Mortality of Pandrug-Resistant Klebsiella pneumoniae Bloodstream Infections in Critically Ill Patients: A Retrospective Cohort of 115 Episodes

 ,
,
Abstract
:1. Introduction
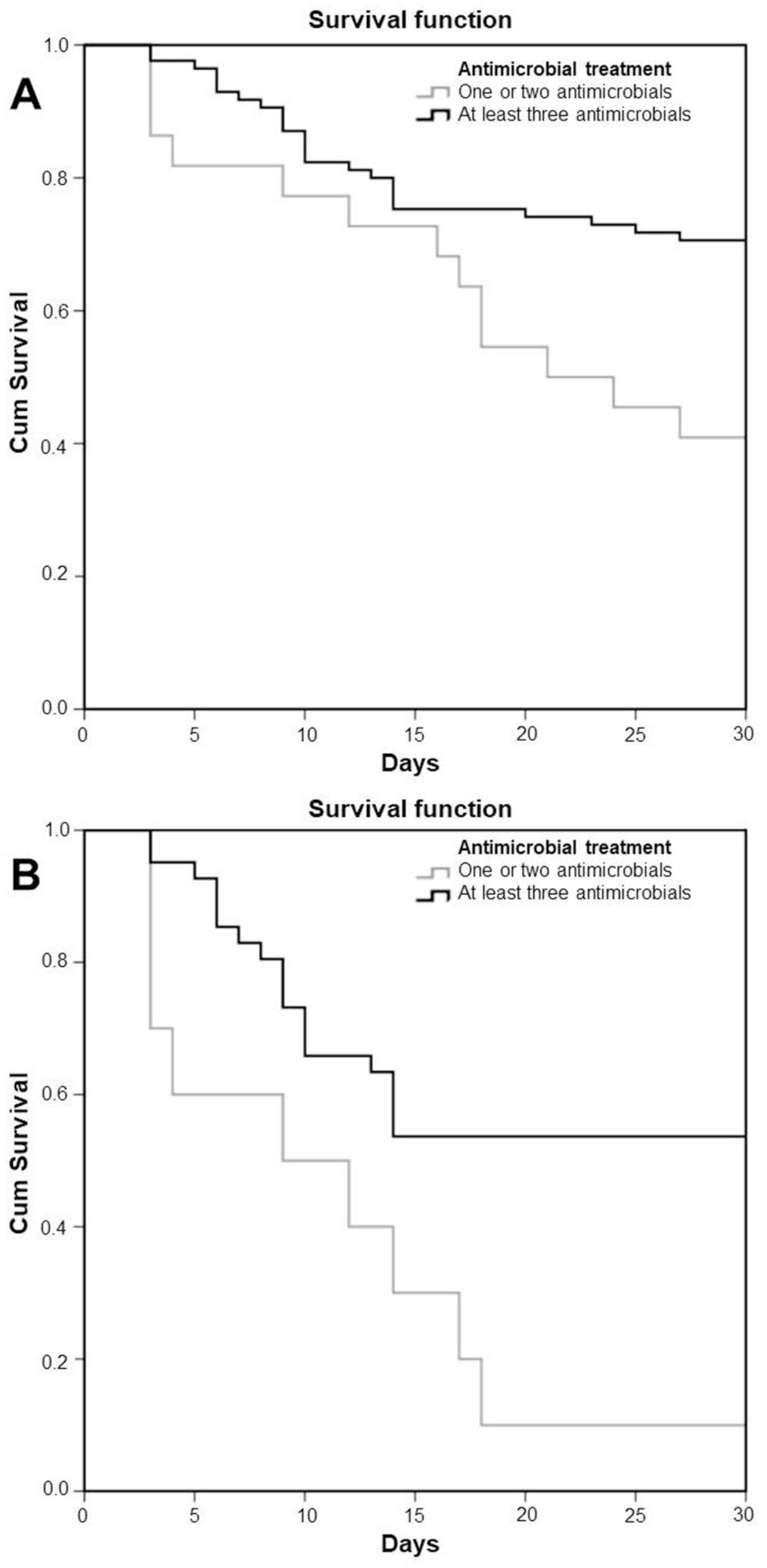
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martin, R.M.; Bachman, M.A. Colonization, Infection, and the Accessory Genome of Klebsiella pneumoniae. Front. Cell. Infect. Microbiol. 2018, 8, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, S.J.; Connor, C.; McNally, A. The evolution and transmission of multi-drug resistant Escherichia coli and Klebsiella pneumoniae: The complexity of clones and plasmids. Curr. Opin. Microbiol. 2019, 51, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Albiger, B.; Glasner, C.; Struelens, M.J.; Grundmann, H.; Monnet, D.L.; The European Survey of Carbapenemase-Producing Enterobacteriaceae (EuSCAPE) Working Group. Carbapenemase-producing Enterobacteriaceae in Europe: Assessment by national experts from 38 countries, May 2015. Eurosurveillance 2015, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutierrez-Gutierrez, B.; Salamanca, E.; de Cueto, M.; Hsueh, P.R.; Viale, P.; Pano-Pardo, J.R.; Venditti, M.; Tumbarello, M.; Daikos, G.; Canton, R.; et al. Effect of appropriate combination therapy on mortality of patients with bloodstream infections due to carbapenemase-producing Enterobacteriaceae (INCREMENT): A retrospective cohort study. Lancet. Infect. Dis. 2017, 17, 726–734. [Google Scholar] [CrossRef]
- Spyropoulou, A.; Papadimitriou-Olivgeris, M.; Bartzavali, C.; Vamvakopoulou, S.; Marangos, M.; Spiliopoulou, I.; Anastassiou, E.D.; Christofidou, M. A ten-year surveillance study of carbapenemase-producing Klebsiella pneumoniae in a tertiary care Greek university hospital: Predominance of KPC- over VIM- or NDM-producing isolates. J. Med. Microbiol. 2016, 65, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Karakonstantis, S.; Kritsotakis, E.I.; Gikas, A. Pandrug-resistant Gram-negative bacteria: A systematic review of current epidemiology, prognosis and treatment options. J. Antimicrob. Chemother. 2020, 75, 271–282. [Google Scholar] [CrossRef]
- Tsioutis, C.; Kritsotakis, E.I.; Maraki, S.; Gikas, A. Infections by pandrug-resistant gram-negative bacteria: Clinical profile, therapeutic management, and outcome in a series of 21 patients. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2010, 29, 301–305. [Google Scholar] [CrossRef]
- Falagas, M.E.; Bliziotis, I.A.; Kasiakou, S.K.; Samonis, G.; Athanassopoulou, P.; Michalopoulos, A. Outcome of infections due to pandrug-resistant (PDR) Gram-negative bacteria. BMC Infect. Dis. 2005, 5, 24. [Google Scholar] [CrossRef] [Green Version]
