
Does Vancomycin Resistance Increase Mortality? Clinical Outcomes and Predictive Factors for Mortality in Patients with Enterococcus faecium Infections

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Clinical Outcomes in Patients with VR-E. faecium and VS-E. faecium Infection
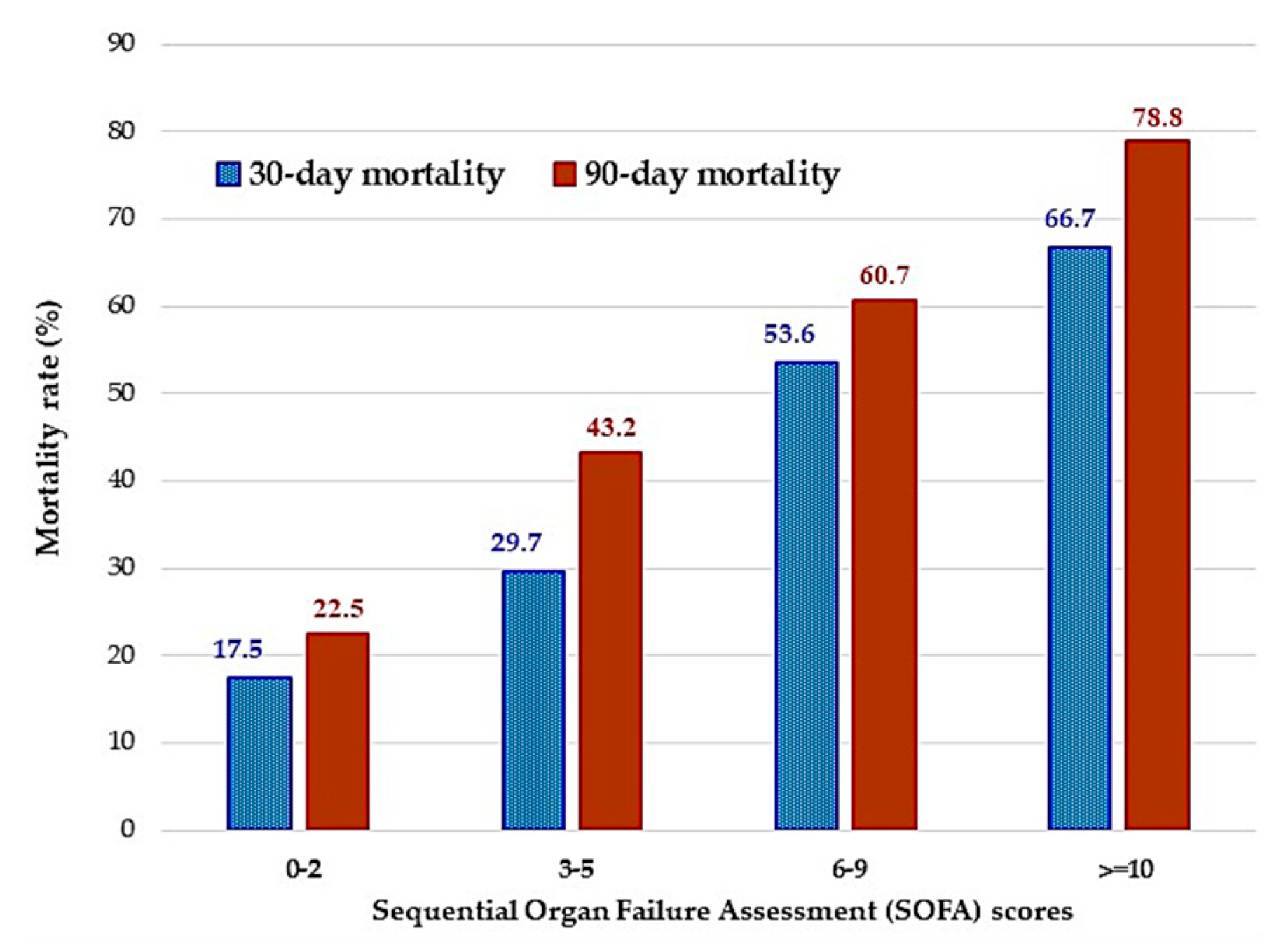
2.2. Risk Factors for 30-Day and 90-Day Mortality
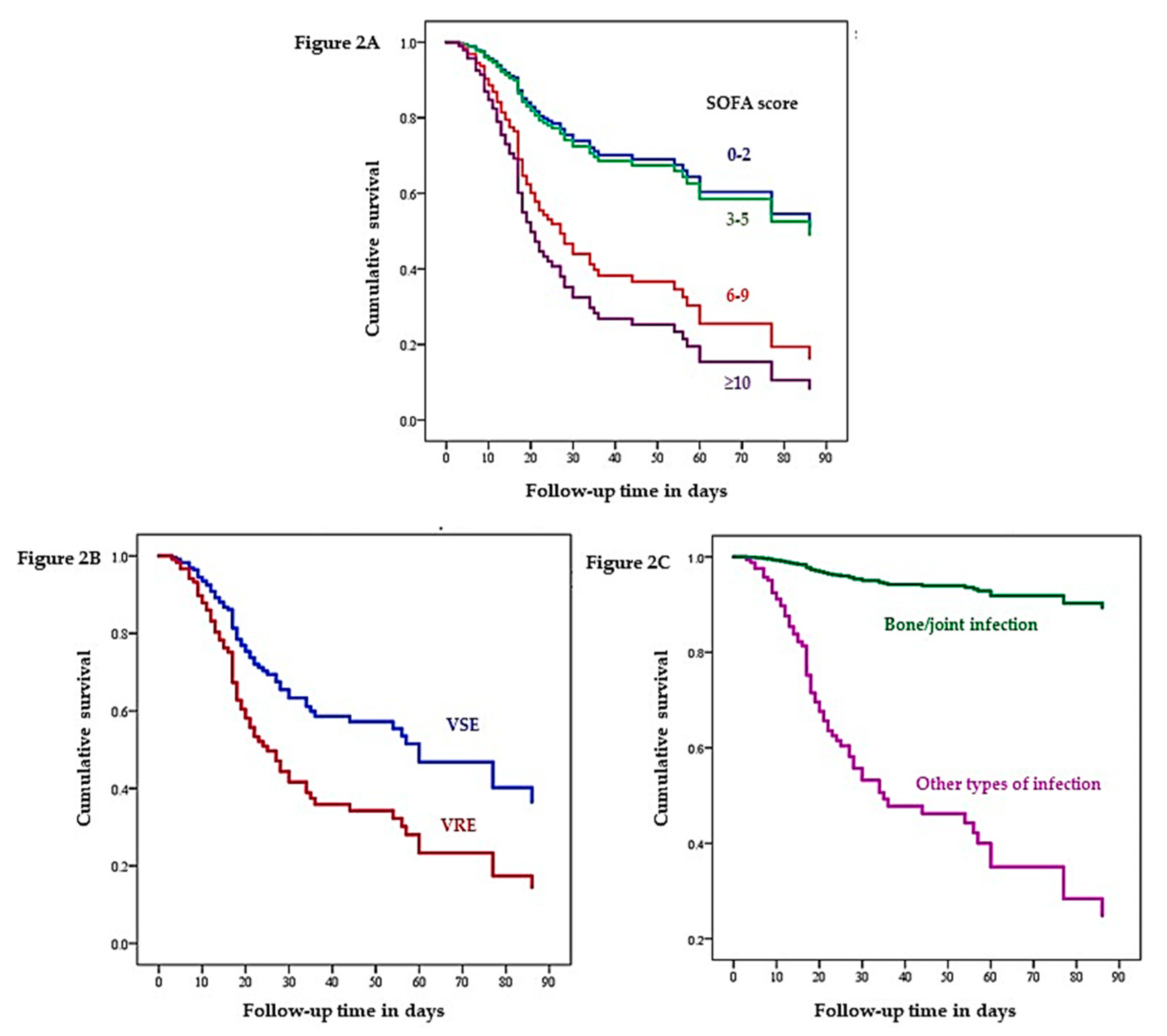
2.3. Cox Proportional Hazard Regression Analysis of 90-Day Survival
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Participants
4.3. Data Collection
4.4. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Faron, M.L.; Ledeboer, N.A.; Buchan, B.W. Resistance Mechanisms, Epidemiology, and Approaches to Screening for Vancomycin-Resistant Enterococcus in the Health Care Setting. J. Clin. Microbiol. 2016, 54, 2436–2447. [Google Scholar] [CrossRef] [Green Version]
- Reyes, K.; Bardossy, A.C.; Zervos, M. Vancomycin-Resistant Enterococci: Epidemiology, Infection Prevention, and Control. Infect. Dis. Clin. North. Am. 2016, 30, 953–965. [Google Scholar] [CrossRef]
- Gorrie, C.; Higgs, C.; Carter, G.; Stinear, T.P.; Howden, B. Genomics of vancomycin-resistant Enterococcus faecium. Microb. Genom. 2019, 5, e000283. [Google Scholar] [CrossRef]
- Hidron, A.I.; Edwards, J.R.; Patel, J.; Horan, T.C.; Sievert, D.M.; Pollock, D.A.; Fridkin, S.K. National Healthcare Safety Network, T.; Participating National Healthcare Safety Network, F., NHSN annual update: Antimicrobial-resistant pathogens associated with healthcare-associated infections: Annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006–2007. Infect. Control. Hosp. Epidemiol. 2008, 29, 996–1011. [Google Scholar]
- Sievert, D.M.; Ricks, P.; Edwards, J.R.; Schneider, A.; Patel, J.; Srinivasan, A.; Kallen, A.; Limbago, B.; Fridkin, S.; National Healthcare Safety Network (NHSN) Team; et al. Antimicrobial-resistant pathogens associated with healthcare-associated infections: Summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010. Infect. Control Hosp. Epidemiol. 2013, 34, 1–14. [Google Scholar] [CrossRef]
- The National Antimicrobial Resistant Surveillance Thailand. Antibiogram. Available online: http://narst.dmsc.moph.go.th/ (accessed on 10 April 2020).
