
Exercise Prescription to Foster Health and Well-Being: A Behavioral Approach to Transform Barriers into Opportunities

Abstract
:1. Introduction
2. Sport and Exercise Medicine
- Conventional medical expertise is needed to adequately assess subjects/patients, to know medical implications of the disease to prevent/treat and of its eventual pharmacological treatment, to tailor exercise and nutrition prescriptions to subjects’/patients’ needs and characteristics, to reveal possible contraindications for some modalities/intensities of exercise.
- Psychological expertise is needed to motivate and help patients to change behavior and/or to manage possible psychological issues resulting from a major disease (if present) [70].
- Technical expertise is needed in order to prescribe exercise, nutrition or for smoking cessation programs, to educate subjects/patients and to help them overcome practical barriers.
3. Models to Implement Exercise into Lifestyle Programs
4. Subject’s Empowerment and Behavioral Medicine as Tools to Prescribe Exercise
4.1. Empowerment
4.2. Multiplicity of the Psychological Theories and Models which Can Be Useful (See Table 3)
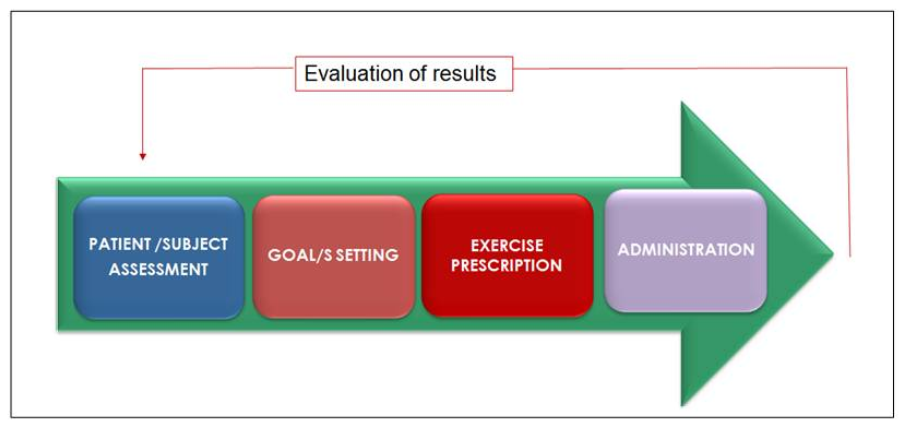
5. From Subject’s Assessment to Exercise Prescription
5.1. Subject Assessment
5.1.1. Clinical Assessment
5.1.2. Lifestyle Assessment
5.2. Goals Setting
5.3. Exercise Prescription
5.3.1. Exercise Modality: To Specify the Activity to Perform in Order to Reach the Set Goals
- Endurance activity entails rhythmic motion of large muscle groups in aerobic activities (walking, jogging, swimming, etc.) [93]. Aerobic activity is physical exercise that depends primarily on the aerobic energy-generating process [60], it may be of low to high intensity depending on subject’s fitness level (i.e., exercise capacity). Endurance aerobic activities are primarily prescribed in order to improve cardiorespiratory fitness, to reduce cardio-metabolic-oncologic risk, to reduce fat mass, to improve wellness and to maintain health [3,19,20,48,93].
- Resistance or strength exercise involves activities that use low- or moderate-repetition movements against resistance [93], it is primarily prescribed in order to increases strength and muscle mass and physical independence. Conventional strength exercises typically consist of lifting heavier weights with longer rest periods (a greater anaerobic component), whereas circuit training consists of lifting lighter weights with shorter rest periods between exercises, introducing a greater aerobic component to the workout [97].
- Flexibility and muscle stretching exercises are focused on improving joint range of motion (flexibility), and on decreasing muscle tension [103], they are primarily prescribed in order to relieve muscle pain associated to muscle tension, to improve joint range and to prevent injuries.
- Balance exercise are aimed to improve the ability to maintain the body’s center of gravity within its base of support and it is primarily prescribed in order to reduce the risk of falls and injury [104].
5.3.2. Exercise Intensity: To Define the Effort to Perform
- Endurance aerobic exercise: (see Table 4) Ideally, to define the intensity of an aerobic endurance exercise, a cardiopulmonary exercise test (CPX) would be required in order to establish cardiorespiratory fitness (VO2max) and subsequently define the exercise intensity as percent of it. From a practical point of view, the exercise intensity is usually indicated by training heart rate, based on the approximate linear relationship between the increase of O2 consumption and the increase of heart rate (HR). Training heart rate may be calculated employing the heart rate reserve (HRR) formula (see Table 4) starting from resting heart rate and actual maximal heart rate measured by conventional maximal (not submaximal!) exercise stress test. If it is not possible to perform even this test, the usage of predefined tables to estimate the training HR might be useful, but this easier approach cannot be considered a tailored exercise intensity prescription (it is only a best guess!) and must not be used in case of patients under pharmacological chronotropic therapies (such as beta blockers) or in subjects particularly deconditioned [105]. Another solution, particularly when it is useless/impossible to perform a maximal exercise stress test (for instance in the initial phase of a training program of a sedentary/deconditioned subject who might be unable to reach maximal cardiovascular response, because of low exercise capacity) empirical methods may be considered, as general physical activity promotion tools (Table 4).
- Strength exercise: to define the intensity of strength exercise is quite difficult. It depends from many factors, such as the resistance (generally represented by a weight to lift) that the muscle must win, the speed of movement and number of repetitions. Usually, there is an inverse association between the weight to lift and the speed of movement: the more elevated is the weight and the less is the speed of movement and/or then the number of repetitions that the subject may sustain. A lower repetition range with a heavier weight (anaerobic) may better optimize muscular strength and power, whereas a higher repetition range with a lighter weight may better enhance muscular endurance. Using weight loads that permit 8 to 15 repetitions will generally facilitate improvements in muscular strength and endurance [97]. To calculate strength intensity one-repetition maximum (1RM) (which is the maximum amount of weight that a person can possibly lift for one repetition, considered also as the maximum amount of force that can be generated in one maximal contraction) is generally employed [20,97]. 1RM can either be calculated directly using maximal testing or indirectly using submaximal estimation [108]. In order to better meet patients’ capabilities, the use of multiple repetitions, usually five (5RM) using a lighter weight, may be considered (5RM represents the maximum amount of weight that can be performed 5 times [20]). This technique helps to avoid maximal exercise which may be difficult to perform and possibly dangerous in risk populations.
