The Motivation Journey: A Grounded Theory Study on Female Cancer Survivors’ Experience of a Psychological Intervention for Quality of Life

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Participants
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Participants
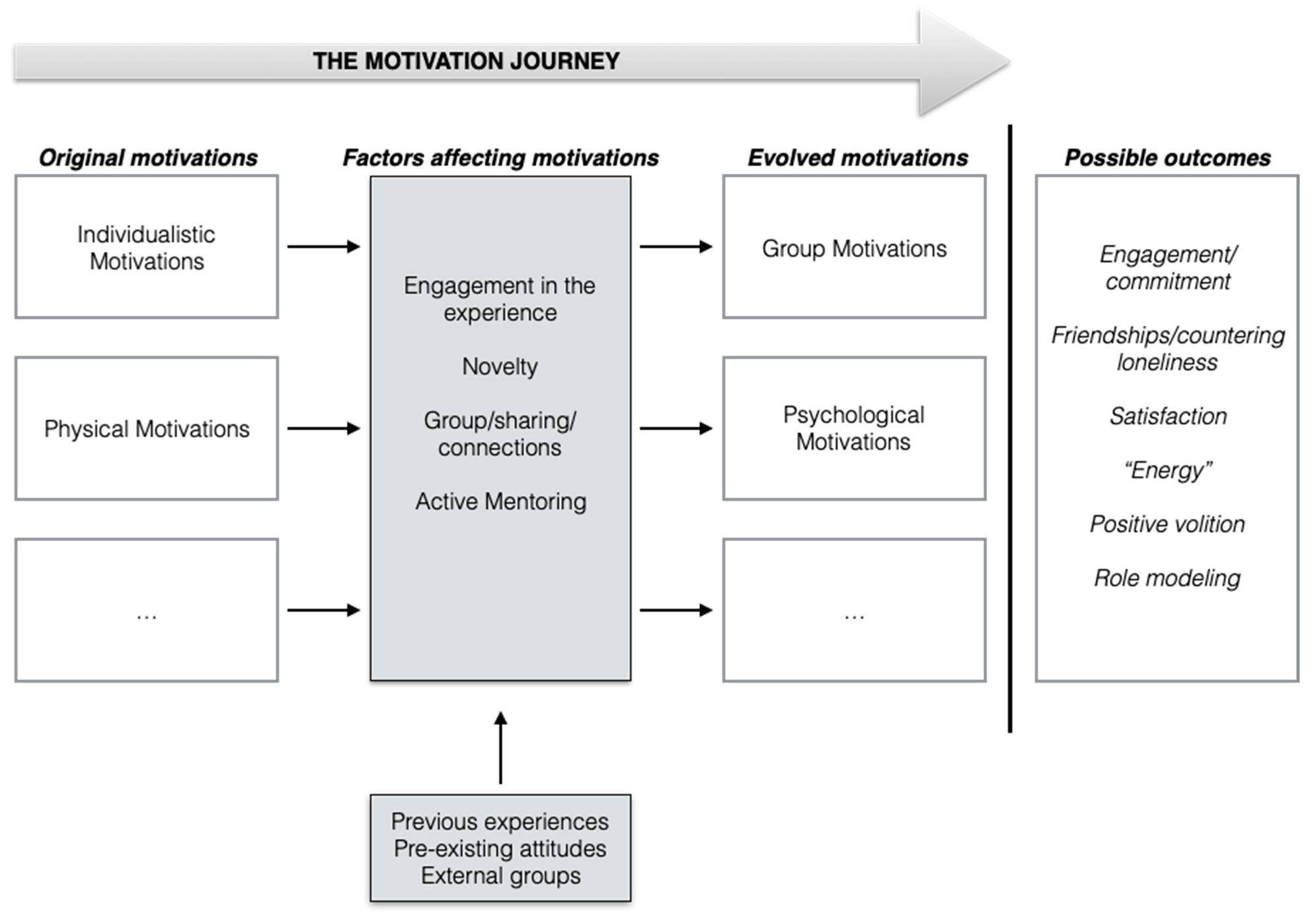
3.2. The Motivation Journey
3.2.1. From Individualistic to Group-Related Motivations
“I decided to join the intervention also to make sense of what had happened to me because I don’t know if I can accept the diagnosis of cancer. Surely, I learned to live with what happened to me, but I also needed to give a sense to my disease (cancer) and therefore participate in this intervention. However, (it was meant to be) also a rebirth for me; because initially it is not so simple to explain ... but there is a need to be reborn, to get cancer out of the shadows” (ID #1).
