Hypoglycemic Effect of Resveratrol: A Systematic Review and Meta-Analysis


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Outcomes
- -
- Serum glucose and insulin levels;
- -
- HbA1c percentage;
- -
- HOMA-IR value.
2.5. Data Extraction
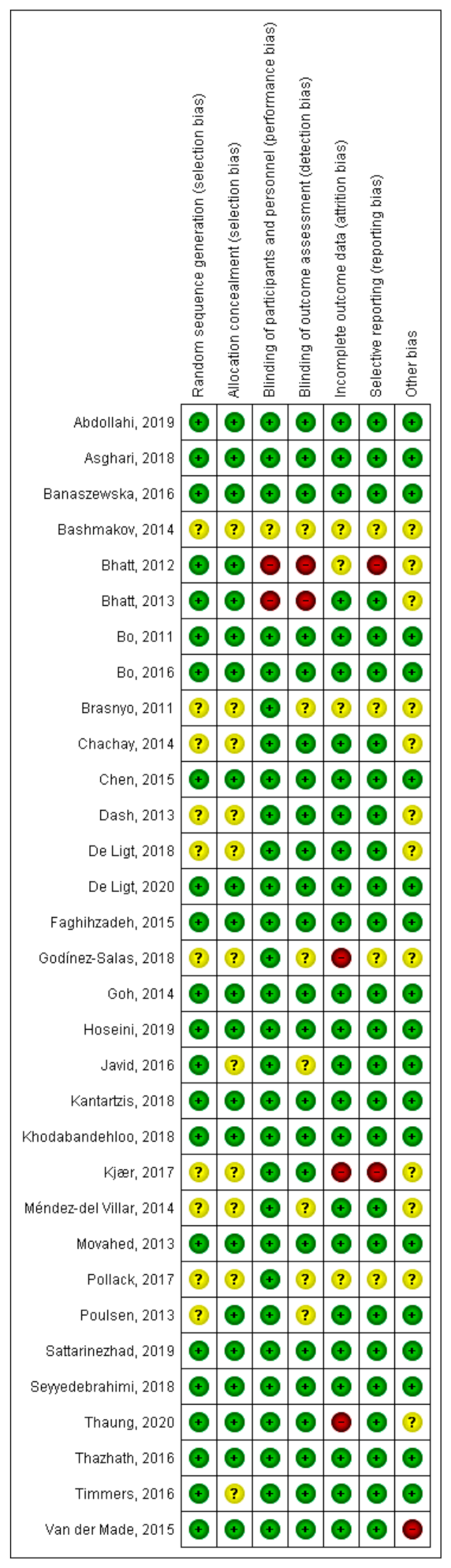
2.6. Assessment of Risk of Bias and Quality of Studies
2.7. Statistical Analysis
3. Results
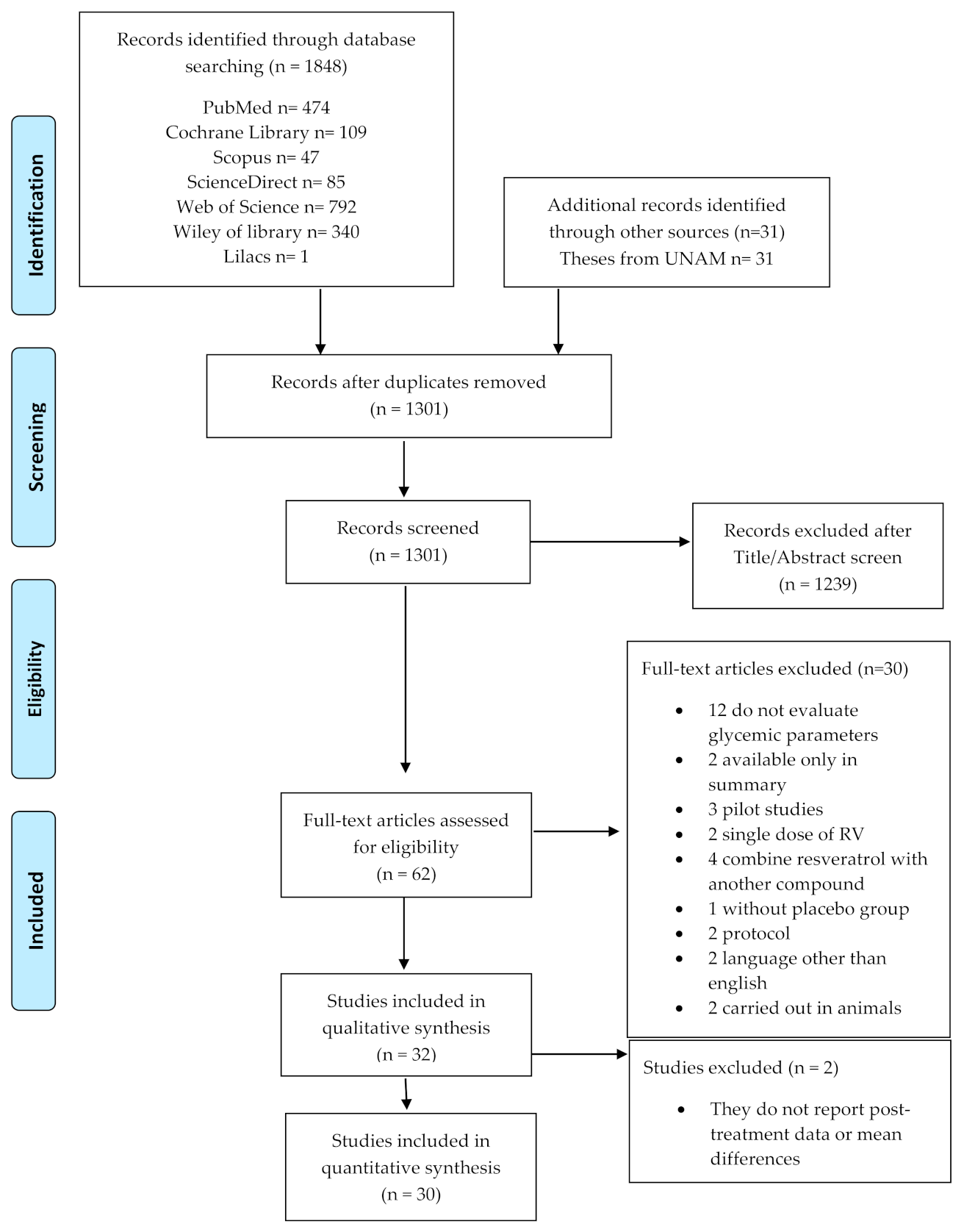
3.1. Literature Search
3.2. Study Characteristics
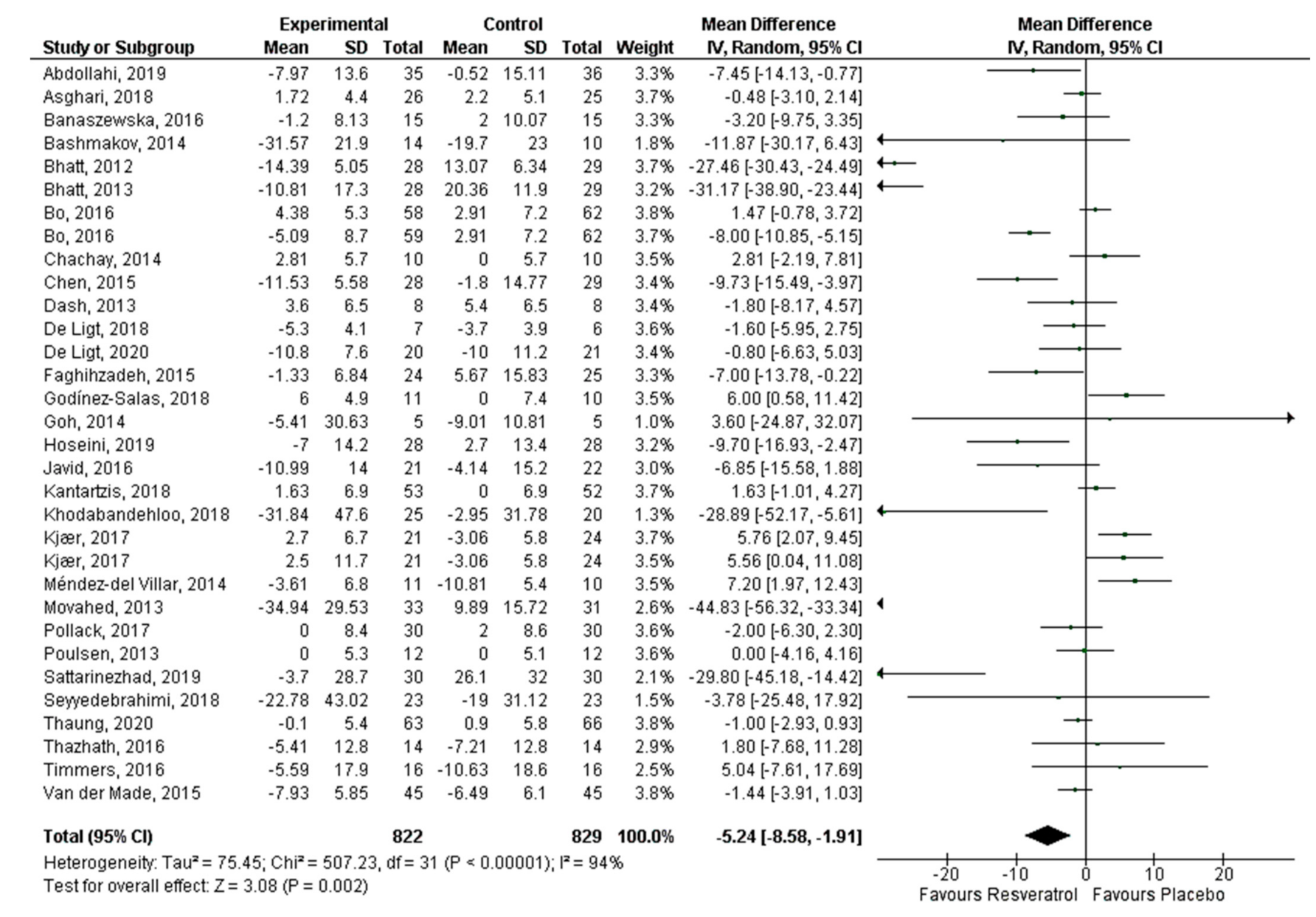
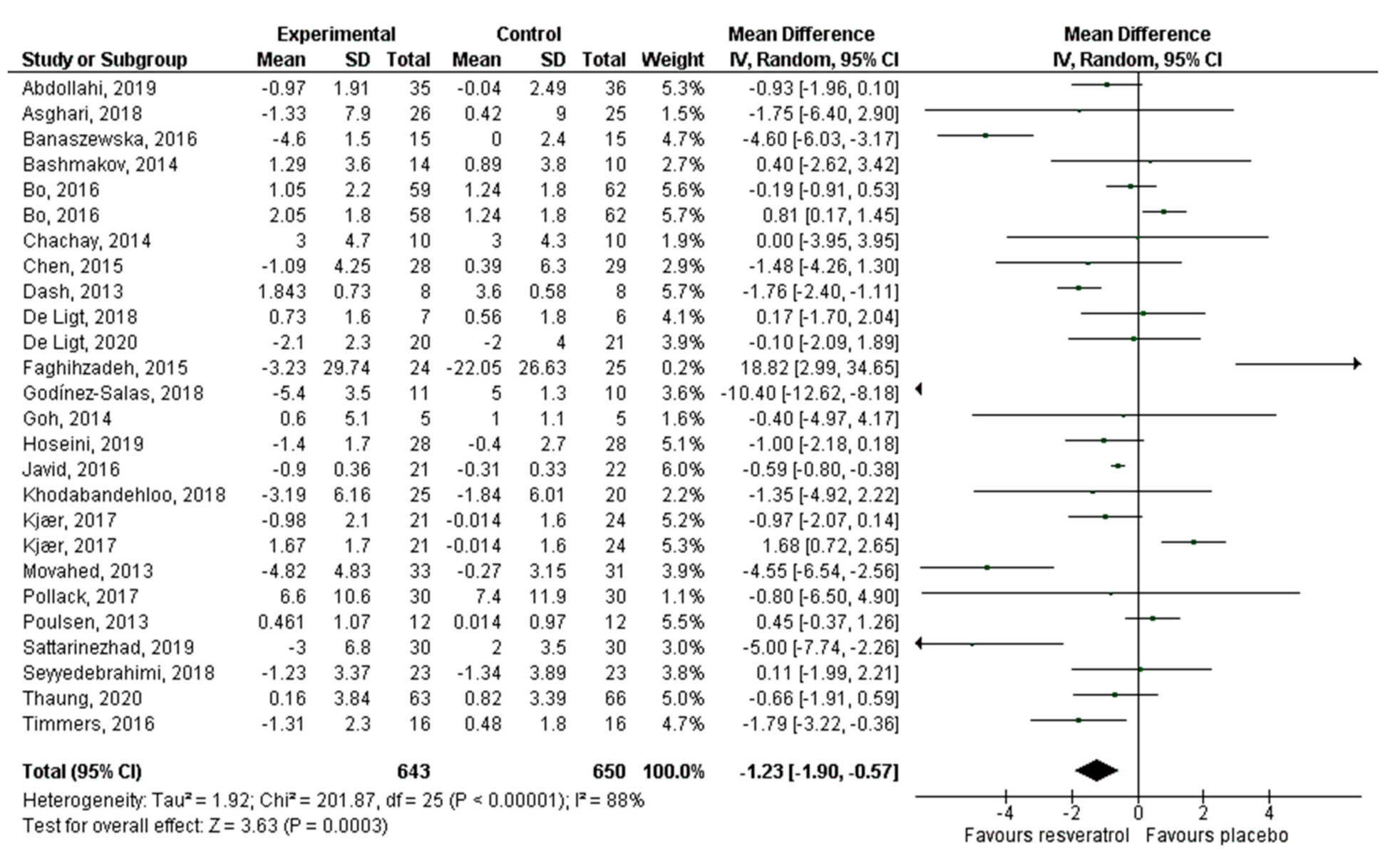
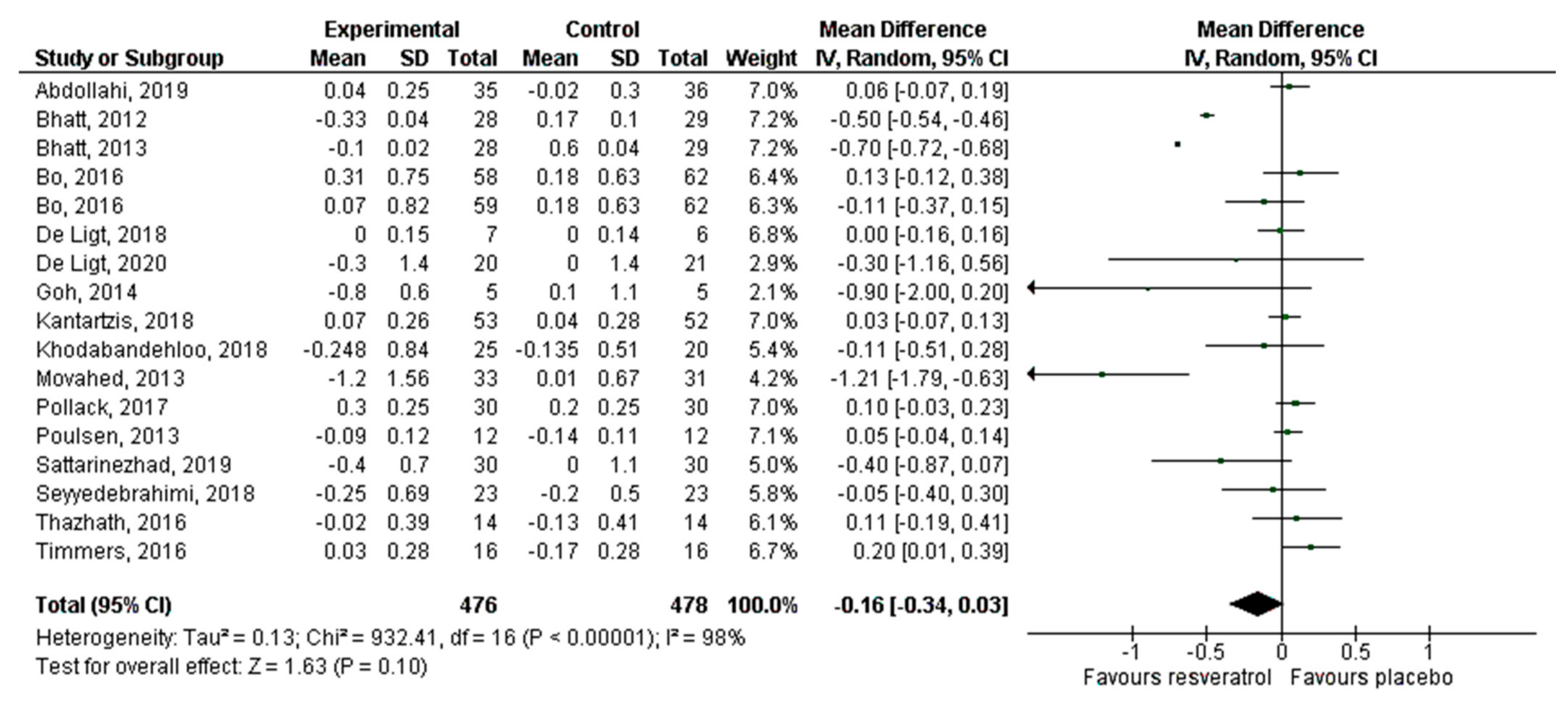
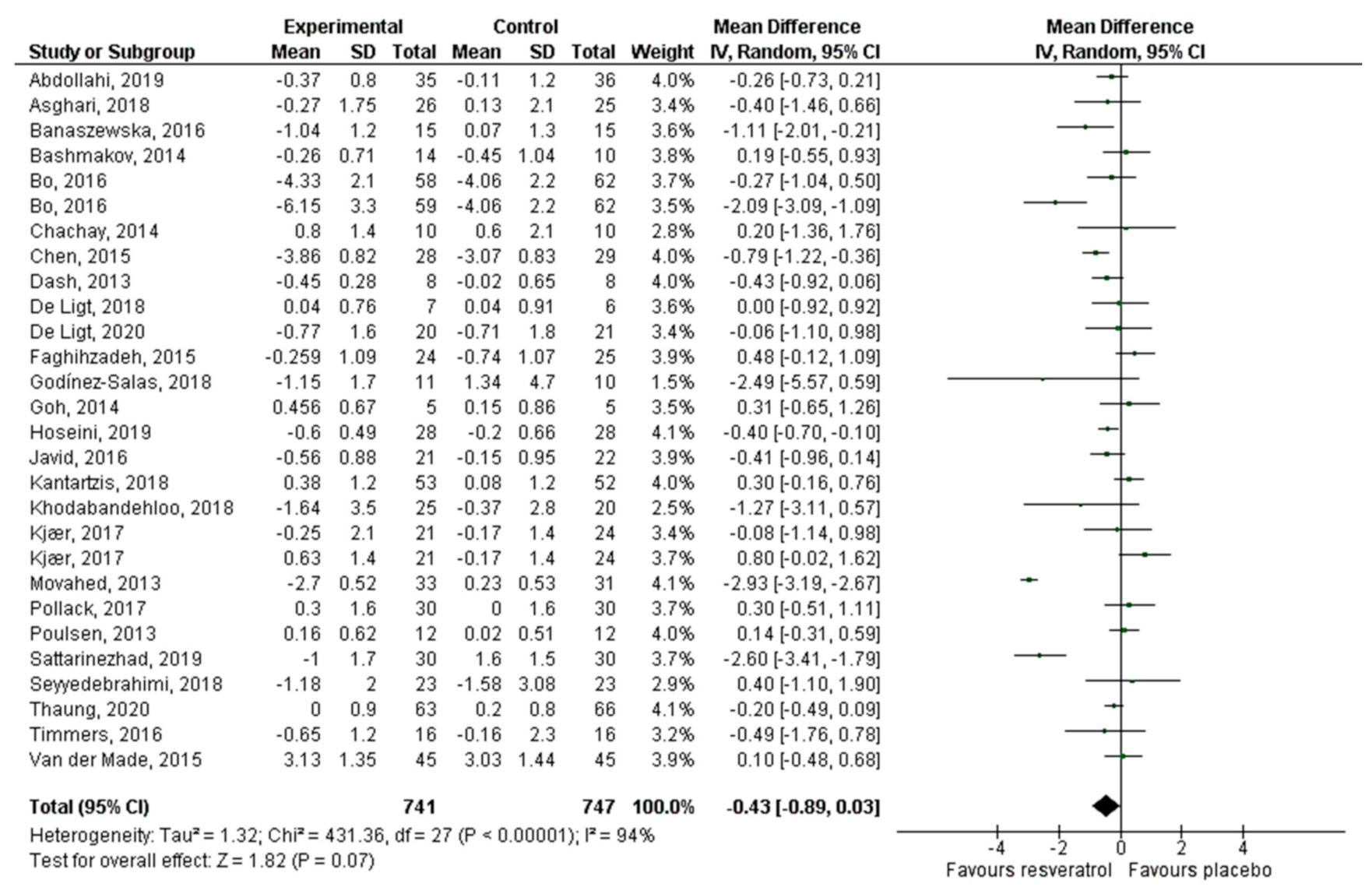
3.3. Meta-Analysis
4. Discussion
4.1. Sub-Analysis by RV Dosage
4.2. Sub-Analysis by Health Condition
- Increases the expression of GLUT4 (an insulin-dependent glucose transporter) and improves glucose uptake;
- Activation of SIRT1, which modulates different metabolic pathways, as follows: (i) It deacetylates the FOXO 1 protein, inhibiting its activity and suppressing the apoptosis of pancreatic β cells; (ii) it reduces the expression of the nuclear factor kappa β, which translates into a decrease in the activity of inflammation markers and oxidative stress, responsible for the production of advanced glycation end products (AGE); (iii) it activates AMPK, which regulates various intracellular processes, such as energy metabolism, mitochondrial functions, and cellular homeostasis. AMPK inactivity is correlated with insulin resistance and tissue damage caused by hyperglycemia; and (iv) it activates FOXO 3 expression, thereby suppressing the production of reactive oxygen species and improving regulation in manganese superoxide dismutase (MnSOD) expression;
- Decreases the expression of the AGE receptor (RAGE) that contributes to insulin resistance by modifying its receptor proteins, by phosphorylating the serine/threonine segment, causing insulin resistance. Therefore, the decrease in the production and activity of AGE improves insulin signaling;
- Activation of factor Nrf2, which is a transcription factor that coordinates the activation of a wide range of genes of antioxidant systems, thereby increasing the activity of the antioxidant enzymes glutathione peroxidase (GPx), glutathione reductase (GR), superoxide dismutase (SOD), and catalase.
4.3. Sub-Analysis by Duration of Intervention
4.4. Sub-Analysis by Age
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Studies Excluded from the Systematic Review and Meta-Analysis
| Study | Reason for Exclusion |
| Abdollahi, et al. BMJ. 2019;9:e026337, doi:10.1136/ bmjopen-2018-026337 | It is a protocol |
| Asghari, et al. Adv Phar Bull. 2018, 8(2), 307–317, doi:10.15171/apb.2018.036 | They do not evaluate glycemic parameters |
| Bo, et al. Acta Diabetol. 2018;55:331–3402018, doi:10.1007/s00592-017-1097-4 | They do not report pre- and post-treatment means of glycemic parameters |
| Brenjian, et al. Am J Reprod Immunol. 2020;83:e13186, doi:10.1111/aji.13186 | They do not evaluate glycemic parameters |
| Cao, et al. Exp Ther Med. 2018; 15: 576–584, doi:10.3892/etm.2017.5400 | They do not evaluate glycemic parameters |
| Crandall, et al. J Gerontol A Biol Sci Med Sci. 2012;67:1307–1312, doi:10.1093/gerona/glr235 | It is a pilot study |
| Foroghi, et al. IJEM. 2018;20:169-176. | Language other than English |
| Gospin, et al. J Investig Med 2016;64:800–825, doi:1 0.1136/jim-2016-000080.35 | Only abstract available |
| Huhn, et al. 2018. NeuroImage Doi:10.1016/j.neuroimage.2018.03.023 | They use a combination of resveratrol with quercetin |
| Kjaer, et al. The Prostate. 2015;75:1255–1263, doi:10.1002/pros.23006 | They do not evaluate glycemic parameters |
| Knop, et al. Diabet Med. 2013;61:1886 Doi:10.1111/dme.12231 | They do not evaluate glycemic parameters |
| Köbe, et al. Front. Neurosci. 2017. 11:105. Doi:10.3389/fnins.2017.00105 | They use a combination of resveratrol with quercetin |
| Konings, et al. Int J Obes. 2014;38:470–473. Doi:10.1038/ijo.2013.155 | They do not evaluate glycemic parameters |
