Singular Value Decomposition for Removal of Cardiac Interference from Trunk Electromyogram

 , , , , and
, , , , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
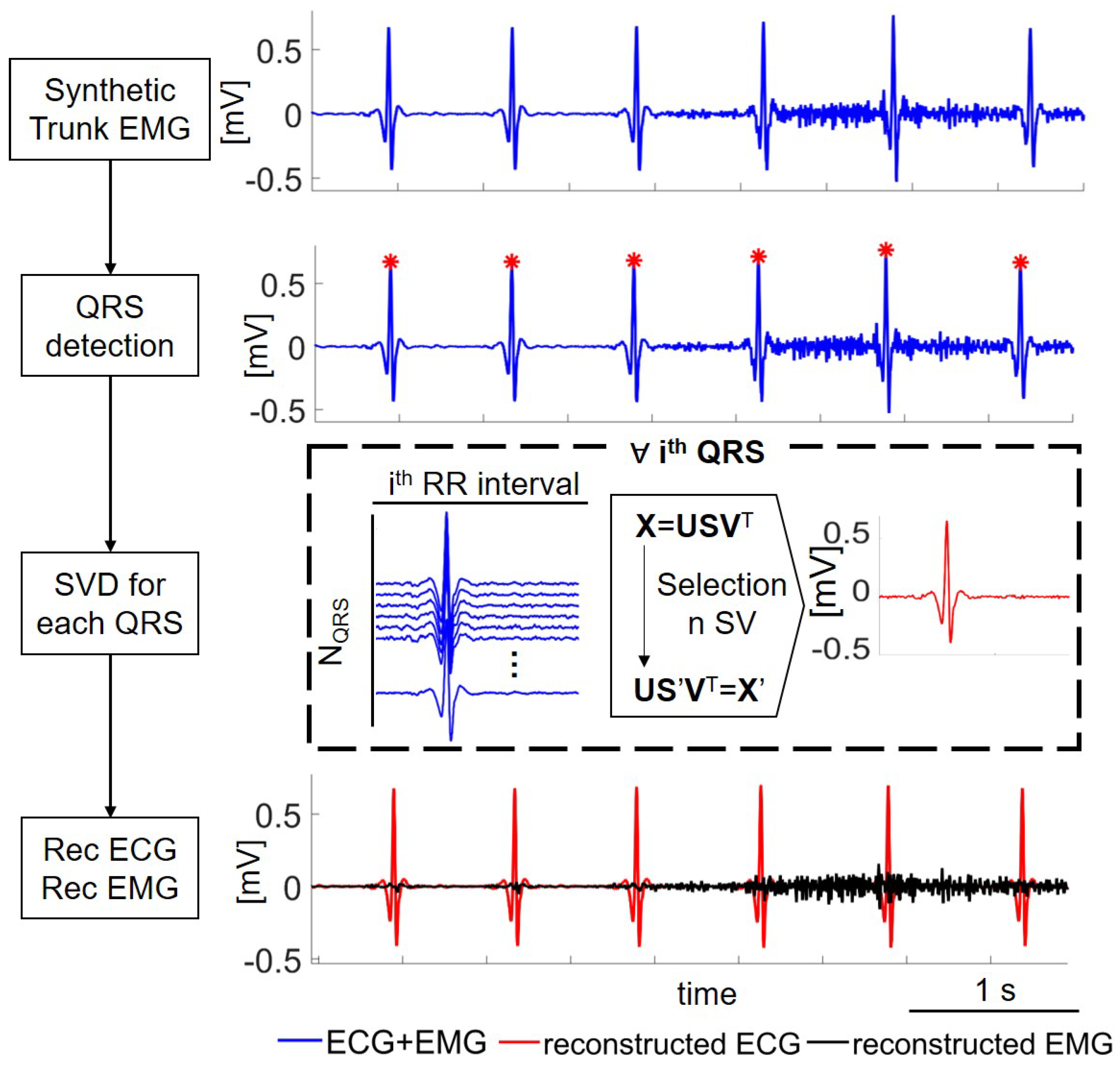
2.1. Synthetic Trunk EMG
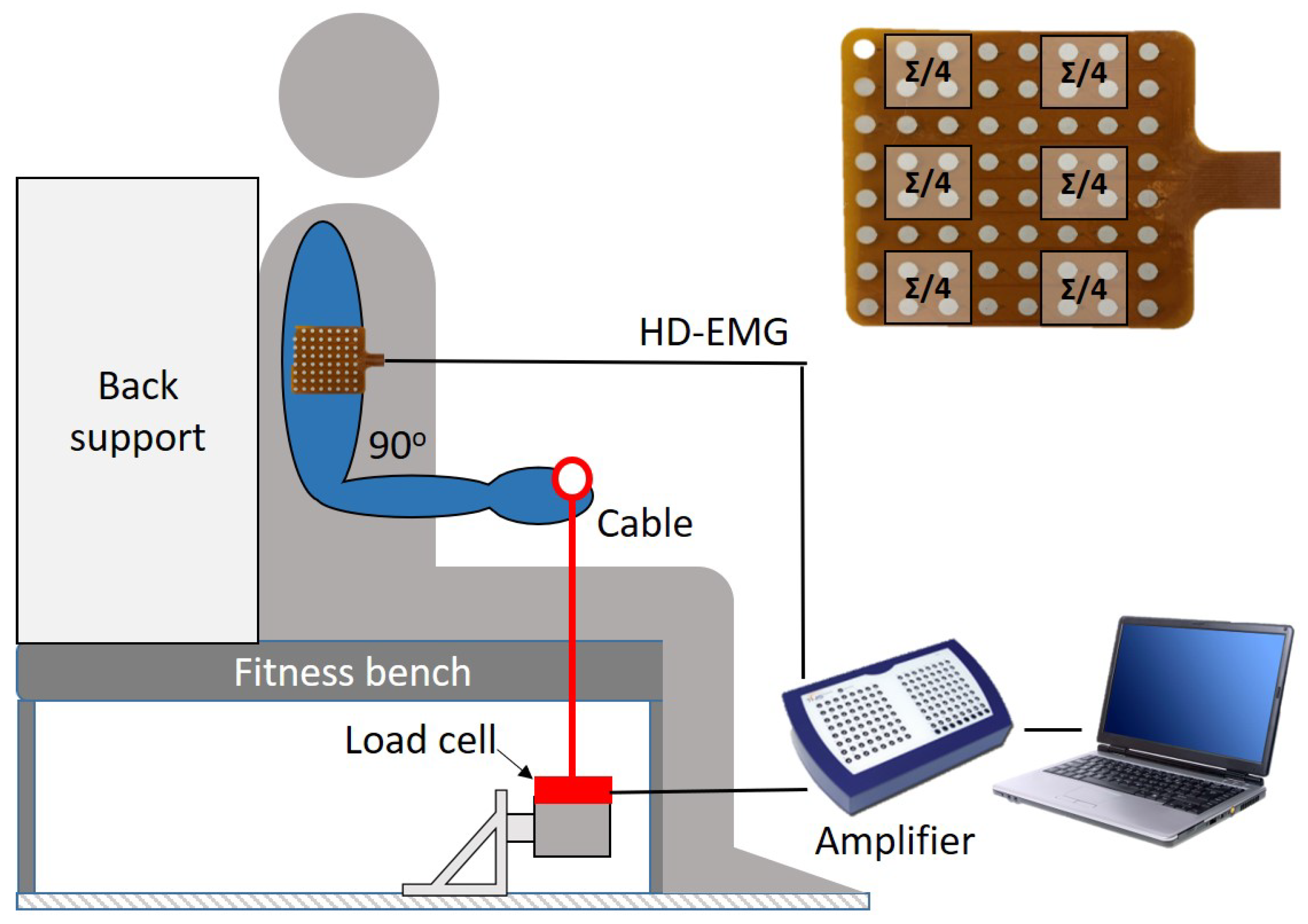
2.2. Real Data from Trunk EMG
2.3. Performance Metrics
2.4. SVD for ECG Denoising
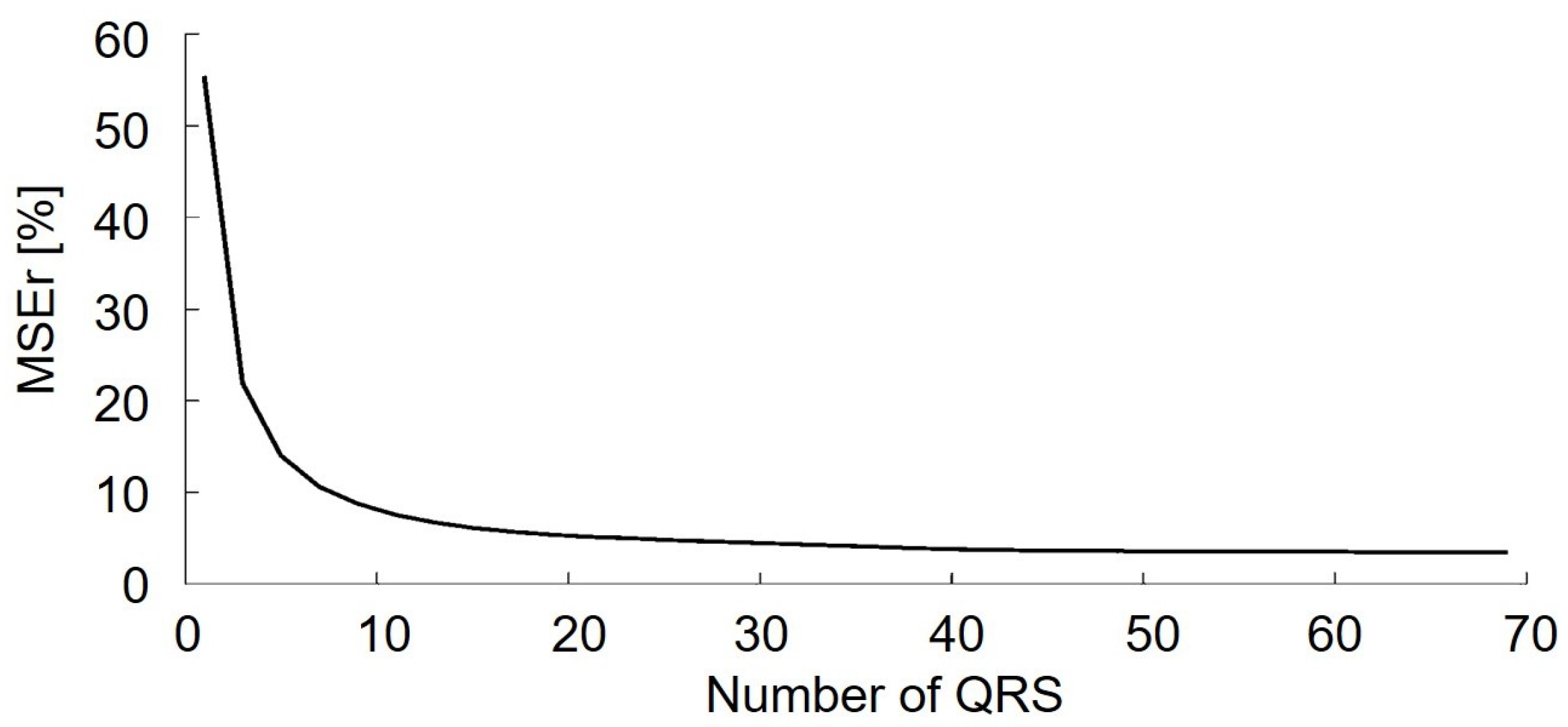
2.4.1. Optimizing the Number of QRS Complexes
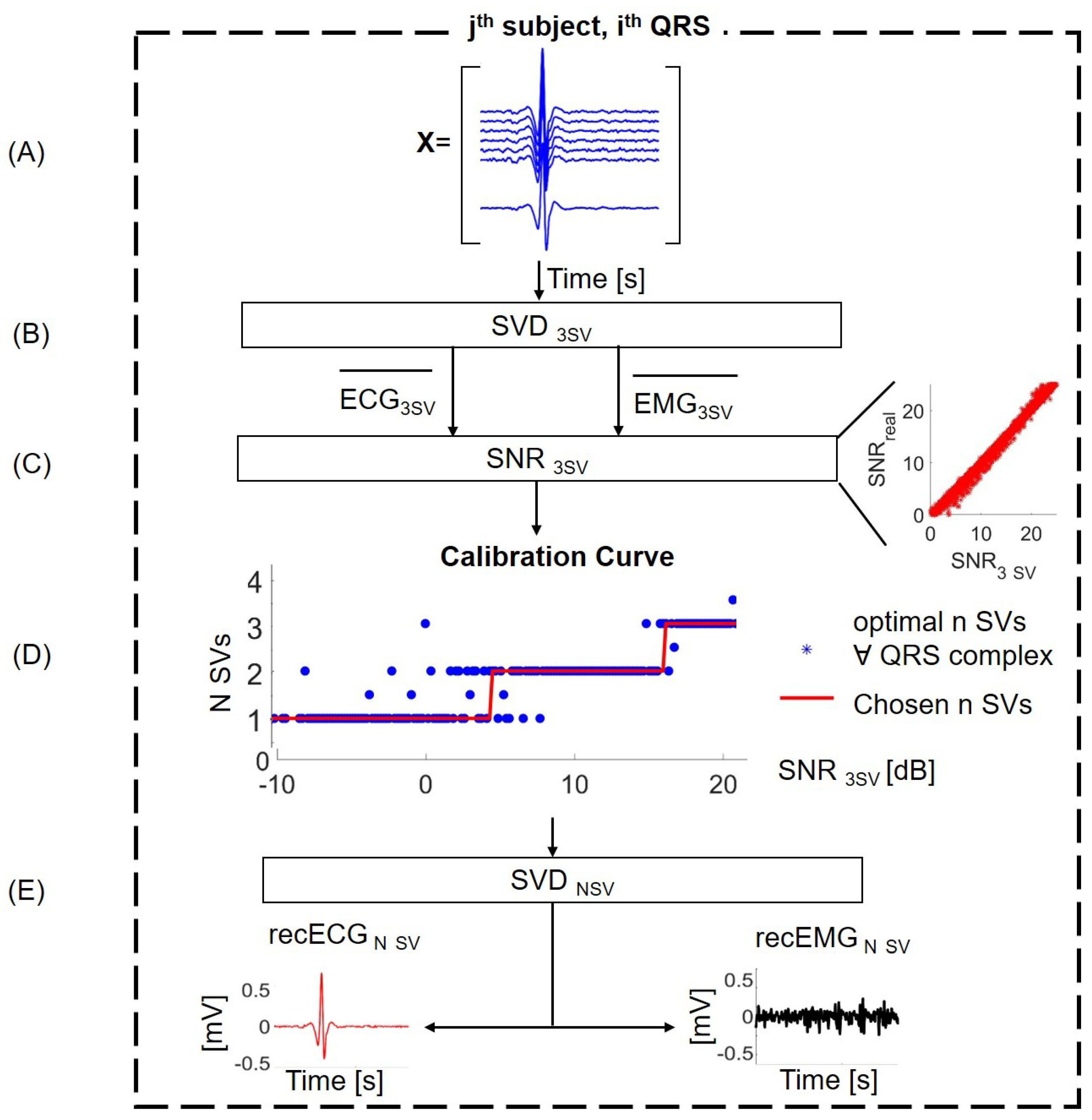
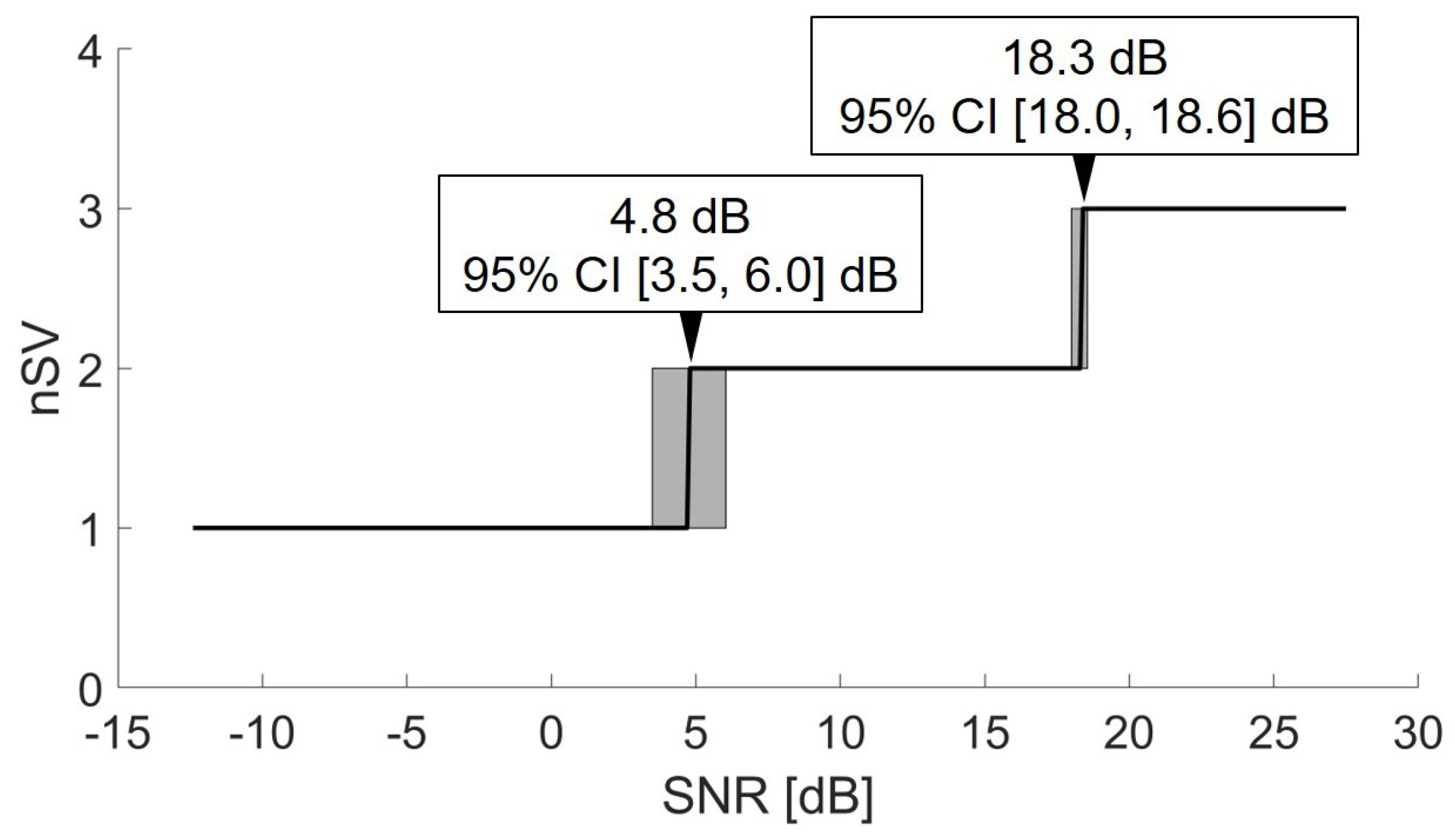
2.4.2. Optimizing the Number of SVs
2.5. Alternative Algorithms
3. Results
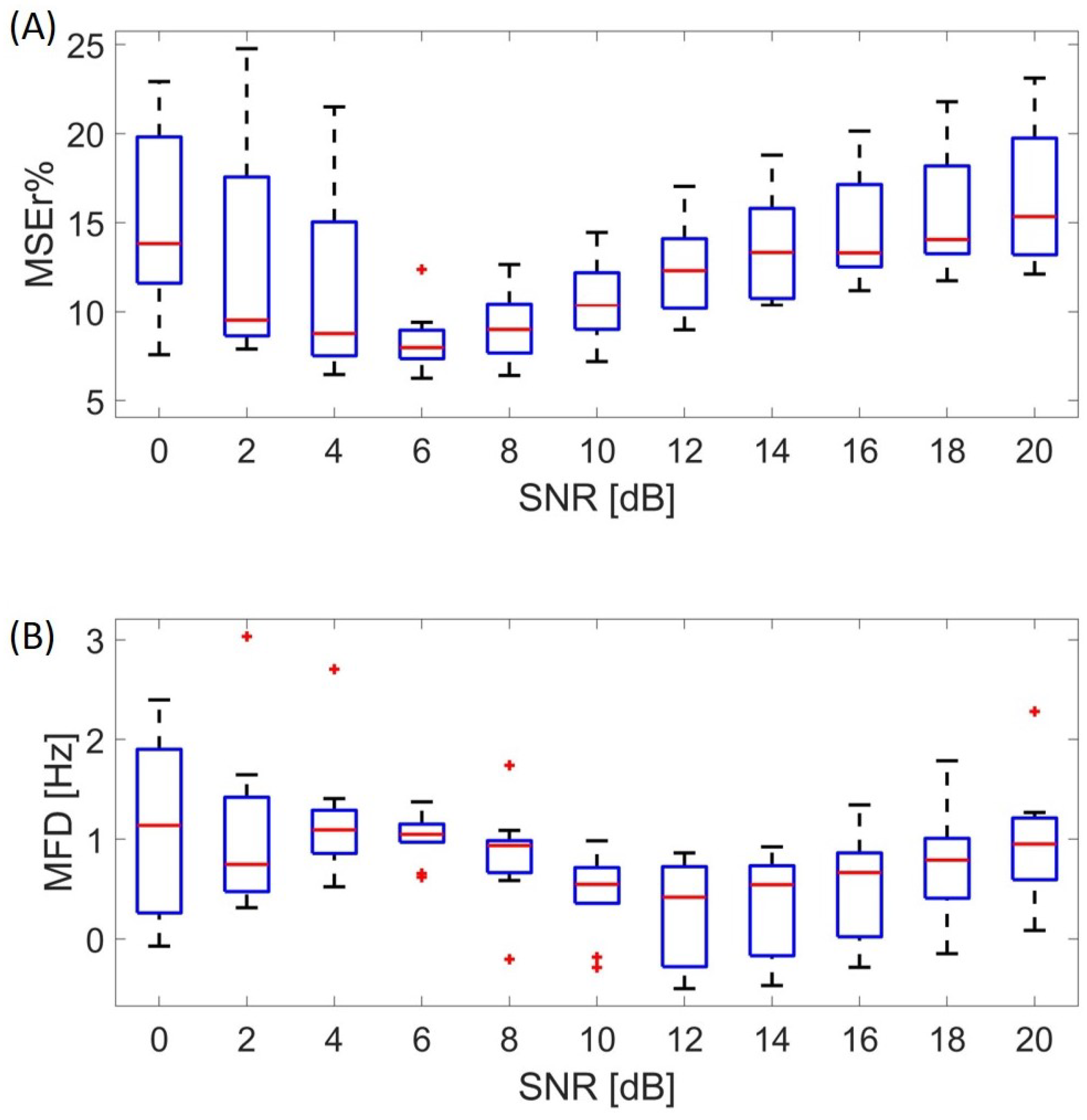
3.1. Performance at Different SNRs
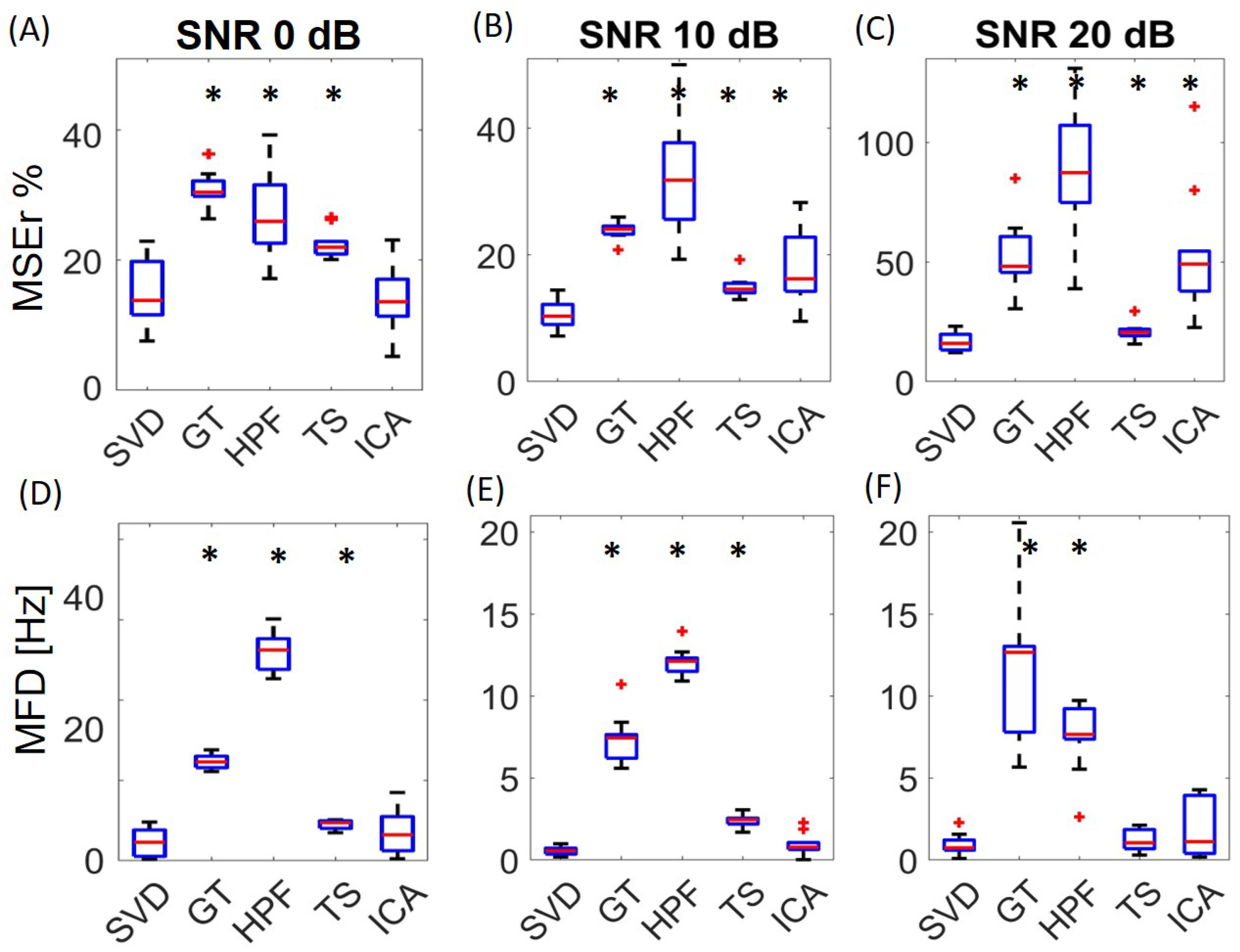
3.2. Comparison with Alternative Algorithms
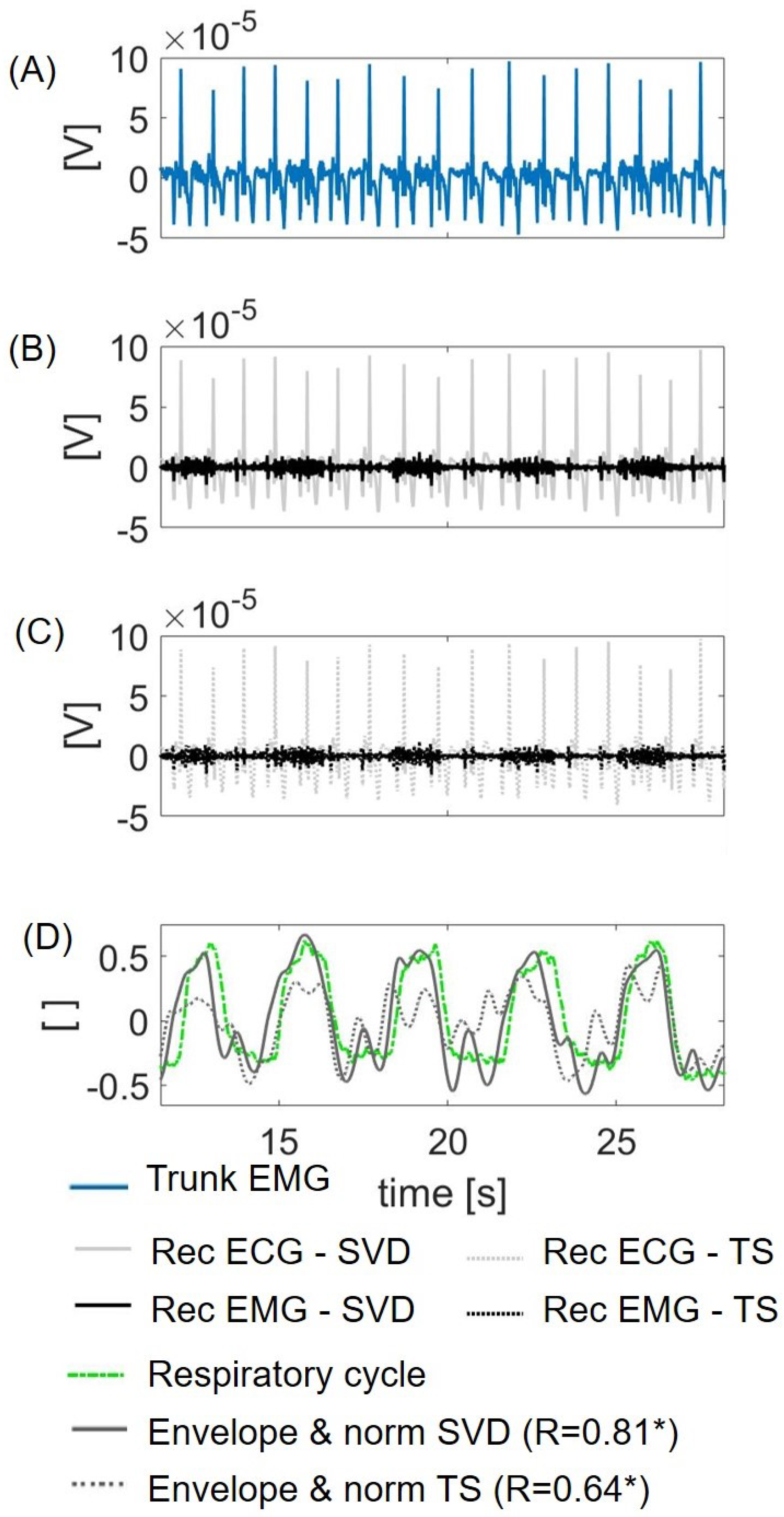
3.3. Feasibility on Real Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stoohs, R.A.; Blum, H.C.; Knaack, L.; Butsch-von-der Heydt, B.; Guilleminault, C. Comparison of pleural pressure and transcutaneous diaphragmatic electromyogram in obstructive sleep apnea syndrome. Sleep 2005, 28, 321–329. [Google Scholar] [PubMed] [Green Version]
- Vandenbussche, N.L.; Overeem, S.; van Dijk, J.P.; Simons, P.J.; Pevernagie, D.A. Assessment of respiratory effort during sleep: Esophageal pressure versus noninvasive monitoring techniques. Sleep Med. Rev. 2015, 24, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Clancy, E.A.; Morin, E.L.; Merletti, R. Sampling, noise-reduction and amplitude estimation issues in surface electromyography. J. Electromyogr. Kinesiol. 2002, 12, 1–16. [Google Scholar] [CrossRef]
