Etiology of ‘Sinus Headache’—Moving the Focus from Rhinology to Neurology. A Systematic Review

 ,
,  , and
, and
Abstract
:1. Introduction
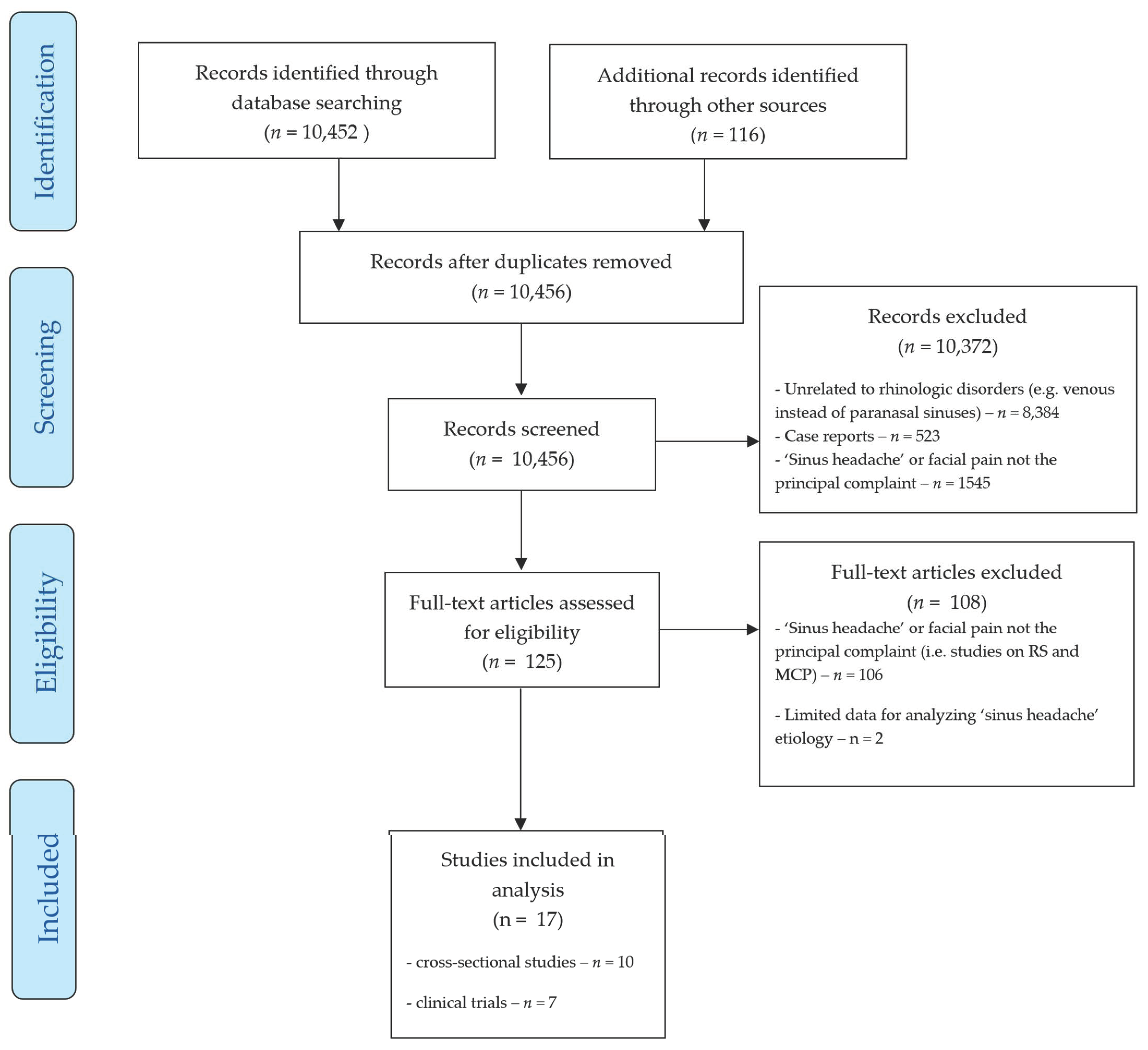
2. Materials and Methods
3. Results
3.1. Causes of Complaints in Patients with ‘Sinus Headache’
3.2. Treatment Approaches to ‘Sinus Headache’
4. Conclusions
- Migraine and tension-type headache are the most prevalent causes of complaints in patients reporting to a physician for treatment of ‘sinus headache and facial pain’.
