R. Patient Monitors. In Clinical Anesthesiology; Morgan, E.G., Mikhail, M.S., Murray, M.J., Larson, C.P., Eds.; McGraw Hill: New York, NY, USA, 2006. [Google Scholar]
- Rebmann, T.; Carrico, R.; Wang, J. Physiologic and Other Effects and Compliance with Long-Term Respirator Use among Medical Intensive Care Unit Nurses. Am. J. Infect. Control 2013, 41, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.J.Y.; Bharatendu, C.; Goh, Y.; Tang, J.Z.Y.; Sooi, K.W.X.; Tan, Y.L.; Tan, B.Y.Q.; Teoh, H.-L.; Ong, S.T.; Allen, D.M.; et al. Headaches Associated With Personal Protective Equipment—A Cross-Sectional Study Among Frontline Healthcare Workers During COVID-19. Headache 2020, 60, 864–877. [Google Scholar] [CrossRef] [Green Version]
- Lim, E.C.H.; Seet, R.C.S.; Lee, K.-H.; Wilder-Smith, E.P.V.; Chuah, B.Y.S.; Ong, B.K.C. Headaches and the N95 Face-Mask amongst Healthcare Providers. Acta Neurol. Scand. 2006, 113, 199–202. [Google Scholar] [CrossRef]
- Hu, K.; Fan, J.; Li, X.; Gou, X.; Li, X.; Zhou, X. The Adverse Skin Reactions of Health Care Workers Using Personal Protective Equipment for COVID-19. Medicine 2020, 99, e20603. [Google Scholar] [CrossRef]
- Tan, K.T.; Greaves, M.W. N95 Acne. Int. J. Dermatol. 2004, 43, 522–523. [Google Scholar] [CrossRef]
- Al Badri, F.M. Surgical Mask Contact Dermatitis and Epidemiology of Contact Dermatitis in Healthcare Workers: Allergies in the Workplace. Curr. Allergy Clin. Immunol. 2017, 30, 183–188. [Google Scholar]
- Ganong, W.F. Review of Medical Physiology; Mcgraw-hill: New York, NY, USA, 1995. [Google Scholar]
- What People with Asthma Need to Know about Face Masks and Coverings during the COVID-19 Pandemic. Available online: Https://Community.Aafa.Org/Blog/What-People-with-Asthma-Need-to-Know-about-Facemasks-and-Coverings-during-the-Covid-19-Pandemic (accessed on 12 February 2021).
- Gronda, E.; Brambilla, G.; Seravalle, G.; Maloberti, A.; Cairo, M.; Costantino, G.; Lovett, E.; Vanoli, E.; Mancia, G.; Grassi, G. Effects of Chronic Carotid Baroreceptor Activation on Arterial Stiffness in Severe Heart Failure. Clin. Res. Cardiol. 2016, 105, 838–846. [Google Scholar] [CrossRef]
- Rosenblueth, A.; Freeman, N. The Reciprocal Innervation in Reflex Changes of Heart Rate. Am. J. Physiol. 1931, 98, 430–435. [Google Scholar] [CrossRef] [Green Version]
- Wustmann, K.; Kucera, J.P.; Scheffers, I.; Mohaupt, M.; Kroon, A.A.; de Leeuw, P.W.; Schmidli, J.; Allemann, Y.; Delacrétaz, E. Effects of Chronic Baroreceptor Stimulation on the Autonomic Cardiovascular Regulation in Patients with Drug-Resistant Arterial Hypertension. Hypertension 2009, 54, 530–536. [Google Scholar] [CrossRef] [Green Version]
- Seravalle, G.; Dell’Oro, R.; Grassi, G. Baroreflex Activation Therapy Systems: Current Status and Future Prospects. Expert Rev. Med Devices 2019, 16, 1025–1033. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Tu, X.; Zhou, X.; Yu, J.; Luo, S.; Ma, L.; Liu, C.; Zhao, Y.; Jin, X. Wearing a N95 Mask Increases Rescuer’s Fatigue and Decreases Chest Compression Quality in Simulated Cardiopulmonary Resuscitation. Am. J. Emerg. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.P.; Wang, D.Y. Objective Assessment of Increase in Breathing Resistance of N95 Respirators on Human Subjects. Ann. Occup. Hyg. 2011, 55, 917–921. [Google Scholar] [CrossRef] [Green Version]
- Fikenzer, S.; Uhe, T.; Lavall, D.; Rudolph, U.; Falz, R.; Busse, M.; Hepp, P.; Laufs, U. Effects of Surgical and FFP2/N95 Face Masks on Cardiopulmonary Exercise Capacity. Clin. Res. Cardiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Melissant, C.F.; Lammers, J.W.; Demedts, M. Relationship between External Resistances, Lung Function Changes and Maximal Exercise Capacity. Eur. Respir. J. 1998, 11, 1369–1375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaw, K.; Butcher, S.; Ko, J.; Zello, G.A.; Chilibeck, P.D. Wearing of Cloth or Disposable Surgical Face Masks Has No Effect on Vigorous Exercise Performance in Healthy Individuals. Int. J. Environ. Res. Public Health 2020, 17, 8110. [Google Scholar] [CrossRef] [PubMed]