- Camins, B.C.; Farley, M.M.; Jernigan, J.J.; Ray, S.M.; Steinberg, J.P.; Blumberg, H.M. A population-based investigation of invasive vancomycin-resistant Enterococcus infection in metropolitan Atlanta, Georgia, and predictors of mortality. Infect. Control Hosp. Epidemiol. 2007, 28, 983–991. [Google Scholar] [CrossRef]
- Han, S.H.; Chin, B.S.; Lee, H.S.; Jeong, S.J.; Choi, H.K.; Kim, C.O.; Yong, D.; Choi, J.Y.; Song, Y.G.; Lee, K.; et al. Vancomycin-resistant enterococci bacteremia: Risk factors for mortality and influence of antimicrobial therapy on clinical outcome. J. Infect. 2009, 58, 182–190. [Google Scholar] [CrossRef]
- Britt, N.S.; Potter, E.M.; Patel, N.; Steed, M.E. Comparison of the Effectiveness and Safety of Linezolid and Daptomycin in Vancomycin-Resistant Enterococcal Bloodstream Infection: A National Cohort Study of Veterans Affairs Patients. Clin. Infect. Dis. 2015, 61, 871–878. [Google Scholar] [CrossRef] [Green Version]
- Ye, J.J.; Shie, S.S.; Cheng, C.W.; Yang, J.H.; Huang, P.Y.; Wu, T.S.; Lee, M.H.; Huang, C.T. Clinical characteristics and treatment outcomes of vancomycin-resistant Enterococcus faecium bacteremia. J. Microbiol. Immunol. Infect. Wei Mian Yu Gan Ran Za Zhi 2018, 51, 705–716. [Google Scholar] [CrossRef]
- Garbutt, J.M.; Ventrapragada, M.; Littenberg, B.; Mundy, L.M. Association between resistance to vancomycin and death in cases of Enterococcus faecium bacteremia. Clin. Infect. Dis. 2000, 30, 466–472. [Google Scholar] [CrossRef]
- Butler, A.M.; Olsen, M.A.; Merz, L.R.; Guth, R.M.; Woeltje, K.F.; Camins, B.C.; Fraser, V.J. Attributable costs of enterococcal bloodstream infections in a nonsurgical hospital cohort. Infect. Control Hosp. Epidemiol. 2010, 31, 28–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheah, A.L.; Spelman, T.; Liew, D.; Peel, T.; Howden, B.P.; Spelman, D.; Grayson, M.L.; Nation, R.L.; Kong, D.C. Enterococcal bacteraemia: Factors influencing mortality, length of stay and costs of hospitalization. Clin. Microbiol. Infect. 2013, 19, E181–E189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, H.-L.; Zhou, Z.; Wang, L.-S.; Fang, Y.; Li, Y.-H.; Chu, C.-I. The Risk Factors, Costs, and Survival Analysis of Invasive VRE Infections at a Medical Center in Eastern Taiwan. Int. J. Infect. Dis. 2017, 54, 18–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gearhart, M.; Martin, J.; Rudich, S.; Thomas, M.; Wetzel, D.; Solomkin, J.; Hanaway, M.J.; Aranda-Michel, J.; Weber, F.; Trumball, L.; et al. Consequences of vancomycin-resistant Enterococcus in liver transplant recipients: A matched control study. Clin. Transplant. 2005, 19, 711–716. [Google Scholar] [CrossRef]
