Characterization of Copy-Number Variations and Possible Candidate Genes in Recurrent Pregnancy Losses


Abstract
:1. Introduction
2. Materials and Methods
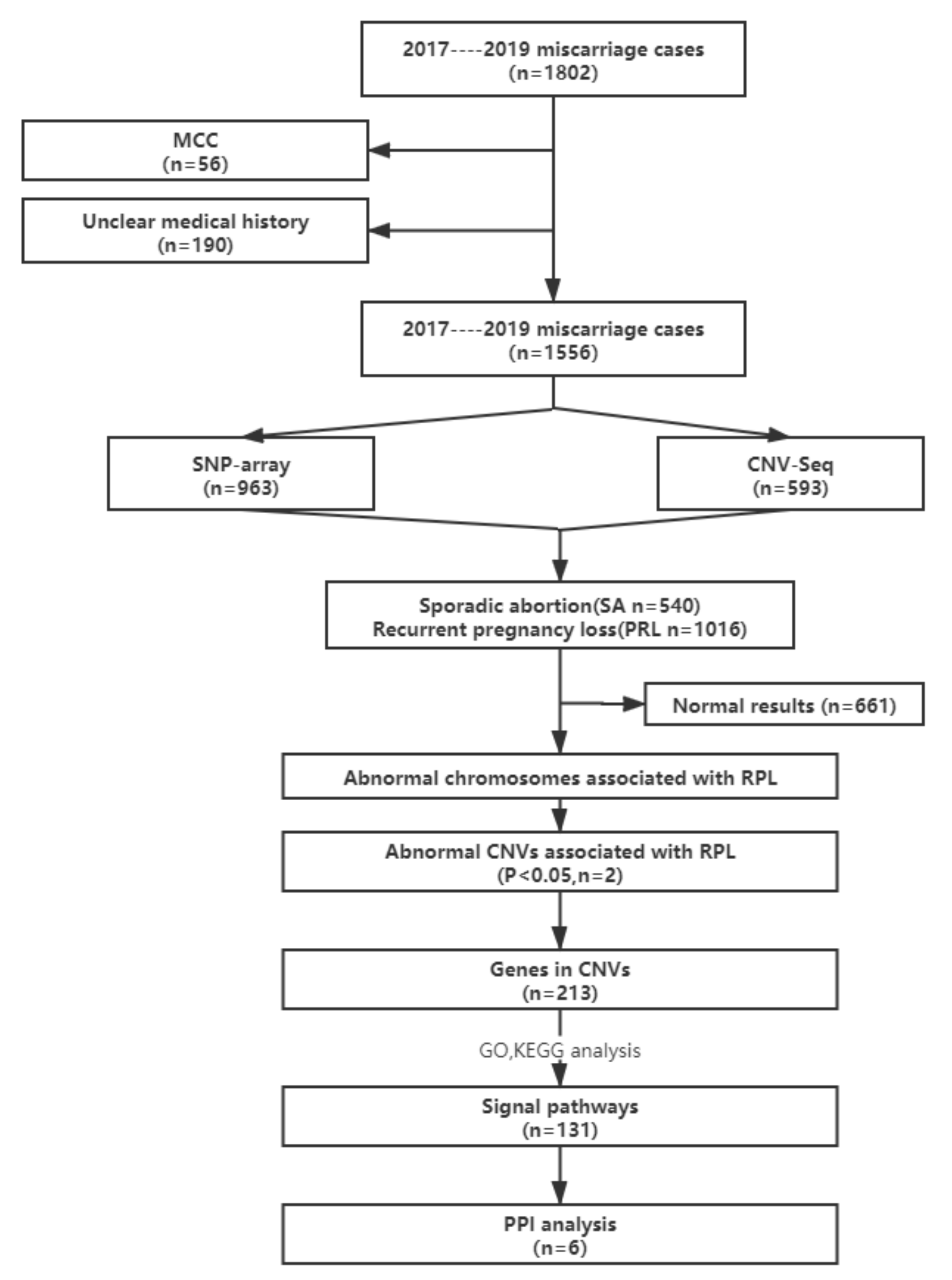
2.1. Study Subjects
2.2. SNP-Array Analysis
2.3. CNV-seq
2.4. Evaluation of CNVs
2.5. Statistical Analysis
2.6. Functional Enrichment Analysis
3. Results
3.1. Specimen Characteristics
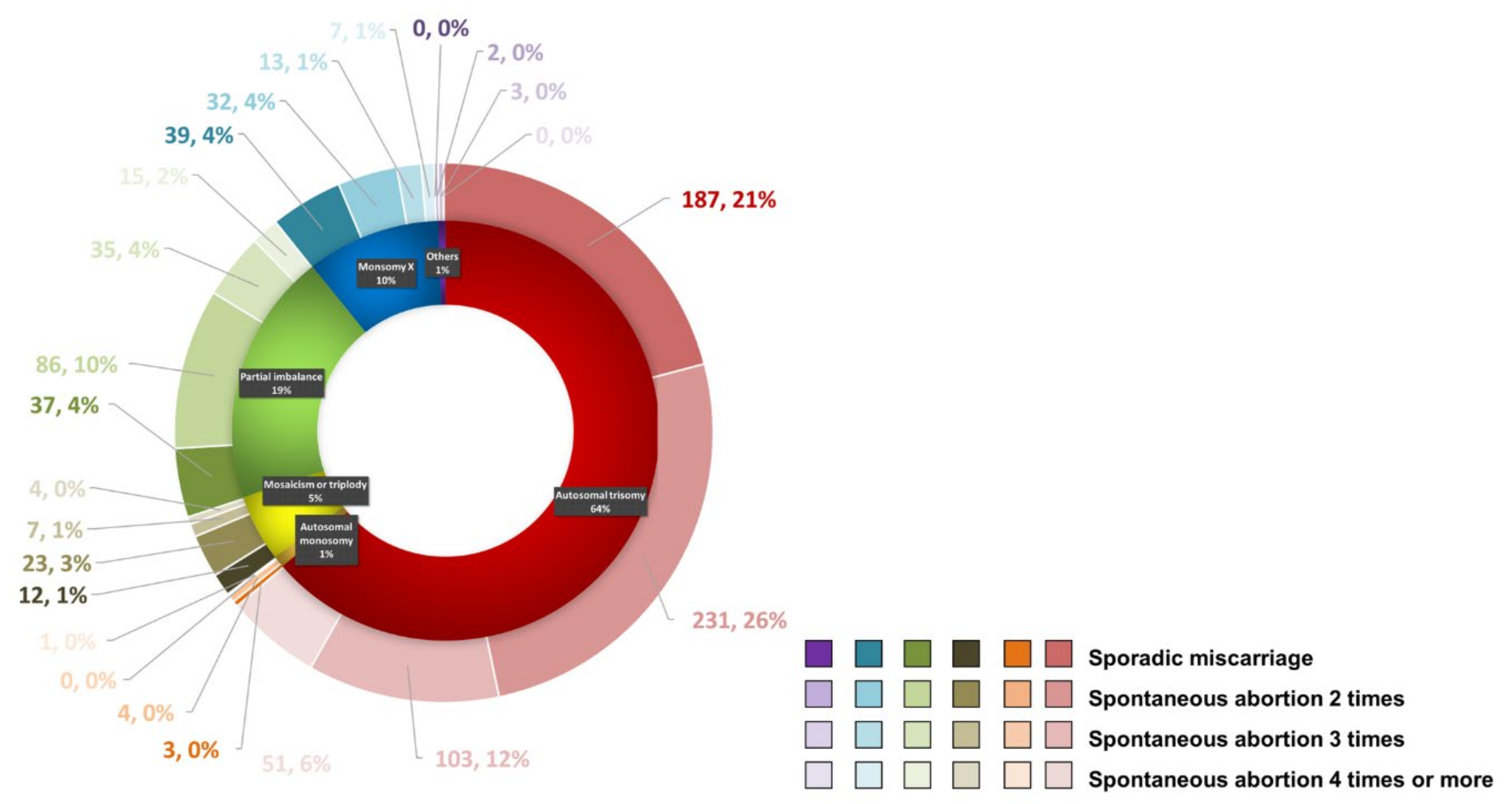
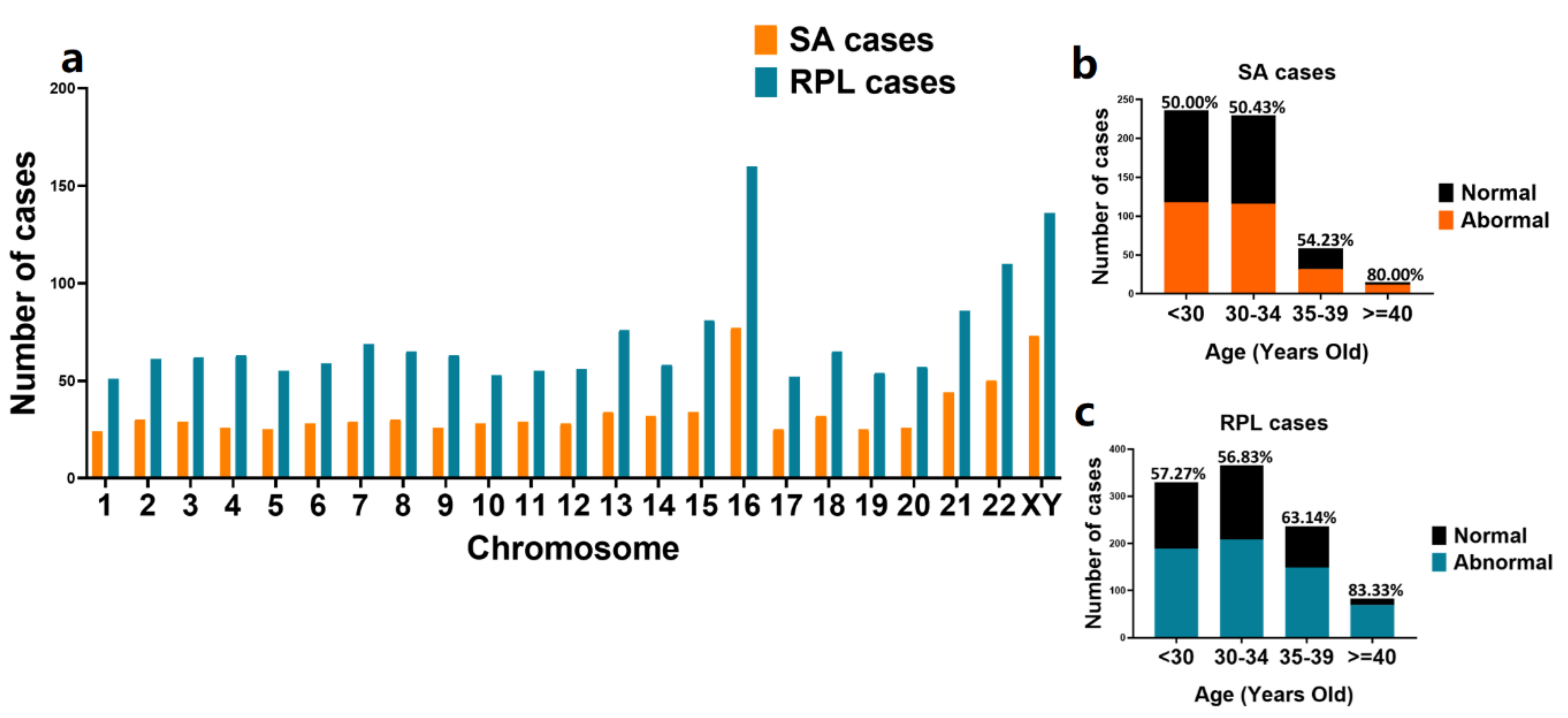
3.2. Chromosomal Abnormalities Detected by Chromosomal Microarray Analysis and CNV-seq
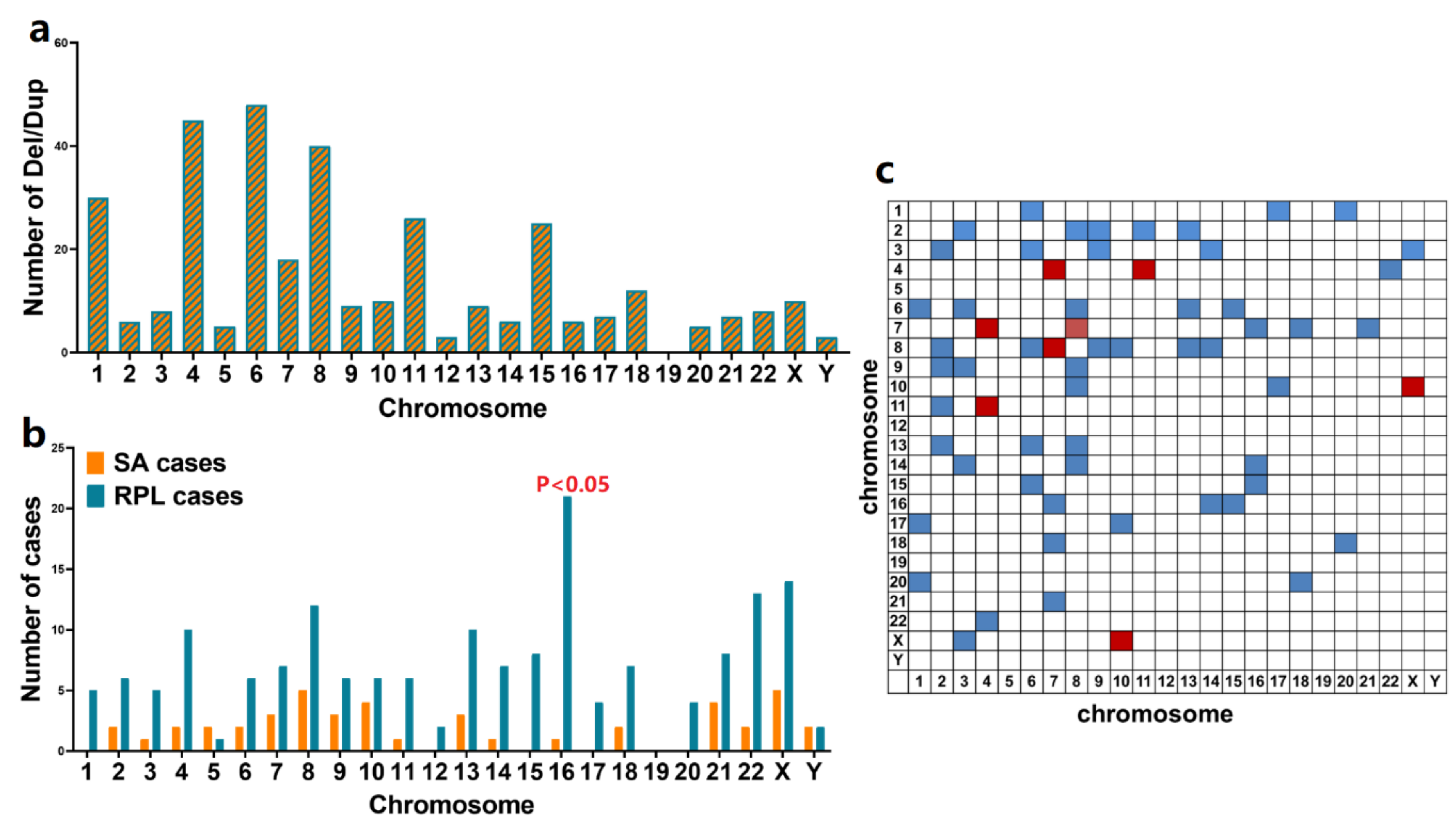
3.3. Identification of Recurrent CNVs Associated with RPL
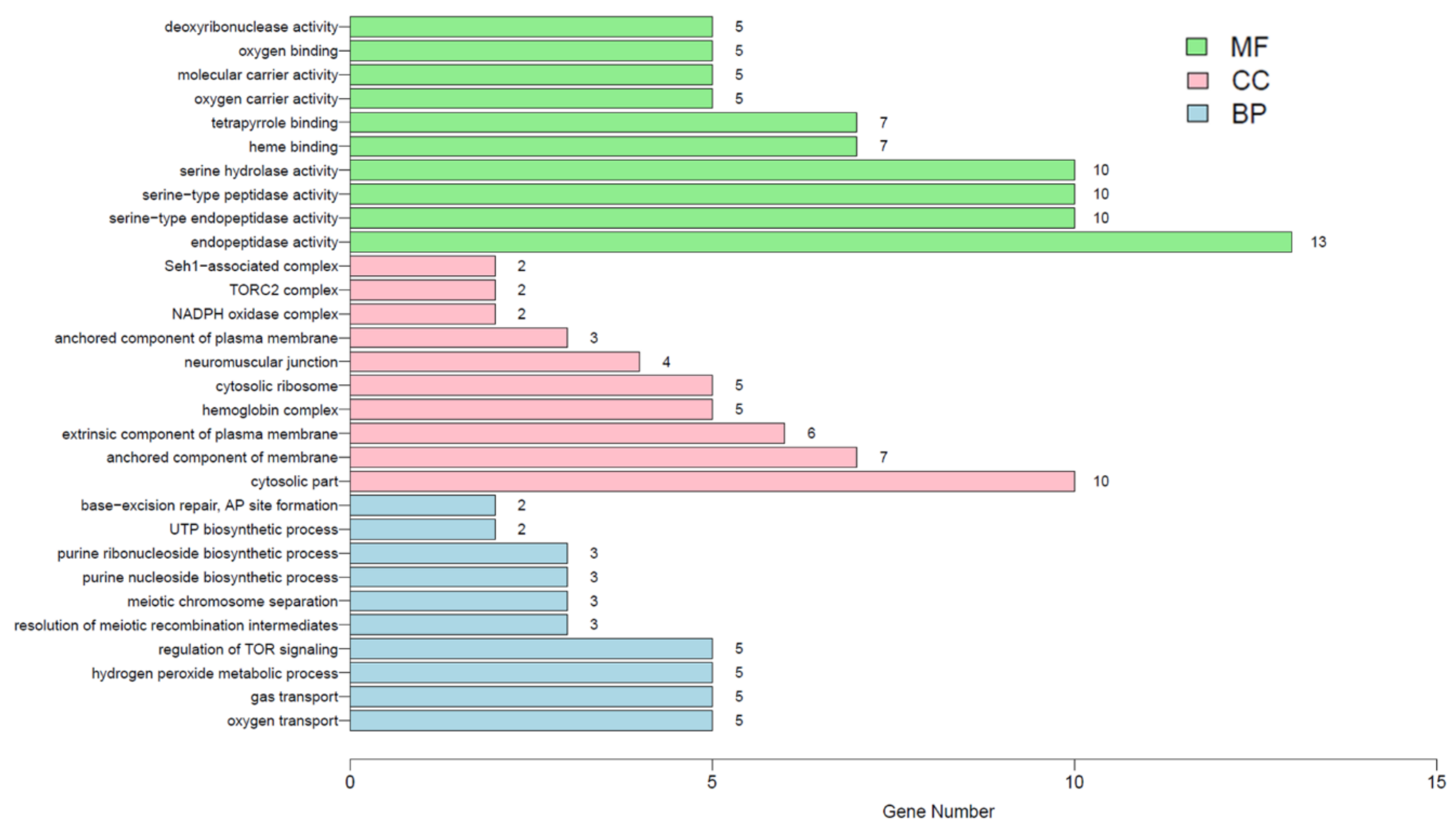
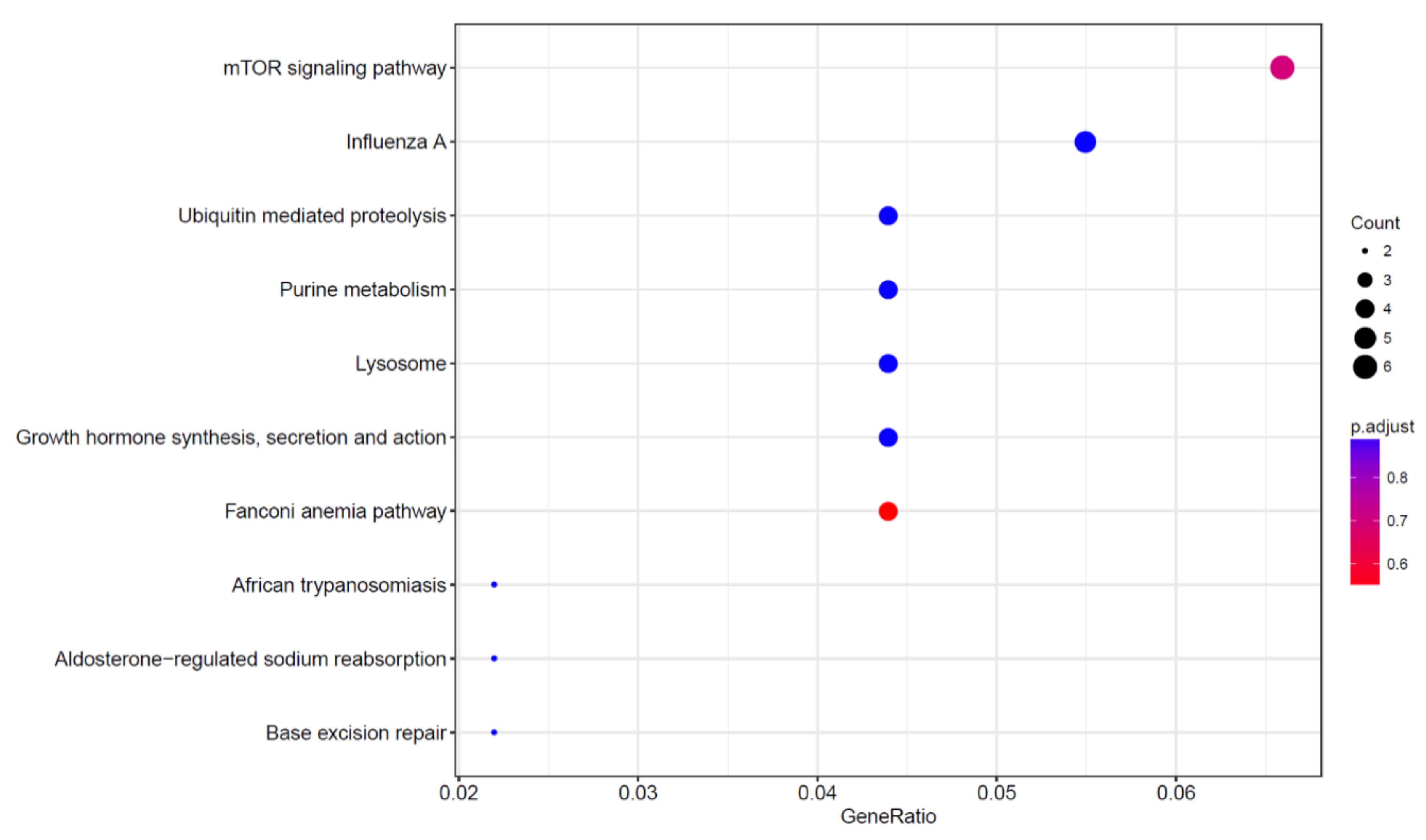
3.4. Identification of RPL Candidate Signaling Pathways and Genes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Colley, E.; Hamilton, S.; Smith, P.; Morgan, N.V.; Coomarasamy, A.; Allen, S. Potential genetic causes of miscarriage in euploid pregnancies: A systematic review. Hum. Reprod. Update 2019, 25, 452–472. [Google Scholar] [CrossRef]
- The ESHRE Guideline Group on RPL; Bender Atik, R.; Christiansen, O.B.; Elson, J.; Kolte, A.M.; Lewis, S.; Middeldorp, S.; Nelen, W.; Peramo, B.; Quenby, S.; et al. ESHRE guideline: Recurrent pregnancy loss. Hum. Reprod. Open 2018, 2018, hoy004. [Google Scholar]
- Coomarasamy, A.; Williams, H.; Truchanowicz, E.; Seed, P.T.; Small, R.; Quenby, S.; Gupta, P.; Dawood, F.; Koot, Y.E.; Atik, R.B.; et al. PROMISE: First-trimester progesterone therapy in women with a history of unexplained recurrent miscarriages a randomised, double-blind, placebo-controlled, international multicentre trial and economic evaluation. Health Technol. Assess. 2016, 20, 1–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmark Roepke, E.; Matthiesen, L.; Rylance, R.; Christiansen, O.B. Is the incidence of recurrent pregnancy loss increasing? A retrospective register-based study in Sweden. Acta. Obstet. Gynecol. Scand. 2017, 96, 1365–1372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deshmukh, H.; Way, S.S. Immunological Basis for Recurrent Fetal Loss and Pregnancy Complications. Annu. Rev. Pathol. 2019, 14, 185–210. [Google Scholar] [CrossRef] [PubMed]