- Falagas, M.E.; Rafailidis, P.I.; Matthaiou, D.K.; Virtzili, S.; Nikita, D.; Michalopoulos, A. Pandrug-resistant Klebsiella pneumoniae, Pseudomonas aeruginosa and Acinetobacter baumannii infections: Characteristics and outcome in a series of 28 patients. Int. J. Antimicrob. Agents 2008, 32, 450–454. [Google Scholar] [CrossRef]
- Kofteridis, D.P.; Andrianaki, A.M.; Maraki, S.; Mathioudaki, A.; Plataki, M.; Alexopoulou, C.; Ioannou, P.; Samonis, G.; Valachis, A. Treatment pattern, prognostic factors, and outcome in patients with infection due to pan-drug-resistant gram-negative bacteria. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2020, 39, 965–970. [Google Scholar] [CrossRef]
- Papadimitriou-Olivgeris, M.; Bartzavali, C.; Nikolopoulou, A.; Kolonitsiou, F.; Mplani, V.; Spiliopoulou, I.; Christofidou, M.; Fligou, F.; Marangos, M. Impact of Tigecycline’s MIC in the Outcome of Critically Ill Patients with Carbapenemase-Producing Klebsiella pneumoniae Bacteraemia Treated with Tigecycline Monotherapy-Validation of 2019′s EUCAST Proposed Breakpoint Changes. Antibiotics 2020, 9, 828. [Google Scholar] [CrossRef]
- Brennan-Krohn, T.; Pironti, A.; Kirby, J.E. Synergistic Activity of Colistin-Containing Combinations against Colistin-Resistant Enterobacteriaceae. Antimicrob. Agents Chemother. 2018, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliva, A.; D’Abramo, A.; D’Agostino, C.; Iannetta, M.; Mascellino, M.T.; Gallinelli, C.; Mastroianni, C.M.; Vullo, V. Synergistic activity and effectiveness of a double-carbapenem regimen in pandrug-resistant Klebsiella pneumoniae bloodstream infections. J. Antimicrob. Chemother. 2014, 69, 1718–1720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzouvelekis, L.S.; Miriagou, V.; Kotsakis, S.D.; Spyridopoulou, K.; Athanasiou, E.; Karagouni, E.; Tzelepi, E.; Daikos, G.L. KPC-producing, multidrug-resistant Klebsiella pneumoniae sequence type 258 as a typical opportunistic pathogen. Antimicrob. Agents Chemother. 2013, 57, 5144–5146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, M.J.; Ko, K.S. Loss of hypermucoviscosity and increased fitness cost in colistin-resistant Klebsiella pneumoniae sequence type 23 strains. Antimicrob. Agents Chemother. 2015, 59, 6763–6773. [Google Scholar] [CrossRef] [Green Version]
- Papadimitriou-Olivgeris, M.; Fligou, F.; Bartzavali, C.; Zotou, A.; Spyropoulou, A.; Koutsileou, K.; Vamvakopoulou, S.; Sioulas, N.; Karamouzos, V.; Anastassiou, E.D.; et al. Carbapenemase-producing Klebsiella pneumoniae bloodstream infection in critically ill patients: Risk factors and predictors of mortality. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2017, 36, 1125–1131. [Google Scholar] [CrossRef]
- Gutierrez-Gutierrez, B.; Salamanca, E.; de Cueto, M.; Hsueh, P.R.; Viale, P.; Pano-Pardo, J.R.; Venditti, M.; Tumbarello, M.; Daikos, G.; Pintado, V.; et al. A Predictive Model of Mortality in Patients With Bloodstream Infections due to Carbapenemase-Producing Enterobacteriaceae. Mayo Clin. Proc. 2016, 91, 1362–1371. [Google Scholar] [CrossRef] [Green Version]