“I had the hope that this project would extend because it had given me an element of hope also in recovering in my normal active life; I saw it as a stage to aim for, a goal to aim for” (ID #11).
“For me, it is a new challenge. It is a challenge because it is a desire to achieve my personal results (...) it is not that I aspire to who knows what ... but (my personal objectives) are important to me, even just running half an hour just like I did the other day was a great satisfaction ... I feel that I would never have being able to do something like this a few years ago” (ID #8).
“By becoming a Pink Ambassador I “come out” as a cancer survivor. After that, many people told me: “But I didn’t know (about your cancer)!” “How did you do it? Your face was always the same!”. Yes ... but it was a mask! ... and I was hiding something different. And it was nice and right because at some point (of your life) that mask has to fall down! I had been wearing it for too long. It was probably not a very conscious choice, but it was what I needed to get myself out of the situation. I thought it had to be done for me and my little daughter” (ID #7).
“I insist a lot on this aspect: for me ... the element that I have emphasized several times ... for me the team has become a really important aspect, the experience of the group … because even in moments of heated conflict, (the team) is an element of strength” (ID #11).
“This new group ... this feeling of being part of a group ... we feel considered in this project... (it is important) to present ourselves to others with a certain energy”(ID #8).
“to make others understand that “the head matters” (the psychological aspects are important) a lot so as to believe in a possibility of normal life is a very important goal for me. (I would like to) be a spokesperson for life after cancer ... like, if you do not abandon yourself to the fatality of the tumor there is an “after”: it is not like after the disease you are a porcelain doll, like, oh my God I can’t do this I can’t do that!” (ID #9).
“I could have been an example of how to deal with this thing even alone, while understanding that we are not alone; because now that I am “exposed”(I shared my experience) I am no longer alone, I am no longer alone because I have a group ... I am no longer alone because people know it ... I am no longer alone because I do not … anymore” (ID #7).
3.2.2. From Physical to Psychological Growth
“Above all, I need to tone my abdomen to do a future reconstruction surgery and the running and training they make us do will help me in this” (ID #5).
“Not necessarily to take this path of sport in my opinion, but in understanding that you can do things anyway and there are more resources that this path is giving me, resources that maybe someone can take as an example and make them their own and be motivated to also deal with the disease differently” (ID #7).
“Become aware of my body...”... “see that my body responds and that in reality I can do what I thought I could not do...” (ID #12).
“I thought if this could be the connection that maybe makes me come back to live, to smile sincerely, not to have the mask I had put on. Because I never wanted to show others what I had inside. I always tried to have this mask, and I wanted to take it off, I wanted to be myself, joking, that never stops“ (ID #6).
“Very nice for me it was the moment when I came out, declaring myself a cancer patient. How many people came to tell me they didn’t know, because my face was always the same ... yes, but it was a mask! Because that face wasn’t there behind it. And it was beautiful and right, because at a certain point that mask had to collapse, it was too long that I had worn it on me, and it was important, it was what I had needed to get me out of the situation” (ID #7).
“Give the opportunity to those who have lived this experience to testify that it can be done and that maybe other people (other women who are in this situation at this moment) by seeing us, they can gain strength, courage, and tell them they did. They were sick as I am sick and they did it “...” pride and pride to be able to be really helpful with my testimony to those who are going through a bad time at this moment“ (ID #12).