| Korsholm, et al. Int. J. Mol. Sci. 2017, 18, 554; doi:10.3390/ijms18030554 | They do not evaluate glycemic parameters |
| Maginley, et al. J Investig Med. 2019;67:793, doi:10.1136/jim-2019-001036.20 | Only abstract available |
| Mahmood, et al. J. Pharm Sci Res. 2018;10(5):999–1005. | They do not evaluate glycemic parameters |
| Milton-Laskibar, et al. IUBMB. 2016, doi:10.1002/biof.1347 | Study carried out on animals |
| Most et al. Am J Clin Nutr 2016;104:215–27, doi:10.3945/ajcn.115.122937 | They use a combination of resveratrol with epigallocatechin |
| Ornstrup, et al. J Clin Endocrinol Metab. 2014;99:4720–4729, doi:10.1210/jc.2014-2799 | They do not evaluate glycemic parameters |
| Pankaj, et al. Biochem Bioph Res Co. 2015. 10.1016/j.bbrc.2015.10.126 | Study carried out on animals |
| Poulsen, et al. Diabetes Obes Metab. 2018;20:2504–2509, doi:10.1111/dom.13409 | They do not report pre- and post-treatment means of glycemic parameters |
| Theodotou, et al. Exp Ther Med. 2018; 18: 559–565, doi:10.3892/etm.2019.7607 | The comparison group is not a placebo |
| Van der Made, et al. Nutrients. 2017;9,596, doi:10.3390/nu9060596 | They do not evaluate glycemic parameters |
| Vatavuk-Serrati, et al. Rev Soc Cardiol Estado de São Paulo-Supl-2019;29(1):88–93 | Language other than English |
| Voduc, et al. Appl. Physiol. Nutr. Metab. 2014. 39:1183–1188. Doi.org/10.1139/apnm-2013-0547 | It is a pilot study |
| Walker, et al. J Clin Transl Res. 2019;4:122–135. Doi:10.18053/jctres.04.201802.004 | It is a pilot study |
| Wicklow, et al. Biochem Cell Biol. 2015; 93: 1–9, doi:/10.1139/bcb-2014-01362015 | It is a protocol |
| Witte, et al. J Neurosci. 2014. 4(23):7862–7870, doi:10.1523/JNEURISCI.0385-14.2014 | They use a combination of resveratrol with quercetin |
| Wong, et al. Nutr Metabol Cardiovasc Dis. 2016, doi:10.1016/j.numecd.2016.03.003 | They use a single dose of RV |
| Wong, et al. Nutrients. 2016, 8, 425, doi:10.3390/nu8070425 | They use a single dose of RV |
References
- Koushki, M.; Amiri-Dashatan, N.; Ahmadi, N.; Abbaszadeh, H.; Rezaei-Tavirani, M. Resveratrol: A miraculous natural compound for diseases treatment. Food Sci. Nutr. 2018, 6, 2473–2490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harikumar, K.B.; Aggarwal, B.B. Resveratrol: A multitarget agent for age-associated. Cell Cycle 2008, 7, 1020–1035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catalgol, B.; Batirel, S.; Taga, Y.; Ozer, N.K. Resveratrol: French paradox revisited. Front. Pharmacol. 2012, 3, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopp, P. Resveratrol, a phytoestrogen found in red wine. A possible explanation for the conundrum of the “French paradox”? Eur. J. Endocrinol. 1998, 138, 619–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galiniak, S.; Aebisher, D.; Bartusik-Aebisher, D. Health benefits of resveratrol administration. Acta Biochim. Pol. 2019, 66, 13–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gambini, I.; Inglés, M.; Olaso, G.; López-Grueso, R.; Bonet-Costa, V.; Gimeno-Mallench, L.; Mas-Bargues, C.; Abdelaziz, K.M.; Gomez-Cabrera, M.C.; Vina, J.; et al. Properties of resveratrol: In vitro and in vivo studies about metabolism, bioavailability and biological effects in animal models and humans. Oxid Med. Cell Longev. 2015, 837042. [Google Scholar] [CrossRef] [Green Version]
- Britton, R.; Kovoor, C.; Brown, K. Direct molecular targets of resveratrol: Identifying key interactions to unlock complex mechanisms. Ann. N. Y. Acad. Sci. 2015, 1348, 124–133. [Google Scholar] [CrossRef]
- Kulkarni, S.S.; Cantó, C. The molecular targets of resveratrol. Biochim. Biophys. Acta 2015, 1852, 1114–1123. [Google Scholar] [CrossRef] [Green Version]
- Rauf, A.; Imran, M.; Rasul, H.; Ahmad, B.; Peters, D.; Mubarak, M. A comprehensive review of the health perspectives of resveratrol. Food Funct. 2017, 8, 4284–4305. [Google Scholar] [CrossRef]