5.3.3. Exercise Duration: Defines How Long the Exercise Session Has to Last
5.3.4. Exercise Frequency: To Define How Many Times the Subject Nneeds to Exercise
- Endurance aerobic exercise needs to be performed ideally every day, at least 5 days/week, particularly if the intensity of exercise is light or moderate. Subjects who are fit and can exercise at aerobic vigorous intensity may also exercise 3 days/week [16,18,20,93,109]. On the other hand when the goal is to improve metabolic control in diabetic and obese patients a high frequency is welcomed [48,111].
5.3.5. Exercise Progression
5.3.6. Exercise Execution
5.3.7. First and Follow Up Visits
6. Exercise to Manage Stress and Functional Syndromes
6.1. Management of Stress and Functional Syndromes
6.1.1. Explanation and Reassurance
6.1.2. Pharmacological and Psychological Treatments
6.1.3. Lifestyle Modifications
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seth, A. Exercise prescription: What does it mean for primary care? Br. J. Gen. Pract. 2014, 64, 12–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shephard, R.J.; Balady, G.J. Exercise as cardiovascular therapy. Circulation 1999, 99, 963–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallis, R.E. Exercise is medicine and physicians need to prescribe it! Br. J. Sports Med. 2009, 43, 3–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucini, D.; Malacarne, M.; Gatzemeier, W.; Pagani, M. A Simple Home-Based Lifestyle Intervention Program to Improve Cardiac Autonomic Regulation in Patients with Increased Cardiometabolic Risk. Sustainability 2020, 12, 7671. [Google Scholar] [CrossRef]
- Sjøgaard, G.; Christensen, J.R.; Justesen, J.B.; Murray, M.; Dalager, T.; Fredslund, G.H.; Søgaard, K. Exercise is more than medicine: The working age population’s well-being and productivity. J. Sport Health Sci. 2016, 5, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Allen, L.N.; Feigl, A.B. Reframing non-communicable diseases as socially transmitted conditions. Lancet Glob. Health 2017, 5, e644–e646. [Google Scholar] [CrossRef] [Green Version]
- Christakis, N.A.; Fowler, J.H. The spread of obesity in a large social network over 32 years. N. Engl. J. Med. 2007, 357, 370–379. [Google Scholar] [CrossRef] [Green Version]
- Eime, R.M.; Harvey, J.T.; Charity, M.J.; Casey, M.M.; Van Uffelen, J.G.; Payne, W.R. The contribution of sport participation to overall health enhancing physical activity levels in Australia: A population-based study. BMC Public Health 2015, 15, 806. [Google Scholar] [CrossRef] [Green Version]
- Sharon-David, H.; Tenenbaum, G. The effectiveness of exercise interventions on coping with stress: Research synthesis. Stud. Sport Hum. 2017, 21, 19–29. [Google Scholar] [CrossRef]
- Lathia, N.; Sandstrom, G.M.; Mascolo, C.; Rentfrow, P.J. Happier People Live More Active Lives: Using Smartphones to Link Happiness and Physical Activity. PLoS ONE 2017, 12, e0160589. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A.N. Physical activity, fitness, cognitive function, and academic achievement in children: A systematic review. Med. Sci. Sports Exerc. 2016, 48, 1197. [Google Scholar] [CrossRef] [Green Version]
- Clark, L.V.; Pesola, F.; Thomas, J.M.; Vergara-Williamson, M.; Beynon, M.; White, P.D. Guided graded exercise self-help plus specialist medical care versus specialist medical care alone for chronic fatigue syndrome (GETSET): A pragmatic randomised controlled trial. Lancet 2017, 390, 363–373. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, R.J.; Ozminkowski, R.J.; Serxner, S. Improving employee productivity through improved health. J. Occup. Environ. Med. 2013, 55, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Milani, R.V.; Lavie, C.J. Health Care 2020: Reengineering Health Care Delivery to Combat Chronic Disease. Am. J. Med. 2015, 128, 337–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, G.; Burke, L.E.; Spring, B.J.; Ewing, L.J.; Turk, M.; Lichtenstein, A.H.; Cornier, M.; Spence, J.D.; Coons, M. New and emerging weight management strategies for busy ambulatory settings: A scientific statement from the American Heart Association endorsed by the Society of Behavioral Medicine. Circulation 2011, 124, 1182–1203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van, H.L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: The American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef] [Green Version]
- Spring, B.; Ockene, J.K.; Gidding, S.S.; Mozaffarian, D.; Moore, S.; Rosal, M.C.; Brown, M.D.; Vafiadis, D.K.; Cohen, D.L.; Burke, L.E. Better population health through behavior change in adults: A call to action. Circulation 2013, 128, 2169–2176. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 74, 1376–1414. [Google Scholar] [CrossRef]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The physical activity guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular diseaseThe Task Force on sports cardiology and exercise in patients with cardiovascular disease of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 1–80. [Google Scholar] [CrossRef]
- Schmitz, K.H.; Campbell, A.M.; Stuiver, M.M.; Pinto, B.M.; Schwartz, A.L.; Morris, G.S.; Ligibel, J.A.; Cheville, A.; Galvão, D.A.; Alfano, C.M. Exercise is medicine in oncology: Engaging clinicians to help patients move through cancer. CA A Cancer J. Clin. 2019, 69, 468–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef] [Green Version]
- Wen, C.P.; Wai, J.P.; Tsai, M.K.; Yang, Y.C.; Cheng, T.Y.; Lee, M.C.; Chan, H.T.; Tsao, C.K.; Tsai, S.P.; Wu, X. Minimum amount of physical activity for reduced mortality and extended life expectancy: A prospective cohort study. Lancet 2011, 378, 1244–1253. [Google Scholar] [CrossRef]
- Lucini, D.; Pagani, M. Exercise: Should it matter to internal medicine? Eur. J. Intern. Med. 2011, 22, 363–370. [Google Scholar] [CrossRef]
- Lucini, D.; Pagani, M. From stress to functional syndromes: An internist’s point of view. Eur. J. Intern. Med. 2012, 23, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Kyu, H.H.; Bachman, V.F.; Alexander, L.T.; Mumford, J.E.; Afshin, A.; Estep, K.; Veerman, J.L.; Delwiche, K.; Iannarone, M.L.; Moyer, M.L. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: Systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. BMJ 2016, 354, i3857. [Google Scholar] [CrossRef] [Green Version]