- Hu, Y.; Mak, J.N.; Luk, K.D. Effect of electrocardiographic contamination on surface electromyography assessment of back muscles. J. Electromyogr. Kinesiol. 2009, 19, 145–156. [Google Scholar] [CrossRef]
- Drake, J.D.; Callaghan, J.P. Elimination of electrocardiogram contamination from electromyogram signals: An evaluation of currently used removal techniques. J. Electromyogr. Kinesiol. 2006, 16, 175–187. [Google Scholar] [CrossRef]
- Schweitzer, T.; Fitzgerald, J.; Bowden, J.; Lynne-Davies, P. Spectral analysis of human inspiratory diaphragmatic electromyograms. J. Appl. Physiol. 1979, 46, 152–165. [Google Scholar] [CrossRef]
- Bartolo, A.; Roberts, C.; Dzwonczyk, R.; Goldman, E. Analysis of diaphragm EMG signals: Comparison of gating vs. subtraction for removal of ECG contamination. J. Appl. Physiol. 1996, 80, 1898–1902. [Google Scholar] [CrossRef]
- Levine, S.; Gillen, J.; Weiser, P.; Gillen, M.; Kwatny, E. Description and validation of an ECG removal procedure for EMGdi power spectrum analysis. J. Appl. Physiol. 1986, 60, 1073–1081. [Google Scholar] [CrossRef]
- Merletti, R.; Parker, P.A.; Parker, P.J. Electromyography: Physiology, Engineering, and Non-Invasive Applications; John Wiley & Sons: Hoboken, MA, USA, 2004; Volume 11. [Google Scholar]