“try to sensitize more people to prevention and self-care, and to that healthy selfishness. But it’s nothing more than thinking a little more about oneself in its entirety, there is not only home, work, family, sport, but doing what makes you feel good. This is a lesson that I learned from the disease, from this experience, because I could have been gone“ (ID #4)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lebel, S.; Ozakinci, G.; Humphris, G.; Mutsaers, B.; Thewes, B.; Prins, J.; Dinkel, A.; Butow, P. From Normal Response to Clinical Problem: Definition and Clinical Features of Fear of Cancer Recurrence. Support. Care Cancer 2016, 24, 3265–3268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bower, J.E.; Ganz, P.A.; Desmond, K.A.; Rowland, J.H.; Meyerowitz, B.E.; Belin, T.R. Fatigue in Breast Cancer Survivors: Occurrence, Correlates, and Impact on Quality of Life. J. Clin. Oncol. 2000, 18, 743. [Google Scholar] [CrossRef] [PubMed]
- Wanchai, A.; Armer, J.M. A Systematic Review Association of Reflexology in Managing Symptoms and Side Effects of Breast Cancer Treatment: Reflexology & Breast Cancer. Complement. Ther. Clin. Pract. 2020, 38, 101074. [Google Scholar] [PubMed]
- Parker, J.J.; Rademaker, A.; Donnelly, E.D.; Choi, J.N. Risk Factors for the Development of Acute Radiation Dermatitis in Breast Cancer Patients. Int. J. Radiat. Oncol. 2017, 99, E40–E41. [Google Scholar] [CrossRef]
- Triberti, S.; Savioni, L.; Sebri, V.; Pravettoni, G. EHealth for Improving Quality of Life in Breast Cancer Patients: A Systematic Review. Cancer Treat. Rev. 2019, 74, 1–14. [Google Scholar] [CrossRef]
- Watanabe, T.; Yagata, H.; Saito, M.; Okada, H.; Yajima, T.; Tamai, N.; Yoshida, Y.; Takayama, T.; Imai, H.; Nozawa, K.; et al. A Multicenter Survey of Temporal Changes in Chemotherapy-Induced Hair Loss in Breast Cancer Patients. PLoS ONE 2019, 14, e0208118. [Google Scholar] [CrossRef]
- Park, J.H.; Chun, M.; Jung, Y.S.; Bae, S.H. Predictors of Psychological Distress Trajectories in the First Year After a Breast Cancer Diagnosis. Asian Nurs. Res. (Korean. Soc. Nurs. Sci). 2017, 11, 268–275. [Google Scholar] [CrossRef] [Green Version]
- Arnaboldi, P.; Lucchiari, C.; Santoro, L.; Sangalli, C.; Luini, A.; Pravettoni, G. PTSD Symptoms as a Consequence of Breast Cancer Diagnosis: Clinical Implications. Springerplus 2014, 3, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Tighe, M.; Molassiotis, A.; Morris, J.; Richardson, J. Coping, Meaning and Symptom Experience: A Narrative Approach to the Overwhelming Impacts of Breast Cancer in the First Year Following Diagnosis. Eur. J. Oncol. Nurs. 2011, 15, 226–232. [Google Scholar] [CrossRef]
- Renzi, C.; Fioretti, C.; Oliveri, S.; Mazzocco, K.; Zerini, D.; Alessandro, O.; Rojas, D.P.; Jereczek-Fossa, B.A.; Pravettoni, G. A Qualitative Investigation on Patient Empowerment in Prostate Cancer. Front. Psychol. 2017, 8, 1215. [Google Scholar] [CrossRef] [Green Version]
- Rowland, J.H.; Meyerowitz, B.E.; Crespi, C.M.; Leedham, B.; Desmond, K.; Belin, T.R.; Ganz, P.A. Addressing Intimacy and Partner Communication after Breast Cancer: A Randomized Controlled Group Intervention. Breast Cancer Res. Treat. 2009, 118, 99–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fioretti, C.; Mazzocco, K.; Pravettoni, G. Psychological Support in Breast Cancer Patients: A Personalized Approach. In Breast Cancer: Innovations in Research and Management; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Ferrari, F.; Faccio, F.; Peccatori, F.; Pravettoni, G. Psychological Issues and Construction of the Mother-Child Relationship in Women with Cancer during Pregnancy: A Perspective on Current and Future Directions. BMC Psychol. 2018, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- Faccio, F.; Mascheroni, E.; Ionio, C.; Pravettoni, G.; Alessandro Peccatori, F.; Pisoni, C.; Cassani, C.; Zambelli, S.; Zilioli, A.; Nastasi, G.; et al. Motherhood during or after Breast Cancer Diagnosis: A Qualitative Study. Eur. J. Cancer Care 2020, 29, e13214. [Google Scholar] [CrossRef] [PubMed]