- Moore, S.C.; Lee, I.M.; Weiderpass, E.; Campbell, P.T.; Sampson, J.N.; Kitahara, C.M.; Keadle, S.K.; Arem, H.; Berrington de, G.A.; Hartge, P.; et al. Association of Leisure-Time Physical Activity With Risk of 26 Types of Cancer in 1.44 Million Adults. JAMA Intern. Med. 2016, 176, 816–825. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Li, Y.; Pan, A.; Wang, D.D.; Liu, X.; Dhana, K.; Franco, O.H.; Kaptoge, S.; Di Angelantonio, E.; Stampfer, M.; Willett, W.C. Impact of healthy lifestyle factors on life expectancies in the US population. Circulation 2018, 138, 345–355. [Google Scholar] [CrossRef]
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Despres, J.P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e653–e699. [Google Scholar] [CrossRef]
- Li, R.; Xia, J.; Zhang, X.I.; Gathirua-Mwangi, W.G.; Guo, J.; Li, Y.; McKenzie, S.; Song, Y. Associations of muscle mass and strength with all-cause mortality among US older adults. Med. Sci. Sports Exerc. 2018, 50, 458. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Keum, N.; Hu, F.B.; Orav, E.J.; Rimm, E.B.; Willett, W.C.; Giovannucci, E.L. Predicted lean body mass, fat mass, and all cause and cause specific mortality in men: Prospective US cohort study. BMJ 2018, 362, k2575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasanen, T.; Tolvanen, S.; Heinonen, A.; Kujala, U.M. Exercise therapy for functional capacity in chronic diseases: An overview of meta-analyses of randomised controlled trials. Br. J. Sports Med. 2017, 51, 1459–1465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kokkinos, P.; Myers, J. Exercise and physical activity: Clinical outcomes and applications. Circulation 2010, 122, 1637–1648. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Atwood, J.E. Exercise capacity and mortality among men referred for exercise testing. N. Engl. J. Med. 2002, 346, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Joyner, M.J.; Green, D.J. Exercise protects the cardiovascular system: Effects beyond traditional risk factors. J. Physiol. 2009, 587, 5551–5558. [Google Scholar] [CrossRef]
- White, D.W.; Raven, P.B. Autonomic neural control of heart rate during dynamic exercise: Revisited. J. Physiol. 2014, 592, 2491–2500. [Google Scholar] [CrossRef]
- Kadoglou, N.P.; Iliadis, F.; Angelopoulou, N.; Perrea, D.; Ampatzidis, G.; Liapis, C.D.; Alevizos, M. The anti-inflammatory effects of exercise training in patients with type 2 diabetes mellitus. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 837–843. [Google Scholar] [CrossRef]
- Hansen, D.; Meeusen, R.; Mullens, A.; Dendale, P. Effect of acute endurance and resistance exercise on endocrine hormones directly related to lipolysis and skeletal muscle protein synthesis in adult individuals with obesity. Sports Med. 2012, 42, 415–431. [Google Scholar] [CrossRef]
- Nieman, D.C.; Wentz, L.M. The compelling link between physical activity and the body’s defense system. J. Sport Health Sci. 2019, 8, 201–217. [Google Scholar] [CrossRef]
- Da Silveira, M.P.; Da Silva Fagundes, K.K.; Bizuti, M.R.; Starck, E.; Calciolari Rossi, C.; Tavares de Resende, E.; Silva, D. Physical exercise as a tool to help the immune system against COVID-19: An integrative review of the current literature. Clin. Exp. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Estaki, M.; Pither, J.; Baumeister, P.; Little, J.P.; Gill, S.K.; Ghosh, S.; Ahmadi-Vand, Z.; Marsden, K.R.; Gibson, D.L. Cardiorespiratory fitness as a predictor of intestinal microbial diversity and distinct metagenomic functions. Microbiome 2016, 4, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucini, D.; Sala, R.; Spataro, A.; Malacarne, M.; Benzi, M.; Tamorri, S.; Pagani, M. Can the use of a single integrated unitary autonomic index provide early clues for eventual eligibility for olympic games? Eur. J. Appl. Physiol. 2018, 118, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Oggionni, G.; Spataro, A.; Pelliccia, A.; Malacarne, M.; Pagani, M.; Lucini, D. Left ventricular hypertrophy in world class elite athletes is associated with signs of improved cardiac autonomic regulation. Eur. J. Prev. Cardiol. 2019. [Google Scholar] [CrossRef]
- Khera, A.V.; Emdin, C.A.; Drake, I.; Natarajan, P.; Bick, A.G.; Cook, N.R.; Chasman, D.I.; Baber, U.; Mehran, R.; Rader, D.J. Genetic risk, adherence to a healthy lifestyle, and coronary disease. N. Engl. J. Med. 2016, 375, 2349–2358. [Google Scholar] [CrossRef] [Green Version]
- Jaenisch, R.; Bird, A. Epigenetic regulation of gene expression: How the genome integrates intrinsic and environmental signals. Nat. Genet 2003, 33, 245–254. [Google Scholar] [CrossRef]
- Van Roojen, S.; Carli, F.; Dalton, S.; Thomas, G.; Bojesen, R.; Le Gueen, M.; Barizien, N.; Awasthi, R.; Minnella, E.; Beijer, S.; et al. Multimodal prehabilitation in colorectal cancer patients to improve functional capacity and reduce postoperative complications: The first international randomized controlled trial for multimodal prehabilitation. BMC Cancer 2019, 19, 98. [Google Scholar] [CrossRef]
- American College of Sports Medicine, Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Lippincot Williams & Wilkins: Philadelphia, PA, USA, 2018. [Google Scholar]
- Racette, S.B.; Weiss, E.P.; Villareal, D.T.; Arif, H.; Steger-May, K.; Schechtman, K.B.; Fontana, L.; Klein, S.; Holloszy, J.O. One year of caloric restriction in humans: Feasibility and effects on body composition and abdominal adipose tissue. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 943–950. [Google Scholar] [CrossRef] [Green Version]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Chau, J.Y.; Grunseit, A.; Midthjell, K.; Holmen, J.; Holmen, T.L.; Bauman, A.E.; Van der Ploeg, H.P. Sedentary behaviour and risk of mortality from all-causes and cardiometabolic diseases in adults: Evidence from the HUNT3 population cohort. Br. J. Sports Med. 2015, 49, 737–742. [Google Scholar] [CrossRef]
- LEXICO: Oxford english and spanish Dictionary. Available online: https://www.lexico.com/definition/wellness (accessed on 4 December 2020).