- Hayakawa, K.; Marchaim, D.; Martin, E.T.; Tiwari, N.; Yousuf, A.; Sunkara, B.; Pulluru, H.; Kotra, H.; Hasan, A.; Bheemreddy, S.; et al. Comparison of the Clinical Characteristics and Outcomes Associated with Vancomycin-Resistant Enterococcus faecalis and Vancomycin-Resistant E. faecium Bacteremia. Antimicrob. Agents Chemother. 2012, 56, 2452. [Google Scholar] [CrossRef] [Green Version]
- DiazGranados, C.A.; Zimmer, S.M.; Klein, M.; Jernigan, J.A. Comparison of mortality associated with vancomycin-resistant and vancomycin-susceptible enterococcal bloodstream infections: A meta-analysis. Clin. Infect. Dis. 2005, 41, 327–333. [Google Scholar] [CrossRef] [Green Version]
- Lautenbach, E.; Bilker, W.B.; Brennan, P.J. Enterococcal bacteremia: Risk factors for vancomycin resistance and predictors of mortality. Infect. Control Hosp. Epidemiol. 1999, 20, 318–323. [Google Scholar] [CrossRef]
- Shay, D.K.; Maloney, S.A.; Montecalvo, M.; Banerjee, S.; Wormser, G.P.; Arduino, M.J.; Bland, L.A.; Jarvis, W.R. Epidemiology and mortality risk of vancomycin-resistant enterococcal bloodstream infections. J. Infect. Dis. 1995, 172, 993–1000. [Google Scholar] [CrossRef]
- Dubler, S.; Lenz, M.; Zimmermann, S.; Richter, D.C.; Weiss, K.H.; Mehrabi, A.; Mieth, M.; Bruckner, T.; Weigand, M.A.; Brenner, T.; et al. Does vancomycin resistance increase mortality in Enterococcus faecium bacteraemia after orthotopic liver transplantation? A retrospective study. Antimicrob. Resist. Infect. Control. 2020, 9, 22. [Google Scholar] [CrossRef]
- Kramer, T.S.; Remschmidt, C.; Werner, S.; Behnke, M.; Schwab, F.; Werner, G.; Gastmeier, P.; Leistner, R. The importance of adjusting for enterococcus species when assessing the burden of vancomycin resistance: A cohort study including over 1000 cases of enterococcal bloodstream infections. Antimicrob. Resist. Infect. Control 2018, 7, 133. [Google Scholar] [CrossRef]
- Chou, C.-H.; Lee, N.-Y.; Lee, H.-C.; Chang, C.-M.; Lee, C.-C.; Ko, W.-C. Emergence of vancomycin-resistant Enterococcus bloodstream infections in southern Taiwan. J. Microbiol. Immunol. Infect. 2012, 45, 221–227. [Google Scholar] [CrossRef] [Green Version]