- Oliveri, S.; Ongaro, G.; Durosini, I.; Curigliano, G.; Pravettoni, G. Breast Implant-Associated Anaplastic Large Cell Lymphoma: Emotional Impact and Guidelines for Psychological Support. Breast Cancer Res. Treat. 2020, 181, 221–224. [Google Scholar] [CrossRef]
- Gudenkauf, L.M.; Ehlers, S.L. Psychosocial Interventions in Breast Cancer Survivorship Care. Breast 2018, 38, 1–6. [Google Scholar] [CrossRef]
- Han, J.; Liu, J.E.; Su, Y.L.; Qiu, H. Effect of a Group-Based Acceptance and Commitment Therapy (ACT) Intervention on Illness Cognition in Breast Cancer Patients. J. Context. Behav. Sci. 2019, 14, 73–81. [Google Scholar] [CrossRef]
- Aschieri, F.; De Saeger, H.; Durosini, I. Therapeutic Assessment and Collaborative: Empirical Evidence [L’évaluation Thérapeutique et Collaborative: Preuves Empiriques]. Prat. Psychol. 2015, 21, 307–317. [Google Scholar]
- Durosini, I.; Tarocchi, A.; Aschieri, F. Therapeutic Assessment with a Client with Persistent Complex Bereavement Disorder: A Single-Case Time-Series Design. Clin. Case Stud. 2017, 16, 295–312. [Google Scholar] [CrossRef]
- Fawzy, F.I.; Fawzy, N.W.; Arndt, L.A.; Pasnau, R.O. Critical Review of Psychosocial Interventions in Cancer Care. Arch. Gen. Psychiatry 1995, 52, 100–113. [Google Scholar] [CrossRef]
- Sebri, V.; Savioni, L.; Triberti, S.; Durosini, I.; Mazzocco, K.; Pravettoni, G. Do You Transfer Your Skills? From Sports to Health Management in Cancer Patients. Front. Psychol. 2020, 11, 546. [Google Scholar] [CrossRef]
- Barsevick, A.M.; Sweeney, C.; Haney, E.; Chung, E. A Systematic Qualitative Analysis of Psychoeducational Interventions for Depression in Patients with Cancer. In Database of Abstracts of Reviews of Effects (DARE): Quality-Assessed Reviews [Internet]; Centre for Reviews and Dissemination (UK): York, UK, 2002. [Google Scholar]
- Montgomery, C. Role of Dynamic Group Therapy in Psychiatry. Adv. Psychiatr. Treat. 2002, 8, 34–41. [Google Scholar] [CrossRef]
- Spiegel, D.; Bloom, J.R. Group Therapy and Hypnosis Reduce Metastatic Breast Carcinoma Pain. Psychosom. Med. 1983, 45, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.R.; Sobel, D.S.; Ritter, P.L.; Laurent, D.; Hobbs, M. Effect of a Self-Management Program on Patients with Chronic Disease. Eff. Clin. Pract. 2001, 4, 256–262. [Google Scholar] [PubMed]
- Benton, M.J.; Schlairet, M.C.; Gibson, D.R. Change in Quality of Life among Breast Cancer Survivors after Resistance Training: Is There an Effect of Age? J. Aging Phys. Act. 2014, 22, 178–185. [Google Scholar] [CrossRef]
- Bail, J.R.; Ivankova, N.; Heaton, K.; Vance, D.E.; Triebel, K.; Meneses, K. Cancer-Related Symptoms and Cognitive Intervention Adherence among Breast Cancer Survivors: A Mixed-Methods Study. Cancer Nurs. 2020, 43, 354–365. [Google Scholar] [CrossRef] [PubMed]
- Mock, V.; Dow, K.H.; Meares, C.J.; Grimm, P.M.; Dienemann, J.A.; Haisfield-Wolfe, M.E.; Quitasol, W.; Mitchell, S.; Chakravarthy, A.; Gage, I. Effects of Exercise on Fatigue, Physical Functioning, and Emotional Distress during Radiation Therapy for Breast Cancer. Oncol. Nurs. Forum 1997, 24, 991–1000. [Google Scholar]
- Segal, R.; Evans, W.; Johnson, D.; Smith, J.; Colletta, S.; Gayton, J.; Woodard, S.; Wells, G.; Reid, R. Structured Exercises Improves Physical Functioning in Women with Stages I and II Breast Cancer: Results of a Randomized Controlled Trial. J. Clin. Oncol. 2001, 19, 657–665. [Google Scholar] [CrossRef]