- UCDAVIS. Available online: https://shcs.ucdavis.edu/wellness/what-is-wellness (accessed on 4 December 2020).
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/hrqol/wellbeing.htm (accessed on 4 December 2020).
- The Preamble of the Constitution of the World HealthOrganization. Available online: https://apps.who.int/iris/bitstream/handle/10665/71722/bulletin_2002_80%2812%29_981-984.pdf?sequence=1&isAllowed=y (accessed on 20 January 2021).
- Farlex Partner Medical Dictionary © Farlex 2012. Available online: https://medical-dictionary.thefreedictionary.com/lifestyle (accessed on 4 December 2020).
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too much sitting: The population health science of sedentary behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Available online: https://www.lexico.com/definition/sport (accessed on 4 December 2020).
- Plowman, S.A.; Smith, D.L. Exercise Physiology for Health, Fitness, and Performance; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007. [Google Scholar]
- American College of Lifestyle Medicine. The American College of Lifestyle Medicine Standards. Available online: https://www.lifestylemedicine.org/ACLM-Standards (accessed on 4 December 2020).
- Thornton, J.S.; Fremont, P.; Khan, K.; Poirier, P.; Fowles, J.; Wells, G.D.; Frankovich, R.J. Physical Activity Prescription: A Critical Opportunity to Address a Modifiable Risk Factor for the Prevention and Management of Chronic Disease: A Position Statement by the Canadian Academy of Sport and Exercise Medicine. Clin. J. Sport Med. 2016, 26, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smart, N.A.; Williams, A.; Lyndon, K. The role and scope of accredited exercise physiologists in the Australian healthcare system. J. Clin. Exerc. Physiol. 2016, 5, 16–20. [Google Scholar] [CrossRef]
- McCrory, P. What is sports and exercise medicine? Br. J. Sports Med. 2006, 40, 955–957. [Google Scholar]
- Gates, A.B.; Kerry, R.; Moffatt, F.; Ritchie, I.K.; Meakins, A.; Thornton, J.S.; Rosenbaum, S.; Taylor, A. Movement for Movement: Exercise as Everybody’s Business? BMJ Publishing Group Ltd: London, UK, 2016. [Google Scholar]
- Bennell, K.; Webb, G. Educating Australian physiotherapists: Striving for excellence in sport and exercise medicine. Br. J. Sports Med. 2000, 34, 241–243. [Google Scholar] [CrossRef] [Green Version]
- Lianov, L.; Johnson, M. Physician competencies for prescribing lifestyle medicine. JAMA 2010, 304, 202–203. [Google Scholar] [CrossRef]
- Hivert, M.F.; Arena, R.; Forman, D.E.; Kris-Etherton, P.M.; McBride, P.E.; Pate, R.R.; Spring, B.; Trilk, J.; Van Horn, L.V.; Kraus, W.E. Medical Training to Achieve Competency in Lifestyle Counseling: An Essential Foundation for Prevention and Treatment of Cardiovascular Diseases and Other Chronic Medical Conditions: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e308–e327. [Google Scholar] [CrossRef] [Green Version]
- Trilk, J.; Nelson, L.; Briggs, A.; Muscato, D. Including Lifestyle Medicine in Medical Education: Rationale for American College of Preventive Medicine/American Medical Association Resolution 959. Am. J. Prev. Med. 2019, 56, e169–e175. [Google Scholar] [CrossRef] [Green Version]
- Engel, B.T. Psychosomatic medicine, behavioral medicine, just plain medicine. Psychosom. Med. 1986, 48, 466–479. [Google Scholar] [CrossRef]
- Phillips, E.; Pojednic, R.; Polak, R.; Bush, J.; Trilk, J. Including lifestyle medicine in undergraduate medical curricula. Med Educ Online 2015, 20, 26150. [Google Scholar] [CrossRef] [PubMed]
- Kraus, W.E.; Bittner, V.; Appel, L.; Blair, S.N.; Church, T.; Despres, J.P.; Franklin, B.A.; Miller, T.D.; Pate, R.R.; Taylor-Piliae, R.E.; et al. The National Physical Activity Plan: A Call to Action From the American Heart Association: A Science Advisory From the American Heart Association. Circulation 2015, 131, 1932–1940. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; Van, M.W.; Pratt, M. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef]
- Heath, G.W.; Parra, D.C.; Sarmiento, O.L.; Andersen, L.B.; Owen, N.; Goenka, S.; Montes, F.; Brownson, R.C. Evidence-based intervention in physical activity: Lessons from around the world. Lancet 2012, 380, 272–281. [Google Scholar] [CrossRef] [Green Version]
- Reis, R.S.; Salvo, D.; Ogilvie, D.; Lambert, E.V.; Goenka, S.; Brownson, R.C. Scaling up physical activity interventions worldwide: Stepping up to larger and smarter approaches to get people moving. Lancet 2016, 388, 1337–1348. [Google Scholar] [CrossRef] [Green Version]
- Friedberg, M.W.; Schneider, E.C.; Rosenthal, M.B.; Volpp, K.G.; Werner, R.M. Association between participation in a multipayer medical home intervention and changes in quality, utilization, and costs of care. JAMA 2014, 311, 815–825. [Google Scholar] [CrossRef] [Green Version]
- Song, Z.; Baicker, K. Effect of a Workplace Wellness Program on Employee Health and Economic Outcomes: A Randomized Clinical Trial. JAMA 2019, 321, 1491–1501. [Google Scholar] [CrossRef]
- Stead, M.; Craigie, A.M.; Macleod, M.; McKell, J.; Caswell, S.; Steele, R.J.; Anderson, A.S. Why are some people more successful at lifestyle change than others? Factors associated with successful weight loss in the BeWEL randomised controlled trial of adults at risk of colorectal cancer. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 87. [Google Scholar] [CrossRef] [Green Version]
- Murray, J.; Craigs, C.L.; Hill, K.M.; Honey, S.; House, A. A systematic review of patient reported factors associated with uptake and completion of cardiovascular lifestyle behaviour change. BMC Cardiovasc. Disord. 2012, 12, 120. [Google Scholar] [CrossRef] [Green Version]
- Lakerveld, J.; Ijzelenberg, W.; Van Tulder, M.W.; Hellemans, I.M.; Rauwerda, J.A.; Van Rossum, A.C.; Seidell, J. Motives for (not) participating in a lifestyle intervention trial. BMC Med. Res. Methodol. 2008, 8, 17. [Google Scholar] [CrossRef] [Green Version]
- Graham, I.M.; Stewart, M.; Hertog, M.G. Factors impeding the implementation of cardiovascular prevention guidelines: Findings from a survey conducted by the European Society of Cardiology. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 839–845. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Available online: https://www.ncbi.nlm.nih.gov/books/NBK144022/ (accessed on 4 December 2020).