- Larsen, E.C.; Christiansen, O.B.; Kolte, A.M.; Macklon, N. New insights into mechanisms behind miscarriage. BMC Med. 2013, 11, 154. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Li, Y.; Chen, Y.; Zhou, R.; Sang, Z.; Meng, L.; Tan, J.; Qiao, F.; Bao, Q.; Luo, D.; et al. Systematic analysis of copy-number variations associated with early pregnancy loss. Ultrasound Obstet. Gynecol. 2020, 55, 96–104. [Google Scholar] [CrossRef] [Green Version]
- Du, Y.; Liu, X.H.; Zhu, H.C.; Wang, L.; Ning, J.Z.; Xiao, C.C. MiR-543 Promotes Proliferation and Epithelial-Mesenchymal Transition in Prostate Cancer via Targeting RKIP. Cell Physiol. Biochem. 2017, 41, 1135–1146. [Google Scholar] [CrossRef]
- Yin, A.H.; Peng, C.F.; Zhao, X.; Caughey, B.A.; Yang, J.X.; Liu, J.; Huang, W.W.; Liu, C.; Luo, D.H.; Liu, H.L.; et al. Noninvasive detection of fetal subchromosomal abnormalities by semiconductor sequencing of maternal plasma DNA. Proc. Natl. Acad. Sci. USA 2015, 112, 14670–14675. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Durbin, R. Fast and accurate short read alignment with Burrows-Wheeler transform. Bioinformatics 2009, 25, 1754–1760. [Google Scholar] [CrossRef] [Green Version]
- Olshen, A.B.; Venkatraman, E.S.; Lucito, R.; Wigler, M. Circular binary segmentation for the analysis of array-based DNA copy number data. Biostatistics 2004, 5, 557–572. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.; Yin, A.H.; Peng, C.F.; Fu, F.; Yang, J.X.; Li, R.; Chen, Y.Y.; Luo, D.H.; Zhang, Y.L.; Ou, Y.M.; et al. Noninvasive prenatal diagnosis of common aneuploidies by semiconductor sequencing. Proc. Natl. Acad. Sci. USA 2014, 111, 7415–7420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, N.; Li, L.L.; Wang, R.X.; Li, L.L.; Yue, J.M.; Liu, R.Z. Clinical and cytogenetic results of a series of amniocentesis cases from Northeast China: A report of 2500 cases. Genet. Mol. Res. 2015, 14, 15660–15667. [Google Scholar] [CrossRef] [PubMed]
- Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: A committee opinion. Fertil. Steril. 2012, 98, 1103–1111. [Google Scholar] [CrossRef]
- Jaslow, C.R.; Carney, J.L.; Kutteh, W.H. Diagnostic factors identified in 1020 women with two versus three or more recurrent pregnancy losses. Fertil. Steril. 2010, 93, 1234–1243. [Google Scholar] [CrossRef] [PubMed]
- Menasha, J.; Levy, B.; Hirschhorn, K.; Kardon, N.B. Incidence and spectrum of chromosome abnormalities in spontaneous abortions: New insights from a 12-year study. Genet. Med. 2005, 7, 251–263. [Google Scholar] [CrossRef] [Green Version]
- Breman, A.; Pursley, A.N.; Hixson, P.; Bi, W.; Ward, P.; Bacino, C.A.; Shaw, C.; Lupski, J.R.; Beaudet, A.; Patel, A. Prenatal chromosomal microarray analysis in a diagnostic laboratory; experience with >1000 cases and review of the literature. Prenat. Diagn. 2012, 32, 351–361. [Google Scholar] [CrossRef]
- Grayton, H.M.; Fernandes, C.; Rujescu, D.; Collier, D.A. Copy number variations in neurodevelopmental disorders. Prog. Neurobiol. 2012, 99, 81–91. [Google Scholar] [CrossRef]
- Dong, Z.; Zhang, J.; Hu, P.; Chen, H.; Xu, J.; Tian, Q.; Meng, L.; Ye, Y.; Wang, J.; Zhang, M.; et al. Low-pass whole-genome sequencing in clinical cytogenetics: A validated approach. Genet. Med. 2016, 18, 940–948. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.; Liu, C.; Yao, F.; Hao, N.; Zhou, J.; Zhou, Q.; Zhang, L.; Liu, X.; Bian, X.; Liu, J. Array-based comparative genomic hybridization is more informative than conventional karyotyping and fluorescence in situ hybridization in the analysis of first-trimester spontaneous abortion. Mol. Cytogenet. 2012, 5, 33. [Google Scholar] [CrossRef] [Green Version]