- Tomé-Carneiro, J.; Larrosa, M.; González-Sarrías, A.; Tomás-Barberán, F.; García-Conesa, M.; Espín, J.C. Resveratrol and clinical trials: The crossroad from in vitro studies to human evidence. Curr. Pharm. Des. 2013, 19, 6064–6093. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, O.; Muñoz, R.; Bustamante, S. Pharmacological properties of resveratrol. A pre-clinical and clinical review. Biochem. Pharmacol. 2015, 4, 5. [Google Scholar] [CrossRef]
- Ramírez-Garza, S.L.; Laveriano-Santos, E.P.; Marhuenda-Muñoz, M.; Storniolo, C.E.; Tresserra-Rimbau, A.; Vallverdú-Queralt, A.; Lamuela-Raventós, R.M. Health effects of resveratrol: Results from human intervention trials. Nutrients 2018, 10, 1892. [Google Scholar] [CrossRef] [Green Version]
- Berman, A.Y.; Motechin, R.A.; Wiesenfeld, M.Y.; Holz, M.K. The therapeutic potential of resveratrol: A review of clinical trials. NPJ Precis. Oncol. 2017, 1, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sergi, C.; Chiu, B.; Feulefack, J.; Shen, F.; Chiu, B. Usefulness of resveratrol supplementation in decreasing cardiometabolic risk factors comparing subjects with metabolic syndrome and healthy subjects with or without obesity: Meta-analysis using multinational, randomised, controlled trials. Arch. Med. Sci. Atheroscler. Dis. 2020, 5, e98–e111. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Yue, H.; Jia, M.; Liu, W.; Qiu, B.; Hou, H.; Huang, F.; Xu, T. Effect of low-ratio n-6/n-3 PUFA on blood glucose: A meta-analysis. Food Funct. 2019, 10, 4557–4565. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Metodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdollahi, S.; Salehi-Abargouei, A.; Toupchian, O.; Sheikhha, M.H.; Fallahzadeh, H.; Rahmanian, M.; Tabatabaie, M.; Mozaffari-Khosravi, H. The effect of resveratrol supplementation on cardio-metabolic risk factors in patients with type 2 diabetes: A randomized, double-blind controlled trial. Phytother. Res. 2019, 33, 3153–3162. [Google Scholar] [CrossRef]
- Ashgari, S.; Ashgari-Jafarabadi, M.; Mohammad-Hossein, S.; Seyed-Mostafa, G.; Rafraf, M. Comparison of calorie-restricted diet and resveratrol supplementation on anthropometric indices, metabolic parameters, and serum sirtuin-1 levels in patients with nonalcoholic fatty liver disease: A randomized controlled clinical trial. J. Am. Coll. Nutr. 2018, 37, 223–233. [Google Scholar] [CrossRef]
- Banaszewska, B.; Wrotynska-Barczynska, J.; Spaczynski, R.Z.; Pawelczyk, L.; Duleba, A.J. Effects of resveratrol on polycystic ovary syndrome: A double-blind, randomized, placebo-controlled trial. J. Clin. Endocrinol. Metab. 2016, 101, 4322–4328. [Google Scholar] [CrossRef]
- Bashmakov, Y.K.; Assaad-Khalil, S.H.; Abou, M.; Udumyan, R.; Megallaa, M.; Rohoma, K.H.; Zeitoun, M.; Petyaev1, I.M. Resveratrol promotes foot ulcer size reduction in type 2 diabetes patients. ISRN Endocrinol. 2014, 2014, 816307. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, J.K.; Thomas, S.; Nanjan, M.J. Resveratrol supplementation improves glycemic control in type 2 diabetes mellitus. Nutr. Res. 2012, 32, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, J.K.; Nanjan, M.J. Resveratrol supplementation in patients with type 2 diabetes mellitus: A prospective, open label, randomized controlled trial. Int. Res. J. Pharm. 2013, 4, 45–249. [Google Scholar] [CrossRef]
- Bo, S.; Ponzo, V.; Ciccone, G.; Evangelista, A.; Saba, F.; Goitre, I.; Procopio, M.; Pagano, G.F.; Cassader, M.; Gambino, R. Six months of resveratrol supplementation has no measurable effect in type 2 diabetic patients. A randomized, double blind, placebo-controlled trial. Pharmacol. Res. 2016, 111, 896–905. [Google Scholar] [CrossRef]
- Bo, S.; Ciccone, G.; Castiglione, A.; Gambino, R.; De Michieli, F.; Villois, D.P.M.; Cavallo-Perin, P.; Cassader, M. Anti-inflammatory and antioxidant effects of resveratrol in healthy smokers. A randomized, double-blind, placebo-controlled, cross-over trial. Curr. Med. Chem. 2011, 20, 1323–1331. [Google Scholar] [CrossRef]