- Medications effective in migraine and tension-type headache also decrease ‘sinus headache’ symptoms. Although this finding cannot be treated as diagnosis confirmation, it supports observations that ‘sinus headache’ is mostly misdiagnosed primary headache.
- Multidisciplinary evaluation of patients with ‘sinus headache’ should be introduced at an early stage. The team should include a headache specialist and rhinologist, as this would allow for the correct classification of headache type and avoidance of unnecessary surgical procedures.
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kaymakci, M.; Cikriklar, H.I.; Pay, G. The Aetiology Underlying Sinus Headaches. J. Int. Med. Res. 2013, 41, 218–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cady, R.K.; Schreiber, C.P. Sinus Headache: A Clinical Conundrum. Otolaryngol. Clin. N. Am. 2004, 37, 267–288. [Google Scholar] [CrossRef]
- Steiner, T.J.; Jensen, R.; Katsarava, Z.; Linde, M.; MacGregor, E.A.; Osipova, V.; Paemeleire, K.; Olesen, J.; Peters, M.; Martelletti, P. Aids to Management of Headache Disorders in Primary Care (2nd Edition): On Behalf of the European Headache Federation and Lifting The Burden: The Global Campaign against Headache. J. Headache Pain 2019, 20, 57. [Google Scholar] [CrossRef] [PubMed]
- Eross, E.; Dodick, D.; Eross, M. The Sinus, Allergy and Migraine Study (SAMS): CME. Headache J. Head Face Pain 2007, 47, 213–224. [Google Scholar] [CrossRef]
- Lipton, R.B.; Munjal, S.; Alam, A.; Buse, D.C.; Fanning, K.M.; Reed, M.L.; Schwedt, T.J.; Dodick, D.W. Migraine in America Symptoms and Treatment (MAST) Study: Baseline Study Methods, Treatment Patterns, and Gender Differences. Headache J. Head Face Pain 2018, 58, 1408–1426. [Google Scholar] [CrossRef]
- Lipton, R.B.; Diamond, S.; Reed, M.; Diamond, M.L.; Stewart, W.F. Migraine Diagnosis and Treatment: Results from the American Migraine Study II. Headache J. Head Face Pain 2001, 41, 638–645. [Google Scholar] [CrossRef] [Green Version]
- Al-Hashel, J.Y.; Ahmed, S.F.; Alroughani, R.; Goadsby, P.J. Migraine Misdiagnosis as a Sinusitis, a Delay That Can Last for Many Years. J. Headache Pain 2013, 14, 97. [Google Scholar] [CrossRef]
- Patel, Z.M.; Kennedy, D.W.; Setzen, M.; Poetker, D.M.; DelGaudio, J.M. “Sinus Headache”: Rhinogenic Headache or Migraine? An Evidence-Based Guide to Diagnosis and Treatment: “Sinus Headache”: Rhinogenic Headache or Migraine? Int. Forum Allergy Rhinol. 2013, 3, 221–230. [Google Scholar] [CrossRef]
- Smith, B.C.; George, L.C.; Svider, P.F.; Nebor, I.; Folbe, A.J.; Sheyn, A.; Johnson, A.P.; Eloy, J.A. Rhinogenic Headache in Pediatric and Adolescent Patients: An Evidence-based Review. Int. Forum Allergy Rhinol. 2019, 9, 443–451. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Farmer, R.L.; Garg, R.K.; Afifi, A.M. Can Functional Nasal Surgery Treat Chronic Headaches? A Systematic Review. Plast. Reconstr. Surg. 2018, 142, 1583–1592. [Google Scholar] [CrossRef] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Mullol, J.; Bachert, C.; Alobid, I.; Baroody, F.; Cohen, N.; Cervin, A.; Douglas, R.; Gevaert, P.; et al. EPOS 2012: European Position Paper on Rhinosinusitis and Nasal Polyps 2012. A Summary for Otorhinolaryngologists. Rhinol. J. 2012, 50, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhin 2020, 58, 1–464. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; Brooks, P.; Woolf, A.; Blyth, F.; March, L.; Bain, C.; Baker, P.; Smith, E.; Buchbinder, R. Assessing Risk of Bias in Prevalence Studies: Modification of an Existing Tool and Evidence of Interrater Agreement. J. Clin. Epidemiol. 2012, 65, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agius, A.M.; Jones, N.S.; Muscat, R. Prospective Three-Year Follow up of a Cohort Study of 240 Patients with Chronic Facial Pain. J. Laryngol. Otol. 2014, 128, 518–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foroughipour, M.; Sharifian, S.M.R.; Shoeibi, A.; Ebdali Barabad, N.; Bakhshaee, M. Causes of Headache in Patients with a Primary Diagnosis of Sinus Headache. Eur. Arch. Oto-Rhino-Laryngol. 2011, 268, 1593–1596. [Google Scholar] [CrossRef] [PubMed]
- Şenbil, N.; Gürer, Y.K.Y.; Üner, Ç.; Barut, Y. Sinusitis in Children and Adolescents with Chronic or Recurrent Headache: A Case–Control Study. J. Headache Pain 2008, 9, 33–36. [Google Scholar] [CrossRef] [Green Version]
- Schreiber, C.P.; Hutchinson, S.; Webster, C.J.; Ames, M.; Richardson, M.S.; Powers, C. Prevalence of Migraine in Patients With a History of Self-Reported or Physician-Diagnosed “Sinus” Headache. Arch. Intern. Med. 2004, 164, 1769. [Google Scholar] [CrossRef] [Green Version]
- Lal, D.; Rounds, A.B.; Rank, M.A.; Divekar, R. Clinical and 22-Item Sino-Nasal Outcome Test Symptom Patterns in Primary Headache Disorder Patients Presenting to Otolaryngologists with “Sinus” Headaches, Pain or Pressure: SNOT-22 Symptoms in Primary Headache Patients. Int. Forum Allergy Rhinol. 2015, 5, 408–416. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd Edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Paulson, E.P.; Graham, S.M. Neurologic Diagnosis and Treatment in Patients with Computed Tomography and Nasal Endoscopy Negative Facial Pain. Laryngoscope 2004, 114, 1992–1996. [Google Scholar] [CrossRef] [PubMed]
- Mehle, M.E.; Kremer, P.S. Sinus CT Scan Findings in “Sinus Headache” Migraineurs. Headache 2008, 48, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Daudia, A.T.; Jones, N.S. Facial Migraine in a Rhinological Setting. Clin. Otolaryngol. Allied Sci. 2002, 27, 521–525. [Google Scholar] [CrossRef] [PubMed]
- West, B.; Jones, N.S. Endoscopy-Negative, Computed Tomography-Negative Facial Pain in a Nasal Clinic. Laryngoscope 2001, 111, 581–586. [Google Scholar] [CrossRef]
- Clifton, N.J.; Jones, N.S. Prevalence of Facial Pain in 108 Consecutive Patients with Paranasal Mucopurulent Discharge at Endoscopy. J. Laryngol. Otol. 2007, 121, 345–348. [Google Scholar] [CrossRef]
- Goadsby, P.J.; Holland, P.R.; Martins-Oliveira, M.; Hoffmann, J.; Schankin, C.; Akerman, S. Pathophysiology of Migraine: A Disorder of Sensory Processing. Physiol. Rev. 2017, 97, 553–622. [Google Scholar] [CrossRef]
- Hansen, A.G.; Stovner, L.J.; Hagen, K.; Helvik, A.-S.; Thorstensen, W.M.; Nordgård, S.; Bugten, V.; Eggesbø, H.B. Paranasal Sinus Opacification in Headache Sufferers: A Population-Based Imaging Study (the HUNT Study-MRI). Cephalalgia 2017, 37, 509–516. [Google Scholar] [CrossRef] [Green Version]