- Bug, S.; Solfrank, B.; Schmitz, F.; Pricelius, J.; Stecher, M.; Craig, A.; Botcherby, M.; Nevinny-Stickel-Hinzpeter, C. Diagnostic utility of novel combined arrays for genome-wide simultaneous detection of aneuploidy and uniparental isodisomy in losses of pregnancy. Mol. Cytogenet. 2014, 7, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, J.; Wu, W.; Gao, C.; Ochin, H.; Qu, D.; Xie, J.; Gao, L.; Zhou, Y.; Cui, Y.; Liu, J. Chromosomal copy number analysis on chorionic villus samples from early spontaneous miscarriages by high throughput genetic technology. Mol. Cytogenet. 2016, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Nagirnaja, L.; Palta, P.; Kasak, L.; Rull, K.; Christiansen, O.B.; Nielsen, H.S.; Steffensen, R.; Esko, T.; Remm, M.; Laan, M. Structural genomic variation as risk factor for idiopathic recurrent miscarriage. Hum. Mutat. 2014, 35, 972–982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardy, K.; Hardy, P.J. 1(st) trimester miscarriage: Four decades of study. Transl. Pediatr. 2015, 4, 189–200. [Google Scholar] [PubMed]
- Menten, B.; Swerts, K.; Delle Chiaie, B.; Janssens, S.; Buysse, K.; Philippé, J.; Speleman, F. Array comparative genomic hybridization and flow cytometry analysis of spontaneous abortions and mors in utero samples. BMC Med. Genet. 2009, 10, 89. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Bartanus, J.; Liang, D.; Zhu, H.; Breman, A.M.; Smith, J.L.; Wang, H.; Ren, Z.; Patel, A.; Stankiewicz, P. Characterization of chromosomal abnormalities in pregnancy losses reveals critical genes and loci for human early development. Hum. Mutat. 2017, 38, 669–677. [Google Scholar] [CrossRef] [PubMed]
- Yamazawa, K.; Inoue, T.; Sakemi, Y.; Nakashima, T.; Yamashita, H.; Khono, K.; Fujita, H.; Enomoto, K.; Nakabayashi, K.; Hata, K. Loss of imprinting of the human-specific imprinted gene ZNF597 causes prenatal growth retardation and dysmorphic features: Implications for phenotypic overlap with Silver-Russell syndrome. J. Med. Genet. 2020. [Google Scholar] [CrossRef]
- Pasternak, Y. The yield of chromosomal microarray testing for cases of abnormal fetal head circumference. J. Perinat. Med. 2020, 48, 553–558. [Google Scholar] [CrossRef]