- Brasnyó, P.; Molnár, G.; Mohás, M.; Markó, L.; Laczy, B.; Cseh, J.; Mikolás, J.; Mikolás, I.A.; Mérei, A.; Halmai, R. Resveratrol improves insulin sensitivity, reduces oxidative stress and activates the Akt pathway in type 2 diabetic patients. Br. J. Nutr. 2011, 106, 383–389. [Google Scholar] [CrossRef] [Green Version]
- Chachay, V.S.; Macdonald, G.; Martin, J.H.; Whitehead, J.P.; O’Moore-Sullivan, T.; Lee, P.; Franklin, M.; Klein, K.; Taylor, P.; Ferguson, M. Resveratrol does not benefit patients with nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2014, 12, 2092–2103. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Zhao, X.; Ran, L.; Wan, J.; Wang, X.; Qin, Y.; Shu, F.; Gao, Y.; Yuan, L.; Zhang, Q. Resveratrol improves insulin resistance, glucose and lipid metabolism in patients with non-alcoholic fatty liver disease: A randomized controlled trial. Dig. Liver Dis. 2015, 47, 226–232. [Google Scholar] [CrossRef]
- Dash, S.; Xiao, C.; Morgantini, C.; Szeto, L.; Lewis, G.F. High-dose resveratrol treatment for 2 weeks inhibits intestinal and hepatic lipoprotein production in overweight/obese men. Arterioscler. Thromb. Vasc. Biol. 2013, 3312, 2895–2901. [Google Scholar] [CrossRef] [Green Version]
- De Ligt, M.; Bergman, M.; Mancilla, R.; Essers, H.; Moonen-Kornips, E.; Havekes, B.; Schrauwen-Hinderling, V.; Schrauwen, P. No effect of resveratrol supplementation after 6 months on insulin sensitivity in overweight adults: A randomized trial. Am. J. Clin. Nutr. 2020, 112, 1029–1038. [Google Scholar] [CrossRef]
- De Ligt, M.; Bruls, Y.; Hansen, J.; Habets, M.F.; Havekes, B.; Nascimento, E.; Moonen-Kornips, E.; Schaart, G.; Schrauwen-Hinderling, V.; Lichtenbelt, W.; et al. Resveratrol improves ex vivo mitochondrial function but does not insulin sensitivity or brown adipose tissue in first degree relatives of patients with type 2 diabetes. Mol. Metab. 2018, 12, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Faghihzadeh, F.; Adibi, P.; Hekmatdoost, A. The effects of resveratrol supplementation on cardiovascular risk factors in patients with non-alcoholic fatty liver disease: A randomised, double-blind, placebo-controlled study. Br. J. Nutr. 2015, 114, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Godínez-Salas, E.T.; Guevara-Cruz, M.; Villanueva-Luna, P.; Del Rocío Guizar-Heredia, M.; Torres, V.G.; Pichardo, O.E.; Nava, G.; Villalvazo, I.; Torres, N.; Tovar, A. Effect of the bioactive compounds genistein and resveratrol on insulin resistance in patients with metabolic síndrome. FASEB J. 2017, 31. [Google Scholar] [CrossRef]
- Goh, K.P.; Lee, H.Y.; Lau, D.P.; Supaat, W.; Chan, Y.H.; Yung, A.F. Effects of resveratrol in patients with type 2 diabetes mellitus on skeletal muscle SIRT1 expression and energy expenditure. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Hoseini, A.; Namazi, G.; Farrokhian, A.; Reiner, Z.; Aghadavod, E.; Bahmania, F.; Asemi, Z. The effects of resveratrol on metabolic status in patients with type 2 diabetes mellitus and coronary heart disease. Food Funct. 2019, 10, 6042–6051. [Google Scholar] [CrossRef]
- Javid, A.Z.; Hormoznejad, R.; Yousefimanesh, H.A.; Zakerkish, M.; Haghighi-zadeh, M.H.; Dehghan, P.; Ravanbakhsh, M. The impact of resveratrol supplementation on blood glucose, insulin, insulin resistance, triglyceride, and periodontal markers in type 2 diabetic patients with chronic periodontitis. Phytother. Res. 2017, 31, 108–114. [Google Scholar] [CrossRef]
- Kantartzis, K.; Fritsche, L.; Bombrich, M.; Machann, J.; Schick, F.; Staiger, H.; Kunz, I.; Schoop, R.; Lehn-Stefan, A.; Heni, M.; et al. Effects of resveratrol supplementation on liver fat content in overweight and insulin-resistant subjects: A randomized, double-blind, placebo-controlled clinical trial. Diabetes Obes. Metab. 2018, 20, 1793–1797. [Google Scholar] [CrossRef]
- Khodabandehloo, H.; Seyyedebrahimi, S.; Esfahani, E.N.; Razi, F.; Meshkani, R. Resveratrol supplementation decreases blood glucose without changing the circulating CD14+ CD16+ monocytes and inflammatory cytokines in patients with type 2 diabetes: A randomized, double-blind, placebo-controlled study. Nutr. Res. 2018, 54, 40–51. [Google Scholar] [CrossRef]