- Dimeo, F.C.; Stieglitz, R.D.; Novelli-Fischer, U.; Fetscher, S.; Keul, J. Effects of Physical Activity on the Fatigue and Psychologic Status of Cancer Patients during Chemotherapy. Cancer 1999, 85, 2273–2277. [Google Scholar] [CrossRef]
- Segal, R.J.; Reid, R.D.; Courneya, K.S.; Malone, S.C.; Parliament, M.B.; Scott, C.G.; Venner, P.M.; Quinney, H.A.; Jones, L.W.; D’Angelo, M.E.S.; et al. Resistance Exercise in Men Receiving Androgen Deprivation Therapy for Prostate Cancer. J. Clin. Oncol. 2003, 21, 1653–1659. [Google Scholar] [CrossRef]
- Ajzen, I.; Madden, T.J. Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control. J. Exp. Soc. Psychol. 1986, 22, 453–474. [Google Scholar] [CrossRef]
- Ricou, M.; Marina, S.; Vieira, P.M.; Duarte, I.; Sampaio, I.; Regalado, J.; Canário, C. Psychological Intervention at a Primary Health Care Center: Predictors of Success. BMC Fam. Pract. 2019, 20, 116. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Lynch, M.F.; Vansteenkiste, M.; Deci, E.L. Motivation and Autonomy in Counseling, Psychotherapy, and Behavior Change: A Look at Theory and Practice 1ψ7. Couns. Psychol. 2011, 39, 193–260. [Google Scholar] [CrossRef]
- Philips, B.; Wennberg, P. The Importance of Therapy Motivation for Patients with Substance Use Disorders. Psychotherapy 2014, 51, 555. [Google Scholar] [CrossRef] [PubMed]
- Clarkin, J.F.; Levy, K.N. The Influence of Client Variables on Psychotherapy. In Bergin and Garfield’s Handbook of Psychotherapy and Behavior Change; Wiley: Hoboken, NJ, USA, 2004. [Google Scholar]
- Sharf, J. Psychotherapy Dropout: A Meta-Analytic Review of Premature Termination. Diss. Abstr. Int. Sect. B Sci. Eng. 2008, 68, 6336. [Google Scholar]
- Teixeira, P.J.; Silva, M.N.; Mata, J.; Palmeira, A.L.; Markland, D. Motivation, Self-Determination, and Long-Term Weight Control. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Martin, E.; Bulsara, C.; Battaglini, C.; Hands, B.; Naumann, F.L. Breast and Prostate Cancer Survivor Responses to Group Exercise and Supportive Group Psychotherapy. J. Psychosoc. Oncol. 2015, 33, 620–634. [Google Scholar] [CrossRef] [Green Version]
- Bernard-Davila, B.; Aycinena, A.C.; Richardson, J.; Gaffney, A.O.; Koch, P.; Contento, I.; Molmenti, C.S.; Alvarez, M.; Hershman, D.; Greenlee, H. Barriers and Facilitators to Recruitment to a Culturally-Based Dietary Intervention among Urban Hispanic Breast Cancer Survivors. J. Racial Ethn. Health Disparities 2015, 2, 244–255. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The General Causality Orientations Scale: Self-Determination in Personality. J. Res. Pers. 1985, 19, 109–134. [Google Scholar] [CrossRef]
- Elfhag, K.; Rössner, S. Who Succeeds in Maintaining Weight Loss? A Conceptual Review of Factors Associated with Weight Loss Maintenance and Weight Regain. Obes. Rev. 2005, 6, 67–85. [Google Scholar] [CrossRef]
- Chen, B.; Vansteenkiste, M.; Beyers, W.; Boone, L.; Deci, E.L.; Van der Kaap-Deeder, J.; Duriez, B.; Lens, W.; Matos, L.; Mouratidis, A.; et al. Basic Psychological Need Satisfaction, Need Frustration, and Need Strength across Four Cultures. Motiv. Emot. 2015, 39, 216–236. [Google Scholar] [CrossRef]
- Jang, H.; Kim, E.J.; Reeve, J. Longitudinal Test of Self-Determination Theory’s Motivation Mediation Model in a Naturally Occurring Classroom Context. J. Educ. Psychol. 2012, 104, 1175. [Google Scholar] [CrossRef] [Green Version]
- Reis, H.T.; Sheldon, K.M.; Gable, S.L.; Roscoe, J.; Ryan, R.M. Daily Well-Being: The Role of Autonomy, Competence, and Relatedness. Pers. Soc. Psychol. Bull. 2000, 26, 419–435. [Google Scholar] [CrossRef]
- Taylor, I.M.; Lonsdale, C. Cultural Differences in the Relationships among Autonomy Support, Psychological Need Satisfaction, Subjective Vitality, and Effort in British and Chinese Physical Education. J. Sport Exerc. Psychol. 2010, 32, 655–673. [Google Scholar] [CrossRef] [Green Version]