- Moore, J.A.; Pullon, B.M.; Drake, K.M.; Brennan, S.O. Novel α(0)-Thalassemia Deletion Identified in an Indian Infant with Hb H Disease. Hemoglobin 2020, 44, 297–301. [Google Scholar] [CrossRef]
- Handrigan, G.R.; Chitayat, D.; Lionel, A.C.; Pinsk, M.; Vaags, A.K.; Marshall, C.R.; Dyack, S.; Escobar, L.F.; Fernandez, B.A.; Stegman, J.C.; et al. Deletions in 16q24.2 are associated with autism spectrum disorder, intellectual disability and congenital renal malformation. J. Med. Genet. 2013, 50, 163–173. [Google Scholar]
- Redaelli, S.; Maitz, S.; Crosti, F.; Sala, E.; Villa, N.; Spaccini, L.; Selicorni, A.; Rigoldi, M.; Conconi, D.; Dalprà, L. Refining the Phenotype of Recurrent Rearrangements of Chromosome 16. Int. J. Mol. Sci. 2019, 20, 1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, J.; Han, C.; Gordon, L.A.; Terry, A.; Prabhakar, S.; She, X.; Xie, G.; Hellsten, U.; Chan, Y.M.; Altherr, M. The sequence and analysis of duplication-rich human chromosome 16. Nature 2004, 432, 988–994. [Google Scholar] [CrossRef]
- Sayed, I.S.M.; Abdel-Hamid, M.S.; Abdel-Salam, G.M.H. KBG syndrome in two patients from Egypt. Am. J. Med. Genet. 2020, 182, 1309–1312. [Google Scholar] [CrossRef] [PubMed]
- Morel Swols, D.; Foster II, J.; Tekin, M. KBG syndrome. Orphanet, J. Rare Dis. 2017, 12, 183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wintergerst, L.; Selmansberger, M.; Maihoefer, C.; Schüttrumpf, L.; Walch, A.; Wilke, C.; Pitea, A.; Woischke, C.; Baumeister, P.; Kirchner, T.; et al. A prognostic mRNA expression signature of four 16q24.3 genes in radio(chemo)therapy-treated head and neck squamous cell carcinoma (HNSCC). Mol. Oncol. 2018, 12, 2085–2101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.; Oh, J.Y.; Sung, Y.A.; Chung, H.; Kim, H.L.; Kim, G.S.; Cho, Y.S.; Kim, J.T. Genome-wide association study identified new susceptibility loci for polycystic ovary syndrome. Hum. Reprod. 2015, 30, 723–731. [Google Scholar] [CrossRef]
- Henrichsen, C.N.; Vinckenbosch, N.; Zöllner, S.; Chaignat, E.; Pradervand, S.; Schütz, F.; Ruedi, M.; Kaessmann, H.; Reymond, A. Segmental copy number variation shapes tissue transcriptomes. Nat. Genet. 2009, 41, 424–429. [Google Scholar] [CrossRef]