- Bhavnani, S.M.; Drake, J.A.; Forrest, A.; Deinhart, J.A.; Jones, R.N.; Biedenbach, D.J.; Ballow, C.H. A nationwide, multicenter, case-control study comparing risk factors, treatment, and outcome for vancomycin-resistant and -susceptible enterococcal bacteremia. Diagn. Microbiol. Infect. Dis. 2000, 36, 145–158. [Google Scholar] [CrossRef]
- Prematunge, C.; MacDougall, C.; Johnstone, J.; Adomako, K.; Lam, F.; Robertson, J.; Garber, G. VRE and VSE Bacteremia Outcomes in the Era of Effective VRE Therapy: A Systematic Review and Meta-analysis. Infect. Control Hosp. Epidemiol. 2016, 37, 26–35. [Google Scholar] [CrossRef] [Green Version]
- Terpenning, M.S.; Zervos, M.J.; Schaberg, D.R.; Kauffman, C.A. Enterococcal infections: An increasing problem in hospitalized patients. Infect. Control Hosp. Epidemiol. 1988, 9, 457–461. [Google Scholar] [CrossRef]
- Thompson, O.; Rasmussen, M.; Stefansdottir, A.; Christensson, B.; Akesson, P. A population-based study on the treatment and outcome of enterococcal prosthetic joint infections. A consecutive series of 55 cases. J. Bone Jt. Infect. 2019, 4, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Fischbacher, A.; Borens, O. Prosthetic-joint Infections: Mortality Over the Last 10 Years. J. Bone Jt. Infect. 2019, 4, 198–202. [Google Scholar] [CrossRef] [Green Version]
- Hemapanpairoa, J.; Changpradub, D.; Thunyaharn, S.; Santimaleeworagun, W. Vancomycin-resistant enterococcal infection in a Thai university hospital: Clinical characteristics, treatment outcomes, and synergistic effect. Infect. Drug Resist. 2019, 12, 2049–2057. [Google Scholar] [CrossRef] [Green Version]
- Chuang, Y.C.; Lin, H.Y.; Chen, P.Y.; Lin, C.Y.; Wang, J.T.; Chang, S.C. Daptomycin versus linezolid for the treatment of vancomycin-resistant enterococcal bacteraemia: Implications of daptomycin dose. Clin. Microbiol. Infect. 2016, 22, 890.e1–890.e7. [Google Scholar] [CrossRef] [Green Version]
- Zasowski, E.J.; Claeys, K.C.; Lagnf, A.M.; Davis, S.L.; Rybak, M.J. Time Is of the Essence: The Impact of Delayed Antibiotic Therapy on Patient Outcomes in Hospital-Onset Enterococcal Bloodstream Infections. Clin. Infect. Dis. 2016, 62, 1242–1250. [Google Scholar] [CrossRef] [Green Version]
- O’Driscoll, T.; Crank, C.W. Vancomycin-resistant enterococcal infections: Epidemiology, clinical manifestations, and optimal management. Infect. Drug Resist. 2015, 8, 217–230. [Google Scholar]