- Kyung, S.Y.; Kim, Y.; Hwang, H.; Park, J.-W.; Jeong, S.H. Risks of N95 Face Mask Use in Subjects With COPD. Respir. Care 2020, 65, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Convertino, V.A.; Cooke, W.H.; Lurie, K.G. Inspiratory Resistance as a Potential Treatment for Orthostatic Intolerance and Hemorrhagic Shock. Aviat. Space Environ. Med. 2005, 76, 319–325. [Google Scholar] [PubMed]
- Ryan, K.L.; Cooke, W.H.; Rickards, C.A.; Lurie, K.G.; Convertino, V.A. Breathing through an Inspiratory Threshold Device Improves Stroke Volume during Central Hypovolemia in Humans. J. Appl. Physiol. 2008, 104, 1402–1409. [Google Scholar] [CrossRef] [PubMed]
- Cheyne, W.S.; Harper, M.I.; Gelinas, J.C.; Sasso, J.P.; Eves, N.D. Mechanical Cardiopulmonary Interactions during Exercise in Health and Disease. J. Appl. Physiol. 2020, 128, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- White, M.K.; Hodous, T.K.; Vercruyssen, M. Effects of Thermal Environment and Chemical Protective Clothing on Work Tolerance, Physiological Responses, and Subjective Ratings. Ergonomics 1991, 34, 445–457. [Google Scholar] [CrossRef]
- Fletcher, S.J.; Clark, M.; Stanley, P.J. Carbon Dioxide Re-Breathing with Close Fitting Face Respirator Masks. Anaesthesia 2006, 61, 910. [Google Scholar] [CrossRef]
- Germonpre, P.; Van Rompaey, D.; Balestra, C. Evaluation of Protection Level, Respiratory Safety, and Practical Aspects of Commercially Available Snorkel Masks as Personal Protection Devices Against Aerosolized Contaminants and SARS-CoV2. Int. J. Environ. Res. Public Health 2020, 17, 4347. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group I 20 min | Group II 20–40 min | Group III 40–120 min | Group IV 120–240 min | |||||
|---|---|---|---|---|---|---|---|---|
| Baseline | After Surgery | Baseline | After Surgery | Baseline | After Surgery | Baseline | After Surgery | |
| O2 saturation | 97.5% ± 0.7 | 94% ± 0.6 | 97.0% ± 0.8 | 94% ± 0.5 | 98.0% ± 0.6 | 92% ± 0.5 | 97.5% ± 0.7 | 91% ± 0.6 |
| p value | p < 0.05 | p < 0.05 | p < 0.01 | p < 0.01 | ||||
| Heart rate | 60 ± 9 bpm | 83 ± 12 bpm | 61 ± 7 bpm | 85 ± 11 bpm | 61 ± 8 bpm | 95 ± 10 bpm | 60 ± 7 bpm | 98 ± 12 bpm |
| p value | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.01 | ||||
| VAS SCORE | Group I 20 min | Group II 20–40 min | Group III 40–120 min | Group IV 120–240 min |
|---|---|---|---|---|
| Short Breathness | 30.33 ± 7.17 | 34.33 ± 6.91 | 35.33 ± 7.09 | 39.33 ± 7.64 |
| Light-headedness- Headaches | 21.33 ± 5.85 | 24.33 ± 5.11 | 28.33 ± 5.87 | 31.18 ± 4.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scarano, A.; Inchingolo, F.; Rapone, B.; Festa, F.; Rexhep Tari, S.; Lorusso, F. Protective Face Masks: Effect on the Oxygenation and Heart Rate Status of Oral Surgeons during Surgery. Int. J. Environ. Res. Public Health 2021, 18, 2363. https://doi.org/10.3390/ijerph18052363
Scarano A, Inchingolo F, Rapone B, Festa F, Rexhep Tari S, Lorusso F. Protective Face Masks: Effect on the Oxygenation and Heart Rate Status of Oral Surgeons during Surgery. International Journal of Environmental Research and Public Health. 2021; 18(5):2363. https://doi.org/10.3390/ijerph18052363
Chicago/Turabian StyleScarano, Antonio, Francesco Inchingolo, Biagio Rapone, Felice Festa, Sergio Rexhep Tari, and Felice Lorusso. 2021. "Protective Face Masks: Effect on the Oxygenation and Heart Rate Status of Oral Surgeons during Surgery" International Journal of Environmental Research and Public Health 18, no. 5: 2363. https://doi.org/10.3390/ijerph18052363