- Valles, J.; Leon, C.; Alvarez-Lerma, F. Nosocomial bacteremia in critically ill patients: A multicenter study evaluating epidemiology and prognosis. Spanish Collaborative Group for Infections in Intensive Care Units of Sociedad Espanola de Medicina Intensiva y Unidades Coronarias (SEMIUC). Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 1997, 24, 387–395. [Google Scholar] [CrossRef] [Green Version]
- Renaud, B.; Brun-Buisson, C.; Group, I.C.-B.S. Outcomes of primary and catheter-related bacteremia. A cohort and case-control study in critically ill patients. Am. J. Respir. Crit. Care Med. 2001, 163, 1584–1590. [Google Scholar] [CrossRef]
- Bassetti, M.; Vena, A.; Sepulcri, C.; Giacobbe, D.R.; Peghin, M. Treatment of Bloodstream Infections Due to Gram-Negative Bacteria with Difficult-to-Treat Resistance. Antibiotics 2020, 9, 632. [Google Scholar] [CrossRef]
- Falagas, M.E.; Skalidis, T.; Vardakas, K.Z.; Legakis, N.J.; Hellenic Cefiderocol Study Group. Activity of cefiderocol (S-649266) against carbapenem-resistant Gram-negative bacteria collected from inpatients in Greek hospitals. J. Antimicrob. Chemother. 2017, 72, 1704–1708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galani, I.; Nafplioti, K.; Adamou, P.; Karaiskos, I.; Giamarellou, H.; Souli, M.; Study, C. Nationwide epidemiology of carbapenem resistant Klebsiella pneumoniae isolates from Greek hospitals, with regards to plazomicin and aminoglycoside resistance. BMC Infect. Dis. 2019, 19, 167. [Google Scholar] [CrossRef]
- Papadimitriou-Olivgeris, M.; Bartzavali, C.; Lambropoulou, A.; Solomou, A.; Tsiata, E.; Anastassiou, E.D.; Fligou, F.; Marangos, M.; Spiliopoulou, I.; Christofidou, M. Reversal of carbapenemase-producing Klebsiella pneumoniae epidemiology from blaKPC- to blaVIM-harbouring isolates in a Greek ICU after introduction of ceftazidime/avibactam. J. Antimicrob. Chemother. 2019, 74, 2051–2054. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EUCAST. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 10; EUCAST: Växjö, Sweden, 2020. [Google Scholar]
- Al-Hasan, M.N.; Lahr, B.D.; Eckel-Passow, J.E.; Baddour, L.M. Predictive scoring model of mortality in Gram-negative bloodstream infection. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2013, 19, 948–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). Jama 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Queenan, A.M.; Bush, K. Carbapenemases: The versatile beta-lactamases. Clin. Microbiol. Rev. 2007, 20, 440–458. [Google Scholar] [CrossRef] [Green Version]