- Jayasena, C.N.; Radia, U.K.; Figueiredo, M.; Revill, L.F.; Dimakopoulou, A.; Osagie, M.; Vessey, W.; Regan, L.; Rai, R.; Dhillo, W.S. Reduced Testicular Steroidogenesis and Increased Semen Oxidative Stress in Male Partners as Novel Markers of Recurrent Miscarriage. Clin. Chem. 2019, 65, 161–169. [Google Scholar] [CrossRef] [Green Version]
- Homa, S.T.; Vassiliou, A.M.; Stone, J.; Killeen, A.P.; Dawkins, A.; Xie, J.; Gould, F.; Ramsay, J.W.A. A Comparison Between Two Assays for Measuring Seminal Oxidative Stress and their Relationship with Sperm DNA Fragmentation and Semen Parameters. Genes 2019, 10, 2236. [Google Scholar] [CrossRef] [Green Version]
- van Dijk, M.M.; Kolte, A.M.; Limpens, J.; Kirk, E.; Quenby, S.; van Wely, M.; Goddijn, M. Recurrent pregnancy loss: Diagnostic workup after two or three pregnancy losses? A systematic review of the literature and meta-analysis. Hum. Reprod. Update 2020, 26, 356–367. [Google Scholar] [CrossRef] [Green Version]
- Rostamzadeh, D.; Yousefi, M.; Haghshenas, M.R.; Ahmadi, M.; Dolati, S.; Babaloo, Z. mTOR Signaling pathway as a master regulator of memory CD8(+) T-cells, Th17, and NK cells development and their functional properties. J. Cell Physiol. 2019, 234, 12353–12368. [Google Scholar] [CrossRef] [PubMed]
- Muyayalo, K.P.; Li, Z.H.; Mor, G.; Liao, A.H. Modulatory effect of intravenous immunoglobulin on Th17/Treg cell balance in women with unexplained recurrent spontaneous abortion. Am. J. Reprod. Immunol 2018, 80, e13018. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Zhang, N.; Lin, J.; Wang, C.; Pan, X.; Chen, L.; Li, D.; Wang, L. Distinct pattern of Th17/Treg cells in pregnant women with a history of unexplained recurrent spontaneous abortion. Biosci. Trends 2018, 12, 157–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Cheng, L.; Deng, X.; Yu, H.; Chao, L. Expression of GRIM-19 in unexplained recurrent spontaneous abortion and possible pathogenesis. Mol. Hum. Reprod. 2018, 24, 366–374. [Google Scholar] [CrossRef] [PubMed]