- Available online: https://www.sbm.org/about/behavioral-medicine (accessed on 4 December 2020).
- Rollnick, S.; Butler, C.C.; Kinnersley, P.; Gregory, J.; Mash, B. Motivational interviewing. BMJ 2010, 340, c1900. [Google Scholar] [CrossRef] [PubMed]
- Dalle Grave, R.; Calugi, S.; Centis, E.; El Ghoch, M.; Marchesini, G. Cognitive-behavioral strategies to increase the adherence to exercise in the management of obesity. J. Obes. 2011, 2011, 348293. [Google Scholar] [CrossRef] [PubMed]
- Artinian, N.T.; Fletcher, G.F.; Mozaffarian, D.; Kris-Etherton, P.; Van Horn, L.; Lichtenstein, A.H.; Kumanyika, S.; Kraus, W.E.; Fleg, J.L.; Redeker, N.S.; et al. Interventions to promote physical activity and dietary lifestyle changes for cardiovascular risk factor reduction in adults: A scientific statement from the American Heart Association. Circulation 2010, 122, 406–441. [Google Scholar] [CrossRef]
- Lucini, D.; Zanuso, S.; Blair, S.; Pagani, M. A simple healthy lifestyle index as a proxy of wellness: A proof of concept. Acta Diabetol. 2015, 52, 81–89. [Google Scholar] [CrossRef]
- Ledderer, L.; Kjaer, M.; Madsen, E.K.; Busch, J.; Fage-Butler, A. Nudging in Public Health Lifestyle Interventions: A Systematic Literature Review and Metasynthesis. Health Educ. Behav. 2020, 47, 749–764. [Google Scholar] [CrossRef]
- Prochaska, J.O.; DiClemente, C.C. The Transtheoretical Approach, 2nd ed.; Oxford University Press: New York, NY, USA, 2005; pp. 147–171. [Google Scholar]
- Bandura, A. Human agency in social cognitive theory. Am. Psychol. 1989, 44, 1175. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Gagné, M.; Deci, E.L. Self determination theory and work motivation. J. Organ. Behav. 2005, 26, 331–362. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C. Exercise standards for testing and training: A scientific statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef]
- Strath, S.J.; Kaminsky, L.A.; Ainsworth, B.E.; Ekelund, U.; Freedson, P.S.; Gary, R.A.; Richardson, C.R.; Smith, D.T.; Swartz, A.M. Guide to the assessment of physical activity: Clinical and research applications: A scientific statement from the American Heart Association. Circulation 2013, 128, 2259–2279. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.A.; Haskell, W.L.; Ades, P.A.; Amsterdam, E.A.; Bittner, V.; Franklin, B.A.; Gulanick, M.; Laing, S.T.; Stewart, K.J. Resistance exercise in individuals with and without cardiovascular disease: 2007 update: A scientific statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism. Circulation 2007, 116, 572–584. [Google Scholar] [CrossRef] [Green Version]
- Coenen, P.; Huysmans, M.A.; Holtermann, A.; Krause, N.; Van, M.W.; Straker, L.M.; Van der Beek, A.J. Do highly physically active workers die early? A systematic review with meta-analysis of data from 193 696 participants. Br. J. Sports Med. 2018, 52, 1320–1326. [Google Scholar] [CrossRef] [Green Version]
- Schnohr, P.; O’Keefe, J.H.; Marott, J.L.; Lange, P.; Jensen, G.B. Dose of jogging and long-term mortality: The Copenhagen City Heart Study. J. Am. Coll. Cardiol. 2015, 65, 411–419. [Google Scholar] [CrossRef]
- Steinberger, J.; Daniels, S.R.; Hagberg, N.; Isasi, C.R.; Kelly, A.S.; Lloyd-Jones, D.; Pate, R.R.; Pratt, C.; Shay, C.M.; Towbin, J.A. Cardiovascular health promotion in children: Challenges and opportunities for 2020 and beyond: A scientific statement from the American Heart Association. Circulation 2016, 134, e236–e255. [Google Scholar] [CrossRef] [Green Version]
- WHO Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age; World Health Organization: Geneva, Switzerland, 2019.