- Rice, L.B. Emergence of vancomycin-resistant enterococci. Emerg. Infect. Dis. 2001, 7, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Alevizakos, M.; Gaitanidis, A.; Nasioudis, D.; Tori, K.; Flokas, M.E.; Mylonakis, E. Colonization With Vancomycin-Resistant Enterococci and Risk for Bloodstream Infection Among Patients with Malignancy: A Systematic Review and Meta-Analysis. Open Forum Infect. Dis. 2017, 4, ofw246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Twenty-Ninth Informational Supplement; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2019; 149p. [Google Scholar]
- CDC 2018 NHSN Patient Safety Component. Available online: https://www.cdc.gov/nhsn/# (accessed on 17 February 2019).



{kind=link}
{kind=link}
| Demographic Data | Values | p-Value | |
|---|---|---|---|
| VR-E. faecium (n = 26) | VS-E. faecium (n = 119) | ||
| Male, n (%) | 19 (73.1) | 61 (51.3) | 0.043 |
| Age, median (IQR), y | 68.5 (57–80) | 74 (59–80) | 0.62 |
| Comorbidity, n (%) | |||
| Cardiovascular diseases | 8 (30.8) | 36 (30.3) | 0.96 |
| Cerebrovascular diseases | 3 (11.5) | 23 (19.3) | 0.57 |
| End-stage kidney disease | 10 (38.5) | 14 (11.8) | 0.002 |
| Liver disease | 6 (23.1) | 13 (10.9) | 0.11 |
| Solid cancer | 7 (26.9) | 49 (41.2) | 0.18 |
| Hematologic malignancy | 3 (11.5) | 3 (2.5) | 0.07 |
| Neutropenia | 4 (15.4) | 6 (5) | 0.08 |
| Ward, n (%) | |||
| Medical-ICU | 11 (42.3) | 32 (26.9) | 0.12 |
| Surgical-ICU | 3 (11.5) | 14 (11.8) | 1.0 |
| Medicine | 7 (26.9) | 43 (36.1) | 0.37 |
| Surgery | 5 (19.2) | 29 (24.4) | 0.58 |
| Others | 0 (0) | 1 (0.8) | 1.0 |
| SOFA score, median (IQR) | 7 (7) | 5 (7) | 0.11 |
| Mechanical ventilator, n (%) | 16 (61.5) | 55 (46.2) | 0.16 |
| E. faecium bacteremia, n (%) | 13 (50) | 50 (42) | 0.46 |
| Polymicrobials, n (%) | 16 (61.5) | 59 (49.6) | 0.27 |
| Type of infections, n (%) | |||
| Bloodstream infection | 7 (26.9) | 18 (15.1) | 0.159 |
| Cardiovascular system infection | 0 | 2 (1.7) | 1.0 |
| Intra-abdominal infection | 8 (30.8) | 38 (31.9) | 1.0 |
| Bone and joint infection | 6 (23.1) | 5 (4.2) | 0.005 |
| Skin and soft tissue infection | 2 (7.7) | 15 (12.6) | 0.539 |
| Urinary tract infection | 3 (11.5) | 39 (32.8) | 0.033 |
| Reproductive tract infection | 0 (0) | 3 (2.5) | 0.633 |
| Clinical outcomes, n (%) | |||
| In-hospital mortality | 19 (73.1) | 59 (49.6) | 0.03 |
| 30-day mortality | 15 (57.7) | 46 (38.7) | 0.075 |
| 90-day mortality | 18 (69.2) | 56 (47.1) | 0.04 |