- D’Ippolito, S.; Tersigni, C.; Marana, R.; Di Nicuolo, F.; Gaglione, R.; Rossi, E.D.; Castellani, R.; Scambia, G.; Di Simone, N. Inflammosome in the human endometrium: Further step in the evaluation of the “maternal side”. Fertil. Steril. 2016, 105, 111–118.e1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roomandeh, N.; Saremi, A.; Arasteh, J.; Pak, F.; Mirmohammadkhani, M.; Kokhaei, P.; Zare, A. Comparing Serum Levels of Th17 and Treg Cytokines in Women with Unexplained Recurrent Spontaneous Abortion and Fertile Women. Iran. J. Immunol. 2018, 15, 59–67. [Google Scholar] [PubMed]
- Saifi, B.; Aflatoonian, R.; Tajik, N.; Erfanian Ahmadpour, M.; Vakili, R.; Amjadi, F.; Valizade, N.; Ahmadi, S.; Rezaee, S.A.; Mehdizadeh, M. T regulatory markers expression in unexplained recurrent spontaneous abortion. J. Matern. Fetal. Neonatal. Med. 2016, 29, 1175–1180. [Google Scholar] [CrossRef]
- Saifi, B.; Rezaee, S.A.; Tajik, N.; Ahmadpour, M.E.; Ashrafi, M.; Vakili, R.; SoleimaniAsl, S.; Aflatoonian, R.; Mehdizadeh, M. Th17 cells and related cytokines in unexplained recurrent spontaneous miscarriage at the implantation window. Reprod. Biomed. Online 2014, 29, 481–489. [Google Scholar] [CrossRef] [Green Version]
- Sato, T.; Migita, O.; Hata, H.; Okamoto, A.; Hata, K. Analysis of chromosome microstructures in products of conception associated with recurrent miscarriage. Reprod. Biomed. Online 2019, 38, 787–795. [Google Scholar] [CrossRef]
- Rull, K.; Laan, M. Expression of β-subunit of HCG genes during normal and failed pregnancy. Hum. Reprod. 2005, 20, 3360–3368. [Google Scholar] [CrossRef]
- Rull, K.; Christiansen, O.B.; Nagirnaja, L.; Steffensen, R.; Margus, T.; Laan, M. A modest but significant effect of CGB5 gene promoter polymorphisms in modulating the risk of recurrent miscarriage. Fertil. Steril. 2013, 99, 1930–1936.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Times of Miscarriage | n | Frequency (%) | Age (Years old) | Normal | Abnormal | ||
|---|---|---|---|---|---|---|---|