- Vansteenkiste, M.; Simons, J.; Lens, W.; Sheldon, K.M.; Deci, E.L. Motivating Learning, Performance, and Persistence: The Synergistic Effects of Intrinsic Goal Contents and Autonomy-Supportive Contexts. J. Pers. Soc. Psychol. 2004, 87, 246. [Google Scholar] [CrossRef] [Green Version]
- Deci, E.L.; Ryan, R.M. The “What” and “Why” of Goal Pursuits: Human Needs and the Self-Determination of Behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Ng, J.Y.Y.; Ntoumanis, N.; Thøgersen-Ntoumani, C.; Deci, E.L.; Ryan, R.M.; Duda, J.L.; Williams, G.C. Self-Determination Theory Applied to Health Contexts: A Meta-Analysis. Perspect. Psychol. Sci. 2012, 7, 325–340. [Google Scholar] [CrossRef]
- Losier, G.F.; Koestner, R. Intrinsic versus Identified Regulation in Distinct Political Campaigns: The Consequences of Following Politics for Pleasure versus Personal Meaningfulness. Pers. Soc. Psychol. Bull. 1999, 25, 287–298. [Google Scholar] [CrossRef]
- Deci, E.L.; Koestner, R.; Ryan, R.M. The Undermining Effect Is a Reality after All--Extrinsic Rewards, Task Interest, and Self-Determination: Reply to Eisenberger, Pierce, and Cameron (1999) and Lepper, Henderlong, and Gingras (1999). Psychol. Bull. 1999, 125, 692–700. [Google Scholar] [CrossRef]
- Deci, E.L.; Koestner, R.; Ryan, R.M. Extrinsic Rewards and Intrinsic Motivation in Education: Reconsidered Once Again. Rev. Educ. Res. 2001, 71, 1–27. [Google Scholar] [CrossRef] [Green Version]
- Weiner, B. An attributional theory of achievement motivation and emotion. Psychol. Rev. 1985, 92, 548. [Google Scholar] [CrossRef]
- Pereira, A.I.; Barros, L. Parental Cognitions and Motivation to Engage in Psychological Interventions: A Systematic Review. Child Psychiatry Hum. Dev. 2019, 50, 347–361. [Google Scholar] [CrossRef] [PubMed]
- Sondell, A.; Rosendahl, E.; Sommar, J.N.; Littbrand, H.; Lundin-Olsson, L.; Lindelöf, N. Motivation to Participate in High-Intensity Functional Exercise Compared with a Social Activity in Older People with Dementia in Nursing Homes. PLoS ONE 2018, 13, e0206899. [Google Scholar] [CrossRef] [PubMed]
- Hughes-Morley, A.; Young, B.; Waheed, W.; Small, N.; Bower, P. Factors Affecting Recruitment into Depression Trials: Systematic Review, Meta-Synthesis and Conceptual Framework. J. Affect. Disord. 2015, 172, 274–290. [Google Scholar] [CrossRef] [PubMed]
- Paige, S.; Stellefson, M.; Singh, B. Patient Perspectives on Factors Associated with Enrollment and Retention in Chronic Disease Self-Management Programs: A Systematic Review. Patient Intell. 2016, 8, 21–37. [Google Scholar] [CrossRef] [Green Version]
- Hyde, M.K.; Dunn, J.; Scuffham, P.A.; Chambers, S.K. A Systematic Review of Episodic Volunteering in Public Health and Other Contexts. BMC Public Health 2014, 14, 992. [Google Scholar] [CrossRef] [Green Version]
- Kane, P.M.; Murtagh, F.E.M.; Ryan, K.; Mahon, N.G.; McAdam, B.; McQuillan, R.; Ellis-Smith, C.; Tracey, C.; Howley, C.; Raleigh, C.; et al. The Gap between Policy and Practice: A Systematic Review of Patient-Centred Care Interventions in Chronic Heart Failure. Heart Fail. Rev. 2015, 20, 673–687. [Google Scholar] [CrossRef] [Green Version]
- Soliman, W.; Tuunainen, V.K. Understanding Continued Use of Crowdsourcing Systems: An Interpretive Study. J. Theor. Appl. Electron. Commer. Res. 2015, 10, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Mills, J.; Bonner, A.; Francis, K. The Development of Constructivist Grounded Theory. Int. J. Qual. Methods 2006, 5, 25–35. [Google Scholar] [CrossRef]
- Bennett, J.A.; Riegel, B.; Bittner, V.; Nichols, J. Validity and Reliability of the NYHA Classes for Measuring Research Outcomes in Patients with Cardiac Disease. Hear. Lung J. Acute Crit. Care 2002, 31, 262–270. [Google Scholar] [CrossRef]