- Kjær, T.N.; Ornstrup, M.J.; Poulsen, M.M.; Stødkilde-Jørgensen, H.; Jessen, N.; Lunde, J.J.; Richelsen, B.; Pedersen, S. No beneficial effects of resveratrol on the metabolic syndrome: A randomized placebo-controlled clinical trial. J. Clin. Endocrinol. Metab. 2017, 102, 1642–1651. [Google Scholar] [CrossRef] [Green Version]
- Méndez-del Villar, M.; González-Ortiz, M.; Martínez-Abundis, E.; Pérez-Rubio, K.G.; Lizárraga-Valdez, R. Effect of resveratrol administration on metabolic syndrome, insulin sensitivity and insulin secretion. Metab. Syndr. Relat. Disord. 2014, 12, 497–502. [Google Scholar] [CrossRef]
- Movahed, A.; Nabipour, I.; Lieben, X.L.; Thandapilly, S.J.; Yu, L.; Kalantarhormozi, M.; Rekabpour, S.; Netticadan, T. Antihyperglycemic effects of short-term resveratrol supplementation in type 2 diabetic patients. Evid. Based Complement. Alternat. Med. 2013, 2013, 851267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollack, R.M.; Barzilai, N.; Anghel, V.; Kulkarni, A.S.; Golden, A.; O’Broin, P.; Sinclair, D.; Bonkowski, M.; Coleville, A.; Powell, D.; et al. Resveratrol improves vascular function and mitochondrial number but not glucose metabolism in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1703–1709. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, M.M.; Vestergaard, P.F.; Clasen, B.F.; Radko, Y.; Christensen, L.P.; Stødkilde-Jørgensen, H.; Møller, N.; Jessen, N.; Pedersen, S.; Jørgensen, J.O.L. High-dose resveratrol supplementation in obese men. An investigator-initiated, randomized, placebo-controlled clinical trial of substrate metabolism, insulin sensitivity, and body composition. Diabetes 2013, 62, 1186–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sattarinezhad, A.; Roozbeh, J.; Yeganeh, S.; Omrani, G.; Shams, M. Resveratrol reduces albuminuria in diabetic nephropathy: A randomized double-blind placebo-controlled clinical trial. Diabetes Metab. 2019, 45, 53–59. [Google Scholar] [CrossRef]
- Seyyedebrahimi, S.; Khodabandehloo, H.; Esfahani, E.N.; Meshkani, R. The effects of resveratrol on markers of oxidative stress in patients with type 2 diabetes: A randomized, double-blind, placebo-controlled clinical trial. Acta Diabetol. 2018, 55, 341–353. [Google Scholar] [CrossRef]
- Thaung, J.; Rowe, P.; Wong, R. Sustained cerebrovascular and cognitive benefits of resveratrol in postmenopausal women. Nutrients 2020, 12, 828. [Google Scholar] [CrossRef] [Green Version]
- Thazhath, S.S.; Wu, T.; Bound, M.J.; Checklin, H.L.; Standfield, S.; Jones, K.L.; Horowitz, M.; Rayner, C.K. Administration of resveratrol for 5 wk has no effect on glucagon-like peptide 1 secretion, gastric emptying, or glycemic control in type 2 diabetes: A randomized controlled trial. Am. J. Clin. Nutr. 2016, 103, 66–70. [Google Scholar] [CrossRef]
- Timmers, S.; De Ligt, M.; Phielix, E.; Van de Weijer, T.; Hansen, J.; Moonen-Kornips, E.; Schaart, G.; Kunz, I.; Hesselink, M.; Hinderling, V.; et al. Resveratrol as add-on therapy in subjects with well-controlled type 2 diabetes: A randomized controlled trial. Diabetes Care 2016, 19, 2211–2217. [Google Scholar] [CrossRef] [Green Version]
- Van der Made, S.M.; Plat, J.; Mensink, R.P. Resveratrol does not influence metabolic risk markers related to cardiovascular health in overweight and slightly obese subjects: A randomized, placebo-controlled crossover trial. PLoS ONE 2015, 10, e0118393. [Google Scholar] [CrossRef] [Green Version]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity and Severe Obesity among Adults: United States, 2017–2018; NCHS data brief, no 360; National Center for Health Statistics: Hyattsville, MD, USA, 2020. [Google Scholar]
- Midway National Health and Nutrition Survey 2016. Final Results Report. Health: History of Chronic Diseases. Mexico. 2016. Available online: https://www.gob.mx/ENSANUT (accessed on 15 October 2020).