- Nordmann, P.; Poirel, L.; Carrer, A.; Toleman, M.A.; Walsh, T.R. How to detect NDM-1 producers. J. Clin. Microbiol. 2011, 49, 718–721. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | All Patients | Patients with Septic Shock | ||||
|---|---|---|---|---|---|---|
| Survivors (n = 70) | Non-Survivors (n = 45) | p | Survivors (n = 23) | Non-Survivors (n = 28) | p | |
| Demographics | ||||||
| Age (years) | 51.5 ± 18.6 | 62.1 ± 15.4 | 0.003 | 59.3 ± 18.5 | 59.4 ± 15.9 | 0.947 |
| Male gender | 49 (70.0%) | 26 (57.8%) | 0.229 | 17 (73.9%) | 18 (64.3%) | 0.552 |
| Comorbidities | ||||||
| Diabetes mellitus | 9 (12.9%) | 10 (22.2%) | 0.207 | 2 (8.7%) | 6 (21.4%) | 0.269 |
| Chronic obstructive pulmonary disease | 3 (4.3%) | 7 (15.6%) | 0.047 | 0 (0.0%) | 4 (14.3%) | 0.117 |
| Chronic heart failure | 3 (4.3%) | 8 (17.8%) | 0.023 | 0 (0.0%) | 4 (14.3%) | 0.117 |
| Chronic kidney disease | 1 (1.2%) | 1 (2.2%) | 1.000 | 1 (4.3%) | 0 (0.0%) | 0.451 |
| Malignancy | 6 (8.6%) | 9 (20.0%) | 0.093 | 2 (8.7%) | 4 (14.3%) | 0.678 |
| Immunosuppressive therapy | 3 (4.3%) | 5 (11.1%) | 0.259 | 1 (4.3%) | 2 (7.1%) | 1.000 |
| Obesity | 20 (28.6%) | 16 (35.6%) | 0.537 | 5 (21.7%) | 11 (39.3%) | 0.232 |
| Charlson comorbidity index | 2.5 ± 3.2 | 4.8 ± 4.3 | 0.002 | 2.8 ± 3.0 | 4.1 ± 3.8 | 0.292 |
| Infection data | ||||||
| Prior surgery (within a month form infection onset) | 34 (48.6%) | 23 (51.1%) | 0.850 | 10 (43.5%) | 16 (57.1%) | 0.404 |
| Days at risk (from ICU admission to infection onset) | 27.4 ± 26.5 | 21.5 ± 21.4 | 0.168 | 30.6 ± 35.2 | 21.6 ± 22.2 | 0.464 |
| Isolate carrying blaKPC | 59 (84.3%) | 39 (86.7%) | 0.794 | 18 (78.3%) | 25 (89.3%) | 0.442 |
| Septic shock | 23 (32.9%) | 28 (62.2%) | 0.002 | - | - | - |
| Type of infection | ||||||
| Primary BSI | 34 (48.6%) | 19 (42.2%) | 12 (52.2%) | 10 (35.7%) | ||
| Catheter-related BSI | 28 (40.0%) | 7 (15.6%) | 8 (34.8%) | 4 (14.3%) | ||
| Othera | 8 (11.4%) | 19 (42.2%) | <0.001b | 3 (13.0%) | 14 (50.0%) | 0.007b |
| Antimicrobial treatment | ||||||
| Monotherapy | 1 (1.4%) | 7 (15.6%) | 0 (0.0%) | 2 (7.1%) | ||
| Combination of two antimicrobials | 9 (12.9%) | 13 (28.9%) | 1 (4.3%) | 7 (25.0%) | ||
| Combination of three or more antimicrobials | 60 (85.7%) | 25 (55.6%) | <0.001 | 22 (95.7%) | 19 (67.9%) | 0.015 |
| Carbapenem-including treatment | 66 (94.3%) | 40 (88.9%) | 0.310 | 21 (91.3%) | 26 (92.9%) | 1.000 |
| Colistin-including treatment | 64 (91.4%) | 38 (84.4%) | 0.366 | 22 (95.7%) | 25 (89.3%) | 0.617 |
| Aminoglycoside-including treatment | 47 (67.1%) | 20 (44.4%) | 0.020 | 16 (69.6%) | 14 (50.0%) | 0.253 |
| Tigecycline-including treatment | 48 (68.6%) | 24 (53.3%) | 0.117 | 18 (78.3%) | 20 (71.4%) | 0.749 |
| Corticosteroid administration during infection | 37 (52.9%) | 32 (71.1%) | 0.055 | 13 (56.5%) | 21 (75.0%) | 0.234 |
| Characteristics | All Patients | Patients with Septic Shock | ||