| Length of hospitalization (day), | 69 (38–124) | 36 (24–58) | 0.001 |
| median (IQR) | |||
| Variables | Death (61 Cases) | Survivors (84 Cases) | Univariate Analysis | Multivariate Analysis † | ||
|---|---|---|---|---|---|---|
| OR | 95% CI | aOR | 95% CI | |||
| Male, n (%) | 34 (55.7) | 46 (54.8) | 1.04 | 0.54–2.02 | ||
| Age ≥ 70 years, n (%) | 41 (50.6) | 40 (49.4) | 2.26 | 1.14–4.47 | 2.05 | 0.89–4.71 |
| Comorbidity, n (%) | ||||||
| Cardiovascular diseases | 22 (36.1) | 22 (26.2) | 1.59 | 0.78–3.27 | ||
| Cerebrovascular diseases | 10 (16.4) | 16 (19) | 0.83 | 0.35–1.99 | ||
| End-stage kidney disease | 13 (21.3) | 11 (13.1) | 1.80 | 0.74–4.34 | ||
| Liver disease | 12 (19.7) | 7 (8.3) | 2.69 | 0.99–7.31 | ||
| Solid cancer | 21 (34.4) | 35 (41.7) | 0.74 | 0.37–1.46 | ||
| Hematologic malignancy | 3 (4.9) | 3 (3.6) | 1.40 | 0.27–7.17 | ||
| Neutropenia, n (%) | 6 (9.8) | 4 (4.8) | 2.18 | 0.59–8.09 | ||
| SOFA score, n (%) | ||||||
| 0–2 points | 7 (12.7) | 33 (39.8) | - | - | - | - |
| 3–5 points | 11 (20) | 26 (31.3) | 2.00 | 0.68–5.86 | 1.52 | 0.49–4.71 |
| 6–9 points | 15 (27.3) | 13 (15.7) | 5.44 | 1.81–16.39 | 4.61 | 1.43–14.87 |
| ≥10 points | 22 (40) | 11 (13.3) | 9.43 | 3.17–28.06 | 6.94 | 2.23–21.59 |
| VR-E. faecium, n (%) | 15 (24.6) | 11 (13.1) | 2.16 | 0.92–5.12 | 3.64 | 1.20–11.07 |
| Type of infections, n (%) | ||||||
| Bloodstream infection | 16 (26.2) | 9 (10.7) | 2.96 | 1.21–7.26 | ||
| Intra-abdominal infection | 22 (36.1) | 24 (28.6) | 1.41 | 0.70–2.85 | ||
| Bone and joint infection | 1 (1.6) | 10 (11.9) | 0.12 | 0.02–0.99 | 0.09 | 0.01–0.91 |
| Skin and soft tissue infection | 4 (6.6) | 13 (15.5) | 0.38 | 0.12–1.24 | ||
| Urinary tract infection | 17 (27.9) | 25 (29.8) | 0.91 | 0.44–1.89 | ||
| Variables | Death (74 Cases) | Survivors (71 Cases) | Univariate Analysis | Multivariate Analysis † | ||
|---|---|---|---|---|---|---|
| OR | 95% CI | aOR | 95% CI | |||
| Male, n (%) | 40 (54.1) | 40 (56.3) | 0.91 | 0.47–1.76 | ||
| Age ≥ 70 years, n (%) | 52 (70.3) | 29 (40.8) | 3.42 | 1.72–6.81 | 3.56 | 1.50–8.48 |
| Comorbidity, n (%) | ||||||
| Cardiovascular diseases | 26 (35.1) | 18 (25.4) | 1.6 | 0.78–3.27 | ||
| Cerebrovascular diseases | 14 (18.9) | 12 (16.9) | 1.15 | 0.49–2.69 | ||
| End-stage kidney disease | 16 (21.6) | 8 (11.3) | 2.2 | 0.87–5.45 | ||
| Liver disease | 13 (17.6) | 6 (8.5) | 2.31 | 0.83–6.46 | ||
| Solid cancer | 28 (37.8) | 28 (39.4) | 0.94 | 0.48–1.83 | ||