- Redfern, M.S.; Hughes, R.E.; Chaffin, D.B. High-pass filtering to remove electrocardiographic interference from torso EMG recordings. Clin. Biomech. 1993, 8, 44–48. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Peri, E.; Vullings, R.; Rabotti, C.; Van Dijk, J.P.; Mischi, M. Comparative Review of the Algorithms for Removal of Electrocardiographic Interference from Trunk Electromyography. Sensors 2020, 20, 4890. [Google Scholar] [CrossRef]
- Bloch, R. Subtraction of electrocardiographic signal from respiratory electromyogram. J. Appl. Physiol. 1983, 55, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Bartolo, A.; Dzwonczyk, R.; Roberts, O.; Goldman, E. Description and validation of a technique for the removal of ECG contamination from diaphragmatic EMG signal. Med. Biol. Eng. Comput. 1996, 34, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Abbaspour, S.; Fallah, A. Removing ECG artifact from the surface EMG signal using adaptive subtraction technique. J. Biomed. Phys. Eng. 2014, 4, 33. [Google Scholar] [PubMed]
- Cardoso, J.F. Blind signal separation: Statistical principles. Proc. IEEE 1998, 86, 2009–2025. [Google Scholar] [CrossRef] [Green Version]
- Willigenburg, N.W.; Daffertshofer, A.; Kingma, I.; Van Dieën, J.H. Removing ECG contamination from EMG recordings: A comparison of ICA-based and other filtering procedures. J. Electromyogr. Kinesiol. 