|---|---|---|---|---|
| p | OR (95% CI) | p | OR (95% CI) | |
| Septic shock | 0.002 | 5.2 (1.8–15.0) | ||
| Charlson comorbidity index | 0.012 | 1.2 (1.0–1.3) | ||
| BSI other than primary or catheter-related | 0.001 | 6.4 (2.0–20.2) | 0.008 | 7.4 (1.7–33.0) |
| Combination of at least three antimicrobials | <0.001 | 0.105 (0.032–0.344) | 0.029 | 0.083 (0.009–0.774) |
| Treatment Regimen | Survivors (n = 70) | Non-Survivors (n = 45) | Mortality (%) |
|---|---|---|---|
| One antimicrobial | 1 | 7 | 87.5 |
| Carbapenem | 1 | 4 | 80.0 |
| Colistin | 0 | 2 | 100 |
| Gentamicin | 0 | 1 | 100 |
| Two antimicrobials | 9 | 13 | 59.1 |
| Carbapenem + Aminoglycoside | 2 | 1 | 33.3 |
| Colistin + Tigecycline | 0 | 1 | 100 |
| Carbapenem + Tigecycline | 2 | 1 | 33.3 |
| Carbapenem + Colistin | 5 | 10 | 66.7 |
| Three antimicrobials | 30 | 9 | 23.1 |
| Colistin + Tigecycline + Aminoglycoside | 2 | 0 | 0.0 |
| Carbapenem + Tigecycline + Aminoglycoside | 15 | 3 | 16.7 |
| Colistin + Tigecycline + Carbapenem | 10 | 5 | 33.3 |
| Colistin + Carbapenem + Aminoglycoside | 1 | 0 | 0.0 |
| Colistin + Tigecycline + Ceftazidime/avibactam | 1 | 0 | 0.0 |
| Colistin + Tigecycline + Fosfomycin | 1 | 1 | 50.0 |
| Four or more antimicrobials | 30 | 16 | 34.8 |
| Carbapenem + Colistin + Tigecycline + Aminoglycoside | 25 | 15 | 37.5 |
| Carbapenem + Colistin + Tigecycline + Aminoglycoside + other antimicrobial | 3 | 0 | 0.0 |
| Double carbapenem + Colistin + Tigecycline + Aminoglycoside | 2 | 0 | 0.0 |
| Carbapenem + Colistin + Tigecycline + Fosfomycin | 0 | 1 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadimitriou-Olivgeris, M.; Bartzavali, C.; Georgakopoulou, A.; Kolonitsiou, F.; Papamichail, C.; Spiliopoulou, I.; Christofidou, M.; Fligou, F.; Marangos, M. Mortality of Pandrug-Resistant Klebsiella pneumoniae Bloodstream Infections in Critically Ill Patients: A Retrospective Cohort of 115 Episodes. Antibiotics 2021, 10, 76. https://doi.org/10.3390/antibiotics10010076
Papadimitriou-Olivgeris M, Bartzavali C, Georgakopoulou A, Kolonitsiou F, Papamichail C, Spiliopoulou I, Christofidou M, Fligou F, Marangos M. Mortality of Pandrug-Resistant Klebsiella pneumoniae Bloodstream Infections in Critically Ill Patients: A Retrospective Cohort of 115 Episodes. Antibiotics. 2021; 10(1):76. https://doi.org/10.3390/antibiotics10010076
Chicago/Turabian StylePapadimitriou-Olivgeris, Matthaios, Christina Bartzavali, Alexandra Georgakopoulou, Fevronia Kolonitsiou, Chrisavgi Papamichail, Iris Spiliopoulou, Myrto Christofidou, Fotini Fligou, and Markos Marangos. 2021. "Mortality of Pandrug-Resistant Klebsiella pneumoniae Bloodstream Infections in Critically Ill Patients: A Retrospective Cohort of 115 Episodes" Antibiotics 10, no. 1: 76. https://doi.org/10.3390/antibiotics10010076