- Padwal, R.S. Obesity, diabetes, and the metabolic syndrome: The global scourge. Can. J. Cardiol. 2014, 30, 467–472. [Google Scholar] [CrossRef]
- Engin, A.B. What is lipotoxicity? In Obesity and Lipotoxicity; AEMB: Cham, Switzerland, 2017; Volume 960, pp. 197–220. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Noncommunicable Diseases 2014; World Health Organization: Geneva, Switzerland, 2014; Available online: https://www.who.int/nmh/publications/ncd-status-report-2014/en/ (accessed on 12 October 2020).
- Balakumar, P.; Maung-U, K.; Jagadeesh, G. Prevalence and prevention of cardiovascular disease and diabetes mellitus. Pharmacol. Res. 2016, 113, 600–609. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan for the Prevention and Control of NCDs 2013–2020; World Health Organization: Geneva, Switzerland, 2013; Available online: https://www.who.int/publications/i/item/9789241506236 (accessed on 12 October 2020).
- Kontis, V.; Mathers, C.D.; Rehm, J.; Stevens, G.A.; Shield, K.D.; Bonita, R.; Ezzati, M. Contribution of six risk factors to achieving the 25×25 non-communicable disease mortality reduction target: A modelling study. Lancet. 2014, 384, 427–437. [Google Scholar] [CrossRef]
- Cione, E.; La Torre, C.; Cannataro, R.; Caroleo, M.C.; Plastina, P.; Gallelli, L. Quercetin, epigallocatechin gallate, curcumin, and resveratrol: From dietary sources to human microRNA modulation. Molecules 2020, 25, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janabi, A.H.W.; Kamboh, A.A.; Saeed, M.; Xiaoyu, L.; BiBi, J.; Majeed, F.; Naveed, M.; Mughal, M.; Korejo, N.; Kamboh, R.; et al. Flavonoid-rich foods (FRF): A promising nutraceutical approach against lifespan-shortening diseases. Iran. J. Basic Med. Sci. 2020, 23, 140. [Google Scholar] [CrossRef]
- Gollucke, A.P.; Peres, R.C.; Odair, A.; Ribeiro, D.A. Polyphenols: A nutraceutical approach against diseases. Recent Pat. Food Nutr Agric. 2013, 5, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Fujitaka, K.; Otani, H.; Jo, F.; Jo, H.; Nomura, E.; Iwasaki, M.; Nishikawa, M.; Iwasaka, T.; Das, D.K. Modified resveratrol Longevinex improves endothelial function in adults with metabolic syndrome receiving standard treatment. Nutr. Res. 2011, 31, 842–847. [Google Scholar] [CrossRef]
- Magyar, K.; Halmosi, R.; Palfi, A.; Feher, G.; Czopf, L.; Fulop, A.; Szabados, E. Cardioprotection by resveratrol: A human clinical trial in patients with stable coronary artery disease. Clin. Hemorheol. Microcirc. 2012, 50, 179–187. [Google Scholar] [CrossRef]
- Patel, K.R.; Brown, V.A.; Jones, D.J.; Britton, R.G.; Hemingway, D.; Miller, A.S.; Brenner, D.E. Clinical pharmacology of resveratrol and its metabolites in colorectal cancer patients. Cancer Res. 2010, 70, 7392–7399. [Google Scholar] [CrossRef] [Green Version]
- Hausenblas, H.A.; Schoulda, J.A.; Smoliga, J.M. Resveratrol treatment as an adjunct to pharmacological management in type 2 diabetes mellitus—systematic review and meta-analysis. Mol. Nut. Food Res. 2015, 59, 147–159. [Google Scholar] [CrossRef]
- Jeyaraman, M.M.; Al-Yousif, N.S.; Mann, A.S.; Dolinsky, V.W.; Rabbani, R.; Zarychanski, R.; Abou-Setta, A.M. Resveratrol for adults with type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef]
- Welsh, K.J.; Kirkman, M.S.; Sacks, D.B. Role of glycated proteins in the diagnosis and management of diabetes: Research gaps and future directions. Diabetes Care 2016, 39, 1299–1306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, B.; Saxena, A. Surrogate markers of insulin resistance: A review. World J. Diabetes 2010, 1, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Wu, C.; Qiu, S.; Yuan, X.; Li, L. Effects of resveratrol on glucose control and insulin sensitivity in subjects with type 2 diabetes: Systematic review and meta-analysis. Nutr. Metab. 2017, 14, 60. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, E.J.; Mattson, M.P.; Calabrese, V. Resveratrol commonly displays hormesis: Occurrence and biomedical significance. Hum. Exp. Toxicol. 2010, 29, 980–1015. [Google Scholar] [CrossRef]
- Price, N.L.; Gomes, A.P.; Ling, A.J.; Duarte, F.V.; Martin-Montalvo, A.; North, B.J.; Hubbard, B.P. SIRT1 is required for AMPK activation and the beneficial effects of resveratrol on mitochondrial function. Cell Metab. 2012, 15, 675–690. [Google Scholar] [CrossRef] [Green Version]
- Mukherjee, S.; Dudley, J.I.; Das, D.K. Dose-dependency of resveratrol in providing health benefits. Dose Response 2010, 8, 478–500. [Google Scholar] [CrossRef]
- Liu, K.; Zhou, R.; Wang, B.; Mi, M.T. Effect of resveratrol on glucose control and insulin sensitivity: A meta-analysis of 11 randomized controlled trials. Am. J. Clin. Nutr. 2014, 99, 1510–1519. [Google Scholar] [CrossRef] [Green Version]
- Oyenihi, O.R.; Oyenihi, A.B.; Adeyanju, A.A.; Oguntibeju, O.O. Antidiabetic effects of resveratrol: The way forward in its clinical utility. J. Diabetes Res. 2016, 2016, 9737483. [Google Scholar] [CrossRef]
- Chang, C.C.; Chang, C.Y.; Wu, Y.T.; Huang, J.P.; Yen, T.H.; Hung, L.M. Resveratrol retards progression of diabetic nephropathy through modulations of oxidative stress, proinflammatory cytokines, and AMP-activated protein kinase. J. Biomed. Sci. 2011, 18, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Lagouge, M.; Argmann, C.; Gerhart-Hines, Z.; Meziane, H.; Lerin, C.; Daussin, F.; Geny, B. Resveratrol improves mitochondrial function and protects against metabolic disease by activating SIRT1 and PGC-1α. Cell 2006, 127, 1109–1122. [Google Scholar] [CrossRef]
- Juan, M.E.; Vinardell, M.P.; Planas, J.M. The daily oral administration of high doses of trans-resveratrol to rats for 28 days is not harmful. J. Nutr. 2002, 132, 257–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timmers, S.; Konings, E.; Bilet, L.; Houtkooper, R.H.; Van de Weijer, T.; Goossens, G.H.; Moonen-Kornips, E. Calorie restriction-like effects of 30 days of resveratrol supplementation on energy metabolism and metabolic profile in obese humans. Cell Metab. 2011, 14, 612–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, X.F.; Li, J.M.; Tang, J.; Li, D. Effects of resveratrol supplementation on risk factors of non-communicable diseases: A meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2018, 58, 3016–3029. [Google Scholar] [CrossRef] [PubMed]
- Crandall, J.P.; Oram, V.; Trandafirescu, G.; Reid, M.; Kishore, P.; Hawkins, M.; Cohen, H.W.; Barzilai, N. Pilot study of resveratrol in older adults with impaired glucose tolerance. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 1307–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witte, A.V.; Kerti, L.; Margulies, D.S.; Flöel, A. Effects of resveratrol on memory performance, hippocampal functional connectivity, and glucose metabolism in healthy older adults. J. Neurosci. 2014, 34, 7862–7870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walle, T.; Hsieh, F.; DeLegge, M.H.; Oatis, J.E.; Walle, U.K. High absorption but very low bioavailability of oral resveratrol in humans. Drug Metab. Dispos. 2004, 32, 1377–1382. [Google Scholar] [CrossRef] [Green Version]