- Starks, H.; Trinidad, S.B. Choose Your Method: A Comparison of Phenomenology, Discourse Analysis, and Grounded Theory. Qual. Health Res. 2007, 17, 1372–1380. [Google Scholar] [CrossRef]
- O’Reilly, M.; Parker, N. “Unsatisfactory Saturation”: A Critical Exploration of the Notion of Saturated Sample Sizes in Qualitative Research. Qual. Res. 2013, 13, 190–197. [Google Scholar] [CrossRef]
- Noble, H.; Mitchell, G. What Is Grounded Theory? Evid. Based. Nurs. 2016, 19, 34–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charmaz, K. Grounded Theory: Objectivist and Constructivist Methods. In Handbook of Qualitative Research, 2nd ed.; Denzin, N.K., Lincoln, Y.S., Eds.; SAGE: Thousand Oaks, CA, USA, 2000. [Google Scholar]
- Charmaz, K. Grounded Theory in the 21st Century. In The Handbook of Qualitative Research, 3rd ed.; SAGE Publications: Thousand Oaks, CA, USA, 2005. [Google Scholar]
- Charmaz, K. Grounded Theory in Global Perspective: Reviews by International Researchers. Qual. Inq. 2014, 20, 1074–1084. [Google Scholar] [CrossRef]
- Henwood, K.; Pidgeon, N. Grounded Theory in Psychological Research. In Qualitative Research in Psychology: Expanding Perspectives in Methodology and Design; American Psychological Association: Worcester, MA, USA, 2004. [Google Scholar]
- Zorogastua, K.; Sriphanlop, P.; Reich, A.; Aly, S.; Cisse, A.; Jandorf, L. Breast and Cervical Cancer Screening among US and Non US Born African American Muslim Women in New York City. AIMS Public Health 2017, 4, 78. [Google Scholar] [CrossRef]
- Lai, Y.H.; Chang, J.T.C.; Keefe, F.J.; Chiou, C.F.; Chen, S.C.; Feng, S.C.; Dou, S.J.; Liao, M.N. Symptom distress, catastrophic thinking, and hope in nasopharyngeal carcinoma patients. Cancer Nurs. 2003, 26, 485–493. [Google Scholar] [CrossRef]
- Thøgersen-Ntoumani, C.; Shepherd, S.O.; Ntoumanis, N.; Wagenmakers, A.J.M.; Shaw, C.S. Intrinsic Motivation in Two Exercise Interventions: Associations With Fitness and Body Composition. Health Psychol. 2016, 35, 195. [Google Scholar] [CrossRef]
- Mascaro, J. A Longitudinal, Randomized and Controlled Study of App-Delivered Mindfulness in the Workplace. J. Wellness 2020, 2, 4. [Google Scholar] [CrossRef] [Green Version]
- Weman-Josefsson, K.; Johnson, U.; Lindwall, M. Zooming in on the Effects: A Controlled Trial on Motivation and Exercise Behaviour in a Digital Context. Curr. Psychol. 2018, 37, 250–262. [Google Scholar] [CrossRef]
- Ryan, R.M. The Oxford Handbook of Human Motivation; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Chiaburu, D.S.; Marinova, S.V.; Lim, A.S. Helping and Proactive Extra-Role Behaviors: The Influence of Motives, Goal Orientation, and Social Context. Pers. Individ. Dif. 2007, 43, 2282–2293. [Google Scholar] [CrossRef]
- Novick, G.; Sadler, L.S.; Kennedy, H.P.; Cohen, S.S.; Groce, N.E.; Knafl, K.A. Women’s Experience of Group Prenatal Care. Qual. Health Res. 2011, 21, 97–116. [Google Scholar] [CrossRef] [Green Version]
- Savioni, L.; Triberti, S. Cognitive Biases in Chronic Illness and Their Impact on Patients’ Commitment. Front. Psychol. 2020, 11, 579455. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Content Areas | Questions and Probes |
|---|---|
| Motivations/factors affecting the decision to participate in the intervention (original motivations) | What motivated you to participate in this intervention? How did you decide to participate in this intervention? What aspects did you take into consideration to decide to participate in this intervention? (Cosa l’ha spinta a decidere di partecipare? Come ha deciso? Quali aspetti ha preso in considerazione?) What objectives did you set for yourself within this training experience? (Quali obiettivi si è posta con la partecipazione a questo percorso di allenamento?) How much do these objectives guide your motivation to train? (Quanto questi obiettivi orientano la sua motivazione ad allenarsi?) Are there any other factors that influenced your decision to participate in this intervention? (Ci sono altri aspetti che hanno influenzato la sua decisione di partecipare a questo programma?) |