- Perry, B.F.; Login, I.S.; Kountakis, S.E. Nonrhinologic Headache in a Tertiary Rhinology Practice. Otolaryngol. Head Neck Surg. 2004, 130, 449–452. [Google Scholar] [CrossRef]
- International Classification of Orofacial Pain, 1st Edition (ICOP). Cephalalgia 2020, 40, 129–221. [CrossRef] [Green Version]
- Van Alboom, E.; Louis, P.; Van Zandijcke, M.; Crevits, L.; Vakaet, A.; Paemeleire, K. Diagnostic and Therapeutic Trajectory of Cluster Headache Patients in Flanders. Acta Neurol. Belg. 2009, 109, 10–17. [Google Scholar] [PubMed]
- van Vliet, J.A. Features Involved in the Diagnostic Delay of Cluster Headache. J. Neurol. Neurosurg. Psychiatry 2003, 74, 1123–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voiticovschi-Iosob, C.; Allena, M.; De Cillis, I.; Nappi, G.; Sjaastad, O.; Antonaci, F. Diagnostic and Therapeutic Errors in Cluster Headache: A Hospital-Based Study. J. Headache Pain 2014, 15, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Kim, Y.; Lim, T.Y. Efficacy of Sphenopalatine Ganglion Block in Nasal Mucosal Headache Presenting as Facial Pain. Cranio 2018, 38, 1–3. [Google Scholar] [CrossRef]
- Bahra, A.; Goadsby, P.J. Diagnostic Delays and Mis-Management in Cluster Headache. Acta Neurol. Scand. 2004, 109, 175–179. [Google Scholar] [CrossRef]
- Chen, K.; Cao, Y.; Wu, J.; Xiang, H.; Huang, X.; Chen, B. Clinical Analysis of Sphenoid Sinus Mucocele With Initial Neurological Symptoms. Headache J. Head Face Pain 2019, 59. [Google Scholar] [CrossRef]
- Rossi, P.; Faroni, J.; Tassorelli, C.; Nappi, G. Diagnostic Delay and Suboptimal Management in a Referral Population with Hemicrania Continua. Headache J. Head Face Pain 2009, 49, 227–234. [Google Scholar] [CrossRef]
- Leong, S.C.; Tsang, H.K.; Wilkie, M.D.; Banhegyi, G. Characterisation of Patients with Endoscopy-Negative, Computer Tomography-Negative Midfacial Segment Pain Using the Sino-Nasal Outcome Test. Rhin 2014, 52, 78–83. [Google Scholar] [CrossRef]
- Ishkanian, G.; Blumenthal, H.; Webster, C.J.; Richardson, M.S.; Ames, M. Efficacy of Sumatriptan Tablets in Migraineurs Self-Described or Physician-Diagnosed as Having Sinus Headache: A Randomized, Double-Blind, Placebo-Controlled Study. Clin. Ther. 2007, 29, 99–109. [Google Scholar] [CrossRef]
- Kari, E.; DelGaudio, J.M. Treatment of Sinus Headache as Migraine: The Diagnostic Utility of Triptans. Laryngoscope 2008, 118, 2235–2239. [Google Scholar] [CrossRef] [Green Version]
- Cady, R.K.; Schreiber, C.P. Sinus Headache or Migraine? Considerations in Making a Differential Diagnosis. Neurology 2002, 58, S10–S14. [Google Scholar] [CrossRef] [PubMed]
- Pedram, D.; Jennifer, H.; John, M. “Sinus Headache” in Chronic Rhinosinusitis (CRS): An Analysis of Otolaryngology Initiated Treatment Efficacy of Migraine in the CRS Patient. J. Sinusitis Migraine 2016, 1, 1–4. [Google Scholar]
- Dadgarnia, M.H.; Atighechi, S.; Baradaranfar, M.H. The Response to Sodium Valproate of Patients with Sinus Headaches with Normal Endoscopic and CT Findings. Eur. Arch. Otorhinolaryngol. 2010, 267, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Boonchoo, R. Functional Endoscopic Sinus Surgery in Patients with Sinugenic Headache. J. Med. Assoc. Thail. 1997, 80, 521–526. [Google Scholar]