- Boocock, D.J.; Faust, G.E.; Patel, K.R.; Schinas, A.M.; Brown, V.A.; Ducharme, M.P.; Steward, W.P. Phase I dose escalation pharmacokinetic study in healthy volunteers of resveratrol, a potential cancer chemopreventive agent. Cancer Epidemiol. Biomarkers Prev. 2007, 16, 1246–1252. [Google Scholar] [CrossRef] [Green Version]
- Gambino, R.; Fanni, G.; Togliatto, G.; Ponzo, V.; Goitre, I.; Cassader, M.; Brizzi, M.F. Bo, S. Rs12778366 single nucleotide polymorphism of Sirtuin 1 (SIRT1) and response to resveratrol supplementation in patients with type 2 diabetes mellitus. Acta Diabetol. 2019, 56, 963–966. [Google Scholar] [CrossRef]
- Cao, Y.; Jiang, X.; Ma, H.; Wang, Y.; Xue, P.; Liu, Y. SIRT1 and insulin resistance. J. Diabetes Complicat. 2016, 30, 178–183. [Google Scholar] [CrossRef]
- Ramsey, K.M.; Mills, K.F.; Satoh, A.; Imai, S.I. Age-associated loss of Sirt1-mediated enhancement of glucose-stimulated insulin secretion in beta cell-specific Sirt1-overexpressing (BESTO) mice. Aging Cell 2008, 7, 78–88. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (Year) | Study Design | RV Dosage | Duration | Subjects | Age | Evaluated Parameters | Findings |
|---|---|---|---|---|---|---|---|
| Abdollahi et al. (2019) [18] | RCT double-blind | 1 g/day | 8 weeks | 71 subjects with T2DM and overweight | 50 ± 7 | Glucose and insulin levels, HbA1c, HOMA-IR, HOMA-β, QUICKI | Significant decrease in glucose (p = 0.03) and insulin (p = 0.02), improvement in HOMA-IR (p = 0.01) and QUICKI (p = 0.008). No significant changes in HOMA-β and HbA1c after resveratrol administration |
| Asghari et al. (2018) [19] | RCT double-blind | 600 mg/day | 12 weeks | 75 subjects with fatty liver | 40 ± 7 | Glucose and insulin levels HOMA-IR | Non-significant changes in the glycemic parameters evaluated |
| Banaszewska et al. (2016) [20] | RCT double-blind | 1.5 g/day | 3 months | 30 women with POS | 27 ± 1 | Fasting blood glucose, insulin sensitivity index | Significant decrease in insulin levels (38%, p = 0.007) and increase in the insulin sensitivity index (66%, p = 0.04) |
| Bashmakov et al. (2014) [21] | RCT parallel-blind | 100 mg/day | 2 months | 24 patients with diabetic food | 56 ± 9 | Glucose and insulin levels, HOMA-IR | Tendency of a decrease of glucose levels in both study groups. No changes in insulin levels and HOMA-IR |
| Bhatt et al. (2012) [22] | RCT open-label | 250 mg/day | 3 months | 57 subjects with T2DM | 57 ± 9 | Fasting blood glucose and HbA1c | Significant decrease in HbA1c levels (p < 0.05) after resveratrol administration |
| Bhatt et al. (2013) [23] | RCT open-label | 250 mg/day | 6 months | 57 subjects with T2DM | 57 ± 9 | HbA1c and glucose levels | Non-significant decrease in HbA1c and glucose levels after intervention |
| Bo et al. (2016) [24] | RCT double-blind | 40, 500 mg/day | 6 months | 179 subjects with T2DM | 65 ± 8 | Glucose and insulin levels, HOMA-IR, HbA1c, C-peptide | Non-significant differences between the study groups after intervention |
| Bo et al. (2013) [25] | RCT double-blind crossover | 500 mg/day | 4 weeks | 49 healthy smokers | 35 ± 9 | Glucose and insulin levels HOMA-IR | Non-significant changes after resveratrol intervention |
| Brasnyó et al. (2011) [26] | RCT double-blind | 10 mg/day | 4 weeks | 19 men with T2DM | 55 ± 9 | Insulin levels, HOMA-IR, HOMA-β | No changes in insulin and HOMA-β levels, tendency of a decrease of HOMA-IR in the experimental group |
| Chachay et al. (2014) [27] | RCT double-blind | 3 g/day | 8 weeks | 20 men with NAFLD | 49 ± 12 | HOMA-IR, glucose and insulin levels | Resveratrol did not improve glucose, insulin, and HOMA-IR levels |
| Chen (2015) [28] | RCT double-blind | 600 mg/day | 3 months | 57 subjects with NAFLD | 44 ± 10 | Glucose, insulin, C-peptide and HOMA-IR | Significant decrease in glucose (p = 0.001) and HOMA-IR (p = 0.016). No significant changes in insulin and C-peptide levels |
| Dash et al. (2013) [29] | RCT double-blind crossover | 1–2 g/day | 2 weeks | 8 overweight and obese subjects | 46 ± 3 | Glucose and insulin levels, HOMA-IR | Non-significant changes in evaluated parameters after resveratrol administration |
| De Ligt et al. (2020) [30] | RCT double-blind | 150 mg/day | 6 months | 41 overweight individuals | 62 ± 1 | Glucose and insulin levels, HbA1c | Non-significant differences in glucose and insulin levels. Significant decrease in HbA1c (p = 0.007) after resveratrol administration |
| De Ligt et al. (2018) [31] | RCT double-blind crossover | 150 mg/day | 4 weeks | 13 men at high risk of T2DM | 66 ± 4 | Glucose and insulin levels, HbA1c | Non-significant differences between the study groups after resveratrol administration |
| Faghihzadeh et al. (2015) [32] | RCT double-blind | 500 mg/day | 12 weeks | 50 subjects with NAFLD | 45 ± 10 | Glucose and insulin levels, HOMA-IR, HOMA-β, QUICKI | Non-significant changes after the resveratrol intervention |
| Godínez-Salas et al. (2018) [33] | RCT double-blind | 150 mg/day | 3 months | 42 subjects with MS | 43 ± 1 | Glucose and insulin levels | Non-significant changes in glucose and insulin levels after resveratrol intervention |
| Goh et al. (2014) [34] | RCT double-blind | 3 g/day | 12 weeks | 10 subjects with T2DM | 56 ± 6 | Glucose and insulin levels, HbA1c, HOMA-IR | Tendency of a decrease in HbA1c, no significant changes in insulin sensitivity |
| Hoseini et al. (2019) [35] | RCT double-blind | 500 mg/day | 4 weeks | 56 subjects with T2DM and CD | 62 ± 9 | Glucose and insulin levels, HOMA-IR, QUICKI | Significant decrease in glucose, insulin (p = 0.01), and HOMA-IR (p = 0.001); QUICKI increase (p = 0.02) |
| Javid et al. (2016) [36] | RCT double-blind | 480 mg/day | 4 weeks | 43 subjects with T2DM and CP | 50 ± 8 | Glucose and insulin levels, HOMA-IR | Significant decrease in insulin and HOMA-IR levels (p < 0.05), non-significant decrease in glucose levels after resveratrol intervention |
| Kantartzis et al. (2018) [37] | RCT double-blind | 150 mg/day | 12 weeks | 105 overweight and obese subjects | 48 ± 13 | Fasting blood glucose, HbA1c, HOMA-IR | No significant changes in evaluated parameters |
| Khodabandenlhoo et al. (2018) [38] | RCT double-blind | 800 mg/day | 2 months | 45 subjects with T2DM | 57 ± 9 | Glucose and insulin levels, HbA1c, HOMA-IR, HOMA-β | Significant decrease in glucose levels (p < 0.05) in experimental group. No changes in HbA1c. No significant changes in insulin, HOMA-IR, and HOMA β levels |