2012, 22, 485–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mak, J.N.; Hu, Y.; Luk, K.D. An automated ECG-artifact removal method for trunk muscle surface EMG recordings. Med. Eng. Phys. 2010, 32, 840–848. [Google Scholar] [CrossRef]
- Kanjilal, P.P.; Palit, S.; Saha, G. Fetal ECG extraction from single-channel maternal ECG using singular value decomposition. IEEE Trans. Biomed. Eng. 1997, 44, 51–59. [Google Scholar] [CrossRef]
- Wildeboer, R.; Schoot, B.; Wijkstra, H.; Mischi, M.; Sammali, F.; Van Sloun, R.; Huang, Y.; Chen, P.; Bruce, M.; Rabotti, C.; et al. Blind Source Separation for Clutter and Noise Suppression in Ultrasound Imaging: Review for Different Applications. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2020, 67, 1497–1512. [Google Scholar] [CrossRef]
- Dongarra, J.; Gates, M.; Haidar, A.; Kurzak, J.; Luszczek, P.; Tomov, S.; Yamazaki, I. The singular value decomposition: Anatomy of optimizing an algorithm for extreme scale. SIAM Rev. 2018, 60, 808–865. [Google Scholar] [CrossRef]
- Jolliffe, I.T.; Cadima, J. Principal component analysis: A review and recent developments. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2016, 374, 20150202. [Google Scholar] [CrossRef]
- Sharma, A.; Paliwal, K.K.; Imoto, S.; Miyano, S. Principal component analysis using QR decomposition. Int. J. Mach. Learn. Cybern. 2013, 4, 679–683. [Google Scholar] [CrossRef]