| Hematologic malignancy | 4 (5.4) | 2 (2.8) | 1.97 | 0.35–11.12 | ||
| Neutropenia, n (%) | 7 (9.5) | 3 (4.2) | 2.37 | 0.59–9.55 | ||
| SOFA score, n (%) | ||||||
| 0–2 points | 9 (13.2) | 31 (44.3) | - | - | - | - |
| 3–5 points | 16 (23.5) | 21 (30) | 2.62 | 0.98–7.04 | 1.89 | 0.64–5.59 |
| 6–9 points | 17 (25) | 11 (15.7) | 5.32 | 1.84–15.38 | 4.40 | 1.34–14.48 |
| ≥10 points | 26 (38.2) | 7 (10) | 12.79 | 4.19–39.09 | 9.78 | 2.93–32.70 |
| VR-E. faecium, n (%) | 18 (24.3) | 8 (11.3) | 2.53 | 1.02–6.27 | 7.35 | 1.79–30.21 |
| Type of infections, n (%) | ||||||
| Bloodstream infection | 19 (25.7) | 6 (8.5) | 3.74 | 1.40–10.3 | ||
| Intra-abdominal infection | 25 (33.8) | 21 (29.6) | 1.22 | 0.60–2.45 | ||
| Bone and joint infection | 1 (1.4) | 10 (14.1) | 0.08 | 0.01–0.67 | 0.034 | 0.02–0.49 |
| Skin and soft tissue infection | 6 (8.1) | 11 (15.5) | 0.48 | 0.17–1.38 | ||
| Urinary tract infection | 21 (28.4) | 21 (29.6) | 0.94 | 0.46–1.93 | ||
| Variable | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Age ≥ 70 years | 1.61 | 0.92–2.82 | 0.093 |
| VR-E. faecium infection | 1.91 | 1.09–3.37 | 0.024 |
| SOFA score | |||
| 0–2 | Reference | Reference | - |
| 3–5 | 1.06 | 0.47–2.52 | 0.894 |
| 6–9 | 2.69 | 1.15–6.29 | 0.022 |
| ≥10 | 3.71 | 1.70–8.13 | 0.001 |
| Bloodstream infection | 1.02 | 0.57–1.83 | 0.949 |
| Bone and joint infection | 0.08 | 0.01–0.62 | 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hemapanpairoa, J.; Changpradub, D.; Thunyaharn, S.; Santimaleeworagun, W. Does Vancomycin Resistance Increase Mortality? Clinical Outcomes and Predictive Factors for Mortality in Patients with Enterococcus faecium Infections. Antibiotics 2021, 10, 105. https://doi.org/10.3390/antibiotics10020105
Hemapanpairoa J, Changpradub D, Thunyaharn S, Santimaleeworagun W. Does Vancomycin Resistance Increase Mortality? Clinical Outcomes and Predictive Factors for Mortality in Patients with Enterococcus faecium Infections. Antibiotics. 2021; 10(2):105. https://doi.org/10.3390/antibiotics10020105
Chicago/Turabian StyleHemapanpairoa, Jatapat, Dhitiwat Changpradub, Sudaluck Thunyaharn, and Wichai Santimaleeworagun. 2021. "Does Vancomycin Resistance Increase Mortality? Clinical Outcomes and Predictive Factors for Mortality in Patients with Enterococcus faecium Infections" Antibiotics 10, no. 2: 105. https://doi.org/10.3390/antibiotics10020105