| Kjaer et al. (2017) [39] | RCT double-blind | 1,501,000 mg/day | 16 weeks | 66 subjects with MS | 50 ± 1 | Glucose and insulin levels, HOMA-IR | No change in glucose and insulin concentrations, no change in HOMA-IR |
| Méndez-del Villar et al.(2014) [40] | RCT double-blind | 1.5 g/day | 3 months | 21 subjects with MS | 40 ± 5 | AUC of glucose and insulin, insulin index | Significant decrease in insulin AUC and insulin index (p < 0.05) |
| Movahed et al. (2013) [41] | RCT double-blind | 1 g/day | 45 days | 64 subjects with T2DM | 52 ± 7 | Glucose and insulin levels, HOMA-IR, HOMA-β | Significant decrease (p < 0.05) in glucose, insulin, and HbA1c levels. Improvement of HOMA-IR and HOMA β in experimental group |
| Pollack et al. (2017) [42] | RCT double-blindcrossover | 2 g/day | 6 weeks | 30 overweight older adults with impaired glucose tolerance | 67 ± 7 | Glucose and insulin levels, AUC of glucose and insulin, HbA1c, HOMA-IR | No effect of resveratrol on glycemic parameters |
| Poulsen et al. (2013) [43] | RCT double-blind | 500 mg/day | 4 weeks | 24 obese subjects | 39 ± 3 | Glucose and insulin levels, HbA1c, HOMA-IR | No changes in evaluated parameters |
| Sattarinezhad et al. (2019) [44] | RCT double-blind | 500 mg/day | 3 months | 60 subjects with T2DM and albuminuria | 57 ± 9 | Glucose and insulin levels, HbA1c, HOMA-IR | Significant decrease in evaluated parameters in experimental group (p < 0.05) |
| Seyyedebrahimi et al. (2018) [45] | RCT double-blind | 800 mg/day | 8 weeks | 46 subjects with T2DM | 58 ± 6 | Glucose and insulin levels, HbA1c, HOMA-IR | No significant changes after resveratrol intervention |
| Thaung et al. (2020) [46] | RCT double-blind | 150 mg/day | 12 months | 129 postmenopausal women | 64 ± 1 | Glucose and insulin levels, HOMA-IR | No significant changes in evaluated parameters |
| Thazhath et al. (2016) [47] | RCT double-blindcrossover | 1 g/day | 5 weeks | 14 subjects with T2DM | 68 ± 2 | Glucose and HbA1c | No significant changes in glucose and HbA1c levels |
| Timmers et al. (2016) [48] | RCT double-blindcrossover | 150 mg/day | 4 weeks | 16 subjects with T2DM | 64 ± 4 | Glucose and insulin levels, insulin sensitivity, HbA1c | No effect of resveratrol on glycemic parameters |
| Van der Made et al.(2015) [49] | RCT double-blindcrossover | 150 mg/day | 4 weeks | 45 overweight and obese subjects | 61 ± 7 | Glucose and insulin levels, HOMA-IR | No changes in HOMA-IR and insulin levels. Glucose levels showed a tendency to decrease |
| Subgroup | No. of Trials | Effect Size | 95% CI | p Value | Heterogeneity (I2) | p Value for I2 |
|---|---|---|---|---|---|---|
| Glucose | ||||||
| Resveratrol dosage (I2 = 76%; p = 0.01) | ||||||
| <500 mg/day | 13 | −5.40 | −11.29, 0.49 | 0.07 | 97% | 0.00001 |
| 500–1000 mg/day | 13 | −7.54 | −12.29, −2.79 | 0.002 | 89% | 0.00001 |
| >1000 mg/day | 6 | 0.82 | −2.78, 4.42 | 0.66 | 51% | 0.00001 |
| Health status (I2 = 91%; p = 0.0008) | ||||||
| With T2DM | 15 | −13.36 | −21.09, −5.63 | 0.0007 | 96% | 0.00001 |
| Without T2DM | 17 | 0.18 | −1.52, 1.89 | 0.83 | 67% | 0.0001 |
| Duration (I2 = 0%; p = 0.89) | ||||||
| <3 months | 15 | −5.29 | −9.20, −1.39 | 0.008 | 81% | 0.00001 |
| ≥3 months | 17 | −4.83 | −9.75, 0.09 | 0.05 | 96% | 0.00001 |
| Age (I2 = 66%; p = 0.05) | ||||||
| <45 years | 6 | 0.08 | −4.08, −4.24 | 0.97 | 79% | 0.0002 |
| 45–59 years | 16 | −11.04 | −19.0, −3.07 | 0.007 | 96% | 0.00001 |
| ≥60 years | 10 | −2.06 | −4.39, 0.27 | 0.08 | 73% | 0.0001 |
| Insulin | ||||||
| Resveratrol dosage (I2 = 0%; p = 0.44) | ||||||
| <500 mg/day | 9 | −1.43 | −2.53, −0.32 | 0.01 | 90% | 0.00001 |
| 500–1000 mg/day | 12 | −0.78 | −1.85, 0.30 | 0.16 | 83% | 0.00001 |
| >1000 mg/day | 5 | −1.23 | −1.90, −0.57 | 0.03 | 73% | 0.006 |
| Health status (I2 = 0%; p = 0.57) | ||||||
| With T2DM | 12 | −0.94 | −1.62, −0.25 | 0.007 | 77% | 0.00001 |
| Without T2DM | 14 | −1.39 | −2.80, 0.01 | 0.05 | 91% | 0.00001 |
| Duration (I2 = 0%; p = 0.38) | ||||||
| <3 months | 13 | −0.93 | −1.53, −0.33 | 0.002 | 69% | 0.0001 |
| ≥3 months | 13 | −1.65 | −3.15, −0.16 | 0.03 | 93% | 0.00001 |
| Age (I2 = 42%; p = 0.18) | ||||||
| <45 years | 5 | −3.60 | −7.65, 0.46 | 0.08 | 96% | 0.00001 |
| 45–59 years | 13 | −0.97 | −1.82, −0.12 | 0.02 | 82% | 0.00001 |
| ≥60 years | 8 | −0.32 | −1.01, 0.36 | 0.35 | 57% | 0.02 |
| HbA1c | ||||||
| Resveratrol dosage (I2 = 0%; p = 0.56) | ||||||
| <500 mg/day | 7 | −0.20 | −0.42, 0.02 | 0.08 | 99% | 0.00001 |
| 500–1000 mg/day | 8 | −0.06 | −0.21, 0.10 | 0.48 | 69% | 0.002 |
| >1000 mg/day | 2 | −0.25 | −1.18, 0.69 | 0.61 | 68% | 0.08 |
| Health status (I2 = 87%; p = 0.005) | ||||||
| With T2DM | 12 | −0.22 | −0.40, −0.04 | 0.02 | 97% | 0.00001 |
| Without T2DM | 5 | 0.05 | −0.01, 0.10 | 0.11 | 0% | 0.78 |
| Duration (I2 = 0%; p = 0.38) | ||||||
| <3 months | 9 | 0.02 | −0.08, 0.13 | 0.66 | 64% | 0.004 |
| ≥3 months | 8 | −0.29 | −0.50, −0.08 | 0.006 | 98% | 0.00001 |
| Age (I2 = 85%; p = 0.001) | ||||||
| <45 years | 1 | 0.05 | −0.04, 0.14 | 0.29 | --- | --- |
| 45–59 years | 9 | −0.34 | −0.54, −0.13 | 0.002 | 98% | 0.00001 |
| ≥60 years | 6 | 0.07 | 0, 0.15 | 0.05 | 0 | 0.48 |
| HOMA-IR | ||||||
| Resveratrol dosage (I2 = 0%; p = 0.62) | ||||||
| <500 mg/day | 11 | −0.22 | −0.55, 0.11 | 0.19 | 57% | 0.01 |
| 500–1000 mg/day | 12 | −0.60 | −1.44, 0.24 | 0.16 | 97% | 0.00001 |
| >1000 mg/day | 5 | −0.22 | −0.74, 0.30 | 0.42 | 46% | 0.11 |
| Health status (I2 = 64%; p = 0.10) | ||||||
| With T2DM | 12 | −0.83 | −1.68, −0.02 | 0.04 | 96% | 0.00001 |
| Without T2DM | 16 | −0.08 | −0.33, 0.17 | 0.54 | 55% | 0.004 |
| Duration (I2 = 0%; p = 0.83) | ||||||
| <3 months | 14 | −0.36 | −1.11, 0.39 | 0.35 | 96% | 0.00001 |
| ≥3 months | 14 | −0.45 | −0.91, 0.00 | 0.05 | 83% | 0.00001 |
| Age (I2 = 0%; p = 0.70) | ||||||
| <45 years | 5 | −0.57 | −1.19, 0.04 | 0.07 | 68% | 0.01 |
| 45–59 years | 14 | −0.39 | −1.25, 0.47 | 0.38 | 96% | 0.00001 |
| ≥60 years | 9 | −0.28 | −0.60, 0.03 | 0.08 | 55% | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Martínez, B.I.; Ruiz-Ramos, M.; Pedraza-Chaverri, J.; Santiago-Osorio, E.; Mendoza-Núñez, V.M. Hypoglycemic Effect of Resveratrol: A Systematic Review and Meta-Analysis. Antioxidants 2021, 10, 69. https://doi.org/10.3390/antiox10010069
García-Martínez BI, Ruiz-Ramos M, Pedraza-Chaverri J, Santiago-Osorio E, Mendoza-Núñez VM. Hypoglycemic Effect of Resveratrol: A Systematic Review and Meta-Analysis. Antioxidants. 2021; 10(1):69. https://doi.org/10.3390/antiox10010069
Chicago/Turabian StyleGarcía-Martínez, Beatriz Isabel, Mirna Ruiz-Ramos, José Pedraza-Chaverri, Edelmiro Santiago-Osorio, and Víctor Manuel Mendoza-Núñez. 2021. "Hypoglycemic Effect of Resveratrol: A Systematic Review and Meta-Analysis" Antioxidants 10, no. 1: 69. https://doi.org/10.3390/antiox10010069