- Ouali, M.A.; Chafaa, K. SVD-based method for ECG denoising. In Proceedings of the IEEE 2013 International Conference on Computer Applications Technology (ICCAT), Sousse, Tunisia, 20–22 January 2013; pp. 1–4. [Google Scholar]
- Bandarabadi, M.; Karami-Mollaei, M.; Afzalian, A.; Ghasemi, J. ECG denoising using singular value decomposition. Aust. J. Basic Appl. Sci. 2010, 4, 2109–2113. [Google Scholar]
- Hyvärinen, A.; Oja, E. Independent component analysis: Algorithms and applications. Neural Netw. 2000, 13, 411–430. [Google Scholar] [CrossRef] [Green Version]
- Junior, J.C.; Ferreira, D.; Nadal, J.; de Sá, A.M. Reducing electrocardiographic artifacts from electromyogram signals with independent component analysis. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 4598–4601. [Google Scholar]
- Hu, Y.; Li, X.; Xie, X.; Pang, L.; Cao, Y.; Luk, K. Applying independent component analysis on ECG cancellation technique for the surface recording of trunk electromyography. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; pp. 3647–3649. [Google Scholar]
- Alty, S.R.; Man, W.D.C.; Moxham, J.; Lee, K.C. Denoising of diaphragmatic electromyogram signals for respiratory control and diagnostic purposes. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 5560–5563. [Google Scholar]
- Chen, M.; Zhang, X.; Chen, X.; Zhu, M.; Li, G.; Zhou, P. FastICA peel-off for ECG interference removal from surface EMG. Biomed. Eng. Online 2016, 15, 65. [Google Scholar] [CrossRef] [Green Version]