- Zubin Maslov, P.; Schulman, A.; Lavie, C.J.; Narula, J. Personalized exercise dose prescription. Eur. Heart J. 2017, 39, 2346–2355. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, K.; Kodama, T.; Mukaino, Y. Effects of active individual muscle stretching on muscle function. J Phys. Sci. 2014, 26, 341–344. [Google Scholar] [CrossRef] [Green Version]
- DiStefano, L.J.; Clark, M.A.; Padua, D.A. Evidence supporting balance training in healthy individuals: A systemic review. J. Strength Cond. Res. 2009, 23, 2718–2731. [Google Scholar] [CrossRef]
- Vanhees, L.; Geladas, N.; Hansen, D.; Kouidi, E.; Niebauer, J.; Reiner, Ž.; Cornelissen, V.; Adamopoulos, S.; Prescott, E.; Börjesson, M. Importance of characteristics and modalities of physical activity and exercise in the management of cardiovascular health in individuals with cardiovascular risk factors: Recommendations from the EACPR (Part II). Eur. J. Prev. Cardiol. 2012, 19, 1005–1033. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.C.; Lavie, C.J.; Vedanthan, R. Optimal dose of running for longevity: Is more better or worse? J. Am. Coll. Cardiol. 2015, 65, 420–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binder, R.K.; Wonisch, M.; Corra, U.; Cohen-Solal, A.; Vanhees, L.; Saner, H.; Schmid, J.P. Methodological approach to the first and second lactate threshold in incremental cardiopulmonary exercise testing. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Marchese, R.; Hill, A. The Essential Guide to Fitness: For the Fitness Instructor; Pearson Education: Sydney, Australia, 2011. [Google Scholar]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrá, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef] [PubMed]
- Vanhees, L.; De Sutter, J.; Geladas, N.; Doyle, F.; Prescott, E.; Cornelissen, V.; Kouidi, E.; Dugmore, D.; Vanuzzo, D.; Börjesson, M. Importance of characteristics and modalities of physical activity and exercise in defining the benefits to cardiovascular health within the general population: Recommendations from the EACPR (Part I). Eur. J. Prev. Cardiol. 2012, 19, 670–686. [Google Scholar] [CrossRef]
- Cefalu, W.T. The journal of clinical and applied research and education. Diabetes Care 2017, 40, 1611–1613. [Google Scholar]
- Thompson, W.R.; Gordon, N.F.; Pescatello, L.S. ACSM’s Guidelines for Exercise Testing and Prescription, 8th ed.; Lippincot Williams & Wilkins: Phyladelphya, PA, USA, 2009. [Google Scholar]
- Engel, B.T. Stress is a noun! No, a verb! No, an adjective. Stress Coping 1985, 1, 3–12. [Google Scholar]
- McEwen, B.S. Protective and damaging effects of stress mediators. N. Engl. J. Med. 1998, 338, 171–179. [Google Scholar] [CrossRef] [Green Version]
- Rozanski, A.; Blumenthal, J.A.; Davidson, K.W.; Saab, P.G.; Kubzansky, L. The epidemiology, pathophysiology, and management of psychosocial risk factors in cardiac practice: The emerging field of behavioral cardiology. J. Am. Coll. Cardiol. 2005, 45, 637–651. [Google Scholar] [CrossRef] [Green Version]
- Selye, H. The Stress of Life; McGraw-Hill: New York, NY, USA, 1956. [Google Scholar]
- Tracey, K.J. The inflammatory reflex. Nature 2002, 420, 853–858. [Google Scholar] [CrossRef]
- Ulrich-Lai, Y.M.; Herman, J.P. Neural regulation of endocrine and autonomic stress responses. Nat. Rev. Neurosci. 2009, 10, 397–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brotman, D.J.; Golden, S.H.; Wittstein, I.S. The cardiovascular toll of stress. Lancet 2007, 370, 1089–1100. [Google Scholar] [CrossRef]
- Dimsdale, J.E. Psychological stress and cardiovascular disease. J. Am. Coll. Cardiol. 2008, 51, 1237–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatcher, S.; Arroll, B. Assessment and management of medically unexplained symptoms. BMJ 2008, 336, 1124–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayou, R.; Farmer, A. ABC of psychological medicine: Functional somatic symptoms and syndromes. BMJ 2002, 325, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Burton, C.; Fink, P.; Henningsen, P.; Lowe, B.; Rief, W. Functional somatic disorders: Discussion paper for a new common classification for research and clinical use. BMC Med. 2020, 18, 34. [Google Scholar] [CrossRef] [Green Version]
- Van Houdenhove, B.; Luyten, P. Customizing treatment of chronic fatigue syndrome and fibromyalgia: The role of perpetuating factors. Psychosomatics 2008, 49, 470–477. [Google Scholar] [CrossRef]
- Van den Bos, R.; Harteveld, M.; Stoop, H. Stress and decision-making in humans: Performance is related to cortisol reactivity, albeit differently in men and women. Psychoneuroendocrinology 2009, 34, 1449–1458. [Google Scholar] [CrossRef]
- Dias-Ferreira, E.; Sousa, J.C.; Melo, I.; Morgado, P.; Mesquita, A.R.; Cerqueira, J.J.; Costa, R.M.; Sousa, N. Chronic stress causes frontostriatal reorganization and affects decision-making. Science 2009, 325, 621–625. [Google Scholar] [CrossRef]
- Wessely, S.; Nimnuan, C.; Sharpe, M. Functional somatic syndromes: One or many? Lancet 1999, 354, 936–939. [Google Scholar] [CrossRef]
- Henningsen, P.; Zipfel, S.; Herzog, W. Management of functional somatic syndromes. Lancet 2007, 369, 946–955. [Google Scholar] [CrossRef]
- Dimsdale, J.E.; Dantzer, R. A biological substrate for somatoform disorders: Importance of pathophysiology. Psychosom. Med. 2007, 69, 850–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucini, D.; Di Fede, G.; Parati, G.; Pagani, M. Impact of chronic psychosocial stress on autonomic cardiovascular regulation in otherwise healthy subjects. Hypertension 2005, 46, 1201–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucini, D.; Malacarne, M.; Solaro, N.; Busin, S.; Pagani, M. Complementary medicine for the management of chronic stress: Superiority of active versus passive techniques. J. Hypertens. 2009, 27, 2421–2428. [Google Scholar] [CrossRef] [PubMed]