- El-Silimy, O. The Place of Endonasal Endoscopy in the Relief of Middle Turbinate Sinonasal Headache Syndrome. Rhinology 1995, 33, 244–245. [Google Scholar]
- Giacomini, P.G.; Alessandrini, M.; DePadova, A. Septoturbinal Surgery in Contact Point Headache Syndrome: Long-Term Results. Cranio 2003, 21, 130–135. [Google Scholar] [CrossRef]
- Huang, H.-H.; Lee, T.-J.; Huang, C.-C.; Chang, P.-H.; Huang, S.-F. Non–Sinusitis-Related Rhinogenous Headache: A Ten-Year Experience. Am. J. Otolaryngol. 2008, 29, 326–332. [Google Scholar] [CrossRef]
- Peter, J.C. Analysis of Headache Outcomes in Patients Treated with Nasal and Sinus Surgery. Arch. Otolaryngol. Rhinold 2019, 020–025. [Google Scholar] [CrossRef] [Green Version]
- Kutluhan, A.; Demir, M.K.; Bozdemir, K.; Callioglu, E.E. Conchal Compression: Is It a New Syndrome? Int. J. Clin. Exp. Med. 2015, 8, 14440–14446. [Google Scholar]
- Laury, A.M.; Chen, P.G.; McMains, K.C. Randomized Controlled Trial Examining the Effects of Balloon Catheter Dilation on “Sinus Pressure” / Barometric Headaches. Otolaryngol. Head Neck Surg. 2018, 159, 178–184. [Google Scholar] [CrossRef]
- Madani, S.A.; Hashemi, S.A.; Morshedzadeh, S.A. Results of Functional Endoscopic Sinus Surgery in Patients with Mucosal Contact Points Suffering from Chronic Daily Headache Non-Responding to Medications. Acta Fac. Med. Naissensis 2013, 30, 159–164. [Google Scholar] [CrossRef] [Green Version]
- Marzetti, A.; Mazzone, S.; Tedaldi, M.; Topazio, D.; Passali, F.M. The Role of Balloon Sinuplasty in the Treatment of Vacuum Rhinogenic Headache. Indian J. Otolaryngol. Head Neck Surg. 2017, 69, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Parsons, D.S.; Batra, P.S. Functional Endoscopic Sinus Surgical Outcomes for Contact Point Headaches. Laryngoscope 1998, 108, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Sanges, G.; Feleppa, M.; Gamerra, M.; Sorrentino, G.; Luca, R.; Merone, M.; Cacace, L.; Bigal, M.E. Fronto-Turbinalis Sinus Expansion and Headache. Curr. Pain Headache Rep. 2011, 15, 308–313. [Google Scholar] [CrossRef]
- Segana, H.A.C.; Nair, R.; Shah, F.A. Endoscopic Solution to Rhinogenic Contact Headaches. Bengal J. Otolaryngol. Head Neck Surg. 2016, 24, 60–67. [Google Scholar] [CrossRef]
- Stammberger, H.; Wolf, G. Headaches and Sinus Disease: The Endoscopic Approach. Ann. Otol. Rhinol. Laryngol. 1988, 97, 3–23. [Google Scholar] [CrossRef]
- Wang, J.; Yin, J.-S.; Peng, H. Investigation of Diagnosis and Surgical Treatment of Mucosal Contact Point Headache. Ear Nose Throat J. 2016, 95, E39–E44. [Google Scholar]
- Wang, J.; Yin, J.; Peng, H. Diagnosis and Surgical Treatment of Mucosal Contact Point Headache: Mucosal Contact Point Headache May Not Be Accurately Diagnosed before Surgery. SM Otolaryngol. 2017, 1, 1003. [Google Scholar] [CrossRef]
- Yarmohammadi, M.E.; Ghasemi, H.; Pourfarzam, S.; Nadoushan, M.R.J.; Majd, S.A. Effect of Turbinoplasty in Concha Bullosa Induced Rhinogenic Headache, a Randomized Clinical Trial. J. Res. Med. Sci. 2012, 17, 229–234. [Google Scholar]


{kind=link}