- Zhou, P.; Kuiken, T.A. Eliminating cardiac contamination from myoelectric control signals developed by targeted muscle reinnervation. Physiol. Meas. 2006, 27, 1311. [Google Scholar] [CrossRef]
- Zhan, C.; Yeung, L.F.; Yang, Z. A wavelet-based adaptive filter for removing ECG interference in EMGdi signals. J. Electromyogr. Kinesiol. 2010, 20, 542–549. [Google Scholar] [CrossRef]
- Marque, C.; Bisch, C.; Dantas, R.; Elayoubi, S.; Brosse, V.; Perot, C. Adaptive filtering for ECG rejection from surface EMG recordings. J. Electromyogr. Kinesiol. 2005, 15, 310–315. [Google Scholar] [CrossRef]
- Xu, L.; Rabotti, C.; Mischi, M. Analysis of vibration exercise at varying frequencies by different fatigue estimators. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 24, 1284–1293. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Rabotti, C.; Mischi, M. Towards real-time estimation of muscle-fiber conduction velocity using delay-locked loop. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 25, 1453–1460. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Negro, F.; Xu, Y.; Rabotti, C.; Schep, G.; Farina, D.; Mischi, M. Does vibration superimposed on low-level isometric contraction alter motor unit recruitment strategy? J. Neural Eng. 2018, 15, 066001. [Google Scholar] [CrossRef] [Green Version]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sörnmo, L.; Laguna, P. Electrocardiogram (ECG) signal processing. In Wiley Encyclopedia of Biomedical Engineering; John Wiley & Sons, Inc.: New York, NY, USA, 2006. [Google Scholar]