| n | Frequency (%) | n | Frequency (%) | ||||
| 1 | 540 | 34.70 | 30.47 (range, 21–46) | 262 | 16.84 | 278 | 17.87 |
| 2 | 586 | 37.66 | 31.63 (range, 21–45) | 208 | 13.37 | 378 | 24.29 |
| 3 | 283 | 18.18 | 32.43 (range, 22–44) | 122 | 7.84 | 161 | 10.35 |
| >=4 | 147 | 9.45 | 33.95 (range, 24–48) | 69 | 4.43 | 78 | 5.01 |
| Total | 1556 | 100 | _ | 661 | 42.48 | 895 | 57.52 |
| Chromosomal Abnormality | Autosomal Trisomy | Autosomal Monosomy | Mosaicism or Triploidy | Partial Imbalance | Monosomy X | Other | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Times of Misscariage | n | Frequency (%) | n | Frequency (%) | n | Frequency (%) | n | Frequency (%) | n | Frequency (%) | n | Frequency (%) | |
| 1 (n = 278.31%) | 187 | 21 | 3 | 0 | 12 | 1 | 37 | 4 | 39 | 4 | 0 | 0 | |
| 2 (n = 378.42%) | 231 | 26 | 4 | 0 | 23 | 3 | 86 | 10 | 32 | 4 | 2 | 0 | |
| 3 (n = 161.18%) | 103 | 12 | 0 | 0 | 7 | 1 | 35 | 4 | 13 | 1 | 3 | 0 | |
| >=4 (n = 78.9%) | 51 | 5 | 1 | 0 | 4 | 0 | 15 | 2 | 7 | 1 | 0 | 0 | |
| Total (n = 895) | 572 | 64 | 8 | 1 | 46 | 5 | 173 | 19 | 91 | 10 | 5 | 1 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sheng, Y.-R.; Hou, S.-Y.; Hu, W.-T.; Wei, C.-Y.; Liu, Y.-K.; Liu, Y.-Y.; Jiang, L.; Xiang, J.-J.; Sun, X.-X.; Lei, C.-X.; et al. Characterization of Copy-Number Variations and Possible Candidate Genes in Recurrent Pregnancy Losses. Genes 2021, 12, 141. https://doi.org/10.3390/genes12020141
Sheng Y-R, Hou S-Y, Hu W-T, Wei C-Y, Liu Y-K, Liu Y-Y, Jiang L, Xiang J-J, Sun X-X, Lei C-X, et al. Characterization of Copy-Number Variations and Possible Candidate Genes in Recurrent Pregnancy Losses. Genes. 2021; 12(2):141. https://doi.org/10.3390/genes12020141
Chicago/Turabian StyleSheng, Yan-Ran, Shun-Yu Hou, Wen-Ting Hu, Chun-Yan Wei, Yu-Kai Liu, Yu-Yin Liu, Lu Jiang, Jing-Jing Xiang, Xiao-Xi Sun, Cai-Xia Lei, and et al. 2021. "Characterization of Copy-Number Variations and Possible Candidate Genes in Recurrent Pregnancy Losses" Genes 12, no. 2: 141. https://doi.org/10.3390/genes12020141