- Salvioli, B.; Pellegatta, G.; Malacarne, M.; Pace, F.; Malesci, A.; Pagani, M.; Lucini, D. Autonomic nervous system dysregulation in irritable bowel syndrome. Neurogastroenterol. Motil. 2015, 27, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Lucini, D.; Riva, S.; Pizzinelli, P.; Pagani, M. Stress management at the worksite: Reversal of symptoms profile and cardiovascular dysregulation. Hypertension 2007, 49, 291–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, J.S.; Wild, H.; Kenzie, E.S.; Wakeland, W.; Budding, D.; Lillas, C. Diverse Autonomic Nervous System Stress Response Patterns in Childhood Sensory Modulation. Front. Integr. Neurosci. 2020, 14, 6. [Google Scholar] [CrossRef] [Green Version]
- Rozanski, A. Integrating psychologic approaches into the behavioral management of cardiac patients. Psychosom. Med. 2005, 67 (Suppl S1), S67–S73. [Google Scholar] [CrossRef]
- Baker, R.; Shaw, E.J. Diagnosis and management of chronic fatigue syndrome or myalgic encephalomyelitis (or encephalopathy): Summary of NICE guidance. BMJ 2007, 335, 446–448. [Google Scholar] [CrossRef] [Green Version]
- Prins, J.B.; Van der Meer, J.W.; Bleijenberg, G. Chronic fatigue syndrome. Lancet 2006, 367, 346–355. [Google Scholar] [CrossRef]
- Henningsen, P.; Herzog, W. Irritable bowel syndrome and somatoform disorders. J. Psychosom. Res. 2008, 64, 625–629. [Google Scholar] [CrossRef] [PubMed]
- Mayou, R. Are treatments for common mental disorders also effective for functional symptoms and disorder? Psychosom. Med. 2007, 69, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Spiller, R.; Aziz, Q.; Creed, F.; Emmanuel, A.; Houghton, L.; Hungin, P.; Jones, R.; Kumar, D.; Rubin, G.; Trudgill, N. Guidelines on the irritable bowel syndrome: Mechanisms and practical management. Gut 2007, 56, 1770–1798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huibers, M.J.; Beurskens, A.J.; Van Schayck, C.P.; Bazelmans, E.; Metsemakers, J.F.; Knottnerus, J.A.; Bleijenberg, G. Efficacy of cognitive-behavioural therapy by general practitioners for unexplained fatigue among employees: Randomised controlled trial. Br. J. Psychiatry 2004, 184, 240–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumenthal, J.A.; Sherwood, A.; Babyak, M.A.; Watkins, L.L.; Waugh, R.; Georgiades, A.; Bacon, S.L.; Hayano, J.; Coleman, R.E.; Hinderliter, A. Effects of exercise and stress management training on markers of cardiovascular risk in patients with ischemic heart disease: A randomized controlled trial. JAMA 2005, 293, 1626–1634. [Google Scholar] [CrossRef]
- Prins, J.B.; Bleijenberg, G.; Bazelmans, E.; Elving, L.D.; De Boo, T.M.; Severens, J.L.; Van der Wilt, G.J.; Spinhoven, P.; Van der Meer, J.W. Cognitive behaviour therapy for chronic fatigue syndrome: A multicentre randomised controlled trial. Lancet 2001, 357, 841–847. [Google Scholar] [CrossRef]
- Lucini, D.; Covacci, G.; Milani, R.; Mela, G.S.; Malliani, A.; Pagani, M. A controlled study of the effects of mental relaxation on autonomic excitatory responses in healthy subjects. Psychosom. Med. 1997, 59, 541–552. [Google Scholar] [CrossRef]
- Tsatsoulis, A.; Fountoulakis, S. The protective role of exercise on stress system dysregulation and comorbidities. Ann. N. Y. Acad. Sci. 2006, 1083, 196–213. [Google Scholar] [CrossRef]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef]
- Busch, A.J.; Schachter, C.L.; Overend, T.J.; Peloso, P.M.; Barber, K.A. Exercise for fibromyalgia: A systematic review. J. Rheumatol. 2008, 35, 1130–1144. [Google Scholar]
- Gordon, B.R.; McDowell, C.P.; Lyons, M.; Herring, M.P. Resistance exercise training for anxiety and worry symptoms among young adults: A randomized controlled trial. Sci. Rep. 2020, 10, 17548. [Google Scholar] [CrossRef] [PubMed]
- Matheson, G.O.; Witteman, H.O.; Mochar, T.G. Disease prevention: What’s really important? Br. J. Sports Med. 2015, 49, 1483–1484. [Google Scholar] [CrossRef] [PubMed]
- Polak, R.; Pojednic, R.M.; Phillips, E.M. Lifestyle medicine education. Am. J. Lifestyle Med. 2015, 9, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Frank, E.; Rothenberg, R.; Lewis, C.; Belodoff, B.F. Correlates of physicians’ prevention-related practices: Findings from the Women Physicians’ Health Study. Arch. Fam. Med. 2000, 9, 359. [Google Scholar] [CrossRef] [PubMed]
- Frank, E. Physician health and patient care. JAMA 2004, 291, 637. [Google Scholar] [CrossRef]
- Wallace, J.E.; Lemaire, J.B.; Ghali, W.A. Physician wellness: A missing quality indicator. Lancet 2009, 374, 1714–1721. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| WELLNESS | The state of being in good health, especially as an actively pursued goal. It is an active process of becoming aware of and making choices toward a healthy and fulfilling life. It is more than being free from illness, it is a dynamic process of change and growth [52,53]. |
| WELL-BEING | Positive outcome that is meaningful for people and for many sectors of society, it states that people perceive that their lives are going well [54]. |
| HEALTH | State of complete physical, mental and social well-being and not merely the absence of disease or infirmity [55]. |
| PREVENTION | Efforts aimed at avoiding a clinical event/disease [16]. - secondary prevention: efforts aimed at preventing the recurrence of clinical events in patients who have manifest clinical disease. - primary prevention: efforts focus on preventing the first occurrence of a clinical event among individuals who are at risk. - primordial prevention: to prevent the development of risk factors in the first place. |
| LIFESTYLE | Set of habits and customs that is influenced by the life-long process of socialization, including social use of substances such as alcohol and tobacco, dietary habits, and exercise, all of which have important implications for health [56]. |
| SEDENTARINESS | Activities which typically are in the energy expenditure range of 1.0–1.5 METs, such as sitting during commuting, in the workplace, in the domestic environment, and during leisure time [57]. |
| PHYSICAL ACTIVITY | Any bodily movement produced by skeletal muscles that results in energy expenditure [58]. |
| EXERCISE | Subset of physical activity that is planned, structured, and repetitive and has as a final or an intermediate objective the improvement or maintenance of physical fitness [58]. |