- van Gilst, M.M.; van Dijk, J.P.; Krijn, R.; Hoondert, B.; Fonseca, P.; van Sloun, R.J.; Arsenali, B.; Vandenbussche, N.; Pillen, S.; Maass, H.; et al. Protocol of the SOMNIA project: An observational study to create a neurophysiological database for advanced clinical sleep monitoring. BMJ Open 2019, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, I.; Behar, J.; Sameni, R.; Zhu, T.; Oster, J.; Clifford, G.D.; Moody, G.B. Noninvasive fetal ECG: The PhysioNet/computing in cardiology challenge 2013. In Proceedings of the Computing in Cardiology 2013, Zaragoza, Spain, 22–25 September 2013; pp. 149–152. [Google Scholar]
- Moon, T.K.; Stirling, W.C. Mathematical Methods and Algorithms for Signal Processing; Prentice Hall: Upper Saddle River, NJ, USA, 2000; Volume 1. [Google Scholar]
- Hyvarinen, A. Fast and robust fixed-point algorithms for independent component analysis. IEEE Trans. Neural Netw. 1999, 10, 626–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vautard, R.; Yiou, P.; Ghil, M. Singular-spectrum analysis: A toolkit for short, noisy chaotic signals. Phys. D Nonlinear Phenom. 1992, 58, 95–126. [Google Scholar] [CrossRef]
- Hassani, H.; Xu, Z.; Zhigljavsky, A. Singular spectrum analysis based on the perturbation theory. Nonlinear Anal. Real World Appl. 2011, 12, 2752–2766. [Google Scholar] [CrossRef]