| Patient Selection | Evaluation of the Entire Study Group | Rhinosinusitis Excluded? | Female/Male (%) | Age | No. of Participants | Migraine (incl. Probable Migraine) (%) | TTH (%) | TACs (%) | Rhinogenic (%) | Other or Unspecified (%) | Bias Risk | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [18] | ENT clinic | N − ENT + CT+, NE+ | No | 69/31 | 16–56 | 409 | 12 | 42 * | 6 | 19 | 21 | Moderate |
| [19] | ENT clinic | N + ENT + CT +, NE+ | Yes | 78/22 | 22–85 | 75 | 37 | 12 | - | - | 51 | Moderate |
| [20] | ENT clinic | N − ENT + CT +, NE+ | n/a | n/a | n/a | 69 | 30 | 3 | 1 | 48 | 18 | High |
| [17] | Headache clinic | N + ENT − CT −, NE− | Yes | 77/23 | 18–65 | 2991 | 88 | 8 | - | - | 4 | Moderate |
| [3] | General population | N + ENT − CT −, NE− | No | 78/22 | 18–81 | 100 | 86 | - | 2 | 3 | 9 | Low |
| [21] | ENT clinic | N − ENT + CT +, NE− | No | n/a | n/a | 35 | 74 | n/a | n/a | n/a | 26 | Moderate |
| [22] | N clinic | N + ENT − CT −, NE− | No | 54/46 | 4–16 | 87 | 77 | 19 | - | 2 | 2 | Moderate |
| [16] | ENT clinic | N + ENT + CT +, NE− | Yes | 62/38 | 10–65 | 58 | 68 | 27 | - | 5 | - | Moderate |
| [23] | ENT clinic | N − ENT+ CT +, NE+ | Yes | 72/28 | 17–63 | 103 | 62 | 25 | 11 | - | 3 | Moderate |
| [24] | ENT clinic | N + ENT + CT +, NE+ | Yes | 67/33 | n/a | 46 | 65 | 15 | - | - | 20 | Moderate |
| Type of Intervention | Study Design | Group Selection | No. of Participants (with Intention to Treat) | Rhinosinusitis Patients Excluded? | Female/Male (%) | Age | Outcome | |
|---|---|---|---|---|---|---|---|---|
| [1] | Sumatriptan 50 mg p.o. | Case series | General population | 37 (47) | Yes | n/a | n/a | Significant reduction of headache in 100% of moderate/severe attacks |
| [39] | Eletriptan 40 mg p.o. | Case series | ENT clinic | 38 (55) | Yes | 67/33 | 23–70 (median 39) | Significant reduction of headache in 81.6% of attacks |
| [38] | Sumatriptan 50 mg p.o. | Randomized double-blind placebo controlled | n/a | 213 (215) | Yes | 70/30 | 18–70 (median 42) | Significant reduction of headache in 69% vs. 47% (p < 0.001) of patients |
| [41] | Eletriptan p.o. (dose n/a) | Retrospective case-control study | ENT clinic | 29 (67) | No | 55/45 | 18–81 (mean 49) | Resolution of headache in 82.8% of CRS migraine subjects (no significant difference with control group of migraineurs without CRS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Straburzyński, M.; Gryglas-Dworak, A.; Nowaczewska, M.; Brożek-Mądry, E.; Martelletti, P. Etiology of ‘Sinus Headache’—Moving the Focus from Rhinology to Neurology. A Systematic Review. Brain Sci. 2021, 11, 79. https://doi.org/10.3390/brainsci11010079
Straburzyński M, Gryglas-Dworak A, Nowaczewska M, Brożek-Mądry E, Martelletti P. Etiology of ‘Sinus Headache’—Moving the Focus from Rhinology to Neurology. A Systematic Review. Brain Sciences. 2021; 11(1):79. https://doi.org/10.3390/brainsci11010079
Chicago/Turabian StyleStraburzyński, Marcin, Anna Gryglas-Dworak, Magdalena Nowaczewska, Eliza Brożek-Mądry, and Paolo Martelletti. 2021. "Etiology of ‘Sinus Headache’—Moving the Focus from Rhinology to Neurology. A Systematic Review" Brain Sciences 11, no. 1: 79. https://doi.org/10.3390/brainsci11010079