| PHYSICAL FITNESS | Set of attributes that are either health- or skill-related that people have or achieve. It is a multidimensional concept. The health-related components of physical fitness are: cardiorespiratory endurance, muscular endurance and strength, body composition and flexibility [58]. |
| SPORT | An activity involving physical exertion and skill in which an individual or team competes against another or others for entertainment [59]. |
| AEROBIC ACTIVITY | Ahysical exercise that depends primarily on the aerobic energy-generating process, it may be of low to high intensity depending on subject’s fitness level [60]. |
| Educating the patient | Informing the patient about the importance of lifestyle in determining cardiometabolic/oncologic risk, discussing personal risk and personal lifestyle assessment [86,87] as described by metrics derived from clinical examination, blood and instrumental tests, and ad hoc questionnaire. |
| Determining an alliance with the patients and enhancing Self Efficacy | Clarifying physician’s and patient’s role and responsibilities, and fostering patient’s proactive role in changing behavior giving special attention to personal strength. |
| Realistic goal setting | Determining priorities for behavior’s improvements based on medical requirements and personal preferences. |
| Motivating patients | Helping patients to find personal resources in order to transform generic and vague thinking into realistic, precisely defined goals so that the change in behavior could be the consequence of patient’s will and not of physician’s imposition. |
| Self-monitoring | Nutrition diary, sedentariness and physical activity monitoring before and during treatment. |
| Problem solving | Helping patients to identify possible barriers to improve lifestyle, brainstorming solutions with their pros and cons, and drawing a realistic action plan. |
| Feedback and reinforcement | Discussing positive and negative results at subsequent follow ups, helping patients to discover new strategies and resources and furthering transformation with deep education in order to continuously improve lifestyle. |
| Self-Efficacy | Considers that an individual’s belief that he/she has the capabilities to produce an effect or reach a certain goal is a major determinant of behavioral change. |
| Transtheoretical Model [89] (also referred to as the ‘Stages of Change’ model) | Suggests to tailor the intervention to individual stage of change: precontemplation (the subject is unaware of the problem and he/she is not even considering changing), contemplation (the subject is aware of the problem and he/she is ambivalent about changing), preparation (the subject intends to take action and is prepared to experiment with small changes), action (the subject takes definitive action to change), maintenance and relapse prevention (the subject works to sustain the behavior change over the long term). |
| Social Cognitive Theory [90] | Focuses on the role of observing and learning from others, and on positive and negative reinforcement of behavior. |
| Theory of Planned Behavior [91] | Assumes that people’s behavior is determined by intention, and is predicted by attitudes, subjective norms (beliefs about whether other people approve or disapprove), and perceived behavioral control (beliefs about whether it is easy or difficult to do). |
| Self Determination Theory [92] | Combining skill development with underlying, intrinsic motivation and reason, is believed essential for lasting change. Intrinsic motivation does not rely on external pressure (for instance rewards or punishment from other people, but it exists within the individual, and is driven by interest or enjoyment in the task itself. People need to feel a sense of choice and responsibility for their actions, to feel capable of achieving the goal and also understood, cared for, and valued by others. |
| Intensity | |||||||
|---|---|---|---|---|---|---|---|
| Effort | Light | Light | Moderate | Hard | Very Hard | Maximal | |
| RELATIVE INTENSITY | VO2max (%) HRR * (%) | <25 | 25–44 | 45–59 | 60–84 | ≥85 | 100 |
| Maximal HR (%) | <30 | 30–49 | 50–69 | 70–89 | ≥90 | 100 | |
| RPE | <9 | 9–10 | 11–12 | 13–16 | >16 | 20 | |
| ABSOLUTE INTENSITY | INTENSITY | Sedentary ** | Light | Moderate | Vigorous | ||
| METs | 1–1.5 | 1.6–2.9 | 3.0–5.9 | 6–9 | ≥9 | ||
| Empirical tools |
|
|
|
|
|
| |
| Examples |
|
|
|
|
| ||
| Training zone *** | Aerobic | Aerobic | Aerobic | Aerobic + Lactate | Aerobic + Lactate + Anaerobic | Anaerobic | |
| 1ST VISIT ACTIONS | Itemized AIMS |
|---|---|
| Welcome |
|
| Clinical history and clinical assessment |
|
| Explanation of diagnosis and of specific benefits derived from lifestyle change |
|
| Setting of specific individual goals |
|
| Education about physical activity and tailored exercise prescription |
|
| FOLLOW UP VISITS ACTIONS | Itemized AIMS |
| Welcome |
|
| Clinical history (from previous encounter to present) and clinical assessment |
|
| Analysis of results and of encountered barriers |
|
| Problem solving |
|
| Setting of further specific individual goals |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucini, D.; Pagani, M. Exercise Prescription to Foster Health and Well-Being: A Behavioral Approach to Transform Barriers into Opportunities. Int. J. Environ. Res. Public Health 2021, 18, 968. https://doi.org/10.3390/ijerph18030968
Lucini D, Pagani M. Exercise Prescription to Foster Health and Well-Being: A Behavioral Approach to Transform Barriers into Opportunities. International Journal of Environmental Research and Public Health. 2021; 18(3):968. https://doi.org/10.3390/ijerph18030968
Chicago/Turabian StyleLucini, Daniela, and Massimo Pagani. 2021. "Exercise Prescription to Foster Health and Well-Being: A Behavioral Approach to Transform Barriers into Opportunities" International Journal of Environmental Research and Public Health 18, no. 3: 968. https://doi.org/10.3390/ijerph18030968