- Ghodsi, M.; Hassani, H.; Sanei, S. Extracting fetal heart signal from noisy maternal ECG by singular spectrum analysis. J. Stat. Its Interface Spec. Issue Appl. SSA 2010, 3, 399–411. [Google Scholar] [CrossRef] [Green Version]
- Lv, Q.; Zhang, X.D.; Jia, Y. Kalman filtering algorithm for blind source separation. In Proceedings of the IEEE International Conference on Acoustics, Speech, and Signal Processing (ICASSP’05), Philadelphia, PA, USA, 18–23 March 2005; Volume 5, p. 257. [Google Scholar]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peri, E.; Xu, L.; Ciccarelli, C.; Vandenbussche, N.L.; Xu, H.; Long, X.; Overeem, S.; van Dijk, J.P.; Mischi, M. Singular Value Decomposition for Removal of Cardiac Interference from Trunk Electromyogram. Sensors 2021, 21, 573. https://doi.org/10.3390/s21020573
Peri E, Xu L, Ciccarelli C, Vandenbussche NL, Xu H, Long X, Overeem S, van Dijk JP, Mischi M. Singular Value Decomposition for Removal of Cardiac Interference from Trunk Electromyogram. Sensors. 2021; 21(2):573. https://doi.org/10.3390/s21020573
Chicago/Turabian StylePeri, Elisabetta, Lin Xu, Christian Ciccarelli, Nele L. Vandenbussche, Hongji Xu, Xi Long, Sebastiaan Overeem, Johannes P. van Dijk, and Massimo Mischi. 2021. "Singular Value Decomposition for Removal of Cardiac Interference from Trunk Electromyogram" Sensors 21, no. 2: 573. https://doi.org/10.3390/s21020573