| Motivations/factor affecting engagement in the intervention after first months (evolved motivations) | What personal benefit do you expect from participating in this intervention? (Quale vantaggio personale si aspetta dalla partecipazione al programma?) What are the most common feelings towards the intervention? (Quali sentimenti più comuni nei confronti del progetto?) How do you imagine the organization of this intervention in the coming months? (Come si immagina l’organizzazione di questa attività nei prossimi mesi?) What additional personal benefits do you see from participating in this intervention? (Quale ulteriore vantaggio personale vede dalla partecipazione a questo programma di allenamento?) What additional features should this intervention have? (Quali ulteriori caratteristiche dovrebbe avere questo programma?) |
| Intervention experience and outcomes | Have your expectations been met (to this point in time)? (Le sue aspettative sono state soddisfatte finora?) How was your experience until now? (Come è andata finora l’esperienza?) Do you want to give us any other information on your personal experience of the intervention? (Vuole darci qualche altra informazione sulla sua esperienza personale dell’intervento?) |
| ID (Hypothetical Name) | Age | Education Level Reached | Marital Status | Type of Cancer Diagnosed in the Past |
|---|---|---|---|---|
| #1 (Rose) | 36 | High school | Maiden | Breast |
| #2 (Mary) | 38 | University degree or higher | Married | Breast |
| #3 (Catrine) | 55 | High school | Domestic partnership | Ovarian |
| #4 (Olivia) | 56 | Secondary degree | Married | Ovarian |
| #5 (Victoria) | 50 | University degree or higher | Married | Breast |
| #6 (Emily) | 55 | Secondary degree | Married | Breast |
| #7 (Charlotte) | 47 | University degree or higher | Married | Breast |
| #8 (Margaret) | 54 | High school | Married | Breast |
| #9 (Susan) | 59 | University degree or higher | Married | Breast |
| #10 (Sarah) | 48 | Secondary degree | Married | Uterine |
| #11 (Elizabeth) | 46 | University degree or higher | Married | Breast |
| #12 (Joanne) | 54 | University degree or higher | Maiden | Breast |
| #13 (Tracy) | 47 | High school | Maiden | Breast |
| #14 (Patricia) | 62 | High school | Married | Breast |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durosini, I.; Savioni, L.; Triberti, S.; Guiddi, P.; Pravettoni, G. The Motivation Journey: A Grounded Theory Study on Female Cancer Survivors’ Experience of a Psychological Intervention for Quality of Life. Int. J. Environ. Res. Public Health 2021, 18, 950. https://doi.org/10.3390/ijerph18030950
Durosini I, Savioni L, Triberti S, Guiddi P, Pravettoni G. The Motivation Journey: A Grounded Theory Study on Female Cancer Survivors’ Experience of a Psychological Intervention for Quality of Life. International Journal of Environmental Research and Public Health. 2021; 18(3):950. https://doi.org/10.3390/ijerph18030950
Chicago/Turabian StyleDurosini, Ilaria, Lucrezia Savioni, Stefano Triberti, Paolo Guiddi, and Gabriella Pravettoni. 2021. "The Motivation Journey: A Grounded Theory Study on Female Cancer Survivors’ Experience of a Psychological Intervention for Quality of Life" International Journal of Environmental Research and Public Health 18, no. 3: 950. https://doi.org/10.3390/ijerph18030950